Podcast: How can communities implement better support programs? (46:11)
Click the link below to listen to all of the researchers answer the question “How can communities implement better support programs?” in audio format on our podcast!

Understanding Homelessness in Canada by Kristy Buccieri, James Davy, Cyndi Gilmer, and Nicole Whitmore is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, except where otherwise noted.
1
Homelessness is an area of study that spans across academic disciplines. This was the premise with which we began this project. “Understanding Homelessness in Canada: From the Street to the Classroom” is a dynamic resource that can be used as a textbook, online course, and/or general interest book. Early in the design process, we had the idea to set up each chapter as a field of study, and we asked ourselves what three questions a student in that field might have about homelessness. We then reached out to many leading homelessness researchers across Canada and posed a sub-set of those questions to them. We recorded the conversations, created a series of videos from each, and imbedded them throughout this book alongside contemporary Canadian research with a focus on publications from 2018 and beyond.
We have included a range of academic disciplines in this book, divided into five parts consisting of Indigenous and Canadian Studies, Mental Health and Public Health Studies, Population Studies, Social Sciences, and Health Sciences. Our intention in doing so, was to provide instructors and students with a resource that contains information and opens a space for further exploration. We do not suggest that the chapters are a definitive resource for each academic discipline, but rather that they present information that students should know related to homelessness and their field. For instance, you will not learn how to be a Social Worker from the Social Work chapter, but you will learn key points Social Workers should know about homelessness. It is our intention that instructors and students will use this resource as a starting point and adapt it with their own theoretical and practical applications.
Each chapter begins with a real life scenario depicting one or more composite individuals. We have taken aspects of real people’s experiences and put them together in a way that highlights key social issues, without identifying any particular person. Throughout this book, you will also notice artwork created by people with lived experience of homelessness, additional information for students who want to learn more, and research ideas for students who wish to undertake an undergraduate or master’s thesis related to homelessness. Our team is very proud of this resource and hope that you will find it useful in your own journeys, learning and teaching about homelessness in Canada.
If you are an instructor who wishes to use the complete book, parts, or individual chapters you may wish to use the direct links below and imbed them directly into your learning management system (such as Blackboard, Moodle, or Canvas), so that students are able to easily locate the material.
Throughout this book, we consistently use a series of icons to identify key parts of each chapter. Below is an overview of what they mean and why you should be on the lookout for them.
 When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have the Autoplay setting turned on to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have the Autoplay setting turned on to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Each chapter is designed to answer three questions that students in the field of study might have about homelessness. This icon is used to indicate a “Featured Reading” related to each of the three questions. Each Featured Reading is Canadian, open-access, recently published, and accessible through a direct link next to the icon. For instructors using this ebook as an online course, we recommend assigning these Featured Readings as required reading.
about homelessness. This icon is used to indicate a “Featured Reading” related to each of the three questions. Each Featured Reading is Canadian, open-access, recently published, and accessible through a direct link next to the icon. For instructors using this ebook as an online course, we recommend assigning these Featured Readings as required reading.

At various points throughout the ebook we use this icon to draw your attention to online resources. These additional resources are points of interest, such as websites and blogs. These are designed to take you directly to the online resource by clicking the link. Please note, they will open in a separate window, so you do not lose your place in the ebook.
Throughout each chapter, we pose questions for students to stop and consider under the heading, “What do  you think?” This icon appears next to these questions to encourage students to temporarily pause and reflect upon the material they are reading and how they feel about it. Instructors may wish to use these as discussion questions, either in class or as part of an online discussion board.
you think?” This icon appears next to these questions to encourage students to temporarily pause and reflect upon the material they are reading and how they feel about it. Instructors may wish to use these as discussion questions, either in class or as part of an online discussion board.

At the end of each section, you will encounter this icon that provides a link to the “Understanding Homelessness in Canada” podcast. The researcher videos contained within the section have been compiled into a podcast episode, for readers who wish to download and listen to them again.
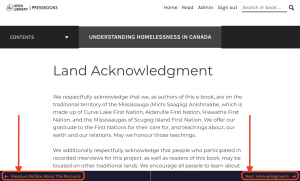
To navigate the chapters, you may use the “Contents” drop-down menu on the left-hand side by clicking on the “+” sign next to the main chapter title. Once you are in a chapter, you may also move through the sections by using the “Previous” and “Next” arrows at the bottom of the page (as shown in the image below). Each page will also have an up arrow at the bottom-middle to take you back to the top.
All of the videos in this ebook are fully captioned. However, depending on your own personal YouTube settings, you may need to turn them on if you want to view them. To turn on closed-captioning, click on the CC button at the bottom of the video player on the video you are watching.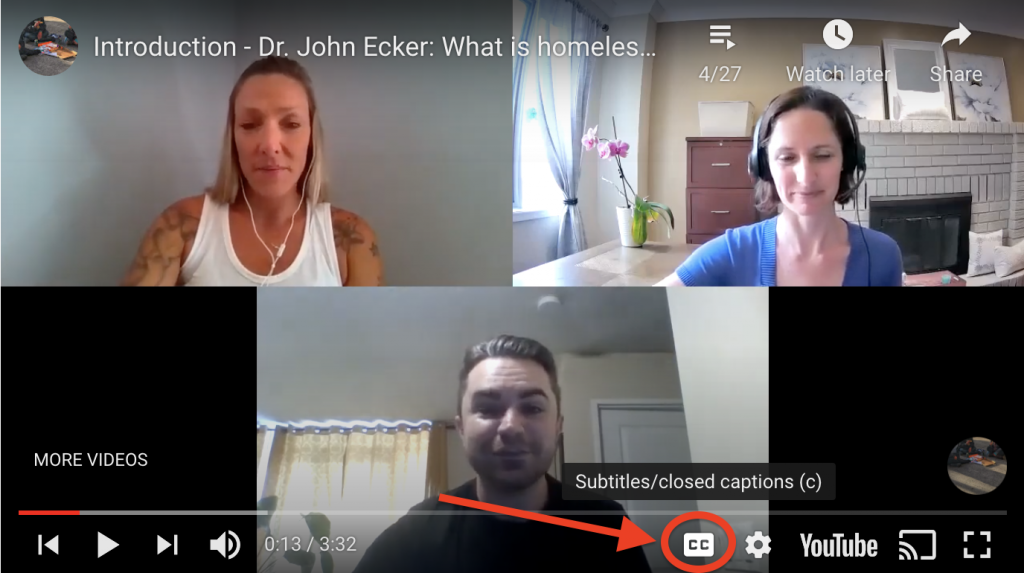
We appreciate your interest in this resource, and hope that you will find it both engaging and informative. After you have read it, we hope that you will provide us with feedback: Share your thoughts with us
Happy Reading,
From the Understanding Homelessness in Canada Team
2
This is an accessibility statement from Understanding Homelessness in Canada: From the Street to the Classroom. It was generated using an online tool from Generate an Accessibility Statement | Web Accessibility Initiative. It is our intention to make this resource as accessible as possible.
Understanding Homelessness in Canada: From the Street to the Classroom takes the following measures to ensure accessibility of the ebook:
We welcome your feedback on the accessibility of the ebook. Please let us know if you encounter accessibility barriers on the ebook:
We try to respond to feedback within 2 business days for electronic communications and 2 weeks for mail communications.
Despite our best efforts to ensure accessibility of the ebook , there may be some limitations. Below is a description of known limitations, and potential solutions. Please contact us if you observe an issue not listed below.
Known limitations for the ebook:
Understanding Homelessness in Canada: From the Street to the Classroom assessed the accessibility of the ebook by the following approaches:
If you have suggestions on how to make this ebook more accessible, please contact us at understandinghomelessness.ebook@gmail.com
This statement was created on 22 February 2022 using the W3C Accessibility Statement Generator Tool.
3
We respectfully acknowledge that we, as authors of this e-book, are on the traditional territory of the Mississauga (Michi Saagiig) Anishnaabe, which is made up of Curve Lake First Nation, Alderville First Nation, Hiawatha First Nation, and the Mississaugas of Scugog Island First Nation. We offer our gratitude to the First Nations for their care for, and teachings about, our earth and our relations. May we honour those teachings.
We additionally respectfully acknowledge that people who participated in recorded interviews for this project, as well as readers of this book, may be located on other traditional lands. We encourage all people to learn about the territories they occupy and the cultures of the land’s original stewards.
The Native-Land.ca website provides a resource for beginning this engagement.
4
![]()
“Understanding Homelessness in Canada: From the Street to the Classroom” was a collaborative effort between Trent University and the Canadian Observatory on Homelessness.
![]()

Thank you to Green Wood Coalition and Peterborough AIDS Resource Network for supporting staff involvement and facilitating artwork contributions for this project.

This project was made possible with funding by the Government of Ontario and through eCampusOntario’s support of the Virtual Learning Strategy.
![]()
To learn more about the Virtual Learning Strategy visit: https://vls.ecampusontario.ca.
Our team would like to thank Emma Armstrong, Katelyn Bell, Phyllis Owusu-Ansah, Kaylie Smith, and Virginia Stammers for being student reviewers. We appreciate the time and energy you dedicated to reviewing chapter drafts and offering insightful feedback.
![]() Thank you to the artists with lived experience of homelessness, whose artwork greatly enriched the content of this book.
Thank you to the artists with lived experience of homelessness, whose artwork greatly enriched the content of this book.
![]() Thank you to the participants who provided the quotes we used in the cards throughout this book.
Thank you to the participants who provided the quotes we used in the cards throughout this book.
![]() Thank you to all of the researchers who contributed their time and knowledge to this book.
Thank you to all of the researchers who contributed their time and knowledge to this book.
5
This resource was created by a whole team of people working together on different aspects. Some of us you will see on camera, but much of the work happened “behind the scenes.” Here is the cast of (sometimes whacky!) characters that produced this book.

NICOLE WHITMORE
JAMES DAVY

CYNDI GILMER

KRISTY BUCCIERI

STEPHANIE FERGUSON

JAMES BAILEY

JOSH ANDREWS

STEPHANIE VASKO

BRAD KEIZERWAARD

CARTER TONGS
6
Our team would like to express our appreciation for the 26 researchers who participated in recorded conversations with us about homelessness in Canada. The collective knowledge of this group is tremendous and provides a depth of understanding we could not have achieved on our own. Below we provide a brief biography of the researchers you will hear from throughout this book. We encourage you to learn more about the amazing work they are doing and to see the reference list for some of their most recent publications.
Please note that researchers have approved their own video segments but have not reviewed each other’s videos nor the written content of the book. We thoroughly enjoyed speaking with these researchers and are confident you will find them engaging as well. Taken together, we have collected 15 hours of their expert reflections on some pretty tough questions. Keep reading to learn more about homelessness in Canada, from the streets to the classroom.

Dr. Alex Abramovich is an Independent Scientist with the Institute for Mental Health Policy Research at the Centre for Addiction and Mental Health.
Abramovich Interview – YouTube Playlist

Dr. Tim Aubry is a Professor of Psychology at the University of Ottawa.
Aubry Interview – YouTube Playlist

Dr. Erin Dej is an Assistant Professor with the Department of Criminology at Wilfrid Laurier University.
Dej Interview – YouTube Playlist

Dr. John Ecker is the Research Manager with the MAP Centre for Urban Health Solutions atUnity Health Toronto.
Ecker Interview – YouTube Playlist

Dr. Nick Falvo is a Research Consultant at Nick Falvo Consulting.
Falvo Interview – YouTube Playlist

Dr. David Firang is an Assistant Professor with the Department of Social Work at Trent University.
Firang Interview – YouTube Playlist

Dr. Cheryl Forchuk is a Research Chair in Aging, Mental Health, Rehabilitation and Recovery at Western University.
Forchuk Interview – YouTube Playlist

Dr. Tyler Frederick is an Associate Professor in Criminology and Justice at Ontario Tech University.
Frederick Interview – YouTube Playlist

Dr. Stephen Gaetz is the President of the Canadian Observatory on Homelessness at York University.
Gaetz Interview – YouTube Playlist

Dr. Jonathan Greene is an Associate Professor in Political Studies at Trent University.
Greene Interview – YouTube Playlist

Dr. Stephen Hwang is the Director of the MAP Centre for Urban Solutions at St. Michael’s Hospital.
Hwang Interview – YouTube Playlist

Dr. Jeff Karabanow is the Associate Director and a Professor with the School of Social Work at Dalhousie University.
Karabanow Interview – YouTube Playlist

Dr. Jacqueline Kennelly is a Professor with the Department of Sociology and Anthropology at Carleton University.
Kennelly Interview – YouTube Playlist

Dr. Nick Kerman is a Post-Doctoral Fellow at the Centre for Addiction and Mental Health.
Kerman Interview – YouTube Playlist

Dr. Sean Kidd is the Chief of the Psychology Division at the Centre for Addiction and Mental Health.
Kidd Interview – YouTube Playlist

Dr. Katrina Milaney is an Associate Professor in Community Health Sciences at the University of Calgary.
Milaney Interview – YouTube Playlist

Dr. Naomi Nichols is a Tier 2 Canada Research Chair with the Department of Sociology at Trent University.

Dr. Bill O’Grady is a Professor with the Department of Sociology and Anthropology at the University of Guelph.
O’Grady Interview – YouTube Playlist

Dr. Abe Oudshoorn is an Associate Professor with the Arthur Labatt Family School of Nursing at Western University.
Oudshoorn Interview – YouTube Playlist

Dr. Bernie Pauly is a Professor with theSchool of Nursing at the University of Victoria.
Pauly Interview – YouTube Playlist

Jessica Rumboldt is a Post-Doctoral Fellow in Indigenous Homelessness at York University.
Rumboldt Interview – YouTube Playlist

Dr. Rebecca Schiff is the Chair and Associate Professor in Health Sciences at Lakehead University.
Schiff Interview – YouTube Playlist

Dr. Kaitlin Schwan is the Director of Research, with Making the Shift at the Canadian Observatory on Homelessness.
Schwan Interview – YouTube Playlist

Dr. Kelli Stajduhar is a Professor with the School of Nursing at the University of Victoria.
Stajduhar Interview – YouTube Playlist

Dr. Naomi Thulien is a Scientist with the Li Ka Shing Knowledge Institute at St. Michael’s Hospital.
Thulien Interview – YouTube Playlist

Dr. Jeannette Waegemakers Schiff is a Professor with the School of Social Work at the University of Calgary.
I
Let’s play a game.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=512#h5p-20
How did you do? If indeed you found this game to be a little too easy, then you have demonstrated an understanding of the term ‘home’ and the subjective meanings we collectively attach to it in society. Home is thought to be a safe and secure internal place that protects us from the dangerous outside world. But is it?
For many Canadians, the home is not a place of refuge but rather a place fraught with conflict, stress, oppression, and/or insecurity. Home can be many things to people, some which are good and some which are not. The reasons that people leave or are pushed out of their homes are varied and complex. Despite a common stereotype that people choose homelessness, very rarely is this the case. Rather, people sometimes come to a point in their lives where homelessness is the only alternative they have. It is not a good one, but it may be the only one.
1
In this chapter you are invited to enter into an ongoing dialogue about what homelessness is, how it was created, and what we can do to prevent it. Many of the themes identified here will re-emerge throughout the chapters that follow. As you begin to engage with the study of homelessness in Canada, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that homelessness is rarely an individual choice, but rather results from circumstances in a person’s life that are often beyond their control. You are encouraged to work through this material with an open mind about what you read, hear, and see, even if (or particularly if) it contradicts previous stereotypical images that might have shaped your perceptions about homelessness and homeless people. Read on to learn more about what homelessness means, how we gather information about it, and why we all would benefit from shifting our collective focus towards prevention.
2
We begin this chapter by presenting two composite scenarios that reflect real-world experiences of homelessness in Canada. As you read through these scenarios, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenarios, and a critical perspective, to think about how the scenarios represent larger issues impacting people in our society.
After pausing respond to reflection questions, we will endeavour to answer each question posed in the learning objectives. What is homelessness? How do we know what we know about homelessness? Why does homelessness prevention matter? Throughout this chapter, we will examine these three questions using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenarios presented at the beginning and reconsider them in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
3
As you being to learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with these real life composite scenarios. Take a moment here to pause and consider these people’s experiences.
John
John is a 45-year-old male who lives downtown in a large city. During the day he can be found on the same street corner, outside a Tim Horton’s sitting with his dog Rex on a flattened cardboard box. He has an empty Tim’s cup in front of him and a small handwritten sign asking for money. He is often asleep or dozing and people walk around him without acknowledging that he is there. Some people drop change into his cup. John spends his nights walking the back alleys downtown attempting to avoid both the police and other street people. He knows that if he stops to try and sleep in a vestibule at a bank or in an underground parking garage he will be hassled by the police. He’ll be given yet another ticket he can’t pay.
Tasha and Raoul
Tasha and Raoul are a young couple. Tasha is new to Canada and her immigration status is in limbo. They are living in an old trailer parked in a wooded area on a field owned by an elderly farmer. The lot is 10 kilometers outside of a small rural town. They have no hydro and no running water. They have rigged up an outdoor shower using buckets of water from a nearby stream. They have four dogs. They rely on hitchhiking for rides into town as they have no other transportation. Tasha has a chronic health issue that requires daily medication. Her overall health is not good and not well managed.
With these scenarios fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to these scenarios again at the end of the chapter.
Reflection Questions
4
As we sat down to write this book, we decided to frame each chapter around a set of questions. While this was an organizational choice, it was also an intentional choice to encourage you to begin your studies with questions at the forefront of your mind. We encourage you to take a moment at the beginning of each section to think about how you would answer the question posed in the title. In this instance, what is homelessness? We have asked this exact question to a series of leading homelessness researchers from across the country, whose work you will also have the opportunity to read.
Before you hear from them, take a moment to answer this question for yourself and see how your definition compares with theirs. This activity is useful in documenting your own starting point and is for your eyes only. It will not be submitted to your instructor, so you should feel free to write as little or as much as you wish to answer the question.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=554#h5p-25
A 1993 book entitled, Down and out in Canada: Homeless Canadians opens with the quote, “In 1990s Canada, the problem of homelessness remains an enigma. The homeless are largely a social crisis for which there is no audience. There is little political currency to be made in championing the cause of the weakest in our society, those who are without benefit of shelter” (O’Reilly-Fleming, 1993, pg.1). Is it still the case that homelessness remains an enigma that no one pays attention to 30 years later? As you will see, interviews with Canadian homelessness researchers show that in fact homelessness is well understood despite its complexity.
What remains the same is O’Reilly-Fleming’s (1993) observation that many Canadians know very little about homelessness and have stereotypical images drawn from momentary and often fearful glimpses on downtown streets or from random media images. These themes emerged as we sat down to speak independently with Dr. Stephen Hwang and Dr. Stephen Gaetz about how they would each define homelessness.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have the Autoplay setting turned on to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Stephen Hwang explains that homelessness can be thought of as being unhoused and not having a stable place of one’s own to live. He argues that homelessness is sometimes mistakenly viewed as an unusual state, when it is really just a continuum of housing instability and inadequacy that are part of a larger phenomenon. He offers the analogy that we recognize the complexity of nutrition as not just being about whether a person eats or starves to death, but rather we consider whether people have access to quality food at an affordable price. By thinking about homelessness in narrow ways as whether someone is absolutely homeless or not, we miss the larger issue of whether people have access to quality housing at an affordable price. Dr. Hwang notes that there are different types of homelessness that exist along a continuum, and as the definition gets broader more people are included, who are difficult to identify and engage with. He concludes that rather than becoming fixated on one specific definition of homelessness, we should focus more on being clear about what we mean when we use the term. This video is 2:36 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: What is homelessness?
In this video, Dr. Stephen Gaetz argues that the category of homelessness is something we came up with to name a problem we created. He notes that as a society we define people by their housing status and then make judgements and infantilize them because of it, on the basis that they are a “homeless person” and therefore different somehow. Dr. Gaetz counters that it is important to begin with the assumption that this is a human being with rights. He encourages us to consider what a developing adolescent or adult experiencing homelessness needs and realize that it is not all that different than the needs of someone who has housing. Dr. Gaetz concludes that we must move towards a greater recognition that people are people, and homelessness is part of a person’s story but that it does not define them. This video is 2:16 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: Creating the homeless person
Dr. Hwang and Dr. Gaetz both make the important point that homelessness does not define a person’s identity. Rather than thinking about homelessness as an unusual state, we must begin with the understanding that it is an experience had by human beings with human rights. The following video, Do you see me? was created by I Heart Home and explores the stories of people living in Calgary, Alberta. As you watch this video we encourage you to remember the advice from Dr. Gaetz, to begin with the assumption that this is a human being with rights, and then go from there.
Keeping at the forefront of our minds that homelessness is an issue impacting human beings who have rights, we can now shift towards exploring the definitions. Here we begin with videos from Dr. Tim Aubry and Dr. Jonathan Greene, where they each provide an overview of the types of homelessness people commonly experience and the different factors that need to be considered in formulating a definition.
In this video, Dr. Tim Aubry explains that homelessness is often defined similarly in research and practice, as occurring when a person lacks their own place that is safe, sheltered, and without short-term length of stay limitations. He notes that there are different types of homelessness, including people residing in emergency shelters, sleeping rough, staying in encampments, or more hidden by staying temporarily with friends or family. Dr. Aubry concludes by discussing the Canadian definition, which further stretches to also include considerations of people who are at-risk of homelessness. This video is 2:38 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: What is homelessness?
In this video, Dr. Jonathan Greene explains that how we define homelessness as a concept, idea, and state of being changes across locations and evolves over time. He argues that since our understandings of homelessness are informed by the political, cultural, and social forces at play, there is no straightforward answer. Dr. Greene notes that currently many government indicators of homelessness reference housing, such as whether there is an adequate supply, but that this is a relatively new approach as Professor David Hulchanski shows, that emerged in the 1980s. Dr. Greene notes that in contemporary Canadian policies, such as the Reaching Home strategy, the government has adopted a continuum approach that incorporates absolutely homeless, emergency sheltered, being insecurely housed, and being at-risk of homelessness. He draws our attention to the temporal aspects of definitions as well, noting that the recent construction of chronic, episodic, and transitional homelessness has created three priority populations. Dr. Greene concludes that the definition of homelessness changes between locations and evolves over time, but that across these we want to think about the ideas of house and home, locations people can be in, and how homelessness can be experienced differently by different individuals and households. This video is 6:05 in length and has closed captions available in English.
Key Takeaways – Dr. Jonathan Greene: What is homelessness?
As we heard from Dr. Aubry and Dr. Greene, there are different types of homelessness that people may experience. These are the result of structural factors, systems failures, and individual circumstances. Take a moment to explore these further in this interactive module from the Homeless Hub entitled Why do people become homeless? You may also wish to share this with others through your social networks and invite them to join the conversation. Be sure to follow us on Twitter using @Homeless_ebook and #UnderstandingHomelessness.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=554#h5p-26
There are many factors that contribute to homelessness and the experience is different for every person. Yet, there is considerable value in recognizing the shared characteristics. In 2012 the Canadian Observatory on Homelessness released a definition that was collaboratively developed and has been widely adopted in research, policy, and practice across the country (Gaetz et al., 2012). Here we discuss this definition with Dr. Stephen Gaetz, President of the Canadian Observatory on Homelessness. Following this video, we encourage you to explore the definition further with an introductory video and then a review of the document itself.
In this video, Dr. Stephen Gaetz explains that homelessness describes a situation in which people do not have adequate, safe, and affordable housing, nor the immediate prospect of getting it. It does not arise from a person’s individual characteristics but rather is produced and sustained by society. He notes that blaming individuals for their homelessness fails to hold society responsible for its need to do something about the problem. Dr. Gaetz concludes by discussing the Canadian definition of homelessness, as a document that provides common language and a typology that has been widely adopted by researchers and governments. This video is 3:03 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: What is homelessness?
Gaetz, S., Barr, C., Friesen, A., Harris, B., Hill, C., Kovacs-Burns, K., Pauly, B., Pearce, B., Turner, A., & Marsolais, A. (2012) Canadian definition of homelessness. Toronto: Canadian Observatory on Homelessness Press.
Canadian Definition of Homelessness | The Homeless Hub
Now that you have had the chance to read through it, what do you think of the Canadian Definition of Homelessness? Is there anything you would add to it or take away?
As we posed the question, “What is homelessness?” to different researchers, the Canadian definition emerged as a key document that shapes the way we collectively have come to think about homeless as existing along a continuum. The Canadian definition also serves as a starting point for thinking about the experiences of different populations and about housing as a fundamental human right.
Here we share our conversations with Dr. John Ecker, Dr. Kaitlin Schwan, and Dr. Erin Dej, where they discuss how the Canadian definition of homelessness has influenced their understandings of what homelessness means. You will also hear reference to the Indigenous definition of homelessness in Canada, published by scholar Jesse Thistle (2017), which is discussed in detail in the chapter on Indigenous Studies.
In this video, Dr. John Ecker offers a comprehensive definition of homelessness as the lack of adequate, suitable, and affordable housing, and as a violation of the human right to housing. Dr. Ecker expands by discussing the four parts of the Canadian Observatory on Homelessness’ definition, which includes people who are unsheltered, emergency sheltered, provisionally accommodated, and at-risk of homelessness. He notes that it is important to think about different subgroups who experience homelessness at higher rates or in unique ways, such as women, families, and youth. Dr. Ecker concludes by drawing attention to how these definitions are westernized understandings, and points towards Jesse Thistle’s definition of Indigenous homelessness as being a useful resource for thinking about homelessness in different ways. This video is 3:32 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: What is homelessness?
In this video, Dr. Kaitlin Schwan explains that homelessness is a condition where people lack access to permanent and affordable housing that is safe, secure, and able to meet their needs. She notes that homelessness exists along a continuum, from absolutely homeless on one end to being in core housing need on the other. Dr. Schwan argues that within a Canadian context it is critical to understand Indigenous homelessness and points towards the definition developed by Jesse Thistle that identifies 12 dimensions. Dr. Schwan concludes by noting that the 2019 National Housing Strategy Act declared housing to be a human right, and that we need to understand homelessness as a violation of this right. This video is 3:19 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: What is homelessness?
In this video, Dr. Erin Dej explains the four elements that make up the Canadian Observatory on Homelessness’ definition of homelessness. She notes that the first two elements – absolutely homeless and emergency sheltered – are what people most often associate with homelessness. However, she notes it is important to pay attention to the additional elements, which sometimes get overlooked. Those who are provisionally accommodated have somewhere to stay but it is temporary, such as transitional housing, couch surfing, and leaving a correctional or hospital facility without identified housing. Dr. Dej argues we must pay special attention to those at-risk of homelessness because while they have somewhere to stay it is not safe, affordable, or acceptable, such as those who are facing eviction, living in overcrowded housing, and/or experiencing domestic violence. Dr. Dej concludes that we can also learn about people at-risk of homelessness by applying the Canada Mortgage and Housing Corporation’s definition, of those spending 30% or more on housing as being in core housing need and one crisis away from homelessness. This video is 3:34 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: What is homelessness?
Throughout this book, we will share quotes from a research study we conducted in two small / rural towns in Ontario, as one way to provide space for the voices of people with lived experience. The first of these cards is presented below. To learn more about this project and the participants, please visit the Trent University Homelessness Research Collective (2019) website.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=554#h5p-27
A key component of the Canadian definition of homelessness is that it includes people who are at–risk of losing their housing, due to issues such as spending too much of their income on rent, living in overcrowded conditions, or living in housing that is not good quality. Whether or not the definition should include people who are at-risk has been a hotly debated topic, with some arguing that a broad definition is needed to allow us to focus on prevention, and others arguing a narrow definition allows us to focus resources on those who are most in need.
Dr. Nick Falvo and Dr. Jeannette Waegemakers Schiff both discuss the issue of risk and vulnerability as factors that need to be considered carefully in crafting a definition of homelessness. As you watch these conversations, consider where you stand on this debate. Should the definition of homelessness include people who are at imminent risk of losing their housing? In this video, Dr. Nick Falvo defines homelessness as relating to people living in an emergency shelter, outside, or in a structure not meant for human habitation. He notes that these individuals tend to be included in point-in-time counts. Beyond this, he explains, there are also individuals who meet the Canada Mortgage and Housing Corporation’s definition of core housing need. Dr. Falvo argues that while a narrow definition is not as widely accepted, for fear those in housing need will be forgotten, it is possible to have a narrow and broad definition that reflects these housing distinctions. This video is 1:21 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: What is homelessness?
In this video, Dr. Jeannette Waegemakers Schiff explains that to understand the risk of homelessness we must consider people’s access to social and economic protections. There are some people who are relatively immune to homelessness because they have secure jobs and strong cash reserves that will allow them to become rehoused again quickly if they lose their housing. However, Dr. Waegemakers Schiff notes there is a large proportion of society who do not have the same supports to protect them, including people with adverse psychosocial issues, youth who have been displaced and alienated from their homes, women who experience domestic violence, and people with serious physical conditions who are reliant on disability income supports. Dr. Waegemakers Schiff argues that the COVID-19 pandemic exposed many pre-existing vulnerabilities and that who is at risk and who is not, casts the great divide. She concludes by discussing recent research into the vulnerability of post-secondary students during the COVID-19 pandemic, particularly as measures closed spaces they rely on for food and shelter. This video is 4:54 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: Defining vulnerability
In this section, we have explored the question, “What is homelessness?” At the beginning, we asked you to write your own response and to keep it in mind as you progressed through the material. We encourage you now to look back at your response, or simply bring it to mind, and consider how it compares to what you have seen, heard, and read. Has your definition of homelessness changed? If so, how would you answer this question now?
When asked to discuss what homelessness is, researchers in the field spoke about many important issues. They began by explaining that homelessness is not an unusual state or a defining characteristic, but rather something that happens to human beings. They discussed the different types of homelessness, the various causes, and the factors that need to be considered in creating a definition. We learned from these researchers that there is a Canadian definition of homelessness that was published in 2012, that has been influential in research, policy, and practice. This definition provides a typology for thinking about homelessness as a continuum, rather than a dichotomy of being ‘homeless or housed.’ The Canadian definition includes those who are at-risk of homelessness, which other definitions classify as those who pay more than 30% of their income, making them in core housing need.
When students sign up to take a course on homelessness they often question what there is to know that could take an entire semester to learn. We hope that even this brief introductory section demonstrates the complexity of homelessness, what we already know, and how much more there is still to learn. Join us in the next section, as we consider how we know what we know about homelessness.
Click the link below to listen to all of the researchers answer the question “What is Homelessness?” in audio format on our podcast!
5
As you begin this section, we encourage you to think about the question of how we know what we know about homelessness. This question, like many we will explore throughout this book, seems deceptively simple because we may confuse our own opinions and beliefs with validated knowledge. What we know comes from many different sources, some more reliable than others. Before you hear from the researchers in this section, we encourage you to take a moment to jot down your own thoughts. You may also want to consider related questions, such as where you have learned about homelessness, like your home or school, what experiences you have had that might have influenced your perceptions, and whether you feel the information you have received comes from credible sources. Remember that your answer here is just for your reflection, it may be as brief or long as you wish, and it is not going to be seen by others.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=556#h5p-28
It may come as no surprise to you that much of what we know about homelessness in Canada comes from research over the past 40 years. The body of research that has developed over time reflects the different methodologies and approaches researchers have used to learn about this issue. You may be interested to know that much of the interactive content for this book comes from our partners at the Canadian Observatory on Homelessness, which is the largest national research institute devoted to homelessness in Canada. They are also the curator of the Homeless Hub, an online library of over 30,000 resources.
Throughout this book, you will get to hear directly from many influential researchers in the field of homelessness, who have helped to create the research that shapes public policy decisions today. As our knowledge continually evolves, we have made the conscious decision to focus on studies that were published by Canadian researchers within the 5 years preceding publication of this book. In the next set of videos, you will hear from Dr. Kaitlin Schwan and Dr. John Ecker, who provide an overview of how research has changed over time, the importance of peer-review and evaluation, and the impact on modern day policy.
In this video, Dr. Kaitlin Schwan explains that mass homelessness, as we know it today in Canada, started to emerge in the 1980s. In response, we have tried many policy and program interventions, which have been evaluated using a range of research methods. The knowledge from these studies has been synthesized in peer-reviewed journals and made publicly available, such as through the Homeless Hub website. Dr. Schwan notes the key to understanding homelessness is listening to people with lived expertise, as they have experienced the ways various systems and structures operate to create conditions for those living without housing. This video is 1:46 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: How do we know what we know about homelessness?
In this video, Dr. John Ecker discusses the trajectory of homelessness research, from an early focus on investigating the causes and consequences, to a modern day focus on applied research into identifying solutions and empowering people with lived experience. He notes that there are many different types of research, and that they are often published in peer-reviewed journal articles which allows for confidence in what is being reported. Dr. Ecker concludes by acknowledging the important work of grassroots advocacy organizations, particularly those led by individuals with lived experience, in providing information and resources to the general public and to policy makers. This video is 4:04 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: How do we know what we know about homelessness?
We heard from Dr. Schwan and Dr. Ecker that research on homelessness has changed over the past 30 to 40 years. In 1993 O’Reilly-Fleming wrote, “One of the great difficulties which confronts any attempt to deal with and analyse the problem of homelessness in Canadian society is the lack of consistent and reliable data on both the number and composition of the homeless population” (pg.11). Trying to learn about the number of people experiencing homelessness in any given community is still challenging today because of hidden homelessness. Some populations are particularly difficult to reach and enumerate, such as Indigenous individuals, refugees and new Canadians, women, and youth. For hidden populations, multi-methods like respondent-driven sampling may be needed in addition to more standard census data collection (Rotondi et al., 2017).
One of the main changes that has occurred in the past decade is the development of point-in-time [PIT] counts to better identify the number of people experiencing homelessness in a given community. These counts are done on a set day and involve volunteers going to shelters, drop-in centres, and public places like city parks to collect information about the people within these spaces who are experiencing homelessness. These counts do not identify every person, and still frequently miss the hidden populations, but they are one approach we have to better understand the occurrence of homelessness in communities across Canada. Learn more with this brief video from Employment and Social Development Canada.
Here Dr. Erin Dej explains more about point-in-time counts, and why it is important we recognize that not all populations will be equally represented in these efforts.
In this video, Dr. Erin Dej explains that the emergence of homelessness research in Canada really began with the rise in mass homelessness in the 1990s. Researchers at the time focused on individuals to see who was experiencing homelessness and why. Over time, this research has evolved to focus on broader systemic and structural causes of homelessness. Dr. Dej notes that more recently we have also learned about homelessness through point-in-time counts in which cities do a one-day count of all the people they can find who are experiencing homelessness. While these counts provide valuable information about homelessness within cities and over years, Dr. Dej also cautions that they tend to miss hidden populations such as women, LGBTQ2S+ persons, youth, and Indigenous persons. This video is 3:43 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: How do we know what we know about homelessness?
Policy makers often use point-in-time data in their decision-making about what programs will get funded in a given community, but this data often misses key populations like women, LGBTQ2S+ persons, youth, and Indigenous people. How do you think we can improve our efforts to identify these hidden populations to policy makers are aware of their unique needs?
Collecting data is an important way that ‘we know what we know’ about homelessness. In addition to point-in-time counts, researchers have also applied mathematical models to better determine where people are located in time across homelessness and housed states (Fisher, Mago, & Latimer, 2020) and used health administrative databases to identify people experiencing homelessness over time (Richard et al., 2019). Likewise, shelter use data can provide valuable information, such as comparisons between usage in different cities (Dutton & Jadidzadeh, 2019) and between populations like single adults, youth, and families (Jadidzadeh & Kneebone, 2018).
According to Echenberg and Munn-Rivard (2020), “Defining and enumerating homelessness is essential in order to understand the nature and extent of the problem, who is affected by it and how to address it” (pg.i). They continue by noting that despite the visibility of homelessness in Canada, it is challenging to count people who lack a permanent address, often remain hidden, and may move in and out of homelessness. Take a moment to read their background paper below, to learn more about the different types of data collection methods used, and how they help us know more about the problem of homelessness in Canada.
Echenberg, H., & Munn-Rivard, L. (2020). Defining and enumerating homelessness in Canada: Background paper. Ottawa, ON: Library of Parliament.
Background Paper: Defining and Enumerating Homelessness in Canada (parl.ca)
As you have just read, there are many different ways we collect data about who is experiencing homelessness. In the next video Dr. Stephen Gaetz expands on this and cautions that while this information is valuable, it only tells us about people who are visibly homeless and in crisis at that moment in time. Listen in as he discusses the limitations of our current data collection approach.
In this video, Dr. Stephen Gaetz explains that much of the data we collect about people experiencing homelessness comes from administrative data, national point-in-time counts, and shelter records. He notes that while we are getting better at collecting data, the information only tells us about people in crisis, such as those who touch the system. Dr. Gaetz explains that our data collection efforts are improving but are still focused on people while in homelessness, and somewhat on exits from homelessness, but are not currently designed to provide information about homelessness prevention. This video is 2:04 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: How do we know what we know about homelessness?
Data collection are important strategies for enumerating the extent of homelessness in Canada and for developing policies thatinform best-practice approaches. Yet, what is most valuable for understanding homelessness in Canada is that we listen to the knowledge of people with lived experience. The importance of authentic lived experience representation has been a central theme throughout the researcher videos, such as in our conversation with Dr. Nick Falvo.
In this video, Dr. Nick Falvo discusses the range of sources of information about homelessness. He notes that it is important to talk to people with lived experience, as much of what we know comes from hearing their stories. Dr. Falvo also notes people who do frontline work at the community level are incredible sources of information. What we know about homelessness also comes from government-coordinated data gathering efforts and researchers located in universities and the community. Dr. Falvo concludes that social media can be an important source of information but that we must be cautious about believing all the information we receive. This video is 2:10 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: How do we know what we know about homelessness?
Today it is common for people with lived experience of homelessness to be paid members of research teams and to inform all aspects of the project’s design, data collection, and analysis. This brief video from United Way Ottawa demonstrates the importance of lived experience driven research.
Developing our understanding of homelessness – how we know what we know – requires strong partnerships between researchers, people with lived experience, policy makers, and the community. Dr. Cheryl Forchuk speaks about the importance of community partnerships in all ofher research projects.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk discusses the importance of relationships with community partners, including people who have lived experience, because addressing homelessness is not something anyone can do alone. She notes that these relationships are essential so people can work together to come up with creative solutions. Dr. Forchuk argues that while community partners may know an issue exists, it is often difficult for them to get policy change unless they can point to data to help increase the political will. This video is 2:44 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Collecting data with community partners
When people who have lived experience of homelessness are asked to speak about the issues impacting their lives, prominent themes include a lack of money, home, privacy, and support, discrimination based on Indigeneity or African descent, living with mental illness and/or addiction, the lived impact of rent, housing, and mortgage policies, and the need for greater awareness of government support systems and services (Ahajumobi & Anderson, 2020).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=556#h5p-30
Listening to people with lived experience is critical to understanding homelessness and generating knowledgethat could be used to inform sound policies. However, while there are active efforts to involve people with lived experience in research, this may not always translate into their voices being included in policy. Benmarhnia et al., (2018) caution that the concept of ‘vulnerability’ is often used in shaping public policies, but the populations who are identified as vulnerable are rarely consulted about whether the term applies to them. Terms like vulnerability, sensitivity, and marginality may be applied indiscriminately (Van den Hoonaard, 2018).In the next video, Dr. Bernie Pauly speaks about how we can move beyond listening to people with lived experience, to having real and authentic engagement.
In this video, Dr. Bernadette [Bernie] Pauly advocates that in whatever role we have, whether practice, policy, or research, it is essential to engage with people who have lived and living experience of homelessness in real and authentic ways. She notes that it is not enough to listen, but that we must believe people when they tell their stories and not be judgemental. Dr. Pauly encourages people in planning and leadership roles to ask themselves how they are engaging with people who have lived experience in a way where they are recognized partners. She concludes that the knowledge they share may be hard to hear, but that we must recognize the system is broken and truly listening is the only way to fix it. This video is 2:45 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: The critical importance of listening to people with lived experience
Zhang and Kteily-Hawa (2018) write that telling one’s story can be an act of agency and advocacy for human rights and personhood. We have heard from many researchers about the importance of listening to people with lived experience. What do you think governments and policy makers can do to move from token engagement to authentic engagement?
In this section, we considered the question, “How do we know what we know about homelessness?” Through a series of videos and readings, we can see that our knowledge comes from many different sources. We have seen how research, point-in-time counts, and administrative data, such as shelter usage and health records, can be used to better understand the scope of homelessness and to inform policy decisions. Along with these sources, you may recall we also saw some of the shortcomings, like the hidden populations that tend to be missed and the increased efforts that are needed to learn about people at risk of homelessness.
We concluded this section by focusing on the critical importance of truly listening to people with lived experience. While they are the experts, they are not always consulted in authentic ways that respect the knowledge they hold. How we know what we know is important to keep in your mind as you move through the book and continue to learn about homelessness from these various sources.
Click the link below to listen to all of the researchers answer the question “How do we know what we know about homelessness?” in audio format on our podcast!
Listen to “How do we know what we know about homelessness?” on Spreaker
6
Canada has gone through three stages to try to reduce homelessness, including an emergency response in the 1990s, an implementation of community plans combined with Housing First initiatives, and more recently is in the beginning stages of moving towards a stronger focus on prevention (Gaetz, 2020). In this section we take a closer look at what homelessness prevention is and why it matters. Before you begin this section, please take a moment to write down your own thoughts about homelessness prevention below.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=558#h5p-31
Homelessness is a trauma that has long-term detrimental effects on the people who experience it. We know from research that the duration of a person’s homelessness can negatively influence their housing outcomes, which is a strong argument for prevention and early intervention that decreases the amount of time a person spends experiencing homelessness (Chen, Cooper, & Rivier, 2021). In these three videos youth homelessness researchers Dr. Naomi Nichols, Dr. Alex Abramovich, and Dr. Kaitlin Schwan speak about the negative impacts of homelessness and how difficult it is to move people out after they become entrenched.
In this video, Dr. Naomi Nichols argues that prevention matters because homelessness erodes people’s well-being and their connections to people and places. She notes that homelessness subjects people to discrimination and stigma, which for youth in particular can have detrimental effects on their physical and mental wellness, as well as their connections to school, work, and other protective institutions. Dr. Nichols further argues that homelessness erodes a person’s sense of safety and while feeling unsafe is not good for anyone, it is particularly problematic for young people to have chronic stress in their bodies at a critical time in their adolescent development. This video is 3:06 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Why does prevention matter?
In this video, Dr. Alex Abramovich explains that we have been talking more about prevention in recent years, but it is still not fully understood. He notes that it can be difficult to support people in successfully exiting homelessness and provides the example of LGBTQ2S+ youth who often have to have something tragic happen before they are provided significant support to exit homelessness. Dr. Abramovich cautions that this is a reactionary response and that if we put more energy and emphasis into prevention, we could help people avoid trauma and instead focus on supporting their long-term health and well-being. This video is 1:51 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Why does homelessness prevention matter?
In this video, Dr. Kaitlin Schwan explains that in Canada, our response to homelessness is emergency-based and that supports are provided on the basis of demonstrating high levels of need. The design of this system is such that people must go through a lot of harm and trauma before the system kicks in to help them. Dr. Schwan provides the example of working with young people who have been unable to access programs until they reached 6 months on the street. She argues that in this time, they can accumulate multiple harms and traumas. Dr. Schwan discusses how homelessness shapes the trajectory of a person’s life and can have lasting inter-generational effects. This is evidenced through the looping effect of involvement in the child welfare system across generations, which particularly impacts racialized and Indigenous communities, making prevention a particularly important equity-based approach. Dr. Schwan concludes that our current emergency response is expensive, and that prevention is the way forward to align with our commitments to human rights in Canada. This video is 4:35 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: Why does homelessness prevention matter?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=558#h5p-32
Our current response to homelessness is a crisis-based one that uses emergency services, like shelters, to help people only once they are on the far end of the homelessness continuum. This model is flawed in many ways, not least of all because of the poor quality of life it creates for service users.
On a systems-level, we can also see that the structure itself is unsustainable. You may have seen news coverage in your own city about shelters reaching capacity and people not having anywhere to go. Research by Jadidzadeh and Kneebone (2018) shows that there is a noticeable increase in shelter users who are experiencing chronic homelessness, which is concerning because it will strain the ability of the shelter system to provide crisis relief and is an indication of a social order in trouble. In this next video, which is brief but succinct, Dr. Jacqueline Kennelly explains that our system has it backwards.
In this video, Dr. Jacqueline Kennelly argues that our system is designed as an emergency crisis response, and that a young person has to be in crisis before they can begin accessing services that allow them to get back into housing. She notes that this is backwards, as the more entrenched a young person becomes in homelessness, the harder it is to get back out. This video is 0:25 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Why does homelessness prevention matter?
If our current system is backwards and only helps people once they are already entrenched in homelessness, what could we do differently? Three researchers who speak in this section, Dr. Erin Dej, Dr. Stephen Gaetz, and Dr. Kaitlin Schwan, have argued that we can learn from countries that have shifted to address the prevention of homelessness, like Australia, Finland, and Wales (Dej, Gaetz, & Schwan, 2020). They have proposed a typology of homelessness prevention that is made up of the five interrelated elements of (i) structural prevention, (ii) systems prevention, (iii) early intervention, (iv) evictions prevention, and (v) housing stabilization.
Building on that typology, through systematically reviewing the literature, Oudshoorn, Dej, Parsons, and Gaetz (2020) add the additional sixth element of empowerment. The ultimate goal of their comprehensive framework is to support communities and governments in more effectively preventing homelessness through upstream approaches that address the root causes (Oudshoorn et al., 2020).
As you begin to learn and think about prevention, it may be useful to consider what our system looks like now, and what it could look like if it focused more on prevention and early intervention. This infographic and video from the Homeless Hub help to illustrate the central concepts.

Shifting towards the prevention of homelessness will require the commitment of public sectors across society. Consider, for instance, the experience of a person who is leaving a jail, hospital, or foster care placement without having somewhere to go. If done well, discharge planning can account for the needs of people as they exit these systems and ensure they receive adequate and appropriate follow-up care. However, as you will see throughout this book, there is often a disconnection between how public systems operate. Many of our public systems do not think about homelessness as being their concern. Dr. Nick Falvo discusses this issue and why prevention matters within this context, in the following video.
In this video, Dr. Nick Falvo identifies prevention as something that has garnered more attention within the past 5 years, in large part due to the work of Professor Stephen Gaetz and the Canadian Observatory on Homelessness. Dr. Falvo explains that it is important to talk about homelessness prevention because when we do, we identify institutions that contribute to the problem and hold them accountable. As an example, Dr. Falvo discusses the corrections system and how inmates are frequently released into homelessness without prior consideration or discussion about their housing status. Additional examples of institutions that discharge into homelessness include hospitals and the child welfare system. Dr. Falvo concludes that talking about prevention forces us to shine a light on institutions that contribute to the problem. This video is 2:35 in length and has closed captions available in English.
Key Takeaways -Dr. Nick Falvo: Why does prevention matter?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=558#h5p-33
The shift towards prevention is markedly different than the current emergency-based system that we are used to. As you learn about this approach, it is useful to keep in mind the question raised by many researchers in this section, about why we make people wait until they are entrenched in homelessness before our system steps in to help them. Dr. Stephen Gaetz has written extensively about our current systems approach and the need to shift towards prevention. In the next video, he shares his thoughts.
In this video, Dr. Stephen Gaetz explains that exposure to homelessness for any length of time has profound and long-lasting effects on physical and mental health and increases the risk of victimization. He notes that by letting people fall into homelessness and not helping them exit immediately, we are contributing to the number and severity of issues they will experience. Dr. Gaetz argues that a “new orthodoxy” has existed for the past 20 years – combining Housing First, community strategies to coordinate efforts, and prioritization of chronically homeless people who have complex mental health and addictions issues. While he notes this bundle of activities is important, he argues that we need to do more to ensure people do not have to wait for housing and supports, because it contradicts Canada’s commitment to the right to housing. Dr. Gaetz notes that people are often reluctant to consider new ways of doing things, but that focusing on prevention would have benefits for individuals, families, and communities. He argues that the problems that create homelessness can be solved if we are willing to think about the issues in a different way, to intervene early, and turn off the inflows. In concluding his response, Dr. Gaetz offers a hypothetical comparison to the COVID-19 outbreak to demonstrate the harm that can be caused if we do not focus on prevention. This video is 6:46 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: Why does homelessness prevention matter?
At this moment we encourage you to pause and read the framework for homelessness prevention developed by Dr. Gaetz and Dr. Dej. It is also noteworthy here that youth homelessness prevention is also critical and has its own framework document (Gaetz, Schwan, Redman, French, & Dej, 2018), which is discussed in depth in the chapter on Child & Youth Studies.
Gaetz, S. & Dej, E. (2017). A new direction: A framework for homelessness prevention [summary]. Toronto: Canadian Observatory on Homelessness Press.
Gaetz and Dej (2017) write that prevention not only makes sense but is standard practice in many areas of society, such as vaccinating to prevent disease or wearing a seatbelt to prevent collision fatalities. Yet, despite its benefits, the impact of prevention can be difficult to measure. How can we prove that someone would have become homeless but did not because of our efforts? This is an issue that Dr. Erin Dej and Dr. John Ecker discuss in the next two videos.
In this video, Dr. Erin Dej explains that prevention matters because it is easier to stop something from happening than to try and fix it afterwards. She argues that prevention makes logical sense and draws parallels in the fields of health care, such as smoking cessation programs to prevent cancer and seatbelts to prevent car accident deaths. Dr. Dej notes that homelessness can be trauma-inducing and we need to think about how to apply the same logic of prevention to intervene before it starts. She concludes that the challenge with prevention is that it is difficult to show something did not happen, and therefore justify it in a budget, but that it is a hurdle we must overcome. This video is 3:18 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: Why does prevention matter?
In this video, Dr. John Ecker argues that if we had stronger homelessness prevention strategies, we would not have the level of homelessness currently seen in Canada. He draws comparisons with Finland and Norway to demonstrate how their stronger social safety nets result in lower levels of homelessness. Dr. Ecker notes that prevention is important because it focuses on the structural and systemic causes of homelessness, such as the need for more affordable housing and increases to income support rates. He identifies institutions, such as hospitals and jails, as having a key role and responsibility to prevent discharge into homelessness, which could be accomplished through legislation. Dr. Ecker notes that prevention allows us to identify risk and address it earlier, through a focus on structures and policies. He concludes that, while prevention efforts are sometimes critiqued for not having measurable outcomes, it is important to remember that what we do now will have an impact on future levels of homelessness. This video is 4:18 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Why does homelessness prevention matter?
One hurdle that researchers have identified with prevention is that it is difficult to measure something that does not happen, which makes it challenging to advocate for funding. If your job was to get funding for homelessness prevention efforts, what would you say to make this argument?
One argument that can be made, is that ending people’s homelessness costs far less than our current emergency-based response. Consider this video discussion with Dr. Tim Aubry and the infographic that follows from the Canadian Observatory on Homelessness.
In this video, Dr. Tim Aubry argues that we are coming to a greater realization that we need to not only address homelessness but also think more broadly about prevention. He explains that homelessness is an awful experience and if we can prevent it, we will save people from going through trauma and a life crisis. Dr. Aubry concludes that from a service and policy standpoint, it is cost-effective and logical to prevent people from having to navigate the complicated system of emergency and crisis supports needed to get back into housing after homelessness has occurred. This video is 2:08 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: Why does homelessness prevention matter?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=558#h5p-34
At this point you may be thinking to yourself, “Okay, prevention sounds good and would save money, but let’s get real. We can never stop every person from becoming homeless!” If you are thinking this, you are absolutely right. Discussions around prevention always raise the concern that homelessness can never be completely avoided in every circumstance.
It may be useful to consider a parallel example of defining an end to homelessness. Turner, Albanese, and Pakeman (2017) explain that in a “functional zero” end to homelessness the goal is to achieve a point where there are enough services and supports to rapidly rehouse people and move them out of the homelessness system. In much the same way, while we may not be able to prevent every person from becoming homeless, we can prevent instances where possible and intervene early where prevention is not possible.
What we need in order to achieve a system where people are prevented from becoming homeless, or moved quickly back into housing, is a change in our thinking. We conclude this section with the optimistic words of Dr. Jeannette Waegemakers Schiff, as she shares her ideas for redesigning society for the collective good.
In this video, Dr. Jeannette Waegemakers Schiff argues that homelessness is first and foremost an issue of not having housing and that we can cut problems in half by keeping people housed. She notes that we are going to continue to perpetuate homelessness until we have government support at a federal and provincial level that provides an adequate supply of social housing. Dr. Waegemakers Schiff shares her wishful thinking ideal system, which includes systemic case management that provides instrumental support for people who are living precarious lives and may be experiencing one or more disabling condition. She concludes that we need to offer people more support, which is a larger political issue of governments recognizing that action needs to be taken for the common good. This video is 2:45 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: Redesigning society for the collective good
In this section we asked you to consider the question, “Why does homelessness prevention matter?” Along the way, the answer to this question became another question in itself – why would we keep a system that makes people experience the trauma of homelessness before it steps in to help them? Homelessness is a horrible experience, yet our system is designed to help people only once they have lost all other supports. As we heard argued, this system is backwards. We have seen throughout this section that a framework for prevention makes sense, as the right thing to do for people and as a way to address homelessness more cost-effectively. Two challenges of prevention are that it requires commitment from various public sectors and that its outcomes are difficult to measure. What we need is a collective repositioning of the way we think, to understand the value of homelessness prevention in the same way we think about seatbelts and vaccines.
Click the link below to listen to all of the researchers answer the question “Why does homelessness prevention matter?” in audio format on our podcast!
7
People do not choose to be homeless. There is invariably an event (or a series of events) that the individual experiences that lead to a loss of housing. This event then leads to the individual being homeless which involves situations that are unpleasant, unhealthy, and unsafe. This trajectory occurs beyond the control of the individual and can be very distressing. Homelessness is a very complex issue and different for each individual.
There are four foundational concepts that we will be visiting and revisiting throughout this book. They are critical to understanding the complexity of homelessness in Canada. These include:
 Person-centred care is not just about giving people whatever they want or just providing information. It is about considering people’s desires, values, family situations, social circumstances, and lifestyles. Also, it is about interacting with the person as an individual and working together to develop appropriate solutions with them. It involves being compassionate, thinking about things from the person’s point of view, and being respectful of the person’s wishes and choice.
Person-centred care is not just about giving people whatever they want or just providing information. It is about considering people’s desires, values, family situations, social circumstances, and lifestyles. Also, it is about interacting with the person as an individual and working together to develop appropriate solutions with them. It involves being compassionate, thinking about things from the person’s point of view, and being respectful of the person’s wishes and choice.
 There are many factors that influence health and well-being. Historically, we have focused on the physical factors such as age, sex, genetics, and various lifestyle or behavioural factors. In order to truly understand health and well-being we need to broaden this lens to include the social and economic factors that influence health. The social determinants of health (SDOH) are related to an individual’s place in society (income, education, employment) and to an individual’s experiences of discrimination, racism, and historical trauma.
There are many factors that influence health and well-being. Historically, we have focused on the physical factors such as age, sex, genetics, and various lifestyle or behavioural factors. In order to truly understand health and well-being we need to broaden this lens to include the social and economic factors that influence health. The social determinants of health (SDOH) are related to an individual’s place in society (income, education, employment) and to an individual’s experiences of discrimination, racism, and historical trauma.
The main social determinants of health include:
(Raphael, 2016)
 This is an approach in the human service field that assumes that an individual is more likely than not to have a history of trauma and recognizes that symptoms of trauma play a role in an individual’s life. The intention of Trauma-Informed Care is not to treat symptoms or issues related to sexual, physical or emotional abuse or any other form of trauma but rather to provide support services in a way that is accessible and appropriate to those who may have experienced trauma.
This is an approach in the human service field that assumes that an individual is more likely than not to have a history of trauma and recognizes that symptoms of trauma play a role in an individual’s life. The intention of Trauma-Informed Care is not to treat symptoms or issues related to sexual, physical or emotional abuse or any other form of trauma but rather to provide support services in a way that is accessible and appropriate to those who may have experienced trauma.
 This concept involves understanding the way in which individuals are made part of structured social relationships and groups. It is a process where all individuals have the opportunity to engage in various social, economic, and political systems. Research has shown that a feeling of belonging to a community and social inclusion are central to mental health. Belonging to a network of supportive relationships is protective of good health and positive wellbeing.
This concept involves understanding the way in which individuals are made part of structured social relationships and groups. It is a process where all individuals have the opportunity to engage in various social, economic, and political systems. Research has shown that a feeling of belonging to a community and social inclusion are central to mental health. Belonging to a network of supportive relationships is protective of good health and positive wellbeing.
8
John
We first met John at the beginning of the chapter. John’s circumstances may have matched with your initial thoughts about: what is homelessness? If you review the Canadian Definition of Homelessness, you will note that his circumstances reflect ‘unsheltered’ homelessness (Gaetz et al., 2012, p. 1). Unsheltered includes people who are absolutely homeless, those living on the street, or in a place that is not intended for human habitation. John has been living between buildings and alleyways in a large urban area, sleeping rough during the day and wandering at night to avoid being hassled by police. If we were to conduct a Point-in-Time count in this area, we would most likely add John to our numbers. This is only the beginning of John’s story.
To fully understand John and his situation we need to look beyond the surface to understand this person experiencing homelessness.
We need to ask ourselves:
Tasha and Raoul
Like John, we were introduced to Tasha and Raoul earlier in the chapter. Tasha and Raoul had been living in an old trailer in a rural area. This young couple, according to the Canadian Definition of Homelessness would be considered ‘provisionally housed” (Gaetz et al., 2012, p.3). They are technically homeless without permanent shelter. Think about the country in which we live. As winter comes in this living arrangement will not be sustainable with no running water or electricity. This is a time limited, precarious situation. People who live in rural areas are often considered the ‘hidden homeless”.’ If we were to conduct a Point-in-Time count in the closest community chances are that Tasha and Raoul would be overlooked. They are far from services such as health care, financial aide, and legal support. This is not their home community.
We need to ask ourselves:
9
We began this introductory chapter by inviting you to join in a dialogue about homelessness in Canada. Whether this was the first time you have considered homelessness in a critical way or whether you have experience of homelessness directly or indirectly, through work or volunteering, we hope that you found this chapter informative and engaging.
At the start of the chapter, we introduced you to the composite characters John, Tasha, and Raoul, who were each experiencing homelessness in their own unique way. The scenarios were presented as an entry point into thinking about the complexity of homelessness. We returned to these individuals’ stories again at the end to demonstrate how they can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “What is homelessness?” Here we learned that homelessness is not an unusual state but rather something that happens to human beings. We were reminded to always begin our thinking with the understanding that first and foremost, we are talking about people with human rights. We explored the different types of homelessness, the reasons it occurs, and the Canadian definition of homelessness, which includes people who are at-risk.
Next we asked, “How do we know what we know about homelessness?” This led us to answers about the importance of research, evaluation, and collecting data in ways such as through shelter usage, health administration records, and point-in-time counts. Each of these methods provides information on the scope of homelessness in Canada. In this section we also discussed the critical importance of listening to people with lived experience, in a way that authentically recognizes and respects their contribution of knowledge.
Finally we asked, “Why does homelessness prevention matter?” In this final section, we looked at how we could reorganize our homelessness responses better by shifting towards prevention. We heard that homelessness is a traumatizing experience that has long-lasting negative impacts, and that the longer a person remains unhoused, the harder it is to move back out of homelessness. Many of the researchers questioned why we keep a system that makes people go through trauma before it steps in to help them. Instead, a framework for the prevention of homelessness was proposed as a new way of thinking and acting across public sectors. Despite the challenge of being difficult to measure, prevention was lauded as a new way forward for the good of individuals and society as a whole.
This introductory chapter is an important first step into understanding homelessness in Canada and we thank you for joining us along the way. We look forward to seeing you again soon, as we continue to explore a new set of seemingly simple questions with complex answers in the chapters that follow.
10
Here are some additional resources you may want to check out!
11
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
12
Ahajumobi, E. N., & Anderson, P. B. (2020). Homeless Canadians’ perspectives on homelessness in Calgary. Journal of Social, Behavioral and Health Sciences, 14(1). https://doi.org/10.5590/JSBHS.2020.14.1.08
Benmarhnia, T., Alexander, S., Price, K., Smargiassi, A., King, N., & Kaufman, J. S. (2018). The heterogeneity of vulnerability in public health: a heat wave action plan as a case study. Critical Public Health, 28(5), 619–625. https://doi.org/10.1080/09581596.2017.1322176
Chen, X., Cooper, I., & Rivier, J. (2021). Homelessness prevention and determinants of housing among first-time and recurrent emergency shelter users in Canada. Housing Studies, 1–17. https://doi.org/10.1080/02673037.2020.1865520
Dej, E., Gaetz, S., & Schwan, K. (2020). Turning off the tap: A typology for homelessness prevention. The Journal of Primary Prevention, 41(5), 397–412. https://doi.org/10.1007/s10935-020-00607-y
Dutton, D. J., & Jadidzadeh, A. (2019). The incidence of homelessness in Canada is a population-level phenomenon: A comparison of Toronto and Calgary shelter use over time. Canadian Studies in Population, 46(2), 161–171. https://doi.org/10.1007/s42650-019-00013-8
Echenberg, H., & Munn-Rivard, L. (2020). Defining and enumerating homelessness in Canada: Background paper. Ottawa, ON: Library of Parliament.
Fisher, A., Mago, V., & Latimer, E. (2020). Simulating the evolution of homeless populations in Canada using modified deep q-learning (MDQL) and modified neural fitted q-iteration (MNFQ) algorithms. IEEE Access, 8, 92954–92968. https://doi.org/10.1109/ACCESS.2020.2994519
Gaetz, S., Barr, C., Friesen, A., Harris, B., Hill, C., Kovacs-Burns, K., Pauly, B., Pearce, B., Turner, A., & Marsolais, A. (2012) Canadian definition of homelessness. Toronto: Canadian Observatory on Homelessness Press.
Gaetz, S. (2020). Making the prevention of homelessness a priority: The role of social innovation. The American Journal of Economics and Sociology, 79(2), 353–381. https://doi.org/10.1111/ajes.12328
Gaetz, S. & Dej, E. (2017). A new direction: A framework for homelessness prevention. Toronto: Canadian Observatory on Homelessness Press.
Gaetz, S., Schwan, K., Redman, M., French, D., & Dej, E. (2018). The roadmap for the prevention of youth homelessness – executive summary. A. Buchnea (Ed.). Toronto, ON: Canadian Observatory on Homelessness Press.
Jadidzadeh, A., & Kneebone, R. (2018). Patterns and intensity of use of homeless shelters in Toronto. Canadian Public Policy, 44(4), 342–355. https://doi.org/10.3138/cpp.2018-013
O’Reilly-Fleming, T. (1993). Down and out in Canada: Homeless Canadians. Toronto: Canadian Scholar’s Press.
Oudshoorn, A., Dej, E., Parsons, C., & Gaetz, S. (2020). Evolving an evidence‐based model for homelessness prevention. Health & Social Care in the Community, 28(5), 1754–1763. https://doi.org/10.1111/hsc.13000
Raphael, D. (2016). Social determinants of health: A Canadian perspective, 2nd Edition. Toronto: Canadian Scholar’s Press.
Richard, L., Hwang, S. W., Forchuk, C., Nisenbaum, R., Clemens, K., Wiens, K., … Shariff, S. Z. (2019). Validation study of health administrative data algorithms to identify individuals experiencing homelessness and estimate population prevalence of homelessness in Ontario, Canada. BMJ Open, 9(10), e030221–e030221. https://doi.org/10.1136/bmjopen-2019-030221
Rotondi, M. A., O’Campo, P., O’Brien, K., Firestone, M., Wolfe, S. H., Bourgeois, C., & Smylie, J. K. (2017). Our health counts Toronto: Using respondent-driven sampling to unmask census undercounts of an urban Indigenous population in Toronto, Canada. BMJ Open, 7(12), e018936–e018936. https://doi.org/10.1136/bmjopen-2017-018936
Thistle, J. (2017). Indigenous definition of homelessness in Canada. Toronto: Canadian Observatory on Homelessness Press.
Trent University Homelessness Research Collective. (2019). “A good day is waking up inside.” Conversations about homelessness, housing vulnerability, and health care across the City of Kawartha Lakes and Haliburton County. ON: Trent University HRC.
Turner, A., Albanese, T., & Pakeman, K. (2017). Discerning “functional and absolute zero:” Defining and measuring an end to homelessness in Canada. The School of Public Policy Publications (SPPP), 10(2), 1–43. https://doi.org/10.11575/sppp.v10i0.42616
Van den Hoonaard, W. (2018). The vulnerability of vulnerability: Why social science researchers should abandon the doctrine of vulnerability. In the Sage Handbook of Qualitative Research Ethics (pp. 305-321). SAFE Publications Ltd.
Zhang, P., & Kteily-Hawa, R. (2018). Poetry, prose, and personhood: The art of storytelling with the homeless. Canadian Journal for the Study of Adult Education, 30(2), 69-79.
II

Indigenous and Canadian Studies are independent, yet related, fields that examine the experiences of Indigenous persons and settlers within our nation. Within this part of the book, we examine historical and contemporary decisions that have been put in place through policy, and the long-term impacts and repercussions of these choices. We begin with a chapter on Indigenous Studies, followed by a chapter on Politics, Policy, and Housing in Canada. As you work through these chapters, you are encouraged to critically reflect upon what these disciplines contribute to our knowledge and understanding of homelessness in Canada.
Perhaps as you read this, you are considering a career that relates to Indigenous and Canadian Studies, such as an Indigenous Youth Worker, Housing Policy Maker, or Politician. The chapters in this section are designed to help you think critically about some of the questions you may encounter in these fields of employment. Understanding homelessness will help you navigate situations and choices you have to make. Consider, for example, a scenario in which a young Indigenous man leaves his family, community, and home on a northern reserve to seek employment in a large urban centre. When he arrives, he is unable to find work and housing is more expensive than he can afford. He is unable to pay for a return bus ticket and is alone in the city. As an Indigenous Youth Worker, this young man may seek you out for tangible assistance, like securing a room at a shelter, as well as for emotional and social support. Would it be better to help this young man return and reconnect with his family in the north, or help him try to find whatever work and housing he can within the city? As a Housing Policy Maker or Politician, the choices you make will trickle down to the availability of housing and supports within the community. How much affordable housing is enough, and what does affordable even mean anyway?
Before you begin, pause to consider how you would respond in each of the roles of the scenario above. With the knowledge you currently have about homelessness in Canada, why do you think it is important to consider Indigenous Studies and Canadian Studies as separate but related chapters? In the scenario, whose responsibility is it to ensure this young man has access to employment and affordable housing, whether he resides on a northern reserve or remains off-reserve in the city?
You are encouraged to keep this scenario in your mind as you read through the next two chapters and ask yourself whether any of your responses change, or are reaffirmed, after learning more about what Indigenous and Canadian Studies can teach us about homelessness in Canada.
II
It is important in opening this chapter to note that none of the team members who created this book identify as having Indigenous ancestry. This raises an issue of concern – you cannot have a course on homelessness without addressing the reality of Indigenous homelessness in Canada, yet none of us are personally qualified to write from the perspective of someone who has firsthand Indigenous knowledge. In attempting to address this, we have reached out to a number of Indigenous scholars to participate in videos. We are deeply appreciative to the Indigenous scholars who agreed to speak with us and to the non-Indigenous scholars who spoke about research they have conducted in partnership with Indigenous communities.
As you work through this chapter, you may notice that there is less written text and more video and multi-media content. This approach is strategic, in order to bring as many Indigenous voices and perspectives into the conversation as possible. Writing this chapter has been a learning journey for us as well. It is our hope that you will engage with the material as deeply and as thoughtfully as we have, in putting it together. We are eager to learn from the voices of Indigenous persons, even if that learning means taking a difficult look at our governments, our communities, and even ourselves. Please join us.
13
In this chapter, you are invited to learn about the different meanings and experiences of homelessness within Indigenous communities, and the deep roots of colonialism upon which they have been built. While tracing these roots and their modern-day implications, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that homelessness has different meanings and root causes for Indigenous communities. This chapter provides an opportunity to learn new ideas about the meaning of home and the damage that is caused when it is taken away. Read on to learn more about Indigenous homelessness in Canada.
14
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to Indigenous Studies. As you work through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After considering the real-world scenario, we will endeavour to answer each question posed in the learning objectives. Is Indigenous homelessness defined differently than settler homelessness? How are the causes of Indigenous homelessness rooted in on-going colonizing practices? How can we begin to decolonize society and decrease Indigenous homelessness? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
15
As you learn about Indigenous homelessness and the complex ways in which it is experienced, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider this person’s experience.
Joseph
Joseph is a 64-year-old Cree male who is a sixties scoop survivor. He was taken from his family in Saskatchewan and adopted by a white family in the United States at the age of 6. He has some memories of his birth family, but they are incomplete and have haunted him for years. He has felt he never fit in with his adoptive family, always feeling apart. When he was 50 years old, he began a search for his birth family. This led him to his on-Reserve family in Saskatchewan. Joseph spent time in the community but did not feel accepted. Again, he felt like an outsider. Years of pain and social isolation have led to substance use issues and eventually homelessness. He now lives rough in the woods just outside a medium-sized city. He hitchhikes into town for food. He has begun to feel a sense of community with the folks he knows on the street in the nearby town, which has led to a small decrease in his social isolation.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to the scenario again at the end of the chapter.
Reflection Questions
16
“Indigenous” is a broad term used to reflect the three distinct cultural groups of status and non-status First Nations, Métis, and Inuit peoples. We use this term throughout this section, and throughout this book, to refer to these diverse cultures and peoples, with the recognition that there are many similarities and also many differences in their experiences. Within the context of this chapter, we are focusing more on the similarities that arise around homelessness. We begin with the question of how Indigenous homelessness is defined. Do people who are Indigenous experience homelessness in the same way and for the same reasons as settler-colonials (i.e. non-Indigenous people) do? If you think they do not, what are the differences? Before you continue through the material of this chapter, we encourage you to take a moment and record your thoughts below.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=599#h5p-56
The Federal Government of Canada collects data on the nation’s population through the Canadian census. In 2016, the census showed there were an estimated 1,673,780 Indigenous people living in private households in Canada and 339,595 Indigenous people living on-Reserve (Statistics Canada, 2020). These figures are likely underestimates (Rotondi et al., 2017) but do indicate a sizable Indigenous population exists in Canada.
The research shows a troubling picture about the relationship between being Indigenous and experiencing homelessness, both visible and hidden (Alberton, Angell, Gorey, & Grenier, 2020). For instance, Indigenous people in Canada have a life expectancy that is 12 years lower than the national average because of health inequities (Kolahdooz, Nader, Yi, & Sharma, 2015) and there are disproportionately high rates of institutionalization particularly amongst Indigenous men (Feir & Akee, 2018). In Canada, Indigenous people are also 8 times more likely than non-Indigenous people to experience homelessness and represent up to 80% of the total population experiencing homelessness in large urban centres (Thistle & Smylie, 2020). Indigenous youth are over-represented amongst people experiencing homelessness (Dunn, 2019) and being Indigenous is significantly associated with being homeless at an earlier age, having a lifetime duration of homelessness longer than 3 years, and having post-traumatic stress disorder, alcohol dependence, substance use issues, and infectious disease (Bingham, 2019a).
Homelessness is clearly a pressing issue that impacts Indigenous peoples and communities in a disproportionate way. The next logical question would then be, “Why does homelessness disproportionately impact Indigenous peoples?” This question is a thread that runs throughout the chapter, but before we can even begin to answer it we must first start with cultural reflexivity. Measures that are designed to address homelessness amongst Indigenous people are bound to fail if they do not reflect Indigenous ways of knowing and being in the world (Cunningham, 2019). To be home-less is to be less (or without) a home. Therefore, before we can talk about homelessness, we must first consider the concept of what home means within an Indigenous worldview. In the first video, Jessica Rumboldt, Post-Doctoral Fellow in Indigenous Homelessness with the Canadian Observatory on Homelessness speaks about the meaning of home and the significance of homemaking practices.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Jessica Rumboldt discusses why it is critical to think about how concepts of home and homelessness are portrayed, perceived, and experienced in distinct ways for Indigenous persons. She explains that home and homelessness are contemporary concepts, and that the loss of social housing in the 1980s and 1990s pushed a significant number of people onto the streets, with many identifying as Indigenous. Rumboldt cites the work of several Indigenous scholars to explain the different meanings and definitions of home in western and Indigenous communities, but she is also clear to note that there are differences between Indigenous groups as well. She concludes by discussing Indigenous homemaking practices as foundational and notes that pathways to homelessness are exasperated when housing policies do not align with or reflect Indigenous homemaking practices. This video is 5:39 in length and has closed captions available in English.
Key Takeaways – Jessica Rumboldt: Is Indigenous homelessness defined differently than settler homelessness?
Home and homemaking are central concepts within an Indigenous worldview, and we cannot even begin to understand the high rates of homelessness within Indigenous communities without them. According to Bowra and Mashford-Pringle (2021) Indigenous conceptualizations of home extend beyond physical and social environments to include relationships that connect a person to all that surrounds them such as people, plants, animals, insects, and land as well as ancestors, stories, language, songs, and traditions. They further note that home has physical, emotional, mental, and spiritual attachments, and that homemaking practices have direct and significant implications for the health and well–being of Indigenous peoples (Bowra & Mashford-Pringle, 2021). In the next video rural homelessness researcher, Dr. Jeannette Waegemakers Schiff, speaks more about the meanings of home within Indigenous cultures.
In this video, Dr. Jeannette Waegemakers Schiff shares a memory of an Indigenous student who told her that within her culture home is more about a feeling of belonging and being connected than it is about being attached to a particular dwelling place. Dr. Waegemakers Schiff states that outside Indigenous communities there is less understanding and awareness of home as belonging to the land. For this reason, she argues, home and belonging need to be defined by Indigenous peoples by and for themselves. This video is 1:13 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: Is Indigenous homelessness defined differently than settler homelessness?
Dr. Waegemakers Schiff raises the critical points that Indigenous conceptualizations of home – and by extension homelessness – must be defined by Indigenous persons and that people who are not Indigenous lack the cultural and spiritual awareness to truly understand. We, as authors, were humbly reminded of this in relation to how we posed the question. We asked, “Is Indigenous homelessness defined differently than settler homelessness?” rather than simply, “How is Indigenous homelessness defined?” We acknowledge here our mistake of setting up Indigenous homelessness in relation to settler-colonial homelessness. You will notice that we have used this question in its original form, as it was the question we posed to the researchers we spoke to. It is our hope that as you read this section, and encounter the question, it will spark a reminder that Indigenous homelessness must not be framed in relation to settler homelessness but rather be considered as its own unique cultural experience. We discuss this further with Dr. Rebecca Schiff, who works closely with rural and Indigenous communities in northern Ontario.
In this video Dr. Rebecca Schiff questions why Indigenous homelessness would be defined in relation to settler homelessness, noting that this dichotomy creates discourses that are not productive in moving towards reconciliation. In considering how Indigenous peoples might experience homelessness in ways that are unique, she identifies a range of issues related to colonial structures, histories of colonialism, and intergenerational trauma. Dr. Schiff concludes by explaining that Indigenous homelessness is not about having a roof but rather about a relationship with the land. This video is 4:31 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: Is Indigenous homelessness defined differently than settler homelessness?
As we have seen, Indigenous homelessness is a unique experience that is situated within Indigenous conceptualizations of home and homemaking practices. In the next video, Jessica Rumboldt explains that while we can consider the typology of homelessness that was reviewed in the Introductionchapter, taking an Indigenous worldview helps to show how Indigenous homelessness is defined in much broader ways.
In this video, Jessica Rumboldt reviews the definition of homelessness produced by the Canadian Observatory on Homelessness, including the typology that ranges from being unsheltered, emergency sheltered, provisionally accommodated, and at-risk of homelessness. She notes that it is important to recognize there is no one set experience that people have, but rather a range of experiences. Taking an Indigenous worldview helps us to see how Indigenous homelessness may be understood differently. Rumboldt notes that individuals, families, and communities who are separated from land, water, location, family, kin, social networks, language, and culture can be recognized as experiencing homelessness. On a cultural, spiritual, emotional, and physical level, Indigenous people facing various forms of homelessness are unable to reconnect with their Indigeneity and lost relationships. This video is 3:18 in length and has closed captions available in English.
Key Takeaways – Jessica Rumboldt: Considering Indigenous and settler definitions of homelessness
Indigenous health scholar Dr. Suzanne Stewart (2018) has written, “What does being homeless mean? An academic definition would describe homelessness as the condition of not being housed or having a fixed address. But in an Indigenous context, defining homelessness requires a more holistic view. Homelessness for many Indigenous people may not simply mean lacking physical housing; it may also include feeling spiritually and culturally bereft” (pg.98). Just as Jessica Rumboldt explained in the previous video, Patrick (2014) reminds us that “It is important to remember that within any overarching historical narrative are unique experiences, understandings and memories” (pg.10). The experience of homelessness has both differences and similarities within Indigenous cultures and communities, which is important to remember when seeking to define homelessness within an Indigenous context.
When we posed the question of how to define Indigenous homelessness, many of the researchers we spoke to, referenced the work of scholar Jesse Thistle (2019), who is the author of “From the ashes: My story of being Métis, homeless and finding my way.” In 2017 Thistle released the Indigenous Definition of Homelessness in Canada, which outlined 12 unique dimensions. The introductory video presented below was made just prior to the release of the definition and shows Jesse Thistle speaking about its forthcoming publication.
The Indigenous Definition of Homelessness in Canada, produced by Thistle in consultation with Indigenous communities, has become a widely influential and highly regarded document. Thistle (2017) begins by discussing home and homelessness in an Indigenous context, situated within historical practices. He then discusses the 12 dimensions of Indigenous homelessness in Canada, which include: [1] historic displacement, [2] contemporary geographic separation, [3] spiritual disconnection, [4] mental disruption and imbalances, [5] cultural disintegration and loss, [6] overcrowding, [7] relocation and mobility, [8] going home, [9] nowhere to go, [10] escaping or evading harm, [11] emergency crisis, and [12] climatic refugee homelessness. The graphic summary below provides an overview of these 12 dimensions.
Click the image below to open a new window and view the full infographic, “The 12 Dimensions of Indigenous Homelessness” by the Homeless Hub. (NOTE: The infographic will appear too small to read when it first opens. Please click on it to zoom in and scroll up/down to view the full infographic).
 The Indigenous Definition of Homelessness in Canada has helped to create a more culturally appropriate guide for defining and understanding homelessness through an Indigenous worldview. This definition was raised by many of the researchers we spoke to. In the next set of videos, Dr. Erin Dej, Dr. John Ecker, and Dr. Abe Oudshoorn each situate this document as being central for learning about Indigenous homelessness.
The Indigenous Definition of Homelessness in Canada has helped to create a more culturally appropriate guide for defining and understanding homelessness through an Indigenous worldview. This definition was raised by many of the researchers we spoke to. In the next set of videos, Dr. Erin Dej, Dr. John Ecker, and Dr. Abe Oudshoorn each situate this document as being central for learning about Indigenous homelessness.
In this video, Dr. Erin Dej notes that there is an Indigenous definition of homelessness in Canada that discusses 12 dimensions, as they relate to the loss of all my relations, such as through disconnection from land, language, culture, and kin. Dr. Dej explains that the Indigenous definition is not about whether a person has a roof over their head, but rather offers a more holistic understanding of what not having a home means. This video is 0:57 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: The Indigenous definition of homelessness
In this video, Dr. John Ecker credits Jesse Thistle for producing an Indigenous definition of homelessness, through deep consultations with Indigenous peoples across Canada. He notes that the definition extends beyond the loss of housing to focus on spiritual, familial, cultural, and emotional elements. Dr. Ecker argues this definition helps to move our thinking beyond traditional westernized understandings of homelessness, towards a more holistic way of thinking. This video is 0:50 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Is Indigenous Homelessness defined differently than settler homelessness?
In this video, Dr. Abe Oudshoorn argues that Indigenous homelessness is defined differently, in a formal way, and that this is important because the causes and subsequent responses are particular in working with Indigenous peoples. He notes that having a distinct definition helps provide a theoretical foundation for understanding why Indigenous homelessness occurs and what can be done about it. This video is 1:03 in length and has closed captions available in English.
Key Takeaways –Dr. Abe Oudshoorn: Is Indigenous homelessness defined differently than settler homelessness?
At this point, we invite you to pause and review the Indigenous Definition of Homelessness in Canada in full, as this section’s featured reading.
Thistle, J. (2017.) Indigenous Definition of Homelessness in Canada. Toronto: Canadian Observatory on Homelessness Press
In this document, Thistle (2017) writes that Canadians must finally agree on some difficult truths. First, that Indigenous people do not choose to be homeless. Second, the experience is negative, stressful, and traumatic. Third, homelessness itself forces a disproportionate number of Indigenous people into activities that are deemed criminal by the state. Fourth, the higher mortality rates of Indigenous people have been ignored for too long. Finally, and Thistle (2017) notes most importantly, “because a lack of home, much as a sense of place or homeplace, is a culturally understood experience, we must develop and recognize an Indigenous definition of homelessness that must inform policy-making to solve the tragedy of Indigenous homelessness” (pg. 8).
The Indigenous definition was created by and for Indigenous peoples. We note here that while resisting the referent of settler homelessness, having an Indigenous definition has been influential in helping non-Indigenous people to better understand an Indigenous worldview. This arose in our discussions with Dr. Nick Falvo as he explains how the definition has been influential in helping him frame his understandings of Indigenous homelessness.
In this video, Dr. Nick Falvo discusses Jesse Thistle’s definition of Indigenous homelessness as a useful resource for helping us to frame our understandings. He notes that the history of Indigenous peoples in Canada has involved government efforts to force assimilation, creation of the Reserves system, reducing rights for Indigenous peoples, taking away ceremony, enforcing residential schooling, and ongoing intergenerational trauma. Dr. Falvo concludes this history has a profound impact on Indigenous peoples’ experiences of homelessness, and that it is important to understand and be sensitive to these historical differences. This video is 1:30 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: Is Indigenous homelessness defined differently than settler homelessness?
We have seen that Indigenous experiences of homelessness are rooted in historical understandings of home, homemaking practices, and all my relations. Without comparing Indigenous to settler homelessness, we must remain aware that settler-colonial practices are the cause of Indigenous homelessness. Colonization and displacement from land, culture, language, and identity are at the root of why Indigenous homelessness occurs. According to Greenwood and Lindsay (2019), “Indigenous knowledge and Indigenous health are both deeply rooted in the land – nurturing and protecting both requires nurturing and protecting the land” (pg.84). As this suggests, Indigenous understandings of health and wellness are not located in biological factors but rather intimately tied to community, land, culture, and family – all of which have been disrupted by colonizing practices (de Leeuw, S., Greenwood, M., & Farrales, 2021). Rural homelessness researcher Dr. Bill O’Grady discusses the historical context as well as how we see its effects in modern day, such as through the disproportionate impact of climate change on Indigenous communities.
In this video, Dr. William [Bill] O’Grady draws on the work of Indigenous scholars from recent years and explains that Indigenous homelessness is different because it is not defined simply as lacking a structure for habitation, but rather is understood more broadly. He identifies the role of historic displacement as a starting point in understanding how Indigenous peoples have been removed from their lands. Dr. O’Grady notes that multiple interrelated factors are important to consider, including colonial control, spiritual disconnection, and cultural disintegration and loss. He explains that some Indigenous peoples migrate to urban areas but are not well-served by the non-Indigenous housing and programs available, and that if they return to their community after a period of time they may be thought of as an outsider. Dr. O’Grady draws our attention to the risk of intimate partner violence as a cause of homelessness in general that also impacts Indigenous communities. He concludes by discussing the ways climate change has had a particularly negative effect on many Indigenous peoples’ livelihoods and cultural practices. This video is 4:36 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: Is Indigenous homelessness defined differently than settler homelessness?
Climate change is having a disproportionately negative impact on northern Indigenous communities. Have you previously considered the impact of climate change on Indigenous communities? What impact do you think climate change is having on northern Indigenous communities’ long-term prospects for livelihoods and housing security?
We encourage you to consider these questions as you watch this documentary (24:11) on the effects of climate change, which was created by the Cree Nation of Mistissini.
A team of researchers reviewed the literature on impacts of climate change and found that people experiencing homelessness are disproportionately exposed to climatic events, their physical and mental health is likely to be negatively impacted, and that implementing structural changes like green infrastructure might help offset some of these outcomes (Bezgrebelna et al., 2021). There are clear health and social implications related to climate change that negatively impact housing security for marginalized individuals (Kidd, Greco, & McKenzie, 2021). Dr. Sean Kidd has been part of this research, analyzing the impact of climate change. In the next video he speaks about the impact for northern Indigenous communities.
In this video, Dr. Sean Kidd directs us towards the definition of Indigenous homelessness developed by Jesse Thistle in consultation with Indigenous communities. Dr. Kidd argues that the terms house and home are not synonymous but that we are not always great at unpacking the differences between these terms. For many Indigenous peoples, the concept of home is deeply connected to land. Dr. Kidd notes that by reviewing the work of Indigenous scholars we can see how for First Nations, Métis, and Inuit communities, the ideas of home and homelessness are deeply rooted in a diverse range of histories and cultures. There is a historical lens to Indigenous understandings of homelessness based in colonization, genocidal violence, and the atrocities that stretch back in time in terms of what has been taken away. Dr. Kidd concludes by drawing our attention to climate change as a current form of land displacement, disproportionately impacting Inuit and far north communities, where people are losing their homes and livelihoods because of pollution they did not create. This video is 5:50 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: Is Indigenous homelessness defined differently than settler homelessness?
Indigenous homelessness is defined and experienced in many different ways. A theme that emerges throughout this book is that there is no one size fits all approach for understanding homelessness. This is true of Indigenous homelessness as well. We need guiding definitions and understandings, but it is also critical to remember that people and communities will be impacted by homelessness in their own unique ways. We conclude this section with a reminder of this message that emerged in our conversations with Indigenous homelessness scholar, Jessica Rumboldt.
In this video, Jessica Rumboldt cites the work of Jesse Thistle and other Indigenous scholars to define Indigenous understandings of homelessness. She notes that answering this question and forming a definition requires engagement with different voices and experiences, and that there is no one size fits all approach. Rumboldt argues that to address the question of whether homelessness is defined differently, we must acknowledge the understandings of what home looks like, what it means, and how the perception of home impacts the state of homelessness. She concludes that we must engage with Indigenous communities to better understand the unique ways homelessness is defined and experienced. This video is 1:30 in length and has closed captions available in English.
Key Takeaways – Jessica Rumboldt: Diverse understandings of Indigenous homelessness
In this section, we set out to learn how Indigenous homelessness is defined. We found that while Indigenous homelessness is rooted in colonial practices it is harmful to frame it in relation to settler homelessness. Instead, we have found that an Indigenous worldview begins with understanding home and homemaking practices as being situated within all my relations. This entails broader perspectives that connect people to all that surrounds them, as well as ancestors, stories, language, songs, and traditions (Bowra & Mashford-Pringle, 2021). We learned that there is an Indigenous Definition of Homelessness in Canada that was produced by Jesse Thistle (2017) in consultation with Indigenous communities. This document outlines 12 dimensions and has been critical in shaping understandings of – and conversations about – Indigenous homelessness in Canada.
Thistle (2017) notes in the definition that Canadians must face some difficult truths. One such truth is that climate change is having a disproportionately negative impact on northern Indigenous communities, creating a loss of culture, livelihood, and homelessness through this disconnection. What we have learned in this section is that homelessness is unique within an Indigenous context, and that there is no one size fits all approach that defines the experiences of all Indigenous peoples.
Click the link below to listen to all of the researchers answer the question “Is Indigenous homelessness defined differently than settler homelessness?” in audio format on our podcast!
17
In the previous section we considered the ways Indigenous homelessness is defined. Alberton et al., (2020) have noted that Indigenous peoples are oppressed in multiple ways and that intersecting sites of oppression increase the risk of Indigenous peoples becoming homeless in Canada. In this section we take a closer look at some of the sources of that oppression. Most notably, we consider how on–going colonizing practices create homelessness and serve to reproduce it within Indigenous communities over generations. Before continuing to the material in this section, we encourage you to pause here and reflect on this question. How do you think the causes of Indigenous homelessness are rooted in on-going colonizing practices? You may use the space below to write as little or as much as you wish to record your thoughts.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=602#h5p-58
In the previous section, we asked you to read the Indigenous Definition of Homelessness in Canada, in which Jesse Thistle (2017) wrote that it is time for Canadians to face some hard truths. We begin this section with the indisputable hard truth that Indigenous homelessness exists because of colonization. Prior to this time, no Indigenous person was homeless, as Jessica Rumboldt explains in the next video.
In this video, Jessica Rumboldt quotes scholars who explain that in the pre-contact era, before the influence of Europeans, no Cree person was homeless. She notes that society was egalitarian, everything was shared, and people were cared for and included through large extended families. Rumboldt explains that through colonization, traditional homelands and legal access to traditional homelands have been taken away, leaving a race of people homeless on a macro level. She concludes that Indigenous ceremonial traditions and cultural institutions that contribute to what constitutes a home, such as ritual languages and matriarchy, have been targeted by colonial powers. This video is 1:34 in length and has closed captions available in English.
Key Takeaways – Jessica Rumboldt: The lack of homelessness in the pre-contact era
Colonizing Indigenous peoples’ homeland has displaced these communities and led to mass-scale homelessness over generations. We see the effects of colonization on Reserve lands that exist today. We present below a video in which Robert Laboucane briefly discusses the history of how Reserves were created in Canada.
You may recall that Statistics Canada (2020) identifies 339,595 Indigenous persons living on-Reserve. This figure is not necessarily accurate, as people frequently move back and forth between Reserves and urban centers (Bono, 2019) and census data reflects western data collection methods which are not reflective of Indigenous ways of knowing. What research with northern Indigenous communities shows is that the effects of colonization have resulted in extreme poverty and overcrowded living conditions, difficulty obtaining affordable and suitable housing, reliance on scarce social services for survival, and valiant attempts to cope with the cold (and threatened) climate (Shaikh & Rawal, 2019). Many Indigenous communities live in remote and isolated regions of Canada (Schiff, Buccieri, Waegemakers Schiff, Kauppi, & Riva, 2020), where housing stock is limited (Pijl & Belanger, 2020).
Living on-Reserve does not mean a person is safely and securely housed. As you watch this next video, “Housing crisis deconstructed” created by APTN News, we encourage you to think deeply about the statement that no Indigenous person was homeless prior to colonization. This video was posted in 2017 and in the time since, Canada has created a National Housing Strategy and National Housing Strategy Act that makes housing a human right (Government of Canada, 2018, 2019). You can learn more about these in the chapter on Politics, Policy, & Housing in Canada. However, for now we ask that while you watch this video you reflect on whether you believe the conditions have improved since 2017 and why adopting a human rights-based approach is critical.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=602#h5p-57
We have seen that within an Indigenous worldview, home is not about a physical place but rather a relation to the land. Through colonization, that land was taken away and turned into private property. In the next video, Dr. Naomi Nichols explains how racist state formation policies have benefited white settlers at the cost of exploiting Indigenous peoples and their land.
In this video, Dr. Naomi Nichols argues that we must acknowledge the fundamental intersection between colonization, private property ownership, land stealing, and the dislocation and entrapment of Indigenous people in Reserve territories. She explains that white settlers in particular will have to let go of exploitative practices that have benefitted them at the expense of others. Rather than attributing property ownership to hard work, Dr. Nichols clarifies that racist state formation policies that dictate who can own land, vote, and act as citizens are at the root of why some people have profited while others have not. This video is 1:23 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Long-standing colonial policies
Colonizing practices have created homelessness amongst Indigenous communities by exploiting them and their lands, for the benefit of white settlers. This is one of the difficult truths that we must face in this chapter. In the following episode of The Agenda with Steve Paikinfrom 2017 entitled, “Indigenous Communities: Surviving Canada” panelists have a riveting debate about the state’s current complicity in keeping Indigenous communities in crisis to exploit their natural resources. We invite you now to watch this video and consider what the panelists say about how the causes of Indigenous homelessness are rooted in on-going colonizing practices.
After watching this debate, where do you stand on the issue of whether Canada is intentionally keeping Indigenous communities in crisis to facilitate the exploitation of their resources? What point or argument stood out the most to you from this debate?
The effects of colonization are clear in Canada today. Historical actions and decisions – like displacing people from their land and culture – still exist today in our modern laws and system of governance. In the next two videos, Dr. Jeannette Waegemakers Schiff and Dr. Rebecca Schiff speak about the immensely detrimental impact of these laws on Indigenous peoples today.
In this video, Dr. Jeannette Waegemakers Schiff reflects on the historical migration of predominantly British individuals to Canada and the subsequent legal actions that pushed Indigenous peoples onto Reserves without consideration for how they would live there. She notes that today we are seeing the outcomes of these horrible and dehumanizing decisions, and that these policies have led us exactly where we are now. Dr. Waegemakers Schiff concludes that undoing this history is going to be a huge challenge. This video is 1:39 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: How are the causes of Indigenous homelessness rooted in on-going colonizing practices?
In this video, Dr. Rebecca Schiff explains that there are complex threads of colonization that intersect in many ways in the lives of Indigenous peoples. She notes examples such as residential schools, the 60s/70s scoop, current scoop, foster care, and the way that the Indian Act controls Indigeneity, location, identity, sovereignty, and self-governance for Indigenous peoples. Dr. Schiff argues that the current pathways into homelessness, such as through correctional systems, child welfare, and mental health and/or substance use challenges are secondary and rooted in colonial systems and structures. Dr. Schiff concludes that we need to dismantle these structures and move towards greater self-governance and sovereignty for Indigenous peoples, in order to eliminate all of the secondary causes that contribute to homelessness. This video is 2:30 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: How are the causes of Indigenous homelessness rooted in on-going colonizing practices?
On-going colonizing practices have removed Indigenous peoples from their land and separated them from their families and cultures. We see this clearly with the state’s removal of children from Indigenous families in the past, such as through the 60s scoop, and in the present through high rates of child welfare involvement. As a population, Indigenous people are at a much higher risk of being involved with child welfare systems, and this involvement has been found to be the strongest predictor of subsequent visible homelessness (Alberton et al., 2020). In a northern Ontario-based study, all of the participants reported having multiple and intergenerational experiences of family separation resulting from child welfare involvement, placement in residential schools, and the death of family members, resulting in lifelong mental health and addictions struggles (Shaikh & Rawal, 2019). In this section’s featured reading, we invite you to reflect upon, “My life story, my youth” written by Rose Henry who was removed from the care of her residential school survivor parents during the 60s scoop. She shares her personal narrative on the impact these colonial traumas have had throughout her life.
Henry, R. (2015). My life story, my youth. In Inclusion Working Group, Canadian Observatory on Homelessness (Eds.). Toronto, ON: Homeless Hub. Chapter 6: My Life Story My Youth.pdf
Rose’s story demonstrates the range and depth of violence Indigenous women are exposed to. We see these women repeatedly being the victims of physical violence, as evidenced by the large number of missing and murdered Indigenous women and girls (National Action Plan, 2021) as well as being victims of institutional and systemic violence. Indigenous women are more likely to be victims of physical and sexual assault, and relatedly meet the criteria for post-traumatic stress disorder, multiple mental disorders, high rates of suicidality, and substance dependence (Bingham et al., 2019b). Children are often central in the lives of Indigenous mothers (Caplan et al., 2020), yet they continue to be removed from their care as an on-going form of colonization across Canada.
Research shows that Indigenous youth are more likely to be involved with child welfare services than non-Indigenous youth (Dunn, 2019). In a national survey of youth using homelessness agencies, Kidd, Thistle, Beaulieu, O’Grady, and Gaetz (2019) found that for Indigenous young people, being involved with child welfare was related to their current distress levels and that this involvement is strongly associated with risk for this population of youth. A subsequent replication of the survey several years later indicated the same findings, that homeless Indigenous youth face high risks related to child welfare involvement and the legacy of colonization (Kidd et al., 2021). In the next two videos, Jessica Rumboldt and Dr. Sean Kidd speak about this legacy and the survey results.
In this video, Jessica Rumboldt discusses research that shows Indigenous homelessness results from the breakdown of relationships rooted in historic processes of colonization. Indigenous youth have taken the brunt of these Canadian nation-state building projects, such as residential schools and the child welfare system, which have traumatized generations of First Nations, Métis, and Inuit communities. This video is 1:11 in length and has closed captions available in English.
Key Takeaways – Jessica Rumboldt: Indigenous youth homelessness and colonizing institutional practice
In this video, Dr. Sean Kidd discusses results of the second national survey of young people accessing homelessness support services. He notes that there are several findings unique to Inuit, Métis, or First Nation respondents. Dr. Kidd identifies child protection as having a longstanding history with multi-generational impacts for these youth in a way that is different than other populations of young people. He further discusses how the survey shows different risk profiles for Inuit, First Nations, and Métis identified young people born and raised on Reserve, but also notes the survey does not speak enough to the resilience these young people have. Dr. Kidd directs us to the work of Indigenous scholars to learn more. This video is 2:49 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: How are the causes of Indigenous homelessness rooted in on-going colonizing practices?
Dr. Kidd raises an important point, that in the discussion about horrors and traumas of colonization, we must recognize the strength of these survivors. Researchers in Winnipeg have found that Indigenous youth experiencing homelessness, who had been involved in child welfare, needed to be seen as resourceful and contributing members of the community (Brown, Knol, Prevost-Derbecker, & Andrushko, 2007). These youth also spoke about their need for on-going support from friends and family, and wanting to have a safe, nurturing, and permanent place to call home (Brown et al., 2007). We encourage you to consider the strength of these Indigenous youth as you watch the video below entitled, “Here and Now Youth Homelessness in Winnipeg.”
Agencies that support people experiencing homelessness are a critical part of the service infrastructure, particularly for Indigenous young people who are displaced from their families and communities. However, as we saw in the preceding video, services must incorporate Indigenous tailored supports. If they do not, they risk being ineffective and even harmful. For instance, we must consider how Indigenous spiritual practices are woven into these support agencies (Von Riesen, 2020) or risk increasing their sense of spiritual disconnection (Thistle, 2017). Bono (2019) notes that as Indigenous peoples move into urban centres, it is critical they be able to access Indigenous-specific organizations like shelters, day centres, and transitional housing.
The value of infusing Indigenous beliefs and practices into housing programs was evident in the Winnipeg site of the At Home / Chez Soi study (Distasio, Zell, & Snyder, 2018). This ground-breaking study, discussed in detail in the Politics, Policy, & Housing in Canada chapter, evaluated the effectiveness of Housing First as a program that supports people to find housing and then provides on-going supports based on their identified needs. In Winnipeg, the focus of the Indigenous Housing First program was to be holistic, relationship-based, strengths-based, and to ensure participants and staff had access to the supports and services they needed (Distasio et al., 2018). In another study evaluating the creation and management of housing for Indigenous people living with HIV, researchers found there was a need to create spaces for ceremonial practices and cultural traditions, and to provide support from an Indigenous perspective (Ion et al., 2018). In the next video Dr. Nick Falvo discusses findings from a housing program evaluation he led and what he learned about the need to integrate Indigenous practices.
In this video, Dr. Nick Falvo argues that the housing needs of Indigenous people are different than the housing needs of non-Indigenous people. He points to the outcomes within a local non-profit housing provider and explains that right from intake, processes may be set up in a way that does not meet the needs of Indigenous tenants. Dr. Falvo discusses his research with this organization’s tenants, Knowledge Keepers, and Elders. He points to ways that housing providers can improve orientation and programming to be more culturally appropriate for Indigenous tenants. Dr. Falvo notes these changes will require money, partnerships with Indigenous organizations, and the will to implement them. This video is 3:44 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: How are the causes of Indigenous homelessness rooted in on-going colonizing practices?
In this section, we posed the question, “How are the causes of Indigenous homelessness rooted in on-going colonizing practices?” We began with the difficult truth that prior to settler colonization, there was no homelessness amongst Indigenous peoples. We saw that the process of displacing people – through the Reserve system – marked the beginning of exploitative practices and traumatic outcomes that are still prevalent today. As part of this section, we presented a debate in which a panelist argued Canada intentionally keeps Indigenous communities in crisis because it benefits the state to be able to access the natural resources on their land. While it may be difficult to accept this, we cannot deny that colonizing practices are not only present but are given power through laws like the Indian Act.
Indigenous people have been removed from their land and taken away from their families since the arrival of settlers in Canada. We see this clearly with the state’s removal of children during residential schooling, the 60s scoop, and through child welfare practices today. We urge you to recall here Rose’s story about how her family was deeply fractured and the trauma that resulted. As Indigenous youth exit care they are likely to end up visibly homeless and living in urban centres. It is important that service agencies be established to support these youth, and Indigenous adults as well, using an Indigenous worldview and practices. Not doing so risks creating further harm and spiritual disconnection. This section has highlighted some of the key colonial practices that are at the root of Indigenous homelessness. We do not in any way suggest that this is a complete list or comprehensive discussion, but rather a starting point that we hope propels you to learn more.
Click the link below to listen to all of the researchers answer the question “How are the causes of Indigenous homelessness rooted in on-going colonizing practices?” in audio format on our podcast!
18
After learning about how the causes of Indigenous homelessness are deeply rooted in on-going colonizing practices, we believe it should be clear that there are no quick fixes that will instantly solve this issue. In asking the question, “How can we begin to decolonize society and decrease Indigenous homelessness?” we are very aware that any solutions will take time. However, we are also aware that beginning is the first step. We will not get anywhere if we do not begin somewhere. This is a daunting question but, just like we have asked of ourselves and you as learners through this chapter, we must approach it with the recognition it is difficult and will involve some hard truths. Yet, this section also contains some very inspiring ways forward. Before you work through the material, we ask that you pause here and record some of your own thoughts on how we can begin to decolonize society and decrease Indigenous homelessness.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=605#h5p-59
As we began our exploration of how to decolonize society, we found that the responses and research all connected to the problems previously identified as root causes. We were inspired by the range of projects and initiatives that are underway to begin to address these problems. Throughout this section we will use a spotlight approach to highlight these projects and make connections to the sources, so you can learn more. We recognize that the scope of work being done towards decolonizing is vast and we are representing only a sample of the remarkable work being done here. As always, we encourage you to explore further and expand your knowledge beyond this chapter.
Dr. Suzanne Stewart, who appeared in the debate from the previous section, has written, “Homelessness is not always easy to discuss. It often elicits strong emotional reactions— pity and sympathy, disdain, anger, blame, fear. In the consciousness of the average Canadian thinking about people who are homeless, particularly Indigenous people, a blame the victim mentality prevails. Non-Indigenous Canadians misunderstand the Indigenous experience of homelessness at best and are ignorant or blatantly racist at worst” (Stewart, 2018, pg.98). Arguably some of the most important things that non-Indigenous people can do are to listen and engage with Indigenous worldviews from a place of respect. We open this section with a video of Jessica Rumboldt, Post-Doctoral Fellow in Indigenous Homelessness at the Canadian Observatory on Homelessness, in which she discusses the importance of having on-going engagement and communication between Indigenous persons and Canadian settlers.
In this video, Jessica Rumboldt argues that addressing Indigenous homelessness is a continuous process that requires ongoing commitment, with respectful and mindful consideration of the various communities and unique individuals involved. She notes that engagement is a key component, such as with Indigenous communities, people with lived experience of homelessness, persons living on and off Reserve, and those inside and outside the sector. Rumboldt argues that it is through open and vulnerable discussions that we can move forward, and that we must work collaboratively rather than in silos. She concludes by discussing a report she and her colleagues created on behalf of the Assembly of First Nations that explores many issues and recommendations related to Indigenous homelessness. This video is 3:48 in length and has closed captions available in English.
Key Takeaways – Jessica Rumboldt: The need for on-going open and vulnerable discussions
 Jessica Rumboldt is part of a team working on the Endaamnaan: Homes for all Nations project, with the Assembly of First Nations. We encourage you to learn more about the literature review and First Nations systems mapping initiative it supports using these links below.
Jessica Rumboldt is part of a team working on the Endaamnaan: Homes for all Nations project, with the Assembly of First Nations. We encourage you to learn more about the literature review and First Nations systems mapping initiative it supports using these links below.
The project spotlighted above entails a systems-mapping component to improve housing quality and availability on Reserves. Decolonizing practices must begin with a recognition of the land that has been stolen from Indigenous peoples and with actions that lead to tangible change. In the next two videos, Dr. Abe Oudshoorn and Dr. Jeannette Waegemakers Schiff speak about these issues.
In this video, Dr. Abe Oudshoorn argues that decolonization is not just about thinking and learning, but rather action that involves consideration of the land. He notes that while it is important we learn, such as through Truth and Reconciliation, we must also acknowledge that the essential element of the colonization process has been the taking away of traditional lands. Dr. Oudshoorn warns that if we do not consider land as the starting point, we are going to end up replicating processes used to address settler forms of homelessness, which are not sufficient. This video is 2:33 in length and has closed captions available in English.
Key Takeaways – Dr. Abe Oudshoorn: How can we begin to decolonize society and decrease Indigenous homelessness?
In this video, Dr. Jeannette Waegemakers Schiff argues that apologies are just words and that actions have more meaning. She challenges us to ask hard questions, such as when are we going to give every Reserve clean drinking water and proper housing? Are we willing to admit that housing on Reserves has been built with cheap materials and poor construction? Dr. Waegemakers Schiff concludes by noting that many people do not want to believe the conditions on Reserves are real because they are so horrible. This video is 1:39 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: How can we begin to decolonize society and decrease Indigenous homelessness?
We have seen throughout this chapter that Indigenous homelessness is about more than the loss of a house, it is about the loss of land and relations. Indigenous communities have been displaced from the free use of land and placed on Reserves, often in rural, remote, and/or northern regions. This is a modern–day practice, as much as an historical one. Ballard, Coughlin, and Martin (2020) have written about a 2011 human-made flood that displaced 17 First Nation communities in the Interlake region of Manitoba, creating forced displacement and resulting in premature death, worsening chronic illness, depression, and loneliness (Ballard, Coughlin, & Martin, 2020). Four years later First Nations Elders held a gathering in Winnipeg to discuss ways to heal, and they engaged in a participatory research project to record their perspectives and recommendations towards reconciliation and minoayawin (well-being). The Elders’ insights into their communities healing involved strategies to: forgive, stand united, promote self-determination, reclaim cultural identity, and connect with the land (Ballard et al., 2020). The video below is one such recording, of Elder Maryjane Sinclair from Little Saskatchewan First Nation sharing her perspective on returning home after her community’s displacement.
When Elders speak, we all must listen and learn. The outcomes of the participatory project described above are well documented and can be accessed using the links below. We encourage you to watch the videos about the flood, read the healing guide, and watch the individual Elders’ recordings.
In the previous section, we shared a video of Dr. Nick Falvo discussing his research documenting what Indigenous youth identified as needing to feel connected and supported within their housing. In the video that follows he shares his thoughts on the importance of representation in decolonization. Just as in the project spotlighted above listening to, and learning from, Indigenous voices is essential if we are to move towards decolonization.
In this video, Dr. Nick Falvo notes that decolonization starts with representation and consideration of who is at the table. He argues that many organizations have a Board of Directors that does not reflect the people they are helping, and that they must work to enhance the presence of Indigenous people at all levels. Dr. Falvo states that looking to Indigenous people for guidance and listening to the knowledge they share is critical, and that it must be done in culturally respectful ways such as offering tobacco as a gift. This video is 2:56 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: How can we begin to decolonize society and decrease Indigenous homelessness?
Dr. Falvo argues that decolonization begins with representation. Why do you think it is important for Indigenous people to see other Indigenous people represented in various roles in a social service agency and more broadly throughout society?
Thistle and Smylie (2020) have written that responses to Indigenous homelessness must be led by Indigenous peoples and grounded in Indigenous worldviews, because the life experience of an Indigenous person with lived experience of homelessness is an invaluable gift that can enrich communities and teach providers. In much the same way that we, as authors, have grappled with writing about Indigenous homelessness as non-Indigenous people, so too have the non-Indigenous researchers we spoke to. For example, in the next two videos, Dr. Rebecca Schiff and Dr. Sean Kidd each draw on their research to speak about the need to end family displacement practices, but also note their limitations in answering this question as non-Indigenous people.
In this video, Dr. Rebecca Schiff questions the role of white people in identifying solutions to decolonize society. She notes that getting rid of the Indian Act is an important step and that keeping Indigenous children with their families is best, regardless of whether they are removed by child welfare or are forced to migrate to larger cities to complete school. Dr. Schiff concludes by discussing the complexity of ending racism, as something that occurs across society and in our institutions, such as related to housing, corrections, and health care. This video is 4:13 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: How can we begin to decolonize society and decrease Indigenous homelessness?
In this video, Dr. Sean Kidd explains that the experience of homelessness can impact a person’s sense of identity and self-worth. Building resiliency involves creating or reclaiming a self-concept that resists stigmatizing messages. Dr. Kidd notes that for Indigenous youth, identifying with their cultures of origin can be a power tool in that effort. He notes that there are some organizations that have been helping to connect these youth with Elders, and to find pathways for engaging with their cultures, histories, families, and communities. Dr. Kidd notes that while we may want to think of Canada as a safe place, there are many forms of discrimination, and that First Nations, Métis, and Inuit youth may experience multiple and interconnected types. He concludes that the best way to learn more about these issues is not to listen to a white man, but to seek out resources and to speak to young people directly. This video is 6:08 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: Supporting Indigenous youth through engagement with their culture and Elders
The research is clear that child welfare involvement is higher amongst Indigenous youth, which is an on-going form of colonization and contributes to the high rates of homelessness amongst this population (Dunn, 2019; Kidd et al., 2019, 2021; Shaikh & Rawal, 2019). In this section’s featured reading, Stewart (2019) explores how a social-constructivist approach to family counselling can be used as a means of working towards decolonization in clinical practice.
Stewart, S. (2019). Family counselling as decolonization: Exploring an Indigenous social-constructivist approach in clinical practice. First Peoples Child & Family Review, 14(1), 43-56.
For Indigenous youth, reconnecting with family and transitioning out of homelessness may be important yet challenging goals. The Housing Outreach Project – Collaborative (HOP-C) is a multi-partner project that focuses on youth leadership and cultural relevance as two key aspects to supporting youth as they make these transitions and lead healthier lives. As one part of the project, Indigenous youth leaders in Thunder Bay, Ontario developed a guide to help other young people using Indigenous knowledge and supports. We encourage you to read the guide and learn more about the project using the links below.
We saw in the previous section that service provision must integrate Indigenous practices and perspectives to be welcoming (Distasio et al., 2018; Ion et al., 2018; Von Riesen, 2020). Particularly within major urban centres, where Indigenous peoples may seek support and opportunities but be isolated from their families, having Indigenous-tailored services may help to provide stability and a sense of connection (Bono, 2019). Indigenous programs and services may integrate arts-based methods as a form of decolonization (Ansloo & Wager, 2020), integrate harm reduction programs in culturally relevant ways (Firestone, Syrette, Jourdain, Recollet, & Smylie, 2019; Victor et al., 2019; Young & Manion, 2017), or use land-based healing to promote reconnection (Redvers, Nadeau, & Prince, 2020).
One innovative program in British Columbia supports Indigenous inmates to grow organic produce and donate it to rural and remote Indigenous communities as a means of reducing food insecurity (Timler, Varcoe, & Brown, 2019). However, the authors of this study are clear to note that while the program helps, it does not address the broader issues such as the effects of colonization on disproportionate incarceration, access to land, use of resources, and the rights inherent in food sovereignty (Timler et al., 2019). This body of literature suggests that while it is important for services to include Indigenous programs, what is really critical is that this be done with recognition of broader historical contexts and the on-going traumas they produce (Bingham et al., 2019b).
In an article on advancing good relations with Indigenous people experiencing homelessness, Thistle and Smylie (2020) write that the considerable work of Pekiwewin, or coming home, needs to be led by Indigenous peoples but will be successful only if non-Indigenous service providers, decision-makers, and organizations are willing to engage on their own journeys of change. Read about their article on Pekiwewin and listen to an interview about this work on CBC Radio using the links below.
Throughout this section, we explored some of the inspiring initiatives being led by Indigenous people to address Indigenous homelessness. We recognize that these processes must be led by Indigenous peoples and ways of knowing, and that the work of decolonization requires non-Indigenous people listen and learn, with respect and willingness to change. We began this section with a reminder that we need to have open, honest, and on-going communication even if (or perhaps even more so because) we are talking about difficult issues. We saw that disconnection from the land is a primary cause of Indigenous homelessness and efforts at decolonization must begin there. However, they must not end there. We further saw that there is a need for representation of Indigenous people in various roles across society. One of the clearest forms of on-going colonization is family separation, such as through child welfare removals, and that family counselling and peer-support can be powerful decolonizing approaches. Integrating Indigenous supports into programs and services is important, particularly in urban settings, but these supports must be informed by Indigenous leadership.
Click the link below to listen to all of the researchers answer the question “How can we begin to decolonize society and decrease Indigenous homelessness??” in audio format on our podcast!
19
Joseph
At the beginning of the chapter, we met Joseph who is living rough outside an urban centre and hitchhiking into that centre for necessities. Joseph is a sixties scoop survivor who has struggled with his identity, most likely for a very long time. If you don’t know much about the sixties scoop please do some research in order to understand what this entailed and what Joseph might have experienced.
As Dr. Falvo has indicated, displacement from identity is one of the root causes of homelessness among Indigenous peoples.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1137#h5p-87
20
We began this chapter by identifying ourselves as non-Indigenous persons. As such, we tried to approach writing as a humble learning exercise. At the start of the chapter, we introduced you to the composite character Joseph as an entry point into thinking about the complexity of Indigenous homelessness. We returned to his story again at the end to demonstrate how it can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for developing a better understanding of Indigenous homelessness in Canada.
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers. We recognize that although many of the people we spoke to engage regularly (and respectfully) with Indigenous research, most do not identify as Indigenous. For this reason, we included more additional materials than in other chapters to open a space for us all to listen and learn from Indigenous perspectives.
First we asked, “Is Indigenous homelessness defined differently than settler homelessness?” Here we saw that although our question was wrong – set against the comparison of settler homelessness – the intention was right. We learned that there are indeed many unique aspects to Indigenous homelessness, rooted in the loss of home and land. We asked you to read the highly cited Indigenous Definition of Homelessness in Canada, produced by Jesse Thistle (2017) to learn about the 12 dimensions. We concluded this section by considering the loss of land and culture that exist today tied to climate change and its disproportionate effects on northern Indigenous communities and livelihoods.
Next we asked, “How are the causes of Indigenous homelessness rooted in on-going colonizing practices?” This led us to reflect upon how homelessness was created by settlers, resulting from colonization. Through the creation of Reserves, Indigenous people have been displaced from their land and experience housing precarity today. The governing powers that implemented colonial rule are still evident today in the Indian Act and the over-representation of Indigenous people in institutions, like prisons and child welfare. There are many Indigenous people who leave the Reserves or age out of state care and become homeless in major urban centres. These cities have a responsibility to provide Indigenous supports, with the risk of causing further harm and homelessness if these services are not in place.
Finally, we asked, “How can we begin to decolonize society and decrease Indigenous homelessness?” In this final section, we looked at some of the inspiring projects currently being led by Indigenous people. It should be noted that the “we” in the question is included with full recognition that settlers have a supporting role, and must be willing to listen, learn, and change, but that any change that occurs must be led by Indigenous peoples. We saw throughout this section that there are many places to start – the land, with representation, dismantling racism, and establishing supports for Indigenous youth to reconnect with Elders are just a few. There are many hard truths that arose through this chapter. Although we know this chapter was simply a brief overview of Indigenous homelessness, we hope that you will continue to learn along with us and support the work towards decolonization in Canada.
21
Here are some additional resources you may want to check out!
22
Research with Indigenous communities must be guided and approved by Indigenous Elders at all stages. As such we do not offer student research ideas here. As non-Indigenous persons doing so would not only be inappropriate, but it would be deeply disrespectful. Instead, we would like to offer these research guides created by Indigenous communities as suggested readings.
23
Alberton, A. M., Angell, G. B., Gorey, K. M., & Grenier, S. (2020). Homelessness among Indigenous peoples in Canada: The impacts of child welfare involvement and educational achievement. Children and Youth Services Review, 111, 104846. https://doi.org/10.1016/j.childyouth.2020.104846
Ansloos, J. P., & Wager, A. C. (2020). Surviving in the cracks: A qualitative study with indigenous youth on homelessness and applied community theatre. International Journal of Qualitative Studies in Education, 33(1), 50–65. https://doi.org/10.1080/09518398.2019.1678785
Ballard, M., Coughlin, J., & Martin, D. (2020). Reconciling with Minoaywin: First Nations Elders’ advice to promote healing from forced displacement. Canadian Journal on Aging, 39(2), 169–177. https://doi.org/10.1017/S0714980819000412
Bezgrebelna, M., McKenzie, K., Wells, S., Ravindran, A., Kral, M., Christensen, J., Stergiopoulos, V., Gaetz, S., & Kidd, S. A. (2021). Climate change, weather, housing precarity, and homelessness: A systematic review of reviews. Int. J. Environ. Res. Public Health, 18, 5812. https://doi.org/10.3390/ijerph18115812
Bingham, B., Moniruzzaman, A., Patterson, M., Distasio, J., Sareen, J., O’Neil, J., & Somers, J. M. (2019a). Indigenous and non-Indigenous people experiencing homelessness and mental illness in two Canadian cities: A retrospective analysis and implications for culturally informed action. BMJ Open, 9(4), e024748–e024748. https://doi.org/10.1136/bmjopen-2018-024748
Bingham, B., Moniruzzaman, A., Patterson, M., Sareen, J., Distasio, J., O’Neil, J., & Somers, J. M. (2019b). Gender differences among Indigenous Canadians experiencing homelessness and mental illness. BMC Psychology, 7(1), 57–57. https://doi.org/10.1186/s40359-019-0331-y
Bono, K. (2019). The faces of Indigenous homelessness: The perpetual Inuit housing struggle. Master’s Thesis. McGill University.
Bowra, A., & Mashford-Pringle, A. (2021). More than a structure: Exploring the relationship between Indigenous homemaking practices and wholistic wellbeing. Wellbeing, Space and Society, 2. https://doi.org/10.1016/j.wss.2020.100007
Brown, J., Knol, D., Prevost-Derbecker, S., & Andrushko, K. (2007). Housing for Aboriginal youth in the inner city of Winnipeg. First Peoples Child & Family Review, 3(2), 56–64. https://doi.org/10.7202/1069464ar
Caplan, R., Nelson, G., Distasio, J., Isaak, C., Edel, B., Piat, M., Macnaughton, E., Kirst, M., Patterson, M., Aubry, T., Mulligan, S., & Goering, P. (2020). Indigenous and non‐Indigenous parents separated from their children and experiencing homelessness and mental illness in Canada. Journal of Community Psychology, 48(8), 2753–2772. https://doi.org/10.1002/jcop.22455
Cunningham, J. (2019). Towards a grounded understanding of the forms of homelessness experienced by Indigenous women in Canada. Recherches amérindiennes au Québec, 49(3), 29. https://doi.org/10.7202/1074538ar
De Leeuw, S., Greenwood, M., & Farrales, M. (2021). Indigeneity and wellness: Critically understanding the health of Indigenous peoples and communities. In K. Chamberlain & A. Lyons (Eds.). Routledge International Handbook of Critical Issues in Health and Illness. New York: Routledge International Handbooks.
Distasio, J., Zell, S., & Snyder, M. (2018). At home in Winnipeg: Localizing housing first as a culturally responsive approach to understanding and addressing urban Indigenous homelessness. Winnipeg: Institute of Urban Studies.
Dunn, K. (2019). A comparative analysis of Indigenous and non-Indigenous homeless youth in Canada. Master’s Thesis. University of Guelph.
Falvo, N. (2021). Improving housing stability among Indigenous residents at horizon housing. Calgary: Nick Falvo Consulting. FINAL_Housing-Stability-for-Indigenous-Residents_Report.pdf
Feir, D. L., & Akee, R. (2018). Estimating institutionalization and homelessness for status First Nations in Canada: A method and implications. International Indigenous Policy Journal, 9(4). https://doi.org/10.18584/iipj.2018.9.4.2
Firestone, M., Syrette, J., Jourdain, T., Recollet, V., & Smylie, J. (2019). “I feel safe just coming here because there are other Native brothers and sisters”: Findings from a community-based evaluation of the Niiwin Wendaanimak Four Winds Wellness Program. Canadian Journal of Public Health, 110(4), 404–413. https://doi.org/10.17269/s41997-019-00192-6
Government of Canada. (2018). Reaching home: Canada’s homelessness strategy directives. Government of Canada, Ottawa. Reaching Home: Canada’s Homelessness Strategy Directives – Canada.ca
Government of Canada. (2019). National housing strategy act. Government of Canada, Ottawa. National Housing Strategy Act (justice.gc.ca)
Greenwood, M. & Lindsay N. M. A. (2019). A commentary on land, health and Indigenous knowledge(s). Global Health Promotion, 26(3), 82-86. https://doi.org/10.1177/1757975919831262
Henry, R. (2015). My life story, my youth. In Inclusion Working Group, Canadian Observatory on Homelessness (Eds.). Toronto, ON: Homeless Hub. Chapter 6: My Life Story My Youth.pdf
Ion, A., Greene, J., Masching, R., Poitras, M., Brownlee, P., St. Denys, R., … Anaquod, J. (2018). Stable homes, strong families: reimagining housing policies and programs for Indigenous peoples living with and affected by HIV and AIDS in Canada. Housing and Society, 45(2), 118–138. https://doi.org/10.1080/08882746.2018.1496696
Kidd, S. A., Gaetz, S., O’Grady, B., Schwan, K., Zhao, H., Lopes, K., & Wang, W. (2021). The second national Canadian homeless youth survey: Mental health and addiction findings. Canadian Journal of Psychiatry, 66(10), 897-905. https://doi.org/10.1177/0706743721990310
Kidd, S. A., Greco, S. & McKenzie, K. (2021). Global climate implications for homelessness: A scoping review. J Urban Health, 98, 385–393. https://doi.org/10.1007/s11524-020-00483-1
Kidd, S., Thistle, J., Beaulieu, T., O’Grady, B., & Gaetz, S. (2019). A national study of Indigenous youth homelessness in Canada. Public Health (London), 176, 163–171. https://doi.org/10.1016/j.puhe.2018.06.012
Kolahdooz, F., Nader, F., Yi, K. J., & Sharma, S. (2015). Understanding the social determinants of health among Indigenous Canadians: Priorities for health promotion policies and actions. Global Health Action, 8(1), 27968–27968. https://doi.org/10.3402/gha.v8.27968
National Action Plan. (2021). 2021 missing and murdered Indigenous women, girls, and 2SLGBTQQIA+ people national action plan: Ending violence against Indigenous women, girls, and 2SLGBTQQIA+ people. Canada.
Patrick, C. (2014). Aboriginal homelessness in Canada: A literature review. Toronto: The Canadian Observatory on Homelessness.
Pijl, E. M., & Belanger, Y. D. (2020). Lost in transition: Entering the liminal space of rural homelessness in a small prairie town. Journal of Social Distress and Homeless, 1–9. https://doi.org/10.1080/10530789.2020.1763575
Redvers, N., Nadeau, M., & Prince, D. (2020). Urban land-based healing: A northern intervention strategy. International Journal of Indigenous Health, 16(2), 322–337. https://doi.org/10.32799/ijih.v16i2.33177
Rotondi, M. A., O’Campo, P., O’Brien, K., Firestone, M., Wolfe, S. H., Bourgeois, C., & Smylie, J. K. (2017). Our health counts Toronto: Using respondent-driven sampling to unmask census undercounts of an urban indigenous population in Toronto, Canada. BMJ Open, 7(12), e018936–e018936. https://doi.org/10.1136/bmjopen-2017-018936
Schiff, R., Buccieri, K., Waegemakers Schiff, J, Kauppi, C., & Riva, M. (2020). COVID-19 and pandemic planning in the context of rural and remote homelessness. Canadian Journal of Public Health, 111(6), 967–970. https://doi.org/10.17269/s41997-020-00415-1
Shaikh, A., & Rawal, H. (2019). Interconnections among homelessness, family separation, and mental health: Implications for multi-sectoral social services. Journal of Social Service Research, 45(4), 543–557. https://doi.org/10.1080/01488376.2018.1481174
Smith, E., Milaney, K., Henderson, R. I., & Crowshoe, L. (2021). Adverse childhood experiences and health among indigenous persons experiencing homelessness. BMC Public Health, 21(1), 85–85. https://doi.org/10.1186/s12889-020-10091-y
Statistics Canada. (2020). 2016 census Aboriginal community portraits. Canada: Statistics Canada.
Stewart, S. (2018). Supporting Indigenous youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Stewart, S. (2019). Family counselling as decolonization: Exploring an Indigenous social-constructivist approach in clinical practice. First Peoples Child & Family Review, 14(1), 43-56. https://fpcfr.journals.publicknowledgeproject.org/index.php/FPCFR/article/view/371
Thistle, J. (2017.) Indigenous definition of homelessness in Canada. Toronto: Canadian Observatory on Homelessness Press.
Thistle, J. (2019). From the ashes. My story of being Métis, homeless and finding my way. Simon Schuster: Toronto, Canada
Thistle, J., & Smylie, J. (2020). Pekiwewin (coming home): Advancing good relations with Indigenous people experiencing homelessness. Canadian Medical Association Journal (CMAJ), 192(10), E257–E259. https://doi.org/10.1503/cmaj.200199
Timler, K., Varcoe, C., & Brown, H. (2019). Growing beyond nutrition: How a prison garden program highlights the potential of shifting from food security to food sovereignty for Indigenous peoples. International Journal of Indigenous Health, 14(2), 95–114. https://doi.org/10.32799/ijih.v14i2.31938
Victor, J., Shouting, M., DeGroot, C., Vonkeman, L., Brave Rock, M., & Hunt, R. (2019). I’taamohkanoohsin (everyone comes together): (Re)connecting Indigenous people experiencing homelessness and substance misuse to Blackfoot ways of knowing. International Journal of Indigenous Health, 14(1), 42–59. https://doi.org/10.32799/ijih.v14i1.31939
Von Riesen, K. (2020). Providing meaningful spiritual care to Indigenous populations experiencing homelessness. Master’s Thesis. University of Manitoba.
Young, M. G., & Manion, K. (2017). Harm reduction through housing first: an assessment of the Emergency Warming Centre in Inuvik, Canada. Harm Reduction Journal, 14(1), 8–8. https://doi.org/10.1186/s12954-016-0128-8
III

On its face, homelessness seems like an easy problem to solve. If we just had more housing, no one would be homeless. There is a sort of logic to this idea, that if we increased the housing supply then we would not have a problem anymore. However, like most things in life, it is just not that simple. Complex problems rarely have easy answers, and homelessness is a complex problem. While homelessness is always a housing issue, it is not only a housing issue.
Homelessness exists in its current state in Canada because of political decisions that were made in the past, and how it will exist in the future depends on the decisions that are made today. While homelessness may be felt at a very personal level, its roots can be found in the decisions that are made by political parties. The power to effect change rests with ruling bodies, but this power is not absolute. Indeed, the power to influence change comes not only from the top down, but from our society at large. We have seen change come from organized groups, such as social movements and non-profit organization leaders. Tracing the politics and policies of housing is a key consideration in understanding homelessness in Canada today.
24
In this chapter, you are invited to consider the history of policies and politics that have led to homelessness in its current state in Canada. While tracing the winding twists and turns in the chronology, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that homelessness exists in society because of decisions that are made by people in power. We may not be able to change the decisions that have been made in the past, but we can have an impact on the decisions that will be made in the future. Read on to learn more about where we have been and where we are now. Where we go next is up to all of us.
25
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to politics, policy, and housing. As you work through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After considering the real-world scenario, we will endeavour to answer each question posed in the learning objectives. What housing policy existed in the past? Is Housing First a solution to homelessness? What is happening with housing and homelessness policy today? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
26
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider this person’s experience.
Tish
Tish is a 32 year old female who lives in and around the downtown area of a medium sized city. They have been living out of a shopping cart, carrying everything with them since being released from hospital 2 years ago. They have a long history of depression and suffer with the chronic effects of an acquired brain injury (ABI). They were struck on the head with a hammer at age 26 during a domestic dispute. Their ABI causes weakness, stiffness, poor balance, and unregulated mood swings which lead to verbal aggression. Bystanders and first responders often mistake them for being intoxicated.
They camp in a rotating number of sites in the city, they set up campsite at night and have to put everything back in the shopping cart during the day. If they sleep late the police or city bylaw enforcement officers roust them, demand they move on, and issue them a $100 ticket for loitering. They cannot pay these fines. If they are not quick enough in the morning, the city confiscates their things, throwing them away. They are not welcome at local shelters due to their history of aggressive behaviour. Each of the shelters in the city have a no tolerance policy for aggressive or violent behaviour, including verbal behaviour. Their Ontario Disability Support Program (ODSP) payments were revoked due to missed appointments and misunderstandings, therefore they have no money for shelter.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to this scenario again at the end of the chapter.
Reflection Questions
27
What is the housing market like in the community where you live? You can check out your neighbourhood and others in the Canadian Mortgage and Housing Corporation’s Housing Market Information Portal. Go ahead – we’ll wait!
Across Canada housing prices are on the rise. Analysis of housing policy trends throughout Canada’s history show that the solutions the government adopts to meet the problems deemed essential at one point in time have often created a new set of problems that require different solutions in the period that follows (Carroll, 1989). Essentially this suggests that much of our housing policy is created as a reaction to the policy choices that came before. In this section, we explore the question of what housing policy existed in the past, as a way to set the stage for understanding what housing policy decisions are being made today.
Before you begin this section, we encourage you to take a moment to reflect on what you already know about historical housing policies in Canada. Whether you are familiar with this issue already, or whether this is your first introduction to the topic, it is beneficial to consider what you know before moving forward. You may wish to write a brief summary of your knowledge or some questions you have at this time. This writing is for your benefit only and not going to be shared with your instructor or fellow classmates. You should feel free to write as little or as much as you wish to help you identify your starting point before moving into the material.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=641#h5p-35
You may find it interesting to know that homelessness did not exist, in its current form, before the 1980s in Canada. Although there were hobos who would ride the rails in search of employment in the early 1900s, we did not have the crisis situation that we have today. We begin this section with an exploration of the idea that mass homelessness is a modern occurrence, through a video of Dr. Bill O’Grady and a blog post from the Homeless Hub.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video Dr. William [Bill] O’Grady draws our attention to the way ‘homelessness’ is a word that is used much more commonly today than it was prior to the 1980s. He notes that while poverty and homelessness existed, there were governmental supports in place to assist people. Dr. O’Grady encourages us to ask hard questions about why the problem of homelessness has emerged over the last 30-40 years and notes we will only find the answers by looking at larger structural changes that have taken place in the Canadian economy and polity from the 1980s onwards. This video is 1:19 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: Homelessness in the past compared to today
Click the image below to open a new window and read the full blog post, “Why Wasn’t Homelessness a Social Problem Until the 1980s?” by Emma Woolley.
Testing drop-shadow through inline CSS
aligncenter wp-image-947 size-large" src="https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-1024x650.png" alt="screenshot of landing page for "why wasn't homelessness a social problem until the 1980s" blog post" width="1024" height="650" srcset="https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-1024x650.png 1024w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-300x190.png 300w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-768x487.png 768w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-1536x975.png 1536w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-2048x1300.png 2048w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-65x41.png 65w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-225x143.png 225w, https://ecampusontario.pressbooks.pub/app/uploads/sites/1249/2021/11/Screen-Shot-2021-12-09-at-3.21.07-PM-350x222.png 350w" sizes="(max-width: 1024px) 100vw, 1024px" title="">Urban restructuring throughout Canadian cities in the 1980s and 1990s meant that society underwent political, economic, and spatial shifts in how people interacted, what kinds of jobs they had, where they lived, and what kinds of supports were available from the government (Greene, 2014). These shifts were polarizing, in that they produced and consolidated new forms of social and spatial segregation, which became evident with the emergence of mass homelessness around this time (Greene, 2014).
Knowing that mass homelessness emerged in the 1980s and 1990s raises the question of “why?” It was not the case that a large number of people suddenly became homeless for no reason. Rather, this was the foreseeable result of policy decisions made by the Federal government at the time. To understand what happened, we need to set our sights even further back in history to the World War II era. Dr. Nick Falvo takes us through the history.
In this video Dr. Nick Falvo speaks about the history of social housing in Canada. Although there was virtually no government assisted housing prior to the second World War in Canada, this time period saw the development of wartime housing. Dr. Falvo explains that this development was jointly driven by the need to house civilians engaged in the war effort making munitions and supplies to send overseas, and the advocacy of soldiers in need of housing upon their return from war. The 1960s and 1970s saw the birth of Canada’s social welfare system and strong support for social housing from high orders of government. In the 1990s policy shifted toward neoliberal declines in social spending. This represented a time period which Dr. Falvo describes as being “very dark years of housing policy in Canada.” This video is 4:09 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: What housing policy existed in the past?
Wartime housing was created for people working in the war-industry, but soldiers had to advocate for themselves to get access to housing upon their return. Consider this brief Heritage Moment clip entitled, “Home from the Wars.”
Canada’s current housing crisis stems from decades of policy decisions, not only about housing but about social welfare supports as well. Dr. Jonathan Greene further explains the timeline of these policy changes, beginning during the second World War when government housing was provided to citizens, not because it was the right thing to do but because it helped the economy.
In this video Dr. Jonathan Greene provides a comprehensive overview of key dates and pieces of legislation in Canada’s social housing policy history. He argues that the consistent bias throughout this history is to allow the market to be pre-eminent in providing housing for Canadians and for the government or public authorities only to intervene to pick up the pieces. Dr. Greene traces the history of social housing, beginning before the second World War, when there was very limited federal or provincial housing interventions. In the early 1940s there was a wartime housing program developed, and the National Housing Act amendments represented a more forceful intervention by the federal government into creating social housing. It is noteworthy that this housing was intended to be short-term and was built to support job development and the economy, as civilians moved to cities to work in the war effort, leading to housing shortages. Dr. Greene further traces the development of social housing in the 1960s, the entry of third-party sectors into building social housing and co-operative housing in the 1970s, the beginning of the federal withdrawal in the 1980s, and the culmination in 1993 when the federal government moved out of creating social housing completely. This video is 6:11 in length and has closed captions available in English.
Key Takeaways – Dr. Jonathan Greene: What housing policy existed in the past?
Federal housing and social policies have undergone many changes since the World War II period. As you watch this brief 17–minute documentary entitled, “Wartime Housing” created by the National Film Board of Canada, it is beneficial to keep in mind that new policies are often created as a reaction to problems that were created by previous policies. What problems do you think followed the post-World War II era in Canada?
Click the image below to open a new window and watch the “Wartime Housing” documentary.

Wartime housing was built throughout Canada for people working in war-related industries, and later for soldiers. Have you noticed any of these houses in your own neighbourhood? The next time you are out for a walk or a drive, take a look around and see if you can find anywhere you live.
Following the Second World War period, that saw strong Federal investments in social housing, a shift began to occur in the 1980s. A recession at the time meant that the government started to decrease their investments in social housing in the 1980s and stopped building it entirely in the 1990s, making it instead the responsibility of Provincial governments. In Ontario, the provincial government further downloaded the responsibility for social housing to municipalities. In the next set of videos Dr. John Ecker, Dr. Erin Dej, and Dr. Jacqueline Kennelly explain this history of policy changes.
In this video, Dr. John Ecker highlights the shifts in affordable housing legislation that have occurred in Canada since the post-World War II period. In 1938 the federal government passed the National Housing Act, which made provision for construction of low rent housing, and in 1949 it was expanded to include funding for publicly owned and provincially managed housing for low-income families, seniors, and people with disabilities. Dr. Ecker notes that we see this legislative support withdrawn in the early 1990s, followed by an announcement in 1996 that the management and ongoing subsidies would be transferred to the provinces. This video is 1:40 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: What housing policy existed in the past?
In this video Dr. Erin Dej discusses the shifts in federal investments for social housing that have occurred over the past several decades in Canada. In the 1950s and 1960s there were strong post-war investments in building social housing, that continued up until the 1980s. Beginning in the 1980s the federal government began to withdraw from their role in building social housing, and in the 1990s formally stepped back from creating new social housing and also from maintaining the social housing stock that already existed. This video is 2:56 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: What housing policy existed in the past?
In this video, Dr. Jacqueline Kennelly discusses the impact of wealth inequality as a risk factor for homelessness. She traces the roots of current poverty and homelessness to federal policy decisions made in the 1990s to withdraw from creating affordable housing, and to download the responsibility to provinces which had varied responses, such as further downloading to municipalities with limited tax bases. This video is 1:38 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Historical downloading of affordable housing
Housing policy decisions made in the past have brought us to where we are today in Canada. Much of our understanding about housing policy comes from the work of Professor David Hulchanski, whose influential research is widely cited. At this time, we encourage you to read some of his co-authored work entitled, “Canada’s Housing Story.”
Chisholm, S., & Hulchanski, D. (2019). Canada’s housing story. In D. Maclennan, H. Pawson, K. Gibb, S. Chisholm, & D. Hulchanski (Eds.). SF 21: Shaping Futures Changing the Housing Story Final Report. University of Glasgow: Policy Scotland.
The lack of affordable housing today is a problem that contributes to high rates of homelessness across the country. However, we also must consider that housing is one piece of a complicated and interconnected puzzle that also requires we address poverty and the lack of financial supports in our current neoliberal state structure. Preventing and ending homelessness requires strategic investment and changes to policies and practices to address the risk factors that contribute to homelessness (Dej & Ecker, 2018). Until the underlying structural and system pieces that contribute to homelessness are addressed, we are going to continue to see high rates (Gaetz, 2010). In these next two videos, Dr. Tim Aubry and Dr. Stephen Gaetz explain how poverty, a lack of affordable housing, and neoliberal state governance are related factors that have carried forward over time.
In this video, Dr. Tim Aubry discusses three macro level policy issues that have driven increased rates of homelessness in Canada. First, beginning in the 1980s and 1990s the Federal government’s decision to withdraw from building social housing has led to a lack of affordable housing in cities across Canada. Second, homelessness needs to be recognized as the face of extreme poverty in Canada, that persists despite some poverty-reduction measures such as the Canada Child Benefit that have had limited impact. Finally, Dr. Aubry argues we must examine additional social policies and institutions that have contributed to homelessness, such as the child welfare and mental health systems. This video is 5:20 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: What housing and homelessness policy existed in the past?
In this video, Dr. Stephen Gaetz argues that we created modern mass homelessness in Canada through a number of policy decisions, a changing economy, and the rise and application of neoliberalism. Beginning in the late 1980s, the federal government shifted from making direct investments in building affordable housing to using market measures, such as tax expenditures, to encourage private sector building and new homeownership. After 30 years of not investing in affordable housing for low-income people, combined with a population increase of 30%, we have created the housing crisis we are living in today. Dr. Gaetz further recognizes the impact of neoliberal cuts to income supports, and a changing economy that promotes part-time and low-paying jobs, as key drivers that have led to a dramatic increase of homelessness in Canada. This video is 3:22 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: What housing policy existed in the past?
In this section, we considered the question, “What housing policy existed in the past?” The answer is important to know because, as we have seen, policy decisions tend to be made in response to problems created by previous policy decisions. We began our timeline around the second World War, when housing was built for people working in the war industry and for soldiers after they advocated for their needs. We saw that Canada had a strong network of social supports in the 1960s and 1970s, but that they declined with the recession of the 1980s. During this period, the federal government began to withdraw from building social housing and subsequently withdrew completely in the 1990s. These neoliberal policy decisions created conditions of extreme poverty and wealth inequality that persist. Although we may not have heard much about homelessness prior to the 1980s, we certainly feel its presence today.
Click the link below to listen to all of the researchers answer the question “What housing policy existed in the past?” in audio format on our podcast!
28
Housing First is one of the many deceptively simple concepts that emerge in this book. Just as the name suggests, the idea is to get people into housing as the first step. From there, if the person wants, they have the choice to access a range of support services. This idea is a departure from previous approaches in which people would have to prove themselves “housing-ready” by meeting a specific set of qualifications, like abstaining from substances for a given period of time or having steady employment. Housing First reverses the order and says that everyone is ready for housing. It has been widely adopted across the country.
Before you begin working through the material in this section, we encourage you to stop and reflect upon the question, “Is Housing First a solution to homelessness?” Housing First has existed – in its current and early forms – within Canada for decades. Yet, we still have crisis levels of homelessness across the nation. We encourage you to pause here and consider what you might have already heard about Housing First, why you think it has been so popular, and why we still have high rates of homelessness. We would also like to remind you that this answer is for your learning benefit only, so that you can take stock of your knowledge before you begin. You may write as much or as little as you wish.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=646#h5p-38
The framework of Housing First in Canada is adapted from the work of Dr. Sam Tsemberis, Founder and CEO of Pathways to Housing in New York. Before we begin our discussion of Housing First in Canada, we would like to set the stage with this brief 4-minute video in which Dr. Tsemberis outlines the core ideas of how his Pathways program began. It is important to remember as you watch this, that he is speaking about the original American program and that we will review the Canada data throughout the section that follows this video.
In the previous section, we said that it is important to know the history of housing policy in Canada to understand our current situation. Well, here we are, saying it again (and will continue to say it in the next section!) because now that you have read the history, it will likely not surprise you to know that early forms of Housing First emerged in the 1990s. As the federal government stepped back from funding social housing and mass homelessness began to emerge, advocates realized that what people needed most was housing. Dr. Nick Falvo explains the connection between the early roots of Housing First and historical policy decisions.
In this video, Dr. Nick Falvo provides background on how Housing First came to be adopted as a homelessness intervention in Canada. He traces the history to the 1990s when large scale cuts were being made to housing and social policy. Housing First was introduced by key advocates under the premise of reallocating existing funding, rather than requiring enhanced funding. Dr. Falvo argues that while taking people from homelessness straight into housing was framed as a new idea, it was a practice already being done in Ottawa and Toronto under the name ‘supportive housing.’ While Dr. Falvo says key decision-makers believed Housing First would lead to dramatic reductions in homelessness, the data over time has not indicated a strong downward trend. This video is 3:32 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: Is Housing First a solution to homelessness?
Today, much of the work around Housing First across the country is informed by the ground-breaking $110 million Mental Health Commission of Canada study known as “At Home / Chez Soi.” This project operated from 2009 to 2013 and was a coordinated effort in the five sites of Vancouver, Winnipeg, Toronto, Montreal, and Moncton, to evaluate Housing First outcomes compared to “Treatment as Usual” in which people accessed the existing support services available without intervention. Each location had its own focus or speciality population. According to Waegemakers Schiff and Rook (2012), by examining the approach in various political contexts, and with different populations, it had the multi-cultural dimensions needed for Canadian adoption of the Housing First approach. New data is published regularly, providing further insight into this initiative. In the video below one of the participants speaks about her experience in the study.
Having housing stability is a critical social determinant of health because housing instability is significantly associated with higher acute care use, having unmet health care needs, and engaging in problematic substance use (Harris et al., 2019). Having housing stability also helps to reduce the stigma and discrimination people face when experiencing homelessness, and improves their well-being and quality of life (Mejia-Lancheros et al., 2021). Analysis of the At Home / Chez Soi project suggests that neurocognitive impairment was high amongst the people in the study (Stergiopoulos et al., 2019), and that Housing First can be beneficial for reducing further harm to people with traumatic brain injuries (Mejia-Lancheros et al., 2020)
Certainly, Housing First has many benefits as an intervention for people experiencing homelessness, particularly amongst those who experience chronic homelessness related to mental health and/or addictions challenges. In the next video, Dr. John Ecker provides an overview of its five main principles and additional supports. The principles are discussed further in the animated video that follows.
In this video, Dr. John Ecker argues that Housing First is not a silver-bullet solution, but that it is effective for the large majority of people experiencing chronic homelessness. He outlines the five key principles that inform the design of Housing First and reviews the associated aspects, such as support team models and housing subsidies. Dr. Ecker reflects on published evaluations of the Housing First model, noting it is highly effective at long-term housing, reducing use of emergency services, and enhancing well-being, but is less successful in outcomes related to community integration, substance use reduction, and improvements in mental health functioning. He concludes that the rights-based foundations of Housing First, such as client choice and being low barrier, are increasingly being taken up in homelessness sector programs. This video is 5:14 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Is Housing First a solution to homelessness?
Housing First is an important evidence-based approach towards ending people’s homelessness, but as we have heard and will hear again, it is not a silver bullet that solves the problem entirely. In assessing Housing First, we must consider both its strengths and its weaknesses. For instance, research from Metro Vancouver has found the strengths of Housing First programs to be their ability to transition people into housing with individuals services, provide supports like rent subsidies, household goods, and connections to community resources, but also identified weaknesses related to eligibility criteria, limited financial subsidies, limited provider capacity, and workload burden for case workers (Canham, Wister, & O’Dea, 2019). In the next video Dr. Rebecca Schiff further explains the benefits and drawbacks of Housing First.
In this video, Dr. Rebecca Schiff argues that while Housing First has many good principles – such as consumer choice, meeting people where they are at, and self-determination – it is not the silver bullet that will solve homelessness because we still have further to go in adapting it to people’s unique support needs. This video is 2:32 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: Is Housing First a solution to homelessness?
We have looked at the principles of Housing First and how they are applied in practice, resulting in both positive and negative outcomes. What do you think are the biggest benefits and drawbacks of Housing First?
When we posed the question, “Is Housing First a solution to homelessness?” to Dr. Stephen Hwang and Dr. Tim Aubry, both researchers in the At Home / Chez Soi study, they gave us very similar responses. In short, Housing First is highly effective for individuals but does not have the capacity to address the social factors that create homelessness. They tell us the key is not to fix people, but to fix their situations.
In this video, Dr. Stephen Hwang discusses how Housing First is both a solution and not a solution to homelessness. At the individual level, research shows Housing First can be very effective for helping people achieve housing stability, particularly if they have mental health and/or substance use issues. However, Dr. Hwang argues that it is hazardous to think of Housing First as a solution to homelessness itself, because homelessness is fundamentally not caused by individual level vulnerabilities. While it may help people exit homelessness, Housing First does not address the structural forces and injustices that create it. He concludes that we need to examine our social, housing, and economic policies to find a solution. This video is 2:01 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Is Housing First a solution to homelessness?
In this video, Dr. Tim Aubry discusses the effectiveness of Housing First as a solution for housing the 15-20% of the homelessness population who have long-term histories. He argues that even though Housing First is intended to address chronic homelessness, its underlying approach – of providing rent supplements and tailored supports – makes it effective for addressing homelessness for other sub-populations as well. He provides the example of the Family Options Study conducted in the United States to show how Housing First principles can reduce poverty and help families get out of homelessness. Dr. Aubry argues that Housing First shows us the key is not to fix people, but to fix their situations. To do so, we need to give people who experience homelessness a sense of choice and agency back in their lives. Compared to other nations, Canada has not shown as strong a commitment to implementing Housing First, preferring instead to allow communities to determine their own approaches. He points to the success of Scandinavian countries in reducing homelessness, by making Housing First part of their national policies. This video is 5:45 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: Is Housing First a solution to homelessness?
As you consider the videos you just watched, we encourage you to take a moment and read Dr. Aubry’sanalysis of Housing First as a practical and policy relevant intervention.
Aubry, T. (2020). Analysis of housing first as a practical and policy relevant intervention: The current state of knowledge and future directions for research. European Journal of Homelessness, 14(1), 13-26.
At this point in our discussion, we hope that it is becoming clear Housing First is much more complicated than it may originally seem. The ten-year story of At Home / Chez Soi demonstrates how Housing First contributed to transformative change from ‘treatment first’ to ‘housing first’ for individuals with severe and persistent mental illness, but it needs to be enshrined in public policy to maximize its impacts (Nelson et al., 2020). Rather than blaming the person or the program when long-term housing stability is not achieved, it is important to consider the system-level forces that create and sustain poverty and inequities (Wallace, Pauly, Perkin, & Cross, 2019). Most notably, Housing First is limited by the availability of affordable housing and inadequate income assistance (Canham et al., 2019; Macnaughton et al., 2018).
In the video that follows Dr. Jonathan Greene explains that an early form of Housing First emerged in Toronto beginning in the 1980s, albeit without the wrap-around supports that are fundamental today. He has written that the changing urban landscape in the 1980s and 1990s also gave rise to new kinds of political activism, such as was seen in the City of Toronto as advocates defined the homelessness crisis as a direct effect of urban restructuring (Greene, 2014). Whether referring to the past or the present, there is a clear and continuous message that we cannot end homelessness with Housing First until we ensure there are mechanisms to address the wealth inequality gaps that make housing financially inaccessible to a large number of Canadians.
In this video, Dr. Jonathan Greene argues that the Housing First philosophy – including the right to housing and choice – is a good idea, but that it cannot solve homelessness by itself because there is nothing within it that mandates the development of affordable housing. Dr. Greene discusses programs that preceded Housing First, in Toronto in the 1980s, in which advocates argued for “housing, not hostels” demonstrating that the idea of rapidly housing people is not entirely new. He concludes that we must continue to evolve our understanding of Housing First, as even when all supports are put in place not every person will remain stably housed long-term. He challenges us to ask ourselves, “What else do we need to learn and know about these approaches?” This video is 4:19 in length and has closed captions available in English.
Key Takeaways – Dr. Jonathan Greene: Is Housing First a solution to homelessness?
Dr. Greene raises the important point that we still have much to learn about Housing First, and we continue to learn more as new research is conducted and published. For instance, we continue to learn about the benefits, such as that the presence of resources rather than risk factors as a key determinant in whether participants achieve housing stability (Aubry et al., 2021). Additionally analysis of the Vancouver At Home / Chez Soi data indicated that employment was associated with an increase in psychiatric recovery and had both immediate and longer-term outcomes (Yazdani et al., 2020).
As research results are published, we also continue to learn about the areas where further study and/or resources are needed. In a sample of participants with mental illness from the At Home / Chez Soi Toronto site, researchers did not find significant impact on primary care retention over time, suggesting that the program may need to be supplemented with additional efforts to connect people with health care (Whisler et al., 2021). Neighbourhood factors also need to be considered when matching a person with housing in Housing First programs, as long-term housing stability is a key determinant of well-being (Distasio et al., 2021).
There is also on-going analysis of the cost-benefit of providing Housing First. Using data from 937 participants in the five cities from the At Home / Chez Soi study, Latimer et al., (2017) calculated the average annual cost of services for those who were absolutely homeless or precariously housed, and not receiving Intensive Case Management [ICM] or Assertive Community Treatment [ACT] to be between $29,610 on the low end in Moncton and $58,972 on the high end in Toronto. To evaluate the cost-effectiveness of Housing First with ICM intervention, compared to treatment as usual, Latimer et al., (2019) recruited 1198 participants in the 5 At Home / Chez Soi study sites and found the intervention costs to be an average of $14,496 per person per year. In Calgary, researchers conducting pre-post assessments of Housing First programs estimated that for every $1 spent on Housing First, the savings from multi-sector usage could be between $1.17 and $2.84 (Jadidzadeh, Falvo, & Dutton, 2020). Dr. Stephen Gaetz and Dr. Tim Aubry explain the cost-benefits further in the next two videos.
In this video, Dr. Stephen Gaetz argues that the current emergency-based approach to managing homelessness is expensive and detrimental to individuals, families, and communities. He cites research on the financial costs of keeping someone homeless for a year, which range from $50,000 to $65,000 in cities across Canada, due to shelter use, hospital visits, and law enforcement. He concludes that Housing First is a better alternative. This video is 1:26 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: The cost of homelessness
In this video, Dr. Tim Aubry argues that the cost of ending people’s homelessness by implementing Housing First is very modest. In 2021, the estimated cost of providing supports and rent supplements ranges between $18,000 and $24,000 per person annually, depending on the type of supports provided. Having housing changes the way people tell their story and opens opportunities, such as for them to cook independently. Dr. Aubry notes that alongside rent supplements, it is important to increase overall financial supports such that people can purchase their own food and engage in ‘citizenship building’ by undertaking activities within their community. This video is 4:45 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: The modest costs and transformative benefits of Housing First
Longitudinal mixed-methods data from participants within the At Home / Chez Soi study, indicated social integration increased over time, and that the Housing First intervention may have led to larger social networks, increased social interest, and psychological integration compared to the ‘treatment as usual’ group (Kirst et al., 2020). For people living with mental illness, having interventions aimed at preventing chronic homelessness is a positive step towards strengthening social networks and community involvement, in addition to providing case management services to help with mental health recovery (Kerman, Sylvestre, Aubry, & Schütz, 2019). However, a systematic review of Housing First evaluations shows that there is inconsistency in the degree to which these programs are being implemented with community integration as an intended outcome (Marshall et al., 2020).
Dr. Aubry spoke about the importance of citizenship building and ensuring people had access to nutritional supports and meaningful activities once they are housed. His research shows that participants within a Housing First program who achieved housing stability had decreased use of psychiatric hospitals and increased use of food banks (Kerman, Sylvestre, Aubry, & Distasio, 2018). Housing First makes it possible for people to engage with food in ways they could not before – such as storing, preparing, cooking, and eating what they wish – which can have a positive impact on their health and well-being, but without financial resources they remain dependent on charitable food programs which may lead them to feel marginalized (Hainstock & Masuda, 2019).
Within Housing First programs, the types of support and extent to which people need them will vary by individual. Dr. Jeannette Waegemakers Schiff and Dr. Nick Kerman explain that while some people may require high levels of intervention, with continuous supports, others may just require housing in order to stabilize.
In this video, Dr. Jeannette Waegemakers Schiff argues that being housed is a human right and should not be conditional on meeting certain behavioural, emotional, and moral standards. She notes that the level of support people need alongside their housing will vary, with some people just needing housing and others requiring more intensive interventions. This video is 2:14 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: Is Housing First a solution to homelessness?
In this video, Dr. Nick Kerman argues that solutions to homelessness need to be tailored to individual and population specific needs. He discusses Housing First, which he says is highly effective for individuals who experience long-term homelessness related to serious mental illness, substance use issues, and/or other complex needs. However, Dr. Kerman notes, there are others experiencing homelessness who may not require the same intensive levels of support that accompany Housing First. He provides the example of families, who often are in financial need and would benefit most from affordable housing and rent subsidies. While Housing First programs may be highly effective for some, they may not be the best solution for others. This video is 1:59 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: Is Housing First a solution to homelessness?
Many researchers have advocated for the importance of choice, in both the videos and in their writing. Yet, the lack of affordable housing makes it difficult to provide people with choice in their housing. Interviews with service providers involved in Housing First suggest that high rents and low vacancy rates create delays in housing clients, may make them feel pressured to accept the first apartment they are offered, and have profound impact on their ability to operate the program and ensure fidelity to the Housing First model (Anderson-Baron & Collins, 2019). In the video that follows Dr. Tim Aubry weighs in on the importance of fidelity to the core Housing First principles.
In this video, Dr. Tim Aubry raises the concern that many Canadian communities are moving towards creating congregate quasi-institutional buildings, under the name of supportive housing, to group together people who have severe mental illness and/or addictions. He notes these programs are not in-line with the Housing First principles of client choice and recovery-orientation. This video is 3:48 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: The importance of choice in Housing First
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=646#h5p-39
A review of Housing First programs found that the majority self-reported high fidelity to the model (Nelson et al., 2017). However, capacity building is needed for communities implementing Housing First such as to help with clarifying principles, enhancing clinical skills and landlord engagement, client prioritization, and conducting fidelity assessments (Hasford et al., 2019).
Fidelity to the principles is important, but so too is adaptability. Different subpopulations have unique needs that are not always well served by the traditional Housing First model. For instance, adaptations may be needed for Indigenous persons (Bowra & Mashford-Pringle, 2021; Kidd, Thistle, Beaulieu, O’Grady, & Gaetz, 2019), women (Jadidzadeh & Falvo, 2019; Oudshoorn, Forchuk, Hall, Smith-Carrier, & Van Berkum, 2018), youth (Gaetz, Walter, and Story, 2021; Gaetz, O’Grady, Kidd, & Schwan, 2016; McParland, Rousseau-Thomas, & Waegemakers Schiff, 2019), seniors (Canham et al., 2018; Chung et al., 2018), and veterans (Bourque et al., 2017; Marsella, Forchuk, & Oudshoorn, 2020).
Dr. John Ecker and Dr. Stephen Gaetz speak about population-specific Housing First approaches in the videos below. Additional information on the unique needs of these subpopulations can be found in this book’s chapters on Indigenous Studies, Gender & Queer Studies, Child & Youth Studies, and Social Work respectively.
In this video, Dr. John Ecker discusses population-specific adaptations to the Housing First model. He begins by reviewing the Winnipeg site of the At Home / Chez Soi study, which focused on Housing First for Indigenous persons, and credits Jesse Thistle’s definition of Indigenous homelessness in Canada as being an excellent source of information for thinking about community and wellness needs. Dr. Ecker then discusses work that is being done by the Making the Shift project to adapt Housing First for youth. He notes that developmental needs require considerations about housing style, transitional lengths, supportive family relationships, and life skill building for young people. Finally, Dr. Ecker briefly discusses Housing First for women as being grounded in safety considerations, particularly for women experiencing domestic violence. This video is 4:55 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Population-specific approaches to Housing First
In this video, Dr. Stephen Gaetz identifies Housing First as an evidence-based best practice in homelessness policy and program design. He argues that it represents a shift in thinking towards seeing housing as a human right – that everybody deserves – and not as something that is earned by going through multiple steps. For Housing First to be implemented properly, Dr. Gaetz argues there needs to be fidelity to the model but also considerations of how it can evolve to suit the specific needs of populations such as Indigenous persons, women, families, and youth. This video is 3:35 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: Is Housing First a solution to homelessness?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=646#h5p-40
Fidelity to the Housing First model was a key consideration that emerged throughout several of the researcher videos. At the same time, Housing First needs to be flexible enough to meet the unique needs of populations such as Indigenous persons, women, youth, seniors, and veterans. Do you think we can achieve fidelity to the model and have flexibility? If so, how? If not, which do you feel is more important?
We end this section with the briefest of clips from Dr. Cheryl Forchuk because it leads us nicely into the final section on where we are heading with housing and homelessness policy today.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk succinctly frames Housing First as an important human-rights based strategy, although not the whole solution to homelessness. This video is 0:27 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Is Housing First a solution to homelessness?
In this section we asked you to consider the question, “Is Housing First a solution to homelessness?” We then set out on a winding journey to find the answer. We started in America with the work of Dr. Sam Tsemberis whose program Pathways to Housing has been greatly influential in developing the Canadian approach to Housing First. You may have been surprised (or not!) to learn that we actually had earlier forms of Housing First that developed around the time mass homelessness emerged in the 1980s and 1990s, but that the early forms had fewer intensive supports associated. Today our approach to Housing First is based on 5 principles and has wrap-around supports in the form of Assertive Community Treatment [ACT] or Intensive Case Management [ICM] depending on a person’s support needs. You can learn more about both of these treatment approaches in the chapter on Mental Health.
The evidence for Housing First in Canada comes largely from the ground-breaking At Home / Chez Soi study. While the research clearly points to the success of the model, it also identifies gaps in its ability to address underlying issues, like wealth inequality and the lack of affordable housing available in many cities across the country. Housing First has been shown to be cost effective, but also requires more work to ensure people feel connected to their communities after being housed. Fidelity to the Housing First principles is critically important, and with this in mind there have been many adaptations made to meet the needs of populations such as Indigenous persons, women, youth, seniors, and veterans.
Housing First is a big idea that, while seemingly quite simple, is actually rather complex. If you wrote down a response to the opening question, “Is Housing First a solution to homelessness?” we encourage you to return to your answer now and see whether your views have changed at all. While we know a lot about the effectiveness of Housing First, we still have a lot more to learn.
Click the link below to listen to all of the researchers answer the question “Is Housing First a solution to homelessness?” in audio format on our podcast!
29
We may have taken the scenic route, but we have arrived at the present day. So, what is happening with housing and homelessness policy today? Before you dive into the material that follows, we encourage you to take a moment and write down your response to this question. Perhaps you have been closely following the news as politicians make public announcements, reading social media posts that offer editorials on contemporary policies, or have no firsthand knowledge of what is currently happening in the housing political arena. If you feel well-versed in contemporary housing and homelessness policy, jot down a few key issues you are aware of, and if you are not, write down what you think might be happening based on everything you have learned up until this point. Remember that policy choices are always a reaction to the outcomes of policies that came before.
Your response in this section may be as brief or as long as you wish and is for your learning purposes only. It will not be seen by your instructor or fellow classmates.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=648#h5p-41
In 2017 Prime Minister Justin Trudeau announced that thirty years after withdrawing from creating social housing, the Federal government was returning to the proverbial table with the roll out of the 10-year $40 billion National Housing Strategy entitled, ““A Place to Call Home” (Government of Canada, 2017). Here is a brief newsclip of the announcement that was made at the time, in November 2017.
Following the announcement of the National Housing Act in 2017, the budget of $40 billion was increased to an allocation of over $70 billion. In 2018 we saw the release of “Reaching Home: Canada’s Homelessness Strategy,” which outlined the federal government’s commitment to reduce chronic homelessness by 50% over 10 years (Government of Canada, 2018). A year later, in 2019, the National Housing Strategy Act was passed (Government of Canada, 2019) making the right to housing a key part of our national housing law. Collectively these represent positive steps towards ending homelessness in Canada, but as the saying goes “show me, don’t tell me.” We are still in the early years of enacting these strategies and legislation pieces. While the commitments are a good starting point, they are just that – a starting point. In the next set of videos Dr. Erin Dej and Dr. Jacqueline Kennelly discuss this further.
In this video, Dr. Erin Dej shares optimism that Canada is experiencing a new wave of investment, albeit rolling out slowly, and a federal return to affordable housing through the National Housing Strategy created in 2017 and the National Housing Strategy Act in passed in 2019 that included a declaration of the right to housing. This video is 1:02 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: A new wave of federal housing policy in Canada
In this video, Dr. Jacqueline Kennelly argues that we need more affordable housing. She credits the National Housing Strategy as being a starting point for the Federal government’s return to housing, after their withdrawal in the 1990s. However, Dr. Kennelly notes that the Strategy has been slow to roll out and there is concern over the long-term commitment to affordability on behalf of landlords and builders who receive these funds. This video is 1:14 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: We need more affordable housing
One of the most impactful elements of the new Federal approach is the declaration of the right to housing. In the National Housing Strategy Act, the Government of Canada (2019) declares to:
In the next two videos, Dr. Stephen Gaetz and Dr. Bernie Pauly discuss the importance of understanding housing as a human right.
In this video, Dr. Stephen Gaetz argues that decades of neglecting affordable housing in Canada has created a massive issue that requires, “all hands on deck.” He sites the National Housing Strategy and legislation as being positive developments at the federal level but pushes for a move towards progressive realization of the right to housing that includes more investments and a focus on prevention. This video is 0:43 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: What is happening with housing and homelessness policy today?
In this video Dr. Bernadette (Bernie) Pauly argues that there are some universal basic human needs, such as for safe, secure, and adequate housing, access to food, an adequate income, and access to community. Beyond these fundamentals, she argues what people need is individualized and there is no “one size fits all” model of housing and supports that will work for everyone. She argues that men, women, and LGBTQ2S+ populations will need different services and supports, based on their unique and individualized needs. Dr. Pauly concludes that if we could focus on a spectrum of housing that is informed and directed by people with lived experience, we would get a radical shift in how we think about housing and support as being self-determined to meet people’s needs. This video is 3:44 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: Housing as a human right
Dr. Gaetz (2020) has written that Canada is in the beginning stages of a move towards prevention. Much of this work hinges on housing being considered a human right. For instance, Housing First operates on the premise that housing is a right but review of the literature suggests that terms related to rights are seldom referenced, and when they are included often lack detail and justification (Collins & Stout, 2021). Saying that housing is a right is different than enacting housing as a human right. We need to see these changes in action.
As part of a strategic move towards implementation, The National Right to Housing Network published three reports in 2021. These reports focused on how to implement the right to adequate housing under the National Housing Strategy Act (Porter, 2021), implement the right to housing in Canada and expand the National Housing Strategy (Biss & Raza, 2021), and implement the right to housing for women, girls, and gender diverse people in Canada (Schwan, Vaccaro, Reid, & Ali, 2021).
In this section’s featured reading from the Centre for Equality Rights in Accommodation and The National Right to Housing Network, we take a closer look at how Canada can fulfill its commitments to human rights under the National Housing Strategy Act.
Centre for Equality Rights in Accommodation and The National Right to Housing Network. (2021). The rights to life, protection of the home & nondiscrimination in Canada: Assessing the housing & homelessness crisis in accordance with Articles 2, 6, 17 & 26 of the ICCPR. Canada: CERA & NRHN.
Following international frameworks, Canada has created legislation that formalizes its commitment to housing as a human right. Why do you think it took until 2019 for Canada to recognize that all humans have a right to be suitably and securely housed?
As you consider this question, of why Canada has only now begun to formalize the right to housing, it is useful to reflect back on the history that has brought us to this point. In the next video, Dr. Jonathan Greene reviews the history and raises additional questions about whether our current strategy goes far enough in making a long-term sustainable impact.
In this video, Dr. Jonathan Greene argues that we must understand the history of housing policy in Canada to understand current housing policy. He notes that in the 1960s through the early-1980s there were federal, provincial, and municipal housing interventions, but that by 1993 the federal government had stopped creating new social housing. In the mid-1990s the devolution of housing meant that responsibility for new social housing went from the federal government down to provinces, and in Ontario under Premier Mike Harris was further downloaded to municipalities. Today, Dr. Greene notes, the National Housing Strategy is providing billions of dollars towards the creation of affordable housing but is projected to have limited impact on those in core housing need. Notably, he cites reports from the Financial Accountability Office in Ontario that indicates new affordable housing developments will offset the existing housing that is being lost due to lack of upkeep, resulting in the same proportion of low-income people without housing in 2027-28 as in 2021. This video is 4:14 in length and has closed captions available in English.
Key Takeaways – Dr. Jonathan Greene: What is happening with housing and homelessness policy today?
The right to housing means not only that the government has an obligation to ensure people have access to housing, but that the housing must also be affordable, safe, and secure. It is important we consider the impact the National Housing Strategy will have on people experiencing chronic homelessness, as well as those who are at-risk or in core housing need. To learn more about core housing need, consider these two brief videos from the Canadian Mortgage and Housing Renewal Corporation.
It is important that as time passes, and we get further away from the announcement of these large federal initiatives like the housing and homelessness strategies, that we maintain the momentum. We do this, in large part, by keeping pressure on the government and ensuring their actions match the commitments that they made. As Dr. Tim Aubry explains in the video that follows, it is easy to shift the focus towards homeownership, which is important but overshadows people who cannot afford housing because they live in deep poverty. We must also hold our elected officials accountable, as Dr. Naomi Nichols subsequently explains.
In this video, Dr. Tim Aubry discusses the introduction of the National Housing Strategy in 2017 as a means for building new affordable housing and repairing the existing stock. He notes that the rising cost of housing is an issue that has overshadowed homelessness, particularly as it relates to first-time home buyers. The issue of rising housing costs impacts more people, so it is a more prominent topic of political discussions. He concludes that we need to find a way to increase affordable housing, whether for rental or private market, such that the supply meets the demand. This video is 2:35 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: What is happening with housing and homelessness policy today?
In this video, Dr. Naomi Nichols discusses systems planning at the level of city councillors, service provision, and community consultants. She argues that city councillors must recognize that placing people in emergency shelters is neither a housing-led approach nor a solution to homelessness, and that they should be held accountable for the responses to homelessness implemented in their communities. Dr. Nichols further notes that at the service provision level, the lack of affordable housing stock means that service providers are being directed to fill out forms and rationalize resource distribution, but without ultimately having the desired effects of reducing waitlist times and homelessness. Finally, she urges communities to think very carefully and critically about the advice they receive from consultants. In recent years some communities have been given damaging advice, such as to make shelters less comfortable, remove arts-based programming, and compare themselves to other communities’ outcomes without considerations of how each are unique. This video is 6:14 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Systems planning and the role of consultants
Contemporary housing and homelessness policies reflect the socio-political desire to change our past approaches, but in order to be effective they must be critically thought through and carefully executed. Bringing people together, whether as part of the Advisory Committee on Homelessness (2018) or through the National Conference on Ending Homelessness (Paradis, 2016), reflects positive community-building initiatives that are occurring within the homelessness sector, as Dr. Nick Falvo explains below. However, even with the increased collaborative mindsets, Dr. Sean Kidd reminds us that we are still seeing homelessness fall through interdepartmental government cracks.
In this video, Dr. Nick Falvo discusses the large community of people working together to end homelessness in Canada. He points to the annual “National Conference on Ending Homelessness” held every fall as one example, in which 1500 service providers, non-profit leaders, researchers, and people with lived experience come together. While Dr. Falvo notes it is bad that homelessness still exists as an issue to be addressed, he is optimistic about this sector’s increased ability to manage resources, gather data, connect outcomes to funding, and communicate key messages to the media. This video is 1:39 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Falvo: What is happening with housing and homelessness policy today?
In this video, Dr. Sean Kidd reflects on how Canadian governments operate in a way that creates barriers to addressing homelessness. He notes that the turnover of political parties and agendas, siloing between Ministries and levels of government, and the way decisions are made is not inline with addressing homelessness. Dr. Kidd argues that we need to find a way of restructuring our government so issues like homelessness do not fall between departmental, governmental level, and party agenda cracks. This would require a consensus and putting policy in place that could not be dismantled with changing administrations. He notes that some organizations, like “Making the Shift” and the “Canadian Alliance to End Homelessness” have begun undertaking this kind of systems-level coordination. Dr. Kidd concludes that the COVID-19 pandemic has demonstrated the interconnected nature of our society and that we must recognize how issues like housing vulnerability and social isolation impact our communities, families, and ourselves. He argues that we must reject an “us and them” mentality, but rather collectively recognize that “this is us,” and that we are all facing these issues together. This video is 3:48 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: Homelessness as an issue that falls through government cracks
It is important as you are learning about the new initiatives occurring in Canada, and the challenges that accompany them, that you also remember the fundamental lesson that when we talk about homelessness, we are talking about something that happens to people. This means that while access to housing is key, we have to also remember the principles of Housing First that tell us having choice and access to supports are fundamental. Dr. Jeff Karabanow explains why there is a need for financial supports to help people as they become stabilized in housing.
In this video, Dr. Jeff Karabanow discusses the idea of basic income supports. He argues that there has been a political movement over the past 40 to 50 years, exploring the concept that providing basic income allows people a foundation to heal from traumatic experiences and return to participation in civil society. Dr. Karabanow notes that the Canada Emergency Response Benefit [CERB] given during COVID-19 demonstrated the safety and security benefits that basic income can provide. This video is 1:42 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: The need for guaranteed income supports
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=648#h5p-42
The lack of affordable housing has been an ongoing problem in Canada, dating back to the federal government’s decision to stop funding social housing in the 1980s and 1990s. At the same time, the right to housing declaration included in the National Housing Strategy Act means that the government has a duty to ensure Canadians have access to good quality affordable housing. What are some specific measures you think the government could take to increase affordable housing and reduce barriers to accessing it?
With rapidly increasing housing prices, we are witnessing an equally problematic rise in eviction practices that push people out of their housing so that it can be rented to someone else at a higher rate. Dr. Naomi Nichols introduces the concept of ‘renovictions’ which is explored further in the CBC News video that follows.
In this video Dr. Naomi Nichols argues that in Canada we have experienced a rapid increase in the cost of private property within the housing market, leading to an increase in rent as well. Consequently, some renters have been pushed out of their housing, through the use of renovictions. She concludes that we as a society have not considered the negative effects of these raising prices on individuals who are unable to participate in the housing market and do not benefit from private property ownership. This video is 1:00 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: The price of housing and rise of evictions
Illegal and underhanded eviction practices have the most detrimental impact on people who lack the resources to advocate for themselves. For instance, people who use drugs commonly experience housing vulnerability. In one study conducted in Vancouver’s Downtown Eastside, participants who used drugs were found to have high rates of unlawful evictions resulting in homelessness, without support of tenancy laws and dispute resolution mechanisms (Fleming et al., 2019). The authors of this study argue that policy reforms are needed to address the high rates of these unlawful evictions, in order to increase these individuals’ housing security (Fleming et al., 2019).
Canada has made great progress towards increasing access to housing and decreasing homelessness, but the right to housing is not truly realized until every person has safe, secure, and affordable housing. We conclude this section with a summary from Dr. John Ecker, in which he highlights many of the key points that have emerged.
In this video, Dr. John Ecker discusses the 2017 National Housing Strategy as a hopeful recommitment to building affordable housing in Canada, by recognizing the need for stronger federal investments and partnership-building between the federal and provincial / territorial governments. He cites the work of Professor David Hulchanski, who states that Federal housing policy has traditionally focused on private home ownership, to the neglect of those who cannot afford to purchase it. Dr. Ecker identifies current challenges with policies that fail to limit the actions of landlords, such as around raising rents and eviction practices. He also discusses inclusionary zoning as one policy that has the potential to increase housing stock, when used equitably to designate a percentage of new developments as affordable housing. Here he refers to the Canadian Housing and Mortgage Corporation’s definition of spending less than 30% on housing as the benchmark for affordability. Dr. Ecker concludes by arguing the need to increase minimum wage and social assistance rates, to correspond with the increased costs of housing. This video is 7:21 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Contemporary housing policies
In this section, we examined the question, “What is happening with housing and homelessness policy today?” We began with the federal government’s return to building affordable housing in 2017, with the announcement of the National Housing Strategy, which was followed shortly thereafter by the 2018 National Homelessness Strategy, and the 2019 National Housing Strategy Act. These initiatives represent important steps forward in Canada’s efforts to address homelessness but are still in the early stages of implementation. Most notably, this time period reflects a shift towards viewing affordable, safe, and secure housing as a basic human right that experiencing homelessness violates.
While it is positive that the Federal government has renewed its commitment to providing affordable housing, it is imperative that the public continue to hold elected officials responsible for meeting their outlined objectives. Collaborative efforts, such as advisory committees and national conferences are key to working together, but we must also attend to the misalignments that can occur if homelessness is not made a priority for all governmental ministries. We concluded this section by considering the additional supports that are needed, such as guaranteed income and eviction protections, to ensure people are able not only to get housing but to keep it long-term.
Click the link below to listen to all of the researchers answer the question “What is happening with housing and homelessness policy today?” in audio format on our podcast!
30
Tish
We met Tish at the beginning of the chapter. They keep mostly to themselves and when approached can be aggressive and challenging. The police and social service workers in the area are familiar with their circumstances and have referred them to many local support agencies over the years. The lack of affordable or subsidized housing policies in the province have had direct effects on their living situation. Tish’s uncontrollable anti-social behaviour and the policies of various agencies have come into direct conflict many times leading to fewer and fewer available resources. They are currently in a desperate, chronic situation with few options. Their health is failing, their use of the Emergency room is high, and their physical and mental well-being is severely compromised.
However, to more fully understand Tish’s situation, we need to move beyond their individual situation and look at the systems challenges. Consider what we have learned from Dr. Hwang and Dr. Aubry- we don’t need to fix people; we need to fix situations.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=916#h5p-87
31
In this chapter we took you back through history to better understand homelessness and housing policy over time. As we noted throughout, the decisions made at one point in time are often in response to decisions that came before. While it may seem apparent that the solution to homelessness is to have more housing, providing that housing has not always been simple. Throughout the time periods we considered in this chapter, from the post-World War Two era up until the present day, politics have shaped the availability of affordable housing.
At the start of the chapter, we introduced you to the composite character Tish, whose access to housing and supports were directed by policy decisions made and enacted outside her control. The scenario was presented as an entry point into thinking about the complexity of housing and homelessness policies. We returned to this story at the end to demonstrate how it can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “What housing policy existed in the past?” To understand the current homelessness crisis, it was important to begin our journey in the post World War Two era. During this period wartime housing was created for people working in the war-industry and later for soldiers. We learned that there was strong social infrastructure in place in the 1960s and 1970s, but that these started to wane with the recession in the 1980s. At that time the federal government began to pull back from funding social housing and in the 1990s withdrew completely, downloading the responsibility to provinces (and in Ontario, further downloading to municipalities). It was in the 1980s that we began to hear about the problem of mass homelessness for the first time, coinciding with the rise of neoliberal politics and great wealth inequality.
Next we asked, “Is Housing First a solution to homelessness?” Just as the name suggests, this approach entails providing people with housing before anything else. The idea of housing people and moving them off the street emerged alongside the homelessness crisis in the 1980s and 1990s, but Housing First was formalized as a program by Dr. Sam Tsemberis’ team at Pathways to Housing in New York. In Canada, Housing First was evaluated with the multi-site At Home / Chez Soi study and has subsequently become a widely adopted policy and programmatic approach. In asking whether it is a solution, we heard multiple times that while it is one solution, it is not the whole solution because it does not address the underlying causes of homelessness, such as the lack of affordable housing and adequate income supports. We further considered the importance of fidelity to the original model and weighed it against the need to be flexible and adaptable to the needs of different populations.
Finally we asked, “What is happening with housing and homelessness policy today?” In this section, we considered where we are now, with a look to where we might be going in the future. Namely, the 2017 National Housing Strategy, 2018 National Homelessness Strategy, and 2019 National Housing Strategy Act signalled a strong federal commitment to ending homelessness, with the declaration of housing as a human right. While this is a positive step, sustained political will is needed to ensure that the planning and strategy translate into action. The commitment to housing people and ending homelessness long-term will require collaboration to ensure it does not fall through governmental cracks, and that we see the implementation of wrap-around supports like guaranteed income and strengthened eviction prevention measures.
To understand our current housing and homelessness landscape, it was important to take a moment and step back in time. We hope that this brief journey helped to inform your understanding of where we have come from as a country, where we are now, and where we might be going in the future.
32
Here are some additional resources you may want to check out!
33
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
34
Advisory Committee on Homelessness. (2018). Final Report. Canada: Employment and Social Development Canada.
Anderson-Baron, J. T., & Collins, D. (2019). “Take whatever you can get”: Practicing Housing First in Alberta. Housing Studies, 34(8), 1286–1306. https://doi.org/10.1080/02673037.2018.1535055
Aubry, T. (2020). Analysis of housing first as a practical and policy relevant intervention: The current state of knowledge and future directions for research. European Journal of Homelessness, 14(1), 13-26. https://www.feantsaresearch.org
Aubry, T., Agha, A., Mejia-Lancheros, C., Lachaud, J., Wang, R., Nisenbaum, R., … Hwang, S. W. (2021). Housing trajectories, risk factors, and resources among individuals who are homeless or precariously housed. The Annals of the American Academy of Political and Social Science, 693(1), 102–122. https://doi.org/10.1177/0002716220987203
Biss, M., & Raza, S. (2021). Implementing the right to housing in Canada: Expanding the national housing strategy. Canada: The National Right to Housing Network. https://housingrights.ca/wp-content/uploads/NRHN-OFHA-Expanding-the-NHS-2021.pdf
Bourque, J., VanTil, L., Nadeau, J., LeBlanc, S. R., Ebner-Daigle, J., Gibbons, C., & Darte, K. (2017). Physical health status of homeless veterans in Canada: A cross-sectional study. Journal of Military, Veteran and Family Health, 3(2), 4–11. https://doi.org/10.3138/jmvfh.4251
Bowra, A., & Mashford-Pringle, A. (2021). More than a structure: Exploring the relationship between Indigenous homemaking practices and wholistic wellbeing. Wellbeing, Space and Society, 2. https://doi.org/10.1016/j.wss.2020.100007
Canham, S. L., Battersby, L., Fang, M. L., Wada, M., Barnes, R., & Sixsmith, A. (2018). Senior services that support Housing First in Metro Vancouver. Journal of Gerontological Social Work, 61(1), 104–125. https://doi.org/10.1080/01634372.2017.1391919
Canham, S. L., Wister, A., & O’Dea, E. (2019). Strengths, weaknesses, opportunities, and threats to Housing First in Metro Vancouver. Evaluation and Program Planning, 75, 69–77. https://doi.org/10.1016/j.evalprogplan.2019.05.004
Carroll, B. W. (1989). Post-war trends in Canadian housing policy. Urban History Review / Revue d’histoire urbaine, 18(1), 64–74. https://doi.org/10.7202/1017825ar
Centre for Equality Rights in Accommodation and The National Right to Housing Network. (2021). The rights to life, protection of the home & nondiscrimination in Canada: Assessing the housing & homelessness crisis in accordance with Articles 2, 6, 17 & 26 of the ICCPR. Canada: CERA & NRHN. ICCPRSubmission-NRHN-CERA-2021.pdf (housingrights.ca)
Chisholm, S., & Hulchanski, D. (2019). Canada’s housing story. In D. Maclennan, H. Pawson, K. Gibb, S. Chisholm, & D. Hulchanski (Eds.). SF 21: Shaping Futures Changing the Housing Story Final Report. University of Glasgow: Policy Scotland. canadas-housing-story-2019-chap-4.pdf (neighbourhoodchange.ca)
Chung, T. E., Gozdzik, A., Palma Lazgare, L. I., To, M. J., Aubry, T., Frankish, J., Hwang, S. W., & Stergiopoulos, V. (2018). Housing First for older homeless adults with mental illness: a subgroup analysis of the At Home/Chez Soi randomized controlled trial. International Journal of Geriatric Psychiatry, 33(1), 85–95. https://doi.org/10.1002/gps.4682
Collins, D., & Stout, M. (2021). Does Housing First policy seek to fulfil the right to housing? The case of Alberta, Canada. Housing Studies, 36(3), 336–358. https://doi.org/10.1080/02673037.2019.1707782
Dej, E. & Ecker, J. (2018). “Homelessness & precarious housing in Canada: Where we have been and where we are going.” Public Sector Digest.
Distasio, J., Adair, C. E., Hwang, S., Hinds, A., Kopp, B. C., Aubry, T., … Kaufman, A. F. (2021). Exploring the relationship between neighbourhood quality (NQ) and housing stability among formerly homeless individuals with mental illness in housing first. Wellbeing, Space and Society, 2, 100008–. https://doi.org/10.1016/j.wss.2020.100008
Evans, J., & Masuda, J. R. (2020). Mobilizing a fast policy fix: Exploring the translation of 10-year plans to end homelessness in Alberta, Canada. Environment and Planning. C, Politics and Space, 38(3), 503–521. https://doi.org/10.1177/2399654419884581
Fleming, T., Damon, W., Collins, A. B., Czechaczek, S., Boyd, J., & McNeil, R. (2019). Housing in crisis: A qualitative study of the socio-legal contexts of residential evictions in Vancouver’s Downtown Eastside. The International Journal of Drug Policy, 71, 169–177. https://doi.org/10.1016/j.drugpo.2018.12.012
Gaetz, S. (2010). The struggle to end homelessness in Canada: How we created the crisis, and how we can end it. Open Health Services and Policy Journal, 3, 21-26. Editorial: How to End Homelessness in Canada: How we Created the Crisis, and How we can End it (homelesshub.ca)
Gaetz, S. (2020). Making the prevention of homelessness a priority: The role of social innovation. The American Journal of Economics and Sociology, 79(2), 353–381. https://doi.org/10.1111/ajes.12328
Gaetz, S., O’Grady, B., Kidd, S., & Schwan, K. (2016). Without a home: The national youth homelessness survey. Toronto: Canadian Observatory on Homelessness Press.
Gaetz, S., Walter, H. and Story, C. (2021). THIS is Housing First for youth. Part 1 – program model guide. Toronto, ON: Canadian Observatory on Homelessness Press.
Government of Canada. (2017). A place to call home: Canada’s national housing strategy. Government of Canada, Ottawa. Canada’s National Housing Strategy (placetocallhome.ca)
Government of Canada. (2018). Reaching home: Canada’s homelessness strategy directives. Government of Canada, Ottawa. Reaching Home: Canada’s Homelessness Strategy Directives – Canada.ca
Government of Canada. (2019). National housing strategy act. Government of Canada, Ottawa. National Housing Strategy Act (justice.gc.ca)
Greene, J. (2014). Urban restructuring, homelessness, and collective action in Toronto, 1980–2003. Urban History Review, 43(1), 21–37. https://doi.org/10.7202/1030805ar
Hainstock, M., & Masuda, J. R. (2019). “We have a roof over our head, but we have to eat too:” Exploring shifting foodscapes from homelessness into Housing First in Kingston, Ontario. Health & Place, 59, 102197–102197. https://doi.org/10.1016/j.healthplace.2019.102197
Harris, M., Gadermann, A., Norena, M., To, M., Hubley, A. M., Aubry, T., Hwang, S. W., & Palepu, A. (2019). Residential moves and its association with substance use, healthcare needs, and acute care use among homeless and vulnerably housed persons in Canada. International Journal of Public Health, 64(3), 399–409. https://doi.org/10.1007/s00038-018-1167-6
Hasford, J., Nelson, G., Worton, S. K., Macnaughton, E., MacLeod, T., Piat, M., Tsemberis, S., Stergiopoulos, V., Distasio, J., Aubry, T., & Goering, P. (2019). Knowledge translation and implementation of housing first in Canada: A qualitative assessment of capacity building needs for an evidence-based program. Evaluation and Program Planning, 75, 1–9. https://doi.org/10.1016/j.evalprogplan.2019.03.001
Jadidzadeh, A., & Falvo, N. (2019). Patterns of exits from housing in a homelessness system of care: the case of Calgary, Alberta. Housing Studies, 34(1), 66–91. https://doi.org/10.1080/02673037.2018.1432755
Jadidzadeh, A., Falvo, N., & Dutton, D. J. (2020). Cost savings of Housing First in a non-experimental setting. Canadian Public Policy, 46(1), 23–36. https://doi.org/10.3138/cpp.2019-017
Kerman, N., Sylvestre, J., Aubry, T., & Distasio, J. (2018). The effects of housing stability on service use among homeless adults with mental illness in a randomized controlled trial of housing first. BMC Health Services Research, 18(1), 190–190. https://doi.org/10.1186/s12913-018-3028-7
Kerman, N., Sylvestre, J., Aubry, T., & Schütz, C. G. (2019). Predictors of mental health recovery in homeless adults with mental illness. Community Mental Health Journal, 55(4), 631–640. https://doi.org/10.1007/s10597-018-0356-3
Kidd, S., Thistle, J., Beaulieu, T., O’Grady, B., & Gaetz, S. (2019). A national study of Indigenous youth homelessness in Canada. Public Health (London), 176, 163–171. https://doi.org/10.1016/j.puhe.2018.06.012
Kirst, M., Friesdorf, R., Ta, M., Amiri, A., Hwang, S. W., Stergiopoulos, V., & O’Campo, P. (2020). Patterns and effects of social integration on housing stability, mental health and substance use outcomes among participants in a randomized controlled Housing First trial. Social Science & Medicine (1982), 265, 113481–113481. https://doi.org/10.1016/j.socscimed.2020.113481
Latimer, E. A., Rabouin, D., Cao, Z., Ly, A., Powell, G., Adair, C. E., … Veldhuizen, S. R. (2019). Cost-effectiveness of Housing First Intervention With Intensive Case Management Compared With Treatment as Usual for Homeless Adults With Mental Illness: Secondary Analysis of a Randomized Clinical Trial. JAMA Network Open, 2(8), e199782–e199782. https://doi.org/10.1001/jamanetworkopen.2019.9782
Latimer, E. A., Rabouin, D., Cao, Z., Ly, A., Powell, G., Aubry, T., Hwang, S. W.,… Goering, P. N. (2017). Costs of services for homeless people with mental illness in 5 Canadian cities: a large prospective follow-up study. CMAJ Open, 5(3), E576–E585. https://doi.org/10.9778/cmajo.20170018
Marsella, O., Forchuk, C., & Oudshoorn, A. (2020). Exploring harm reduction among Canadian veterans experiencing homelessness. Journal of Military, Veteran and Family Health, 6(2), 17–25. https://doi.org/10.3138/jmvfh-2019-0042
Marshall, C. A., Boland, L., Westover, L. A., Marcellus, B., Weil, S., & Wickett, S. (2020). Effectiveness of interventions targeting community integration among individuals with lived experiences of homelessness: A systematic review. Health & Social Care in the Community, 28(6), 1843–1862. https://doi.org/10.1111/hsc.13030
Macnaughton, E., Nelson, G., Worton, S. K., Tsemberis, S., Stergiopoulos, V., Aubry, T., … Goering, P. (2018). Navigating complex implementation contexts: Overcoming barriers and achieving outcomes in a national initiative to scale out Housing First in Canada. American Journal of Community Psychology, 62(1-2), 135–149. https://doi.org/10.1002/ajcp.12268
McParland, K., Rousseau-Thomas, J., & Waegemakers Schiff, J. (2019). A critical review of research and policy in youth-focussed Housing First. Canadian Review of Social Policy (1987), 79, 50–. https://crsp.journals.yorku.ca/index.php/crsp/article/view/40333
Mejia-Lancheros, C., Lachaud, J., Stergiopoulos, V., Matheson, F. I., Nisenbaum, R., O’Campo, P., & Hwang, S. W. (2020). Effect of Housing First on violence-related traumatic brain injury in adults with experiences of homelessness and mental illness: findings from the At Home/Chez Soi randomised trial, Toronto site. BMJ Open, 10(12), e038443–e038443. https://doi.org/10.1136/bmjopen-2020-038443
Mejia-Lancheros, C., Lachaud, J., Woodhall-Melnik, J., O’Campo, P., Hwang, S. W., & Stergiopoulos, V. (2021). Longitudinal interrelationships of mental health discrimination and stigma with housing and well-being outcomes in adults with mental illness and recent experience of homelessness. Social Science & Medicine (1982), 268, 113463–113463. https://doi.org/10.1016/j.socscimed.2020.113463
Nelson, G., Aubry, T., Tsemberis, S., & Macnaughton, E. (2020). Psychology and public policy: The story of a Canadian Housing First project for homeless people with mental illness. Canadian Psychology = Psychologie Canadienne, 61(3), 257–268. https://doi.org/10.1037/cap0000206
Nelson, G., Caplan, R., MacLeod, T., Macnaughton, E., Cherner, R., Aubry, T., … Goering, P. (2017). What happens after the demonstration phase? The sustainability of Canada’s At Home/Chez Soi Housing First programs for homeless persons with mental illness. American Journal of Community Psychology, 59(1-2), 144–157. https://doi.org/10.1002/ajcp.12119
Oudshoorn, A., Forchuk, C., Hall, J., Smith-Carrier, T., & Van Berkum, A. (2018). An evaluation of a Housing First program for chronically homeless women. Journal of Social Inclusion, 9(2), 34–. https://doi.org/10.36251/josi.136
Paradis, E. (2016). Outsiders within: Claiming discursive space at national homelessness conferences in Canada. Social Inclusion, 4(4), 97–107. https://doi.org/10.17645/si.v4i4.670
Porter, B. (2021). Implementing the right to adequate housing under the national housing strategy act: The international human rights framework. Canada: The National Right to Housing Network. NRHN OFHA Report Cover 2021 (housingrights.ca)
Schwan, K., Vaccaro, M. E., Reid, L., & Ali, N. (2021). Implementation of the right to housing for women, girls, and gender diverse people in Canada. Canada: The National Right to Housing Network. Microsoft Word – EN_CHRC_13.docx (housingrights.ca)
Stergiopoulos, V., Naidu, A., Schuler, A., Bekele, T., Nisenbaum, R., Jbilou, J., … Rourke, S. B. (2019). Housing stability and neurocognitive functioning in homeless adults with mental illness: A subgroup analysis of the At Home/Chez Soi study. Frontiers in Psychiatry, 10, 865–865. https://doi.org/10.3389/fpsyt.2019.00865
Urbanoski, K., Veldhuizen, S., Krausz, M., Schutz, C., Somers, J. M., Kirst, M., … Goering, P. (2018). Effects of comorbid substance use disorders on outcomes in a Housing First intervention for homeless people with mental illness. Addiction (Abingdon, England), 113(1), 137–145. https://doi.org/10.1111/add.13928
Waegemakers Schiff, J., & Rook, J. (2012). Housing first: Where is the evidence? Toronto: Homeless Hub.
Wallace, B., Pauly, B., Perkin, K., & Cross, G. (2019). Where’s the housing? Housing and income outcomes of a transitional program to end homelessness. Journal of Poverty, 23(2), 161–178. https://doi.org/10.1080/10875549.2018.1549185
Whisler, A., Dosani, N., To, M. J., O’Brien, K., Young, S., & Hwang, S. W. (2021). The effect of a Housing First intervention on primary care retention among homeless individuals with mental illness. PloS One, 16(2), e0246859–e0246859. https://doi.org/10.1371/journal.pone.0246859
Woolley, E. (2015). Why wasn’t homelessness a social problem until the 1980s? Homeless Hub. https://www.homelesshub.ca/blog/why-wasnt-homelessness-social-problem-until-1980s
Yazdani, K., Nikoo, M., Sayre, E. C., Choi, F., Jang, K., & Krausz, R. M. (2020). The impact of employment on recovery among individuals who are homeless with severe mental illness in the Vancouver At Home/Chez Soi trial. Social Psychiatry and Psychiatric Epidemiology, 55(12), 1619–1627. https://doi.org/10.1007/s00127-020-01887-9
IV

Mental Health and Public Health Studies are fields that focus on the mental and physical well-being of individuals and groups. Within this part of the book, we examine the impacts of mental health and public health as they relate to the contributing factors and outcomes for persons experiencing homelessness in Canada. We begin with a chapter on Mental Health, followed by a chapter on Public Health. As you work through these chapters, you are encouraged to critically reflect upon what these disciplines contribute to our knowledge and understanding of homelessness in Canada.
Perhaps as you read this, you are considering working in a career within the fields of Mental Health or Public Health, such as a Psychiatrist, Harm Reduction Worker, or Public Health Nurse. The chapters in this section are designed to help you think critically about some the questions you may encounter in these fields of employment. Understanding homelessness will help you navigate situations and choices you have to make. Consider, for example, a scenario in which a woman has had her children removed by Child Protection Workers, because she is struggling with severe mental illness. As a means of coping with the loss of custody, she has begun to self-medicate with alcohol and injection drug use. As a Psychiatrist you may meet this woman in your clinical practice. What will you recommend to help improve her mental health and well-being? As a Harm Reduction Worker or Public Health Nurse, you may meet this woman to help ensure she is using substances as safely as she can, or you may meet her in an emergency room following an overdose episode. What connections will you make between the loss of her children, diagnosed mental illness, and use of substances? What supports will you be able to offer her with this insight?
Before you begin, pause to consider how you would respond in each of the roles of the scenario above. With the knowledge you currently have about homelessness in Canada, why do you think mental health and public health are commonly intersecting fields? In the scenario, what might you do to prevent this woman’s mental and physical health from deteriorating, because of her circumstances?
You are encouraged to keep this scenario in your mind as you read through the next two chapters and ask yourself whether any of your responses change, or are reaffirmed, after learning more about what Mental Health and Public Health Studies can teach us about homelessness in Canada.
IV
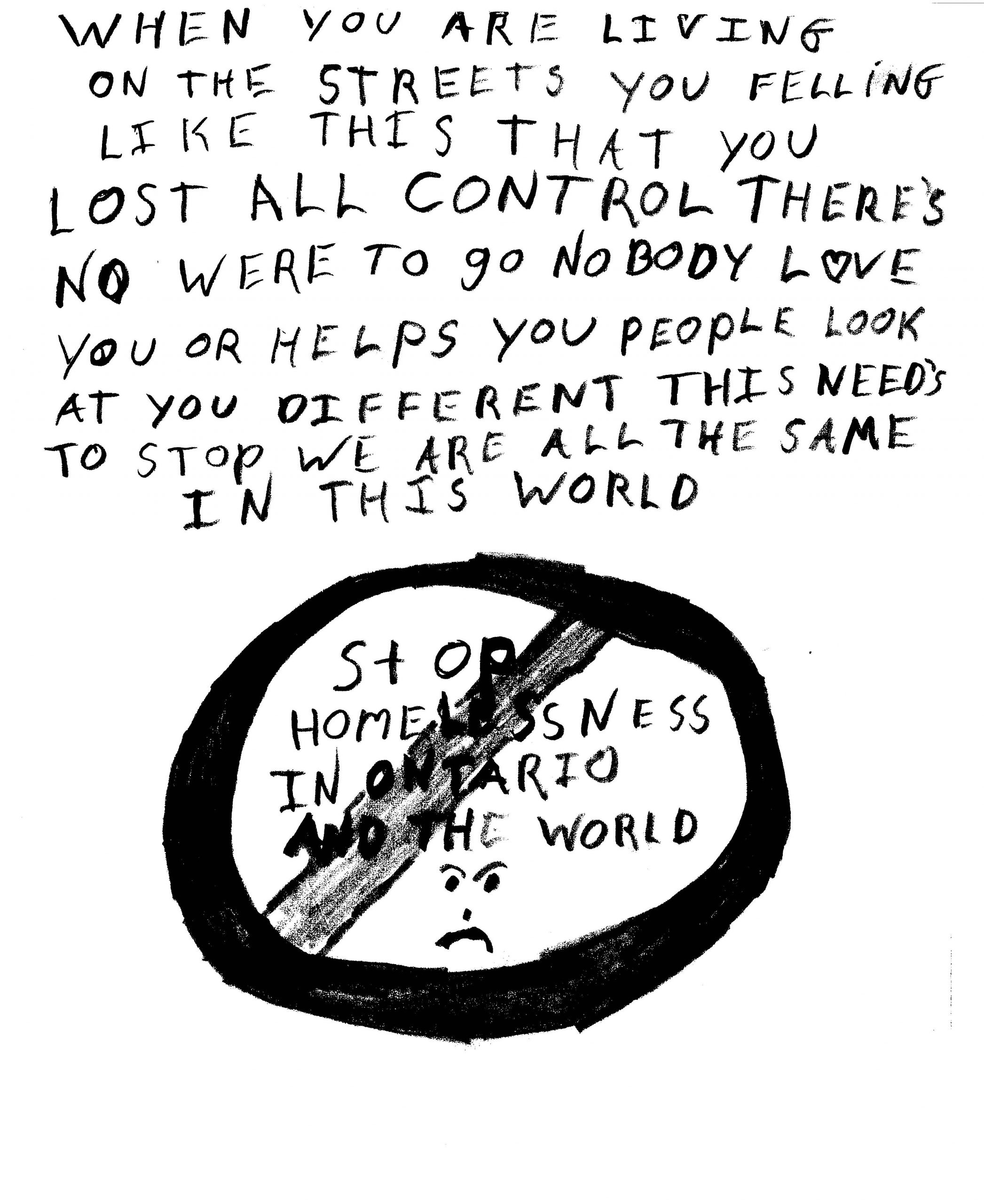
You have likely heard the age-old riddle, “What came first, the chicken or the egg?” The same idea applies to the relationship between homelessness and mental distress. We know that, as a group, people who experience homelessness tend to have higher rates of mental illness. However, the experience of homelessness itself is one that contributes greatly to mental anguish. So, what comes first, homelessness or poor mental health? This chapter delves into the complicated relationship between mental health and homelessness, with an understanding that they are intricately connected in a way that often makes it difficult to tease apart.
As you work through this chapter, you are encouraged to question any preconceptions about mental illness and homelessness that you may have. Perhaps your image of a homeless person is a stereotypical one of a person pushing a shopping cart, talking to themself, while collecting bottles out of a trashcan. This notion, while a common one that is often depicted in the media, is a caricature without depth. Through this chapter, we will add dimension by taking a much deeper look at mental health and its relationship to homelessness.
35
In this chapter, you are invited to critically engage with the complex relationship that exists between homelessness and mental health. While learning more about the research and lived reality, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind the complex nature of the relationship between homelessness and mental health. While not all individuals who experience homelessness will have a diagnosed condition, the experience of homelessness itself is a trauma that impacts mental wellness. Read on to learn more about the dynamic processes involved and the approaches that help.
36
We begin this chapter by presenting two composite scenarios that reflect real-world experiences of homelessness in Canada, as they pertain to the field of Mental Health. As you work through the scenarios, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenarios, and a critical perspective, to think about how the scenarios represent larger issues impacting people in our society.
After considering the real-world scenarios, we will endeavour to answer each question posed in the learning objectives. What is the prevalence of mental health issues for people who experience homelessness? Why is mental illness so high among people experiencing homelessness? What are the treatments that improve mental health, and do they work? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenarios presented at the beginning and reconsider them in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
37
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with these real life composite scenarios. Take a moment here to pause and consider these people’s experiences.
Arin
Arin is a 22- year-old male who has been “couch surfing” between family members for a number of years. He has a low self-image, causing him to hear every comment made to him as a criticism and to be argumentative to the point of never conceding that there is a different interpretation of events. He has significant mood swings from severe depression to violent rage. He lives in a constant state of anxiety. He sleeps very little and paces throughout the night. His extended family has been extremely supportive, taking turns having Arin live with them. They are all exhausted and when he trashed his brother’s apartment over a mild dispute about household chores Arin left in a rage and refuses to see anyone in the family because, in his eyes, they are all out to get him. He is now living on the street and fighting attempts by family members to get him to see a psychiatrist for a diagnosis. The family doctor believes Arin may have a borderline personality disorder; however, he needs a formal diagnosis to qualify for assisted living arrangements supported by a local community mental health agency. The M-Heart team (a joint team of mental health workers and police officers) has been checking in with him twice a week. They are having very little success in convincing Arin to follow through with appointments set up with a psychiatrist. He is consistently a “no show” and the team, although willing to get him there, cannot find him the day of the appointment.
Tanzia
Tanzia is a 45-year-old female currently living in an encampment in a large city. She is working with a local agency to find housing. In the past 15 years she has lived in 23 different apartments/rooming houses with a large number of different roommates. When she is drug-free she has a sunny disposition and positive outlook on finding work. She is very social. She has worked in the food service industry off and on. Unfortunately, due to many reasons, she has a history of reverting to substance misuse. When she is using, she has inconsistent moods, steals from her roommates and from her employers to buy her drugs. She becomes sexually aggressive. Subsequently she is asked to leave her housing and reverts to the streets. She has been bounced from one agency to the next and has not found the support she needs to break this pattern. Tanzia has experienced 3 overdoses in the last 12 months where friends have revived her with Naloxone. She worries that her luck is running out.
With these scenarios fresh in your mind, consider the reflection questions that follow. You may wish to record your answers before moving on to the next section. We will return to the scenarios again at the end of the chapter.
Reflection Questions
38
Homelessness is a traumatic experience that can have deeply negative implications for a person’s mental health. At the same time, a person who is struggling to manage a mental illness may be at greater risk of losing their housing because of challenges associated with their condition. For instance, earning the income needed to pay rent may not be possible for someone who has clinical depression and is unable to go to work, someone who has schizophrenia and is unable to maintain organized thought, or someone who has post-traumatic stress disorder and whose body is in a constant state of alert. It is indisputable that homelessness and mental health are related, but it is not a straightforward relationship.
Before you begin this section, we encourage you to take a moment and consider the question of prevalence. What percentage of people who experience homelessness do you think are impacted by mental illness? What mental illnesses do you think are most common amongst people who experience homelessness? Is everyone’s experience of mental illness and homelessness the same? Thinking about these questions helps us to better understand the complex nature of the relationship between homelessness and mental health. We will explore this relationship throughout this section and chapter, but we invite you to use the space below to record your thoughts before moving forward.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=663#h5p-60
This book was written in the fall and winter of 2021, as the COVID-19 pandemic was in its second year and the Omicron variant was emerging. Two years of lockdowns, distancing, and social isolation were weighing heavily on people’s minds. You may be reading this as the pandemic continues, or in a time past as it has come under control. Either way, we ask you to pause for a moment here and reflect on your own mental well-being as well as that of your family and friends. How have you coped with the pressures of living through a global health crisis? What measures have you and your loved ones taken to improve your mental health? What support did you find from your community?
The experience of living through a pandemic and living through homelessness have some commonalities. They are both highly stressful and isolating events, and while people may draw upon their own personal strength and coping skills, their lives are heavily impacted by the decisions government officials make. The pandemic is not a perfectly parallel comparison to homelessness, but it helps to highlight how stress, isolation, and loss of personal agency can lead to poor mental health.
As you reflect on your experience with the COVID-19 pandemic, we encourage you to think about how it has impacted your higher education studies. Even prior to the pandemic, student mental health concerns had been identified as an emergent crisis issue. We begin this section with a look at student mental health, beginning with a video entitled, “Combating the Mental Health Crisis on Canadian Campuses” created by CBC News: The National in October 2017. We then present a video entitled, “Jennifer’s Story: Hope, Courage and Recovery From Mental Illness” about a young woman whose untreated mental illness caused her to leave university in her fourth year of study and subsequently become homelessness.
We begin with the intersection of university students, mental health issues, and homelessness to highlight some important points. First, when we talk about mental health and homelessness, we are not talking about the one-dimensional stereotypes you may have seen in the media, but rather about real people’s lives. Second, while mental illness may be felt at a personal level, by the person who is affected and their loved ones, it is also shaped by broader social factors. This means that even within your own university, the policies that are in place will determine what kinds and how much support are available for students who are struggling with their mental wellness. We invite you now to watch these two videos, about mental health and homelessness, while considering it from a student perspective. Consider while you watch, what supports your university offers and how effective you think they are at buffering against the risk of housing loss.
We began with these two videos as a way of presenting a more complex image of mental illness and homelessness than is commonly shown in movies and on television. You likely have seen the images of someone who is experiencing severe psychosis, such as hearing voices, and is sleeping outside in public spaces. Certainly, this is some people’s experience. However, we want you to approach this chapter with a much broader perspective. In framing the question for this section, we asked about the prevalence of mental health issues, rather than mental illness. This was done intentionally, with the recognition that mental illnesses are diagnosed through clinical assessment, whereas mental health issues are more broadly defined. A person may not have a clinical diagnosis but may still not be mentally well. We wanted to capture the full spectrum in posing this question.
What we found was that there is no clear answer to this question. What is the prevalence of mental health issues for people experiencing homelessness? No one knows. What is clear, is there is no precise accounting of mental illness rates, but that it is higher than the general public. When we asked homelessness researchers who specialize in mental health about the prevalence, they explained that the rates differ depending on a range of factors, such as which conditions are included in the estimate. For instance, if we are talking about diagnosed severe mental illness, the rates are lower than if we expand the question to consider people who may not have a diagnosis but are nonetheless mentally unwell. In the next two videos, Dr. Tim Aubry and Dr. Nick Kerman explain how the estimates vary depending on the parameters used.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Tim Aubry discusses how severe and persistent mental illness is a health vulnerability for the 15% – 20% of the homeless population who experience chronic homelessness. He argues that there are also very high rates of depression and anxiety for people who experience homelessness in general, as a result of living in poverty, experiencing homelessness, and/or being victimized on the street. This video is 1:37 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: What is the prevalence of mental health issues for people who experience homelessness?
In this video, Dr. Nick Kerman explains that it can be challenging to identify the prevalence rates of mental illness for people experiencing homelessness because the studies that have tried to collect this information vary widely in methodology. He notes that those who experience homelessness have higher rates of mental illness than the general population, with a conservative estimate being approximately 40% – 50%. Dr. Kerman further notes that the category of ‘mental health problems’ is broad and may include both severe mental illness but also more common mental health conditions, such as depression and anxiety. He concludes that considerations of mental health must also include a discussion of substance use, which may be used as a coping strategy by some individuals. As a solution, connecting people with safe and affordable housing may improve mental well-being and decrease substance use problems. This video is 2:54 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: What is the prevalence of mental health issues for people who experience homelessness?
Substance use is common amongst people who have mental illness and are experiencing homelessness, often as a form of self-medicating and trying to cope with hardships. The research shows a complex relationship between mental illness, substance use, and homelessness. For instance, Gicas et al., (2021) questioned whether there is a connection between psychosis in adults experiencing homelessness and the age at which they first used cannabis. They conducted research in Vancouver’s Downtown Eastside using surveys and a battery of neurocognitive tests including the use of structural and diffusion tensor imaging MRI scans. They found that early cannabis exposure (prior to age 15) was associated with an increased risk of developing substance induced psychosis and that later first-usage increased the risk of developing schizophrenia or schizoaffective disorder. Further, the results also indicated that early cannabis exposure may result in changes in regional brain volume (Gicas et al., 2021).
Another study from Vancouver was conducted to examine whether patterns of substance use and risk behaviours were associated with specific psychiatric disorders amongst people who had experienced homeless (Vogel et al., 2019). The results showed a complex picture. They found that major depressive disorder was associated with the use of stimulants and benzodiazepines, post-traumatic stress disorder (PTSD) was associated with stimulant use, panic disorder was associated with alcohol and benzodiazepine use, opioid use was less common in participants with a psychotic disorder, injection drug use occurred more frequently among participants with major depressive disorder, PTSD, and mood disorder with psychotic features (Vogel et al., 2019). These findings are important because they show us that while substance use may commonly co-occur with mental illness amongst people experiencing homelessness, it is not a straightforward relationship.
In another study, a sample of 1,585 people experiencing homelessness were assessed for alcohol and/or substance dependence and bipolar disorder, unipolar depression, and psychotic disorder to better understand whether relationships existed between these conditions (Maremmani et al., 2018). The researchers found that alcohol and/or substance dependence was more common amongst those who were younger, of Indigenous ancestry, lower educated, and located in Western Canada. The odds of alcohol and/or substance dependence were higher among those affected by bipolar disorder, and unipolar depression to a lesser extent. This study shows that people experiencing homelessness who have a major mental illness are at high risk of concurrent alcohol and/or substance dependence but that there are factors such as diagnosis, ethnicity, and location that need to be considered (Maremmani et al., 2018). We invite you now to learn more about this study – and the relationship between substance use, mental illness, and homelessness – in this section’s featured reading below.
Maremmani, A. G. I., Bacciardi, S., Somers, J. M., Nikoo, M., Schütz, C., Jang, K. L., & Krausz, M. (2018). Substance dependence among bipolar, unipolar depression and psychotic homeless: A Canadian national study. Frontiers in Psychiatry, 9, 701–701.
The prevalence of mental health issues among people experiencing homelessness is difficult to determine, in large part because substance use is a complicating factor. Concurrent mental health and substance use disorders are highly prevalent for people experiencing homelessness. In a study from British Columbia, researchers used a range of assessments with 500 individuals living in shelters or on the street and categorized participants into four groups: (1) those without any current mental disorder, (2) those with substance use disorders only, (3) those with substance use disorders only, and (4) those with concurrent substance use and mental disorders (Schütz et al., 2019). Results showed that those with dual diagnoses report more severe physical and psychological symptoms, and these individuals were more likely to be younger, Indigenous, and to be unsheltered. Importantly, they also reported significantly more challenges receiving the health care services they need. This group, with both mental illness and substance use disorders, is highly vulnerable because they lack access to basic services, like health care and shelter, despite having some of the most complex needs (Schütz et al., 2019).
This population’s inequitable access to mental health services is another key reason we lack definitive rates of mental health issues. If we were to only account for those with diagnosed mental illnesses, the rates would be considerably lower than if we consider poor mental health more generally. Although many people would qualify as meeting the criteria for mental illness, their lack of access to mental health professionals makes those diagnoses and treatments less likely. There are many complicated reasons why people who experience homelessness have inequitable access to health care, as we discuss further in the chapters on Primary Care & Nursing and Emergency Medicine, but a lack of communication, discrimination, and stigma are key drivers for these poor outcomes.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=663#h5p-61
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=663#h5p-62
All Canadians, whether housed or experiencing homelessness, are facing a shortage of mental health supports. To learn more, we invite you to watch this brief segment from Global News about how access to mental health services has become a national problem. As you watch this, we encourage you to think about how this lack of access may be even more detrimental for people experiencing homelessness. This video was also released in October 2019, prior to the COVID-19 pandemic. How do you think the demand for mental health services may have changed during this period of time?
There are not enough mental health services across the country to meet the needs of Canadians. What do you think could be done to increase both the number of mental health services and their accessibility? How can we ensure people who experience homelessness have access to the mental health supports they need to be well?
The prevalence of mental health issues amongst people experiencing homelessness is not well known because many do not have access to mental health practitioners who could offer diagnoses and treatments. In the next two videos, Dr. John Ecker and Dr. Katrina Milaney explain the estimates of mental health issues vary widely for people experiencing homelessness, and that the lack of mental health services is a key reason why.
In this video, Dr. John Ecker argues it is difficult to identify an exact prevalence rate of mental illness for people experiencing homelessness because the research is varied, with estimates ranging from 10% – 60%, and because not every person living with a mental illness will have been diagnosed or received proper mental health care. However, Dr. Ecker concludes that we can, with some degree of certainty, say that people who experience homelessness as a group have a higher rate of mental health challenges compared to the general population. This video is 0:57 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: What is the prevalence of mental health issues for people who experience homelessness?
In this video, Dr. Katrina Milaney discusses the wide range of mental illness prevenance estimates found in the literature. She notes that studies variously indicate 25% to 75% of individuals who experience homelessness have mental health concerns. Dr. Milaney argues that determining an exact figure is a complicated issue because many people who experience homelessness, and chronic homelessness, in particular, have been excluded from mainstream health care and may not have received a proper diagnosis nor adequate care. Further, she postulates that the experience of homelessness itself is a form of mental distress, and may serve to exacerbate existing mental health conditions. This video is 1:11 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: What is the prevalence of mental health issues for people who experience homelessness?
The exact prevalence of mental health issues for people experiencing homelessness is unknown, in part because of different considerations about what is included and in part because these individuals often lack access to mental health services that could provide diagnoses and treatments. We have seen a range of different estimates throughout this section so far, with researchers identifying studies that show figures as low as 10% and as high as 75%.
When we set out to write this book our mission was to explore seemingly simple questions that had complex answers. The prevalence of mental health issues is no exception. Homelessness, poor mental health, and substance use are often connected, but not in straightforward nor singular ways. People may experience a mental illness that results in housing loss, or they may be experiencing homelessness and find that their mental well-being declines as a result. In the next video Dr. Sean Kidd, Chief of the Psychology Division at the Centre for Addiction and Mental Health in Toronto, explains that when we take a broad view, we see that nearly every person who experiences homelessness will have mental health challenges because of the associated stress, violence, and trauma.
In this video, Dr. Sean Kidd explains that there are different estimates of mental illness prevalence for people experiencing homelessness, based on what is included in the definition. When considering major mental health disorders, such as major depression, PTSD, schizophrenia, and the overlay of addictions, it is estimated that this impacts 50% of people experiencing homelessness. When extended to general mental well-being, nearly every person who has experienced homelessness for a period of time will have mental health challenges, large amounts of stress, and experiences of violence. Dr. Kidd argues that homelessness is traumatizing, not in a single event kind of way, but as an everyday, ongoing form of deprivation. This video is 1:56 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: What is the prevalence of mental health issues for people who experience homelessness?
In much the same way, Dr. Cheryl Forchuk argues that we need to broaden our perspectives and consider every person who experiences homelessness part of a disenfranchised mental health population. Dr. Forchuk explains that it is better to be over-inclusive and ensure everyone receives the mental health services they need than to be more restrictive and miss people who could benefit from the support. She explains further in the video that follows.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk makes the argument that the homeless population should be treated as a disenfranchised mental health population. In one study 187 youth experiencing homelessness were given proper assessments, and 100% were diagnosed with mental health and/or addictions issues. Dr. Forchuk argues that not every person is comfortable revealing their situation, and so it is better to provide everyone experiencing homelessness with mental health and addictions supports than to miss people who may benefit. This video is 1:23 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: What is the prevalence of mental health issues for people who experience homelessness?
Throughout this section, we sought to identify the prevalence of mental health issues amongst people experiencing homelessness. What we found is that it is somewhere between 10% and 100%. That may not seem very helpful, but it is insightful. What it tells us, is that we are lacking knowledge in this area and that not enough people who are experiencing homelessness and poor mental health are coming into contact with the mental health care system. What we know definitively is that the rates of diagnosed mental illnesses and overall poor mental health are higher for people who experience homelessness than for those who are housed. Yet, despite being amongst the most in need of mental health services, many people who experience homelessness do not receive timely mental health care.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=663#h5p-63
We began this section by asking you to consider your own experiences of stress, isolation, and loss of agency during the COVID-19 pandemic. While we noted that this is not a perfect comparison, it does demonstrate some of the daily conditions that people who experience homelessness have to live with. Mental health challenges often arise as a result of homelessness and people may turn to substance use as a means of coping. Homelessness may also be the result of an untreated mental illness that began while a person was housed. The relationship between homelessness, mental health, and substance use is a complex one that is at the root of why we see such varied estimates. There is an old saying that it is better to be safe than sorry. With this in mind, we argue that whether the prevalence rates are 10% or 100%, what matters most is that we address the causes of homelessness, reduce the amount of time people spend in it, and increase access to supports and services for everyone.
Click the link below to listen to all of the researchers answer the question “What is the prevalence of mental health issues for people who experience homelessness?” in audio format on our podcast!
39
The reasons why mental illness (or more broadly, mental health problems) is so high for people experiencing homelessness is intricately related to the prevalence rates. This means that we have already considered some of the reasons already. We have seen, for instance, that there is a lot of stress, violence, and trauma that accompanies the experience of homelessness. We have also seen that the use of substances is related to mental illness for many, although not all, people who experience homelessness. These are key factors that contribute to high rates of mental health problems for this population. However, there is much more we can say about these and other contributing factors. We invite you at this moment to pause and consider why you think mental illness is high among people who experience homelessness. You may use the space below to record your thoughts before proceeding through the section.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=665#h5p-64
In the previous section, we explored the prevalence rates of mental health issues and found that the estimates vary widely. There is no precise statistic that we can point to because studies that have attempted to record these figures have varied in their inclusion criteria. What we do know is that people who experience homelessness have higher rates of mental illness than people who are housed. The reasons for why this occurs are equally complex, as it can be difficult to identify “which came first.” For many people, mental health challenges exist prior and are then exacerbated by losing their housing and experiencing the trauma that accompanies homelessness. In the first video of this section, Dr. Tim Aubry explains further.
In this video, Dr. Tim Aubry explains that some people are more vulnerable to becoming homeless because of their mental health problems. He notes that once a person experiences homelessness, their mental health often gets worse due to the poor living conditions. Dr. Aubry notes that part of the way we think about mental health today involves substance use, which is more commonly related to single adult and youth homelessness, than family homelessness. He argues that mental illness is high among people experiencing homelessness because they are in a crisis situation, trying to survive every day, and they have the stress and uncertainty of not knowing how they will get out. This video is 3:21 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: Why is mental illness so high among people experiencing homelessness?
In the preceding video, Dr. Aubry explained that mental health challenges can arise as people live in constant states of crisis, trying to meet their daily needs amidst great uncertainty. To understand why this has occurred we must travel back through history to the deinstitutionalization of psychiatric patients in the 1970s and 1980s. During this period, people who had previously been placed in asylums were released with the idea that they could receive pharmaceuticals and mental health care while living in the community. While treatment in asylums was highly problematic – a discussion beyond the scope of this chapter – it is noteworthy that deinstitutionalization raised many issues as well.
Below we present a brief video, created by Dr. Pashak, about deinstitutionalization and its effect on contemporary homelessness. While this video contains American statistics, the timeline and outcomes are very similar to what occurred historically in Canada. As you watch this video, we encourage you to think about the idea raised in the previous section that every person who experiences homelessness should be considered part of a disenfranchised mental health population.
Deinstitutionalization moved people out of asylums and into the community without proper planning or consideration for where they would go. In the following video Dr. Nick Kerman, a Post-Doctoral Fellow at The Centre for Addiction and Mental Health (CAMH), explains how the effects of deinstitutionalization are still felt in Canada today. If you are interested in learning more about deinstitutionalization, and about how CAMH has transitioned through it, we encourage you to watch the video “If These Walls Could Talk” found in the “Want to Learn More?” section of this chapter.
In this video Dr. Nick Kerman explains how the history of deinstitutionalization in Canada in the 1970s and 1980s led to the closure of psychiatric hospitals, resulting in a large number of people who had nowhere to go for support. He notes that the effects of these policy decisions have been seen through decades of over-representation of people with serious mental illness in the homeless population. Dr. Kerman discusses the complex relationship between mental illness and homelessness, noting that mental illness can be a pathway into homelessness but can also be a consequence of the victimization and trauma that often result from homelessness. Dr. Kerman concludes by noting that two of the basic building blocks of mental health – sleep and nutrition – are often compromised as well for people who are sleeping in shelters on an ongoing basis. This video is 6:00 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: Why is mental illness so high among people experiencing homelessness?
Dr. Kerman has researched mental health and homelessness in contemporary society, finding that the way services are organized today allows people to survive but keeps them marginalized such as through limited access to nutritional food, sustained social isolation, and insufficient incomes to participate in recreational activities (Kerman & Sylvestre, 2020). The history of deinstitutionalization has shaped our modern homelessness infrastructure and contributed to the high rates of homelessness across the country, as people were released into the community without the proper supports in place. This occurred at a time when the Federal government was decreasing their role in building affordable housing, which you read more about in the chapter on Politics, Policy, & Housing in Canada. Dr. Cheryl Forchuk refers to this as a perfect storm of policy changes that occurred at the same time and contributed to the high rates of homelessness we see today. She explains further in the video that follows.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk explains that the question of why mental illness is high amongst people experiencing homelessness is complex because it is a “chicken and egg” scenario of considering what comes first. She notes that we need to consider the perfect storm of policy changes that occurred when the Federal government withdrew from funding social housing, income supports were reduced, and deinstitutionalization closed psychiatric facilities with no housing provisions. Dr. Forchuk argues that people who experience mental illness are the most discriminated and stigmatized group in society and that people who become homeless often lack the social supports that might keep others with the same issues housed. Dr. Forchuk concludes by noting that addiction issues can also be a “chicken and egg” situation, such that if a person does not have an addiction issue prior to homelessness, they are likely to have one afterward. This video is 3:21 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Why is mental illness so high among people who experience homelessness?
It is a recurring theme throughout this book that historical decisions, such as those related to housing and other social policies, have an impact on contemporary rates of homelessness. However, we can also see that homelessness is related to a range of additional factors that serve to create the conditions and prevent people from being able to find stability in their lives. As Dr. Forchuk noted in the previous video, homelessness is related to the kinds of social supports a person has in place and whether they have people they can turn to for help. Many people who experience homelessness lack the kinds of strong social connections that might prevent those with stronger networks from falling into homelessness during a crisis situation.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=665#h5p-65
The lack of strong social supports, such as friends and family members, can have very negative effects on a person’s mental health and well-being. Jones et al., (2020) have found that social isolation may have roots in the brain, as they examined 60 people experiencing homelessness and found that those with larger amygdala and central nucleus volumes had a larger social network. A key factor to consider is that people who experience homelessness have often had adverse childhood experiences (Smith, Milaney, Henderson, & Crowshoe, 2021) which can alter the brain’s neural pathways. The video that follows entitled, “Childhood Trauma and the Brain” was created by the UK Trauma Council and explains this association further.
Researchers who conducted a cross-sectional study using national data from 2,235 adults with mental illness experiencing homelessness in Canada found that on average these individuals reported 4 adverse childhood experiences, such as maltreatment, sexual abuse, neglect, divorce, and/or household dysfunction (Liu et al., 2021). Their data also indicated that these adverse childhood experiences were higher among women, and that they can be linked to poor mental health outcomes (Liu et al., 2021). The effects of trauma can persist over time and those experienced during childhood continue to impact people into adulthood. We see this clearly when we consider how many people experiencing homelessness also report mental illness and childhood trauma (Lévesque & Abdel-Baki, 2020).
Interested in learning more about Adverse Childhood Experiences? Check out this extensive collection of resources from the Centres for Disease Control and Prevention.
Social isolation and loneliness are both causes and consequences of being mentally unwell. They are also risk factors for suicidal ideation (i.e. considering suicide) and for committing suicide. This is evident from a body of research on homelessness and mental health. For instance, a study of 455 people who were formerly or currently homeless showed that 16% reported suicidal ideation and 7% had attempted suicide (Gentil, Grenier, & Fleury, 2021). The same study showed a complex association with mental health disorders and substance use. Notably, suicidal ideation was higher for those with generalized anxiety disorder, substance use disorders, and schizophrenia spectrum and other psychotic disorders (Gentil et al., 2021). Higher rates of suicide attempts were reported by those with higher functional disability, more frequent hospitalizations, and those with substance use and mental health disorders (Gentil et al., 2021).
Amongst youth, the risks of suicidal ideation and attempts have been found to be even higher. Researchers conducting the first national survey on youth homelessness collected 1,103 responses from young people accessing homelessness services in 42 communities across Canada and found that 42% reported at least one suicide attempt and 85% were in high psychological distress (Kidd, Gaetz, & O’Grady, 2017). These risks were particularly evident amongst those who experienced homelessness for the first time at an early age, were female gender, and identified as lesbian, gay, bisexual, transgender, queer or questioning, or two-spirit [LGBTQ2S+] (Kidd et al., 2017). The second survey, conducted four years later, included 1,375 youth accessing homelessness services in 49 communities and found that 35% reported at least one suicide attempt and 33% had a drug overdose that required hospitalization (Kidd et al., 2021). Dr. Kaitlin Schwan was a researcher on the national youth homelessness survey project and lead author on a proposal for improving mental health care for these young people in Canada (Schwan, Kidd, Gaetz, O’Grady, & Redman, 2017). Here she speaks more about the findings and the implications homelessness has for the mental health of young people.
In this video, Dr. Kaitlin Schwan discusses the results from a survey conducted by the Canadian Observatory on Homelessness with 1,100 youth experiencing homelessness across Canada. She notes that many young people report huge increases in health challenges, such as lacking a place to rest and wash, experiencing high rates of stress, and not recovering from illness as quickly. Dr. Schwan explains that this survey showed high rates of nutritional vulnerability and that 30% of respondents indicated they did not have access to clean water on a daily basis. She further notes that mental health and addictions challenges were found to be high, with 42% having attempted suicide and 85% in high symptom distress categories. Dr. Schwan explains that despite public misconceptions, these youth are much more likely to be the victims of crime than the offenders. She concludes by arguing that all of these conditions make it difficult for young people to be healthy and well, which is why we need to focus on successfully exiting them out of homelessness and into secure housing. This video is 4:31 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: The stress of youth homelessness
In the second national survey on youth homelessness, of which Dr. Schwan speaks, sexual violence emerged as a key factor in the identification of youth experiencing the greatest distress (Kidd et al., 2021). These researchers also found high rates of suicidality and mental health challenges, particularly for females, Indigenous youth, and those who identify as LGBTQ2S+ (Kidd et al., 2021). In the next video, Dr. Alex Abramovich explains how the daily stigma and discrimination LGBTQ2S+ young people face escalates their risk of mental health challenges.
In this video, Dr. Alex Abramovich explains that LGBTQ2S+ youth experiencing homelessness face high levels of stress and stigma, which has a negative effect on their mental health. He notes that amongst this population there are significantly higher rates of depression, anxiety, substance use, suicidality, and suicide completion compared to heterosexual and cisgender youth. Dr. Abramovich is clear to note that these mental health challenges stem from the daily stigma, discrimination, and violence these youth experience in society, and not from their gender or sexual identities. He concludes by arguing that more specialized mental health assessments and supports are needed for this population of young people. This video is 1:37 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: LGBTQ2S youth, stigma, and mental health supports
Social support is key to people’s well-being. Without a strong network of friends, family, or community members, individuals often feel isolated and lonely. This message was clear in a study conducted with 76 youth experiencing homelessness and residing across 8 shelters (Gauvin, Labelle, Daigle, Breton, & Houle, 2019). Researchers found that youth who had not attempted suicide perceived more social support (both tangible assistance and guidance) whereas those who had attempted suicide reported using more non-productive coping strategies like keeping to themselves, isolation, and self-blame (Gauvin et al., 2019). Humans are social beings and having others to turn to is critically important for mental wellness. There is a pervasive and deeply harmful stigma associated with experiencing homelessness that serves to keep people isolated, subsequently decreasing their already poor mental health.
Even when people move out of homelessness and into secure housing, one of the biggest challenges they continue to face is reintegrating into the community around them. Research with youth transitioning out of homelessness in Toronto demonstrates that as young people work through this transition and seek to be more socially integrated, they grapple with their identity (Thulien, Gastaldo, McCay, & Hwang, 2019). This sense of inclusion can be challenging as they follow a non-linear path, from the street to social integration, that can leave them feeling bogged down, confused, and exhausted by the competing aims of feeling integrated and trying to meet their basic needs (Thulien, Gastaldo, Hwang, & McCay, 2018). Dr. Naomi Thulien and her team have studied the pathways young people take in exiting homelessness and the mental struggles of trying to feel connected and socially included through the process. In the next video, Dr. Thulien discusses this research further.
In this video, Dr. Naomi Thulien argues that relationship building is critically important in supporting people experiencing homelessness and should be actively cultivated. Without trusting relationships, she notes, support can unravel. Dr. Thulien explains that loneliness and boredom are linked to homelessness, poor mental health, and addictions in an existential kind of way. She notes that trying to keep busy is a reminder of how socially isolated people can be and changes the way they experience the passing of time. Dr. Thulien concludes that housing people is important, but we must also ensure they have meaningful activities to fill their time. This video is 7:08 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: Loneliness, social isolation, and relationship building
How well integrated a person feels within their community is dependent on a range of factors related to the housing itself, such as the neighbourhood safety and location, whether people are using substances, and the housing quality (Ecker & Aubry, 2017). However, community integration can also be related to personal factors, such as whether a person feels they have meaningful activity in which to engage that helps prevent boredom (Marshall, Keogh-Lim, Koop, Barbic, & Gewurtz, 2020a). In the preceding video, Dr. Thulien spoke about the kind of existential boredom that people can experience once they are housed but have no meaningful activities to fill their time. There is limited research on boredom and homelessness, but a scoping review has found themes related to coping strategies, the impact of boredom, the environment as a determinant, and possible interventions (Marshall et al., 2020b).
Boredom is something we all inevitably face. You may have found yourself at times having nothing to do and wondering how to fill the time or, dare we say it, sitting through a class that does not hold your interest (of course not this one!). This kind of boredom is common and not what we mean here. Many people who experience homelessness do not have activities, like work, to fill their time. They also often lack money to engage in leisure activities. With endless time, limited social contacts, and no money to spend, the hours stretch on. People may continue to use service agencies, and many spend time volunteering, but these require transportation which also costs money.
Preventing boredom and finding meaningful activities are key for helping people who have experienced homeless feel socially integrated into their community. Consider the area where you live. What kinds of activities are available for people that do not cost money and are open to anyone who wants to join? What other programs might be needed to increase opportunities for people to get involved without costing money?
When experiencing homelessness and even after obtaining housing, people’s mental well-being is often dependent on having meaningful activities that allow them to engage with others and develop relationships within the community. In this section’s featured reading we present an article from Dr. Thulien and her team about a pilot study that explored the feasibility of improving socio-economic inclusion for young people transitioning out of homelessness by bolstering their identity capital, such as their sense of purpose and control, self-efficacy, and self-esteem. We invite you now to learn more about Dr. Thulien’s research in the featured reading below.
hulien, N. S., Wang, A., Mathewson, C., Wang, R., & Hwang, S. W. (2021). Tackling exclusion: A pilot mixed method quasi-experimental identity capital intervention for young people exiting homelessness. PLOS ONE.
Helping individuals increase their identity capital is a promising approach for building upon and offering them assistance as they transition out of homelessness and into secure housing (Thulien et al., 2021). Addressing issues such as a person’s sense of inclusion and identity are critical for improving mental health and achieving long-term housing stability. This is particularly important for people who experience homelessness because, as we have seen, they face considerable stigma and discrimination. Research has shown that there is an urgent need to identify strategies and policies to reduce the stigma and discrimination that people who experience homelessness and mental illness go through (Mejia-Lancheros et al., 2020). We need to recognize and acknowledge the loss they experience as well. Consider, for instance, the impact that losing one’s home, family, workplace, and community might have on a person’s sense of self-identity.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=665#h5p-66
Homelessness is deeply harmful to people’s mental health because it is grounded in loss. It is right there in the word – a person is not only less a home but also less all the social relations that go along with it. We encourage you to pause for a moment and reflect upon how you identify your own sense of self. Are you someone’s significant other? Do you have children and identify as a parent? Do you refer to yourself as someone’s brother or sister? Do you have a job that you relate with your sense of identity? When a person experiences homelessness they lose many of the markers they previously identified with, which has a negative impact on their mental well-being. In the video that follows Dr. Sean Kidd explains the importance of recognizing identity and identity loss in understanding why people who experience homelessness are often in poor mental health.
In this video, Dr. Sean Kidd explains that people have different experiences and trajectories of homelessness, but that a common factor driving people’s physical and mental health outcomes is the social determinants of health. He notes that for many people who experience homelessness, their challenges began while they were housed. For youth this is often in the form of trauma or neglect within the home or school. For adults, this may be related to job loss, divorce, and/or mental health and addictions issues. Dr. Kidd notes that when a person loses their housing they also often lose their identities such as tied to being employed, someone’s spouse, or a homeowner. These identities may be replaced with assumptions that they are now dangerous, lazy, and/or a criminal. These labels create new mental health challenges that lead to a vicious cycle. Dr. Kidd concludes that this cycle demonstrates the importance of homelessness prevention, so people’s problems do not become compounded. This video is 4:53 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: Why is mental illness so high among people who experience homelessness?
The loss of identity has profound implications for a person’s mental well-being, as Dr. Kidd has explained. We encourage you to think about this key takeaway message as you watch a brief documentary created by CBC Docs about a man named Roger who lost his job, wife, and child and has struggled with recurrent episodes of homelessness in Toronto.
The experience of homelessness is stressful, isolating, and traumatic. It is not surprising then that many people, if not all, who experience homelessness will also have poor mental health and potentially a severe mental illness. Yet, we also must recognize that surviving through this experience takes a great deal of personal strength. We began this section by discussing the deinstitutionalization of asylums that saw mass numbers of people removed from institutions and put out in the community with nowhere to go. In the decades since, there remains a lack of adequate mental health services to treat what Dr. Cheryl Forchuk has called a disenfranchised mental health population. We conclude this section with a video of Dr. John Ecker that brings these ideas together. Today, 60 years past deinstitutionalization, we still have much work to do to coordinate systems responses like hospital discharge, but we also need to recognize the strength people show amidst these institutional failures.
In this video, Dr. John Ecker explains that mental health challenges can happen prior to homelessness, as a result of homelessness, or in combination. He notes that structural and systemic failures need to be considered, such as inadequate mental health and financial supports, as well as the lack of coordinated discharge practices from hospital. Dr. Ecker explains that experiencing homelessness can be traumatic and have negative consequences for physical and mental health. He concludes by noting that we must also recognize the strength and resourcefulness of people who experience homelessness, and the importance of the social bonds they create with others, which can help buffer mental health challenges. This video is 3:18 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Mental health challenges and supports
People who experience homelessness face tremendous adversity but still show remarkable resilience, strength, and positivity despite these hardships (Shankar, Gogosis, Palepu, Gadermann, & Hwang, 2019). We set out in this section to identify why mental illness is so high among this population and found that there are many complex reasons. While we may be tempted to ask the chicken and egg question of what comes first, the reality for many people is that they cannot be so easily teased apart. People may be mentally unwell and have difficulties maintaining their housing as a result. Once in shelter, moving between temporary accommodations, or on the street, the stress of living in a constant state of crisis makes their mental health worse.
Historically when people were mentally ill they would be sent to live in an asylum. These places, while deeply problematic, created a new problem when they closed in the 1970s and 1980s. Deinstitutionalization occurred as they closed their doors and moved people out into the community with the notion that they could receive pharmaceuticals and mental health treatment outside the hospitals. However, this occurred at the same time the Federal government stopped funding new social housing, creating a lack of affordable places for these patients to live, and Provincial governments decreased the income supports they would provide. These policies and decisions created a situation that left mass numbers of people unhoused, living in deep poverty, and without access to the same levels of mental health services.
This sense of disconnection from society and social supports has carried through to the current day. Having people that one can count on – whether family, friends, or support workers – is critical to good mental health. However, when people experience homelessness they often feel isolated and cut off from others. As we saw in this section, this social exclusion leads to high rates of suicidal ideation and suicide attempts. This is particularly true for young people, with those who identify as LGBTQ2S+ at the highest risk. People who experience homelessness often feel a deep sense of loneliness and express the need to find meaningful activities to fill their time. The sense of boredom that accompanies homelessness, and which follows people even after they are housed, can weigh heavily on their minds, and ultimately threaten their housing security.
When people lose their housing they also lose the sense of identity that is tied into it, like being a homeowner, spouse, parent, or worker in a particular job. Not only do people lose the identities they have, but they are often substituted for stereotypes such as that the person must be a criminal or dangerous because they are homeless. The loss of identity and the discrimination that people face is a key reason why mental illness is so high among this population. In the time since the deinstitutionalization movement, we have continued to see institutional failures, yet amidst these conditions, many people who experience homelessness demonstrate remarkable personal strength. The question we need to ask is not what comes first, mental illness or homelessness, but rather how we can help make both better so that we do not need to wonder at all.
Click the link below to listen to all of the researchers answer the question “Why is mental illness so high among people experiencing homelessness?” in audio format on our podcast!
40
Homelessness is always a difficult issue to consider, and this chapter is particularly challenging because it highlights all the daily struggles that lead to poor mental health outcomes. At this point we have seen that there are high rates of mental health issues, with estimates as high as 100% of people who experience homelessness being affected. We have seen that these high rates are caused by trauma, discrimination, social isolation, loss of identity, and a lack of mental health services to support people. This is a dire picture. However, people do recover from mental illness and from homelessness so the discussion cannot end there. Instead, we need to consider what approaches work to treat mental illness and to help improve mental well-being overall. We invite you now to consider what you have learned about the causes of poor mental health and see if you have ideas on what treatments might help. You may use the space below to record your thoughts.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1203#h5p-67
Like all of the questions in this book, this question does not have a simple answer. What treatments work will depend on many variables, such as an individual’s personal history, what diagnoses(s) they have, and their willingness or ability to engage in treatment. Therefore, we cannot point to one approach and say it is the answer for everyone. What we can say is that there are a range of approaches that may work for people individually or in combination and that the foundation of success must be based on social determinants, such as having housing, proper nutrition, adequate rest, and a livable income. As we have seen, social support is also a critical piece of mental wellness for people experiencing homelessness and developing intimate relationships can help contribute to their recovery (Ecker, Cherner, Rae, & Czechowski, 2018).
The research literature points to a number of mental health approaches that have shown some effectiveness in helping people experiencing homelessness and housing vulnerability to improve their well-being. Brakenhoff and Slesnick (2018) for instance have argued that the community reinforcement approach and motivational enhancement therapy have been shown to be among the most promising interventions for mental illness and substance use problems. The community reinforcement approach is guided by the assumption that people continue to use substances because they are reinforced to do so through their environment, and that people can recover if they shift the focus such that non-substance using behaviours are more reinforcing (Brakenhoff & Slesnick, 2018). Motivational enhancement therapy is premised on the belief that everyone has the ability to change but that people have different levels of motivation, and so this intervention is structured to encourage behavioural change by increasing people’s motivation (Brakenhoff & Slesnick, 2018).
Mindfulness practice has grown from cognitive behavioural approaches and helps train people to identify their automatic thinking patterns and then to challenge them (Brown & Bender, 2018). Individuals can improve their mental well-being and promote more adaptive functioning by changing their negative automatic thoughts and improving their emotions and behaviours (Brown & Bender, 2018). Another related evidence-based intervention that has shown promise with people experiencing homelessness and mental illness is dialectical behaviour therapy (DBT), which is designed to treat a range of conditions including mood and anxiety disorders, self-harm practices, and suicidality (McCay & Aiello, 2018). Dialectical behaviour therapy is premised on the notion that conditions arise through inadequate emotion regulation due to biological factors and/or interpersonal circumstances like exposure to trauma (McCay & Aiello, 2018).
The dialectical behaviour therapy approach is comprised of cognitive behavioural approaches and acceptance-based practices that come from the Zen school of Buddhism, emphasizing the need for therapeutic acceptance, and a focus on changing maladaptive coping mechanisms (McCay & Aiello, 2018). In the video that follows Dr. Marsha Linehan, creator of the dialectical behaviour therapy approach, describes how she draws upon Zen practice to help people develop core mindfulness skills.
Population mental health interventions that exist in the community have not been documented in the same way as controlled public health interventions, but we can extract findings from quasi-experimental interventions that meet scientific standards while also showing promise of positive impacts on mental health equity (Simpson, Furlong, & Jetha, 2018). For instance, while there is limited research on the personal recovery needs of community-dwelling Canadians with mental illness, one multi-site cross-sectional study has shown that adults who receive community-based mental health supports in an urban setting reported high levels of empowerment, hope, and optimism about the future (Barbic et al., 2018). However, the same participants also reported low levels of perceived connectedness, identity, and meaning in life, suggesting that recovery-oriented patient report outcomes offer a complex picture of how these patients view their well-being and treatment needs (Barbic et al., 2018).
An increasingly recognized approach for promoting mental wellness in the community is that of recovery education centres, like the Supporting Transitions and Recovery Learning Centre in Toronto (Durbin et al., 2019). Reid et al., (2020) conducted a qualitative study with 20 people involved in the recovery education centre and learned that the process of recovery was supported through factors such as a judgement-free environment, supportive relationships, mutuality and role modelling, deconstruction of self-stigma, and reclaiming one’s power (Reid et al., 2020). As we have seen in the previous section, people who experience homelessness often feel isolated, discriminated against, and as though they have lost their sense of identity. The recovery education centre helped these individuals to improve their self-esteem, confidence, sense of empowerment, interpersonal skills, and ability to self-advocate (Reid et al., 2020).
You can learn more about this study from this research snapshot!
There are many interventions that have shown promising outcomes for people who are experiencing homelessness and impacted by mental illness. The research literature discussed above points to the community reinforcement approach and motivational enhancement therapy (Brakenhoff & Slesnick, 2018), mindfulness practice and cognitive behavioural therapy (Brown & Bender, 2018), dialectical behaviour therapy (McCay & Aiello, 2018), community-based population mental health interventions (Barbic et al., 2018; Simpson et al., 2018), and recovery education centres (Durbin et al., 2019; Reid et al., 2020). These are all interventions that have shown some effectiveness in helping people experiencing homelessness with mental illness.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1203#h5p-68
Brakenhoff and Slesnick (2018) importantly note that, “Regardless of the chosen intervention, service providers must ensure youth who are homeless are given the space to identify treatment goals that are meaningful to them. While progress may be slow given the extensive challenges these youth experience, research has demonstrated that with the right tools and support, change and behavioural improvement is possible, even for the most vulnerable youth” (pg.14). The need for individuals to set their own goals and their own pace is true for youth as well as for adults. In the next video, Dr. Sean Kidd discusses these interventions and the importance of tailoring the support to an individual’s self-identified needs in further detail.
In this video, Dr. Sean Kidd discusses the complexity of treating people who are experiencing homelessness and have mental health problems. He explains that while the treatments are the same, there are fundamental conditions that need to be met for the person to be able to engage in treatment. He notes that these conditions can be met in different sequences, depending on the person’s needs but may include factors such as safe and secure housing, nutritional security, medication, and supportive social contacts. Dr. Kidd explains that while the foundational pieces are being put in place, it is possible to have early conversations to prepare people for treatments such as psychosocial interventions, supported employment, cognitive behavioral therapy, and psychotherapy. He argues that what is needed is careful assessment of the spectrum of factors to tailor a person’s supports to their needs, provided in an order that works for them. He concludes by highlighting the under-funded nature of mental health care for people experiencing homelessness and noting that funding greatly influences what we can offer and its effectiveness. This video is 5:43 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: What are the treatments that improve mental health, and do they work?
The lack of funding for mental health systems in Canada reduces the capacity for people who need treatment. Dr. Kerman and Dr. Kidd (2020) have argued that embedding mental health recovery within a quality improvement framework would increase leverage for systems change and create advancements in recovery practice. They point to the Triple Aim, with the goals of improving healthcare outcomes, quality, and costs as all being relevant within the context of mental health systems and in working towards the integration of a social determinants of health lens (Kerman & Kidd, 2020). We have identified the social determinants of health as a foundational principle throughout this book because they are central for understanding what contributes to people’s health and well-being on a broad level. Certainly, one of the most important social determinants is whether people have safe, secure, and affordable housing. We present the next video about “My Place Supportive Housing in Vernon, British Columbia” to demonstrate the critical importance of housing as a social determinant of mental health. As you watch it, we encourage you to reflect upon how housing has improved the mental well-being of the tenants in the video.
In the chapter on Politics, Policy, & Housing in Canadawe looked at the rise of Housing First as a targeted intervention for people who have severe mental illness and experience chronic homelessness. The underlying idea is that people need housing as a starting point, without having to demonstrate they have met housing-readiness requirements. Advocates had been arguing for this approach since the 1980s but the program as we know it today was shaped by Dr. Sam Tsemberis and Pathways to Housing in New York. In Canada, the effectiveness of Housing First was evaluated by a multi-year, multi-site study known as the “At Home / Chez Soi” project funded through the Mental Health Commission of Canada (Goering et al., 2014). Housing First has been widely adopted (and at times adapted) as a means of housing people with mental illness. As a brief refresher on Housing First, we invite you to watch this video created by the Homeless Hub that explains how this approach is recovery-oriented and implemented to help people experiencing homelessness move rapidly into permanent housing.
Housing in itself is a critical social determinant of health and mental health. However, what Housing First offers is an additional level of wrap-around supports based on people’s own self-identified needs. This means, for example, that if a person believes their substance use is a problem in their lives they can request support for substance use, or if they wish to return to school and earn a higher education they can request education supports. Research has shown that employment is associated with an increase in recovery for some people in the context of Housing First (Yazdani et al., 2020). The key aspect is that people have choice not only in their housing but in the type of supports they receive. It is important that residents within these housing programs be able to foster their own pathways to recovery with the recognition (as we so often say throughout this book) that when it comes to housing and supports one size does not fit all (Montgomery, Mossey, & McCauley, 2019).
In the chapter on Social Work we examine the role of case management in supporting people who are experiencing homelessness. Within the Housing First approach, there are two models of case management that are commonly used – these include assertive community treatment [ACT] and intensive case management [ICM]. Both approaches are designed to assist people who have high levels of support needs. According to the ICM Toolkit developed by Employment and Social Development Canada (2018), “Providing Housing First intensive case management to high acuity clients is a complex process. Each agency, area and client population has its own unique strengths and challenges, and each program will need to be flexible, innovative and responsive. Housing First intensive case management is a constantly changing process, with ongoing learning at every stage. This important work provides vulnerable individuals with housing, support, dignity and safety, and will empower them to live the best life possible and reach their inherent potential” (pg. 38).
Intensive case management provides a higher level of on-going support compared to the more traditional case management approach discussed in the chapter on Social Work. These case managers will help people who have severe mental illness and/or addiction issues to become and remain stably housed by assisting with their daily support needs. For example, an intensive case manager may accompany a person to medical appointments, help them create a budget for their household, go grocery shopping with them, and help them to ensure their home is properly cared for. They may also need to advocate for individuals who have severe mental illness and as result of previous behaviour have been banned from service agencies or parts of the community. Their key role is to offer on-going and (as the name suggests) intensive levels of support. The following video from the Canadian Mental Health Association of Toronto shows how they use intensive case management to support clients in their Housing First program.
In comparison, assertive community treatment is similarly designed to assist people who have high acuity and complex support needs but is conducted as a team-based approach. In this model, a diverse team of professionals works to support the various needs clients may have. The principles of an assertive community treatment team include that they work collaboratively to deliver mental health services to a group of consumers, that consumer needs direct the delivery of care, service is targeted to the population most in need, the team works assertively and flexibly to provide outreach rather than expecting consumers to come to services, and the treatment is designed to prevent hospitalization and help consumers live successfully in the community (Government of British Columbia, n.d.). The following video was created by Gwen Haworth and shows how assertive community treatment is used as a model of care in RainCity Housing’s program in Vancouver.
Intensive case managers work with a smaller caseload of clients than traditional case managers and provide their clients with more frequent and on-going support. Assertive community treatment is done by a team of diverse professionals who provide different types of support to clients who have complex needs in the community. What do you think the benefits of each approach are? Why do you think some Housing First programs use intensive case management while others use assertive community treatment?
Dr. Nick Kerman has conducted research on Housing First and mental health recovery. He and his team examined predictors of recovery for people with mental illness using longitudinal Housing First data and found that the most effective interventions were aimed at preventing chronic homelessness, strengthening social networks, increasing community involvement, and providing case management services (Kerman, Sylvestre, Aubry, & Schütz, 2019). Dr. Kerman and his team further found through a multi-site randomized controlled trial that Housing First is effective in helping people with mental illness, who frequently use emergency hospital services, to become stably housed (Kerman et al., 2020). In the next video, Dr. Kerman discusses the evidence base and role of intensive case management and assertive community treatment in helping people with mental illness move into secure housing.
In this video, Dr. Nick Kerman explains that there are a wide range of treatments for mental health, that generally fall into the categories of individual treatments and medication. He notes that within the context of homelessness, it is important to recognize that the best way to promote wellness and treat mental health problems is to get people into safe and secure housing. Once housed, Dr. Kerman explains that assertive community treatment [ACT] and intensive case management [ICM] are two evidence-based approaches that improve wellness, depending on the person’s level of support needs. Dr. Kerman concludes that when talking about mental wellness it is important to recognize the importance of preventing mental health problems and promoting positive well-being. This video is 4:25 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: What are the treatments that improve mental health, and do they work?
Ponka et al., (2020) have conducted a systematic review of the effectiveness and cost-effectiveness of different case management intervention styles on the health and social outcomes for people experiencing homelessness. Among their conclusions was that intensive case management significantly reduced the number of days a person spent homeless, and that assertive community treatment had promising effects on housing stability and was more cost-effective than more traditional case management styles. We invite you now to learn more about how these different case management styles compare for helping people with mental illness move out of homelessness, in this section’s featured reading below.
Ponka, D., Agbata, E., Kendall, C., Stergiopoulos, V., Mendonca, O., Magwood, O… & Pottie, K. (2020). The effectiveness of case management interventions for the homeless, vulnerably housed and persons with lived experience: A systematic review. PLoS ONE, 15(4): e0230896.
Housing is a key social determinant for health and mental health. You may be sick of us saying that, but we persist in repeating ourselves because it is true, and we want you to remember it. We have seen that Housing First has become an increasingly popular approach for connecting people with housing and offering supports through intensive case management or assertive community treatment. Dr. Tim Aubry was a lead researcher on the original At Home / Chez Soi study and has continued to conduct evaluations of the Housing First approach. We conclude this section with a video of Dr. Aubry discussing what the research shows about the effectiveness of Housing First for helping people who have mental health issues become securely housed.
In this video, Dr. Tim Aubry explains that community mental health treatments and programs are proven to be effective for people experiencing homelessness who have mental health issues. He identifies assertive community treatment [ACT] and intensive case management [ICM] as the two approaches that most effectively support people to exit chronic homelessness, with the approach determined based on the person’s level of support needs. Dr. Aubry notes that these approaches have a long history of demonstrated effectiveness. When paired with Housing First supports, such as rent supplements and housing choice, they show success rates as high as 85% – 90%. This video is 3:52 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: What are the treatments that improve mental health, and do they work?
In this section we examined the question of what treatments exist to help people and whether they are effective for people experiencing homelessness. We found through the literature and researcher interviews that there are many different approaches that have shown promise. Most notably these include the community reinforcement approach and motivational enhancement therapy (Brakenhoff & Slesnick, 2018), mindfulness practice and cognitive behavioural therapy (Brown & Bender, 2018), dialectical behaviour therapy (McCay & Aiello, 2018), community-based population mental health interventions (Barbic et al., 2018; Simpson et al., 2018), and recovery education centres (Durbin et al., 2019; Reid et al., 2020). These are all clinical interventions that can help people who experience homelessness and are living with mental illness.
Along the way, we heard the message that what matters more than the specific approach used, is that the intervention is tailored to the expressed needs of the individual. People may be at different levels of willingness and ability to engage in therapeutic practices because of factors like inadequate housing, a lack of rest, poor nutrition, and low social support. These are key reasons why we have heard – and argue strongly – that housing is a primary social determinant of health that needs to be addressed for people to get well. This is the premise of Housing First, which connects people with housing and then provides support through either intensive case management or assertive community treatment, depending on the needs and wishes of the client.
We have seen throughout this chapter that people who experience homelessness often have poor mental health. This may begin while they are housed or may be the result of the trauma and stress that characterize many people’s experiences of homelessness. While there are different pathways to recovery, and they must be traversed at each individual’s own speed, it is promising to know that there are interventions and approaches that have shown success. It is important that we continue to seek ways to improve the mental health of people experiencing homelessness, and this must begin with providing safe, secure, and affordable housing.
Click the link below to listen to all of the researchers answer the question “What are the treatments, and do they work?” in audio format on our podcast!
41
Arin and Tanzia
Let’s return to the two people we met at the beginning of the chapter. Arin is an individual who has underlying mental health issues and struggles with stability in many aspects of their life, including housing. Tanzia is an individual who has had significant challenges with substance use, changing mental health circumstances, and subsequently a long history of unstable housing.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1182#h5p-87
42
We began this chapter on Mental Health with the age-old riddle of, what comes first the chicken or the egg? This riddle is often posed in relation to mental illness and homelessness because the two are so closely intertwined that it can be challenging to tease them apart. Often people experience poor mental health that results in housing loss and then gets exacerbated by the stress and trauma of homelessness. Throughout this chapter, we considered the prevalence, reasons, and possible treatments for people living with mental illness and experiencing homelessness.
At the start of the chapter, we introduced you to the composite characters Arin and Tanzia who were each experiencing homelessness in their own unique way. The scenarios were presented as an entry point for thinking about the complexity of homelessness as it relates to poor mental health. We returned to these individuals’ stories again at the end to demonstrate how they can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada.
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “What is the prevalence of mental health issues for people who experience homelessness?” Here we saw a diverse range of estimates that emerge from research using different parameters for inclusion. Should we consider only people with diagnosed mental illness or should we open it up and also consider people who are generally mentally unwell? These factors shape estimates, that range as low as 10% to as high as 100%. What we know is that the rates of mental health issues are significantly higher for people experiencing homelessness than amongst those who are housed, and that despite this, their access to mental health services remains low. Homelessness is a traumatic experience that makes it nearly impossible to maintain mental wellness.
Next we asked, “Why is mental illness so high among people experiencing homelessness?” We began with the important message that people who experience homelessness live in a constant state of crisis, having to meet their daily needs without the security of a reliable place to live. The mass number of people living with mental illness and navigating service agencies was traced to historical decisions such as the deinstitutionalization of psychiatric patients at a time when cuts were being made to social housing and income supports. We saw through this section that people who experience homelessness are often isolated, lonely, and report a lack of meaningful activities in their lives. These feelings can lead to poor mental health and greatly increase the risk of suicidal ideation and suicide attempts, particularly amongst young people, and markedly those who identify as LGBTQ2S+. When people lose their housing, they often also lose the identities associated with it, like being married, a parent, or employed, which get replaced by discriminatory and harmful labels. While people who experience homelessness often show remarkable personal strength in these situations, the institutions within our society still have a long way to go in providing coordinated and integrated mental health services for them.
Finally, we asked, “What are the treatments that improve mental health, and do they work?” Throughout this chapter, we discussed many difficult realities of life for people who experience homelessness. The trauma and daily stressors of operating in a constant state of crisis create the conditions for poor mental health and possible mental illness diagnoses. We concluded, in this this last section, by taking a more hopeful approach and looking at some of the interventions that have shown promise for this population. Most notably, we saw that building relationships, the community reinforcement approach and motivational enhancement therapy, mindfulness practice and cognitive behavioural therapy, dialectical behaviour therapy, community-based population mental health interventions, and recovery education centres are all approaches that can help people who experience homelessness and are living with mental illness. Regardless of which method is used, we saw that what matters most is that it is tailored to the needs of the client and progresses at their own pace. In the final part of this section, we saw how Housing First offers people with mental illness the opportunity to identify and work on their mental health needs after becoming securely housed, through the assistance of either intensive case management or assertive community treatment. We ended this section – and will end this chapter – with the critical message that housing is the most fundamental social determinant of health and mental health. If we want to help people become mentally well, we need to begin with ensuring they have a safe and secure place in which to recover.
43
Here are some additional resources you may want to check out!
44
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
45
Barbic, S. P., Kidd, S. A., Durisko, Z. T., Yachouh, R., Rathitharan, G., & McKenzie, K. (2018). What are the personal recovery needs of community-dwelling individuals with mental illness? Preliminary findings from the Canadian personal recovery outcome measurement (C-PROM) study. Canadian Journal of Community Mental Health, 37(1), 29-47. https://www.cjcmh.com/doi/pdf/10.7870/cjcmh-2018-005
Brakenhoff, B., & Slesnick, N. (2018). Substance use and mental health interventions for youth who are homeless: The community reinforcement approach and motivational enhancement therapy. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Brown, S. M., & Bender, K. (2018). Mindfulness approaches for youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Durbin, A., Kapustianyk, G., Nisenbaum, R., Wang, R., Aratangy, T., Khan, B., & Stergiopoulos, V. (2019). Recovery education for people experiencing housing instability: An evaluation protocol. International Journal of Social Psychiatry, 65(6), 468–478. https://doi.org/10.1177/0020764019858650
Ecker, J., & Aubry, T. (2017). A mixed methods analysis of housing and neighbourhood impacts on community integration among vulnerably housed and homeless individuals. Journal of Community Psychology, 45(4), 528–542. https://doi.org/10.1002/jcop.21864
Ecker, J., Cherner, R., Rae, J., & Czechowski, K. (2018). Sexual intimacy, mental illness, and homelessness. American Journal of Community Psychology, 61(1-2), 131–140. https://doi.org/10.1002/ajcp.12213
Employment and Social Development Canada. (2018). Toolkit for intensive case management in Canada: A resource for those using a case management program for the housing first model. Canada: Government of Canada.
Gauvin, G., Labelle, R., Daigle, M., Breton, J. J., & Houle, J. (2019). Coping, social support, and suicide attempts among homeless adolescents. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 40(6), 390–399. https://doi.org/10.1027/0227-5910/a000579
Gentil, L., Grenier, G., & Fleury, M. J. (2021). Determinants of suicidal ideation and suicide attempt among former and currently homeless individuals. Social Psychiatry and Psychiatric Epidemiology, 56(5), 747–757. https://doi.org/10.1007/s00127-020-01952-3
Gicas, K. M., Cheng, A., Panenka, W. J., Kim, D. D., Yau, J. C., Procyshyn, R. M., … Barr, A. M. (2021). Differential effects of cannabis exposure during early versus later adolescence on the expression of psychosis in homeless and precariously housed adults. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 106, 110084–110084. https://doi.org/10.1016/j.pnpbp.2020.110084
Goering, P., Veldhuizen, S., Watson, A., Adair, C., Kopp, B., Latimer, E., Nelson, G., MacNaughton, E., Streiner, D., & Aubry, T. (2014). National at home / chez soi final report. Calgary, AB: Mental Health Commission of Canada. National At Home/Chez Soi Final Report | The Homeless Hub
Government of British Columbia. (n.d.). B.C.’s mental health reform, assertive community treatment best practices. BC, Government of British Columbia, Ministry of Health and Ministry Responsible for Seniors. Assertive Community Treatment Guidelines for BC (gov.bc.ca)
Jones, P. W., Thornton, A. E., Jones, A. A., Knerich, V. M., Lang, D. J., Woodward, M. L., … Gicas, K. M. (2020). Amygdala nuclei volumes are selectively associated with social network size in homeless and precariously housed persons. Frontiers in Behavioral Neuroscience, 14, 97–97. https://doi.org/10.3389/fnbeh.2020.00097
Kerman, N., Aubry, T., Adair, C. E., Distasio, J, Latimer, E., Somers, J., & Stergiopoulos, V. (2020). Effectiveness of housing first for homeless adults with mental illness who frequently use emergency departments in a multisite randomized controlled trial. Administration and Policy in Mental Health Services Research, 47, 515-525. https://doi.org/10.1007/s10488-020-01008-3
Kerman, N., & Kidd, S. A. (2020). The healthcare triple aim in the recovery era. Administration and Policy in Mental Health and Mental Health Services Research, 47, 492-496. https://doi.org/10.1007/s10488-019-00997-0
Kerman, N., & Sylvestre, J. (2020). Surviving versus living life: Capabilities and service use among adults with mental health problems and histories of homelessness. Health & Social Care in the Community, 28(2), 414–422. https://doi.org/10.1111/hsc.12873
Kerman, N., Sylvestre, J., Aubry, T., & Schütz, C. G. (2019). Predictors of mental health recovery in homeless adults with mental illness. Community Mental Health Journal, 55(4), 631–640. https://doi.org/10.1007/s10597-018-0356-3
Kidd, S. A., Gaetz, S., & O’Grady, B. (2017). The 2015 national Canadian homeless youth survey: Mental health and addiction findings. The Canadian Journal of Psychiatry, 62(7), 493-500. https://doi.org/10.1177/0706743717702076
Kidd, S. A., Gaetz, S., O’Grady, B., Schwan, K., Zhao, H., Lopes, K., & Wang, W. (2021). The second national Canadian homeless youth survey: Mental health and addiction findings. The Canadian Journal of Psychiatry, 66(10), 897-905. https://doi.org/10.1177%2F0706743721990310
Lévesque, I. S., & Abdel-Baki, A. (2020). Homeless youth with first-episode psychosis: A 2-year outcome study. Schizophrenia Research, 216, 460–469. https://doi.org/10.1016/j.schres.2019.10.031
Liu, M., Mejia-Lancheros, C., Lachaud, J., Latimer, E., Aubry, T., Somers, J., … Hwang, S. W. (2021). Overall and gender-specific associations between dimensions of adverse childhood experiences and mental health outcomes among homeless adults. Canadian Journal of Psychiatry, 706743721989158–706743721989158. https://doi.org/10.1177/0706743721989158
Maremmani, A. G. I., Bacciardi, S., Somers, J. M., Nikoo, M., Schütz, C., Jang, K. L., & Krausz, M. (2018). Substance dependence among bipolar, unipolar depression and psychotic homeless: A Canadian national study. Frontiers in Psychiatry, 9, 701–701. https://doi.org/10.3389/fpsyt.2018.00701
Marshall, C. A., Keogh-Lim, D., Koop, M., Barbic, S., & Gewurtz, R. (2020a). Meaningful activity and boredom in the transition from homelessness: Two narratives. Canadian Journal of Occupational Therapy (1939), 87(4), 253–264. https://doi.org/10.1177/0008417420941782
Marshall, C. A., Roy, L., Becker, A., Nguyen, M., Barbic, S., Tjörnstrand, C., … Wickett, S. (2020b). Boredom and homelessness: A scoping review. Journal of Occupational Science, 27(1), 107–124. https://doi.org/10.1080/14427591.2019.1595095
McCay, E., & Aiello, A. (2018). Dialectical behaviour therapy to enhance emotional regulation and resilience among street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Mejia-Lancheros, C., Lachaud, J., O’Campo, P., Wiens, K., Nisenbaum, R., Wang, R., Hwang, S. W., & Stergiopoulos, V. (2020) Trajectories and mental health-related predictors of perceived discrimination and stigma among homeless adults with mental illness. PLoS ONE, 15(2), e0229385. https://doi.org/10.1371/journal.pone.0229385
Montgomery, P., Mossey, S., & McCauley, K. (2019). Priorities for supportive housing services: Perspectives of people with mental illness in northeastern Ontario. Canadian Journal of Nursing Research, 51(4), 264–273. https://doi.org/10.1177/0844562119835730
Ponka, D., Agbata, E., Kendall, C., Stergiopoulos, V., Mendonca, O., Magwood, O… & Pottie, K. (2020). The effectiveness of case management interventions for the homeless, vulnerably housed and persons with lived experience: A systematic review. PLoS ONE, 15(4): e0230896. https://doi.org/10.1371/journal.pone.0230896
Reid, N., Khan, B., Soklaridis, S., Kozloff, N., Brown, R., & Stergiopoulos, V. (2020). Mechanisms of change and participant outcomes in a recovery education centre for individuals transitioning from homelessness: A qualitative evaluation. BMC Public Health, 20(1), 497–497. https://doi.org/10.1186/s12889-020-08614-8
Schütz, C., Choi, F., Jae Song, M., Wesarg, C., Li, K., & Krausz, M. (2019). Living with dual diagnosis and homelessness: Marginalized within a marginalized group. Journal of Dual Diagnosis, 15(2), 88–94. https://doi.org/10.1080/15504263.2019.1579948
Schwan, K., Kidd, S., Gaetz, S., O’Grady, B., & Redman, M. (2017). Mental health care for homeless youth: A proposal for federal, provincial, and territorial leadership, coordination, and targeted investment. Toronto: Canadian Observatory on Homelessness Press. Canadian Observatory On Homelessness Policy Brief (homelesshub.ca)
Shankar, S., Gogosis, E., Palepu, A., Gadermann, A. M., & Hwang, S. W. (2019). “I haven’t given up and I’m not gonna”: A phenomenographic exploration of resilience among individuals experiencing homelessness. Qualitative Health Research, 29(13), 1850–1861. https://doi.org/10.1177/1049732318798353
Simpson, A., Furlong, A., & Jetha, N. (2018). At-a-glance: Bringing equity into the fold: A review of interventions to improve mental health. Health Promotion and Chronic Disease Prevention in Canada, 38(10), 380–384. https://doi.org/10.24095/hpcdp.38.10.04
Smith, E., Milaney, K., Henderson, R. I., & Crowshoe, L. (2021). Adverse childhood experiences and health among indigenous persons experiencing homelessness. BMC Public Health, 21(1), 85–85. https://doi.org/10.1186/s12889-020-10091-y
Thulien, N. S., Gastaldo, D., Hwang, S. W., & McCay, E. (2018). The elusive goal of social integration: A critical examination of the socio-economic and psychosocial consequences experienced by homeless young people who obtain housing. Canadian Journal of Public Health, 109, 89-98. https://doi.org/10.17269/s41997-018-0029-6
Thulien, N. S., Gastaldo, D., McCay, E., & Hwang, S. W. (2019). “I want to be able to show everyone that it is possible to go from being nothing in the world to being something”: Identity as a determinant of social integration. Children and Youth Services Review, 96, 118-126. https://doi.org/10.1016/j.childyouth.2018.11.005
Thulien, N. S., Wang, A., Mathewson, C., Wang, R., & Hwang, S. W. (2021). Tackling exclusion: A pilot mixed method quasi-experimental identity capital intervention for young people exiting homelessness. PLOS ONE. https://doi.org/10.1371/journal.pone.0256288
Vogel, M., Nikoo, M., Nikoo, N., Schütz, C. G., Walter, M., Somers, J., & Krausz, M. (2019). Association of substance use patterns with psychiatric disorders in homeless persons with psychiatric disorders in Vancouver. Int J Ment Health Addiction 17, 1200–1213. https://doi.org/10.1007/s11469-018-0040-4
Yazdani, K., Nikoo, M., Sayre, E. C., Choi, F., Jang, K., & Krausz, R. M. (2020). The impact of employment on recovery among individuals who are homeless with severe mental illness in the Vancouver at home / chez soi trial. Social Psychiatry and Psychiatric Epidemiology, 55(12), 1619–1627. https://doi.org/10.1007/s00127-020-01887-9
V

If you have turned on the TV, read the news, or scrolled through social media in recent years you have encountered a story about public health. The primary goal of public health is to support a population to be as healthy as possible, through the non-judgmental implementation of programs and interventions. Perhaps the most obvious public health story to dominate the news cycle in 2020 and beyond is that of the COVID-19 pandemic. We have been reminded to sanitize our hands, wear masks, and keep our distance.
However, there is another epidemic – that of drug overdoses – that is occurring in communities across Canada. Although COVID-19 has received more national attention, both are pressing public health issues that impact our society, with unique ramifications for individuals experiencing homelessness. As you work through this chapter you are asked to think about the health of individuals experiencing homelessness on a population level and learn how public health measures are being implemented to improve their well-being.
46
In this chapter, you are invited to consider how individuals who experience homelessness may be thought of as a population, and the ways in which public health measures can be enacted to promote their health and wellness. Our discussion is directed by three key questions that guide this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that adopting a public health lens requires us to think about issues such as vulnerability to a pandemic and substance use as being rooted in the organization of society, rather than as an outcome of individual behaviour or choices. Read on to learn more about how homelessness is a public health issue and what measures can be put in place to improve well-being at a population level.
47
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to public health studies. As you work through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After pausing to think about a set of reflection questions, we will endeavour to answer each question posed in the learning objectives. Why are people who experience homelessness at higher risk during a pandemic? How is drug use a public health issue? Why is a harm reduction approach necessary? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
48
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider these people’s experiences.
Stephan and Zane
Stephan and Zane are a young couple. They met at college where they were each completing a course in heavy machinery repair. Upon graduation neither was able to find a job in their field. They have bounced from one construction job to the next, often being paid in cash. No contracts, no benefits. Staggering debts from their education have left them unable to sustain permanent housing. They have been marginally involved with some recreational drug use; however, they have recently lost three friends to overdose and are frightened.
They are currently living in a shelter in a medium-sized city. They would like to get out west as they have heard that there are jobs there but have no money to fund this move and no solid prospects. In the shelter, they are sleeping in a dormitory style room with 12 other men. Cots are lined up close together, head-to-head.
There is no private space. Shower and clothes washing facilities are very limited. Each person is given a mask to last the week. Hand wash stations are few and far between. They have just learned that one of the residents has tested positive for COVID-19 meaning that all residents will have to isolate “at home” for 14 days. Although the shelter has a “no drug” policy, drug use is very prevalent in the surrounding community.
Stephan and Zane are feeling very confused, isolated, and unsafe.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to this scenario again at the end of the chapter.
Reflection Questions
49
The chances are pretty good that you have heard about the COVID-19 pandemic, so we will not devote a considerable amount of space to explaining its particulars. It should suffice to contextualize it as a worldwide outbreak that emerged in 2019 and continued at least up until the time this book was being written in the late Fall of 2021. Whether you are reading this while the effects of the COVID-19 pandemic are still being felt around the world, or whether you are fortunate to be reading this in a post COVID-19 era, we encourage you to take a moment here to think about its impact on people experiencing homelessness. This reflection may be as brief or as long as you wish.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=705#h5p-44
 Photo by Alex Azabache on Unsplash Photo by Alex Azabache on Unsplash |
When you think of COVID-19, what comes to mind? Perhaps you recall the many messages we all commonly heard during this period:
All good advice, if you have a home, the ability to stay away from others, hygiene facilities in which to wash, access to multiple masks or laundry facilities, and have been given priority vaccination status. Based on what you have learned so far in this book, how much of this advice do you think applies to people experiencing homelessness?
The importance of having safe and secure housing as a determinant of health became abundantly clear during the COVID-19 lockdowns that were implemented across Canada, and more broadly around the world. You may recall hearing that people experiencing homelessness are at increased risk during a pandemic. Indeed, this risk is two-fold. They are medically at risk because of a high rate of underlying chronic health conditions, and socially at risk because of a lack of housing and control over their living environments which makes it particularly challenging to follow public health directives like staying at home and keeping one’s distance (Perri, Dosani, & Hwang, 2020). In the video that follows Dr. Rebecca Schiff discusses these medical and social conditions in more detail.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Rebecca Schiff argues that there are several reasons people who experience homelessness are at higher risk during a pandemic. Notably, she states the COVID-19 pandemic demonstrated that having a home or private space is the safest place to avoid infection, but those who experience homelessness do not have this same access. Additionally, shelters are congregate settings where people live and work in close quarters, increasing the risk of transmission. Lastly, people who experience homelessness are often in poor health and may lack a strong immune system to fight off infection. This video is 1:54 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: Why are people who experience homelessness at higher risk during a pandemic?
It has become commonplace to use the terms, “COVID-19” and “the pandemic” interchangeably, but it is critical to recognize that there have been pandemic outbreaks in previous years, such as SARS in 2003 and H1N1 in 2009-2010. During the H1N1 pandemic, a team of researchers from across Canada conducted a multi-site study to evaluate the readiness of homelessness sectors to deal with infectious outbreaks. This study took place in Victoria (Pauly, Perkins, & Cross, 2016), Toronto (Buccieri, 2016; Gaetz & Buccieri, 2016), Calgary (Waegemakers Schiff & Lane, 2016), and Regina (Schiff, 2016b).
Writing about this study, Gaetz and Buccieri (2016) indicated that we need to consider the ways the infrastructure we have built to respond to homelessness – such as crowded shelters, congregate sleeping and eating spaces, and inadequate onsite hygiene facilities – organize the lives of people within these spaces in a way that increases their risk while simultaneously reducing their sense of control. The findings of this study were published in an open access e-book entitled “Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada“, which is freely available on the Homeless Hub website (Buccieri & Schiff, 2016).
This book was released in October 2016. As part of its launch, the co-editors Dr. Rebecca Schiff and Dr. Kristy Buccieri wrote a conversational blog post discussing the importance of pandemic planning for people experiencing homelessness and the impact they hoped the book would have for pandemic planning and preparedness in the future. We invite you to read the blog post now while keeping in mind that this was written many years before the COVID-19 outbreak.
Click the image below to open a new window and read the full blog post, “What did Canada learn about homelessness from H1N1?” by Dr. Rebecca Schiff and Dr. Kristy Buccieri.
 |
Reflecting on the H1N1 outbreak in Toronto, Gaetz and Buccieri (2016) have written, “A key question to ask is whether we are prepared – or more to the point, is it possible to prepare – to adequately respond to the risks faced by the homeless population in the event of a serious pandemic?” This piece of foreshadowing was written well before the COVID-19 outbreak began. Looking backward, do you think we were adequately prepared to respond to the risks of COVID-19 for people experiencing homelessness? Was it possible to be more prepared?
Lead co-researchers on the project, Dr. Jeannette Waegemakers Schiff, Dr. Bernie Pauly, and Dr. Rebecca Schiff wrote in the book, “We hope, in the event of future pandemics, the important lessons from H1N1, an outbreak that did not turn out to be as severe as expected, will be taken up by regional and provincial health planners to ensure the health and safety of people who are homeless. There is also a clear need to initiate a public health response to homelessness, even when there is no imminent threat of a pandemic” (Waegemakers Schiff, Pauly, & Schiff, 2016, pg. 180). Here Dr. Jeannette Waegemakers Schiff shares her thoughts on the COVID-19 outbreak and the lessons not learned from H1N1.
In this video, Dr. Jeannette Waegemakers Schiff reflects on the increased psychological, moral, and physical harm that people who are unsheltered face during a pandemic. She notes that while people are told to stay home, those without housing are unable to shelter in place and lack the ability to store food and other essential supplies. She argues that people who experience homelessness are at greater risk of not being able to take self-protective measures, such as remaining socially distant in congregate service settings. Additionally, while people who are unsheltered are at increased risk of exposure, they also have fewer protections. For instance, access to disposable masks or laundry facilities for cloth masks is limited in homelessness agencies. Dr. Waegemakers Schiff notes that during COVID-19 many service agencies struggled to meet the needs of their clients. While some were prepared and able to implement social distancing measures, many people still were left sleeping on mats on the floor, next to others. In response, some cities moved unsheltered people who tested positive or showed symptoms of having COVID-19 to hotels to quarantine. While Dr. Waegemakers Schiff notes that the public health need for this was clear, additional considerations should have been made for individuals who had previously been incarcerated and/or who use substances and might find the hotel quarantine protocols overly restrictive. This video is 7:05 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: Why are people who experience homelessness at higher risk during a pandemic?
The current way we manage homelessness – by keeping strangers close together in overcrowded settings with limited hygiene facilities – is the complete opposite of what public health officials advise in pandemic outbreaks. While the COVID-19 pandemic impacted society as a whole, homelessness shelters and agencies are often plagued by outbreaks of tuberculosis, influenza, lice, and bed bugs. An investigation of risk factors for Group A Streptococcus outbreak in shelters showed the need for improved wound care, infection prevention and control practices, early screening and detection of skin and soft tissue infections (Dohoo, Stuart, Finkelstein, Bradley, & Gournis, 2020), which is outside the scope of care most shelters are able to provide. In the next video, Dr. Stephen Hwang discusses infection, displacement, and the broad range of factors that put people at particularly high risk when experiencing homelessness during a pandemic.
In this video, Dr. Stephen Hwang tells the story of a research associate who was surprised at the congregate nature of shelters and drop-in centres during the COVID-19 pandemic. Dr. Hwang notes that the pandemic did not create, but rather unmasked, the conditions that were already present increasing the risk of airborne and droplet born diseases in these settings. He argues that while infection is a concern, there are also a range of additional risks people who experience homelessness face during a pandemic, related to displacement and the lack of access to basic services. Notably, he cites the lack of access to washrooms, higher rates of overdose deaths, increased levels of stress, and impaired mental health as particular risk factors for people experiencing homelessness. Dr. Hwang concludes that for those living in encampments, routine clearances have led not only to displacement but to the disruption of social and support networks as well. This video is 3:11 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Why are people who experience homelessness at higher risk during a pandemic?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=705#h5p-45
Given the standard crisis–management approach to homelessness, it is not surprising that there were outbreaks of COVID-19 within shelters across Canada. In the brief clip that follows, from Global News, we take a look at the crisis scenarios that unfolded across the country.
Many cities and regions implemented measures to provide spaces for people experiencing homelessness, to promote physical distancing, and to provide isolation or quarantine services (Perri, Dosani, & Hwang, 2020). Some cities attempted to create alternative spaces, like the igloos seen in the video above, or the use of hotels to provide temporary private accommodations. We also witnessed the rise of tent encampments – and their subsequent demolition – in many cities, as people experiencing homelessness tried to create safer spaces for themselves. We will take a closer look at encampments in the chapter on Sociology & Crimino-Legal Studies.
During the COVID-19 pandemic, researchers monitored the outbreak in different ways. They outlined plans to compare screening strategies in shelters (O’Shea et al., 2020), reviewed administrative health data (Richard et al., 2021), and undertook retrospective chart audits within shelters (Kiran et al., 2021). In Toronto, researchers found that among 504 COVID-19 tests completed in homelessness shelters between April and July 2020, 14% were positive (Kiran et al., 2021). Another study found that people with a recent history of homelessness were more likely to be tested for COVID-19 and to have a positive test result (Richard et al., 2021). In the peak period, people who had a recent history of homelessness were over 20 times more likely to be admitted to hospital for COVID-19, over 10 times more likely to require intensive care for COVID-19, and over 5 times more likely to die within 21 days of their first positive test result (Richard et al., 2021). In the next video a member of this project’s team, Dr. Cheryl Forchuk, speaks about the research.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk argues there are many reasons people who experience homelessness are at higher risk during a pandemic. From a general health perspective, she notes, these individuals often have impaired nutritional status, prolonged exposure to the elements, compromised sleep, and may use substances. Dr. Forchuk notes that while conducting research during the pandemic, her team found that people experiencing homelessness were not being prioritized for vaccination; they published a paper as a form of advocacy and noticed within days the group was being given priority. She concludes by noting that because social service agencies tend to be congregate settings, the residents and staff are often sick and that the COVID-19 pandemic highlighted issues within the homelessness sector that already existed. This video is 3:28 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Why are people who experience homelessness at higher risk during a pandemic?
Dr. Forchuk’s team demonstrated the importance of rapid peer-reviewed publications informing policy decisions. We invite you to pause here and read the article she spoke about that demonstrated the high–risk conditions of people experiencing homelessness and need for priority vaccination.
Richard, L., Booth, R., Rayner, J., Clemens, K. K., Forchuk, C., & Shariff, S. Z. (2021). Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: A retrospective cohort study. CMAJ Open, 9(1), E1–E9.
It is important to remember, as you learn about homelessness, that managing a pandemic outbreak in this context is deeply challenging. During H1N1 social service workers were often expected to take on health-care related roles despite not being formally trained or equipped to do so. Access to supplies was a commonly cited concern, related to confusion over what supplies were needed, the cost of purchasing them outside a regular budget, and not having enough storage to stockpile and meet demand (Buccieri, 2020).
In a pandemic, frontline workers are asked to take on crisis management roles, but homelessness itself is always a crisis situation (Schiff, 2016a). This makes planning for a crisis – on top of managing an already existing crisis – an astronomically difficult task. During the COVID-19 lockdown, research from Nova Scotia showed that social workers continued to work remotely and tirelessly trying to find housing for their clients amidst dire circumstances (Wu & Karabanow, 2020). This high level of commitment and dedication is likely a large part of the reason why in a sample of 701 direct service providers in homelessness agencies, 80% reported a decline in their mental health during the pandemic (Kerman, Ecker, Gaetz, Tiderington, & Kidd, 2021).
At the same time, that frontline workers are struggling to manage client needs and their own well-being, closing services entirely risks even greater harm, such as related to unsafe substance use and intimate partner violence (Perri, Dosani, & Hwang, 2020). During a pandemic, there are some populations experiencing homelessness that may be even more marginalized than others. Notably, women and girls are at risk of socio-economic exclusion in a pandemic because of the disproportionate burden of poverty, inequitable childcare responsibilities, and proliferation of violence against women (Schwan, Dej, & Versteegh, 2020). Those living in rural and remote communities are also at high risk, particularly if services shut down, because they have limited alternative places to seek help (Schiff, 2016; Schiff, Buccieri, Waegemakers Schiff, Kauppi, & Riva, 2020). In the next video, Dr. Bernie Pauly explains that the COVID-19 pandemic highlighted the deep inequities and disparities between people in society.
In this video Dr. Bernadette [Bernie] Pauly argues that the lack of adequate housing options increases vulnerability during a pandemic. For instance, during the COVID-19 pandemic, people who were couch surfing may not have been able to find a place to stay and many shelters reduced the clients they served to meet physical distancing requirements. She notes that individuals experiencing homelessness also had increased vulnerability because they were unable to implement basic protective measures. Some agencies closed access to their washrooms, and some cities turned off the water in public places, meaning those without housing were largely unable to wash their hands. Dr. Pauly argues that the public health messaging to ‘stay at home’ is not useful to those without housing and that permitting people to stay in tents does not guarantee they will have access to food and water. She concludes that people who experience homelessness lack access to the basic social determinants of health and that the COVID-19 pandemic highlighted the existing disparities between these individuals’ level of need and housed individuals, who had the privilege of time at home to start new hobbies. This video is 3:18 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: Why are people who experience homelessness at higher risk during a pandemic?
COVID-19 messaging often conveyed the idea that “we are all in this together,” such as to encourage people to do their part by staying home and reducing the spread.However, some individuals faced additional social and medical risks. In the chapter on Politics, Policy, & Housing in Canada, we noted that Canada has passed legislation declaring housing a basic right. How do you think the COVID-19 pandemic would have been different if every Canadian were housed?
In this section, we asked you to consider why people who experience homelessness are at higher risk during a pandemic. We began by considering the public health messages we hear, such as to stay home, keep your distance, and change your mask, which are difficult requests to make of people living in congregate shelter settings with limited resources. Indeed, it is the combination of social determinants, like poor living conditions, and medical factors that make people who experience homelessness doubly at risk during a pandemic. The COVID-19 pandemic has highlighted the importance of housing as a social determinant of health and it also raises the question of whether our current emergency-based approaches to addressing homelessness should be re-evaluated (Perri, Dosani, & Hwang, 2020).
While we learned a lot about how pandemics impact people experiencing homelessness from the previous H1N1 outbreak, many cities were unprepared to deal with the COVID-19 outbreak in homelessness sectors. In large part this is because homelessness is already a crisis that the sector is trying to manage. The design of many services, where people sleep and eat in close proximity, is contrary to public health advice and creates the conditions for rapid spread of disease. We saw that people who experience homelessness were 20 times more likely to be hospitalized, 10 times more likely to require intensive care, and 5 times more likely to die from COVID-19 than housed individuals (Richard et al., 2021). Amidst these outbreaks, service providers worked diligently at the expense of their own mental wellness to continue supporting clients. The need for housing, addictions, and mental health programming to continue was dire, particularly for subgroups, like women and those living in rural communities. COVID-19 highlighted many existing social inequities in Canada. People who use drugs are amongst the most discriminated against in society, and this was readily apparent in the high rates of overdose deaths that occurred during the pandemic.
Click the link below to listen to all of the researchers answer the question “Why are people who experience homelessness at a higher risk during a pandemic?” in audio format on our podcast!
50
Although this is not a chapter on Sociology, we begin this section by drawing on the work of Charles Wright Mills (1967), as he describes the Sociological Imagination as the ability to understand personal troubles as public issues. Public health lends itself nicely to the challenge of broadening our perspectives and thinking beyond our own experience. Drug use, or substance use more broadly, has long been vilified in our society. Think, for instance, of prohibition days and the discriminatory stereotypes that it has bred about people who use drugs.
Before you continue through this section, we encourage you to pause here and take up Mills’ challenge of thinking about this issue at a societal level. While we know that drug use may be a personal trouble, it is also a public issue that affects our society as a whole. How do you think drug use is a public health issue? Use the space below to write your response. It may be as brief or as long as you wish.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=707#h5p-46
We are told from the time we are children that drugs are bad. This message is not just something we encounter passively, but rather it is actively marketed to us. In the early 1990s there was a public service announcement, in which children danced around in a circle to a catchy little tune (that even 30 years later still gets stuck in one’s head) that goes, “Drugs, drugs, drugs. Which are good? Which are bad? Drugs, drugs, drugs. Ask your mom or ask your dad.” If you have heard this song, it is no doubt stuck in your head now. Sorry about that. If you have not heard it, consider yourself among the lucky ones. Of course, now you are going to go Google it, aren’t you? Well, don’t say we didn’t warn you.
Marketing drug awareness to children is not a bad thing, but the campaigns tend to be so over-simplified or one-sided that the message that comes across is that drugs are bad and should not be used. Period. Yet, we as a society use drugs and mind-altering substances all the time. Raise your hand if you poured yourself a coffee or tea before sitting down to read this, if you plan to take a cigarette break at the end of the section, or you had a beer or glass of wine yesterday evening as a way to unwind. Substance use, whether drugs or alcohol, is commonplace in Canada, as in many other countries. Rather than saying drugs are bad, we need to take a more balanced approach. This way we can better understand when substance use becomes problematic such as through addiction, what impacts problematic use has on people within society, and how our government’s approach impacts the programmatic responses we are able to provide.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=707#h5p-47
Before moving into our discussion of drug use as a public health issue, it is beneficial to start here with some information on addiction. The Centre for Addiction and Mental Health (CAMH, 2021) defines addiction as, “the problematic use of a substance” with harms ranging from mild (e.g., feeling hungover, being late for work) to severe (e.g., homelessness, disease). They note that people become addicted due to a combination of factors that include genetic predisposition, brain chemistry, socialization and influences within the home and community, mental health issues, and coping with trauma or difficult life circumstances (CAMH, 2021). We can see from this, that addiction is not a matter of personal choice but rather the result of many complex and intersecting factors. We have to look beyond the personal trouble to see the public issue. We do this in Canada through policy and legislation.
As a country, Canada has wavered in its approach to managing drugs. In 2003 reducing alcohol and drug-related harms was a national priority under Canada’s Drug Strategy, and a range of harm reduction approaches and therapeutic interventions were identified. In 2007 new Federal policy was released to replace Canada’s Drug Strategy. The new one was called the National Anti-Drug Strategy, and it consisted of a three-part action plan focused on prevention, treatment, and enforcement. Noticeably absent from this lineup was the “fourth pillar” of harm reduction (Buccieri, 2013). Fast forward to December 2016 when the Minister of Health announced the Canadian Drugs and Substances Strategy, which brought harm reduction back into the 4-pillars of prevention, treatment, harm reduction, and enforcement (Government of Canada, 2016).
The importance of harm reduction as a priority approach is discussed further in the section that follows. It is exactly as the name suggests – taking measures to reduce the harm associated with substance use. We introduce it briefly here to demonstrate that the landscape of drug policy, that is how we have responded to drug use as a country, has shifted back and forth over the years hinging on the issue of harm reduction in contrast to more punitive measures. In the video that follows Dr. Bernie Pauly, a leading harm reduction researcher in Victoria, discusses Canadian drug policy.
In this video Dr. Bernadette [Bernie] Pauly argues that drug use is a public health issue because a lot of the harms of drug use are driven by drug policy. Some drugs, such as heroin, cocaine, and crystal meth, are made illegal resulting in a lack of regulation around them. When a person uses these drugs, they are accessing an unregulated and potentially unsafe supply. Dr. Pauly notes that during the COVID-19 pandemic the unregulated supply of drugs became more toxic, resulting in increased rates of harm and high rates of overdose deaths. She concludes that the lack of regulation around certain drugs, and resulting harms, is a public health issue because it impacts a whole population of people, who have varying degrees of vulnerability. This video is 1:45 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: How is drug use a public health issue?
Much like Canadian drug policy, the laws around drug use in Canada have changed over time as well. The current legislation, passed in 1996, is the Controlled Drugs and Substances Act, which outlines legal aspects such as offences, punishment, enforcement, and disposition (Government of Canada, 2021b). There are a number of regulations made under this Act, such as ‘Safe Food for Canadians Regulations,’ ‘Narcotic Control Regulations,’ and ‘Benzodiazepines and Other Targeted Substances Regulations’ (Government of Canada, 2021b). However, you might be most familiar with the legalization and regulation of the Cannabis Act passed in October 2018 with the three stated goals of (1) keeping cannabis out of the hands of youth, (2) keeping profits out of the pockets of criminals, and (3) protecting public health and safety by allowing adults access to legal cannabis (Government of Canada, 2021a).
The decision to legalize and regulate cannabis was not made lightly. Indeed, you may recall it was a hotly debated topic across the country. However, while not everyone agreed with the new legislation, it was supported by research evidence and public health guidance. Passing this law signaled a commitment from the Federal government that harm reduction was an important part of the national Canadian Drugs and Substances Strategy. These policies and legislation are a step forward, but there are calls to do more. Particularly during the COVID-19 pandemic, deaths from opioid poisonings and overdoses rose, in large part because of an unregulated drug supply. We invite you here to consider this 8-minute segment from CBS News: The National that examines the calls to decriminalize drugs. We encourage viewer discretion, should drug paraphernalia be a personal trigger.
Decriminalization means that people would not face criminal charges associated with drug use. This is sometimes confused with legalization, which involves governmental regulation of production and access. After watching the video segment and hearing from Dr. Pauly, how do you think Canada should approach drug policy and law? Should we decriminalize and/or legalize other drugs, following the Cannabis Act?
Decriminalization would represent a major shift in our approach to drug policy in Canada. Although we have made some steps in that direction, with Federal policy and legislation embracing harm reduction, there is still much debate. Consider where you stand on this issue as you read this policy brief published in the Canadian Journal of Addiction that argues in support of the decriminalization of drug use and possession for personal use.
Leger, P., Hamilton, A., Bahji, A., & Martell, D. on behalf of the CSAM Policy Committee. (2021). Policy brief: CSAM in support of the decriminalization of drug use and possession for personal use. The Canadian Journal of Addiction, 12(1), 13-15
Criminalizing drug use has a disproportionate impact on different people in society. Not everyone faces the same levels of surveillance and policing as others, which is a topic we will explore further in the chapter on Sociology & Crimino-Legal Studies. It is important to note that not every person who experiences homelessness uses drugs, but the risk of homelessness is considerably higher for people who do. Research has shown that for people experiencing homelessness or housing instability, the use of drugs at clinically significant rates decreases the chances of achieving residential stability over time (Nasmith et al., 2020).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=707#h5p-48
Research from Vancouver’s Downtown Eastside, a low-income inner-city neighbourhood, demonstrates the housing precarity of people who use drugs. Using qualitative baseline and follow-up interviews with people who use drugs and were recently evicted, Fleming et al., (2019) found that most participants had been evicted unlawfully into homelessness. This study shows that existing housing policies and tenancy supports are generally not designed to support people who use drugs, who face related social and economic challenges, and who may not be able to advocate for their rights.
The overdose crisis requires novel and targeted public health interventions (Bardwell, Boyd, Kerr, & McNeil, 2018). A qualitative study of the overlapping housing and overdose crises in Vancouver shows that being evicted has serious implications for people who use drugs, including challenges navigating drug supply changes, decreased access to trusted dealers, an increase in public drug use, and a change in drug use patterns (McNeil et al., 2021). The risks of losing one’s housing, and experiencing homelessness, as a result of drug use are real and growing concerns, as housing prices rise and the market becomes more competitive in cities across the country.
The connection between addiction and housing precarity is the topic of Episode 6 in the podcast “Crackdown,” which looks at the war on drugs from the inside perspective of drug users as war correspondents. We encourage you here to sit back and listen to “Room 821” about tenants of the rundown Balmoral Hotel standing up for their rights amidst a growing overdose crisis. You will also find many more episodes to explore on a range of public health and substance use topics. Have a listen below and remember to consider how these personal troubles are actually larger public issues that impact society as a whole.
Click the image below to open a new window and listen to the podcast “Episode 6: Room 821” of Crackdown.
While this podcast and much of the research comes out of Vancouver, the opioid crisis is occurring all across the country. People are dying from unregulated drug supplies, often alone or in the presence of others who are unable to help them. Dr. Naomi Nichols discusses this in the next video as it relates to young people and their families.
In this video, Dr. Naomi Nichols argues that there is currently insufficient capacity to address opioid poisonings in most community health systems, and that the opioid crisis is affecting families. She notes that homelessness is an intersecting risk factor, as people who use drugs alone or with others who are nervous to administer Naloxone or call emergency services are at an increased risk in the event of a drug overdose. This video is 1:01 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Youth and the risk of overdose
As Dr. Nichols mentions, youth who use drugs are vulnerable to experiencing or being with someone who experiences a drug overdose and may be fearful of calling 9-1-1 for help (Selfridge, Greer, Card, Macdonald, & Pauly, 2020). Put yourself in their shoes for a minute and imagine how it would feel to be with a friend who was experiencing a drug overdose while potentially carrying or using drugs yourself. You might worry that if you called 9-1-1 police would show up and arrest you for having drugs in your possession. In fact, this was what used to happen prior to the passing of the “Good Samaritan Drug Overdose Act” in 2017, which offers exemption from charges for people who seek emergency medical or law enforcement assistance for themselves or another person following overdosing on a controlled substance (Government of Canada, 2021c).
This Federal law means that a person can call for help and not be charged, but it is only effective if people know about it. In British Columbia researchers interviewed 38 youth, aged 16-30 who used drugs at least weekly and had encountered police in the past year, to learn about their understanding of the Good Samaritan Drug Overdose Act (Selfridge et al., 2020). Their results showed participants had some knowledge of the Act but were still hesitant about calling for help due to concerns over criminalization (Selfridge et al., 2020).
People who experience homelessness and use substances in problematic ways may have low rates of physical and psychological integration in society (Cherner, Aubry, & Ecker, 2017). This social exclusion may increase the risk of using substances alone, further increasing the danger of overdose. Peer-based supervised injection interventions have been implemented in some shelters and community agencies as a way to normalize drug use and reduce stigma and shame, but research has shown that social norms and material constraints still lead some people to inject alone and/or in unsafe spaces (Bardwell, Boyd, Kerr, & McNeil, 2018). In the next video, Dr. Rebecca Schiff reflects on the broader implications of how people who use drugs are treated in society and its impact on their health and safety.
In this video, Dr. Rebecca Schiff makes a distinction between drug use as a public health issue related to harm reduction programs, and the broader implications of how people who use drugs are treated by society. She argues that the public health issue is not drug use itself, but rather how people who use drugs are forced to do so in unsafe ways. Dr. Schiff argues that when drugs are criminalized, people who lack safe and private spaces may be forced to use them in hidden and dangerous public spaces. She concludes that there are also broader considerations for demands on the health care system, such as when a person who has an alcohol use disorder consumes types or volumes of alcohol that are unsafe. This video is 5:40 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: How is drug use a public health issue?
In this section, we asked you to adopt a wide lens and think about how drug use is not only a personal trouble that impacts individuals, but also a public issue that requires thoughtful policies and legislation. We began by discussing the limitations of many public awareness campaigns aimed at children and arguing that we need a more balanced message about drug use in our society. By reviewing the national policies and legislation, we saw how Canada has gone back and forth on harm reduction as one of its key pillars over the past few decades. At the time of writing, in late 2021, harm reduction is currently part of our nation’s strategic approach.
At the same time, our review of the current research showed that people who use drugs in our society are highly marginalized, particularly in relation to housing. We asked you to listen to an episode of the podcast “Crackdown” that explored this issue, and to consider calls from leading researchers and advocates to decriminalize drugs. Individuals who use drugs and experience homelessness are often isolated and risk overdosing alone or with others who are also using drugs at the time. National legislation has been passed in Canada to allow people to call for emergency medical or police help without fear of arrest, but many are still rightfully worried about calling for help in a society that discriminates against people who use drugs. In the next section, we take a closer look at harm reduction, as a strategy that uses a rights-based approach to offer non-discriminatory person-centered care to people who use drugs.
Click the link below to listen to all of the researchers answer the question “How is drug use a public health issue?” in audio format on our podcast!
Listen to “How is drug use a public health issue?” on Spreaker
51
In the previous section, we discussed Canada’s changing love-hate relationship with harm reduction as part of our shifting national drug policy landscape. We, as authors of this book, are not conflicted. Harm reduction is a critically important public health response for people who use substances problematically. You will notice we have given away our position right in the question, by not asking if a harm reduction approach is necessary, but rather why it is necessary. Following from the section on drug use as a public health issue, you likely have a pretty keen sense of why we think it is important, but we would like you to begin this chapter by outlining the thoughts you have at this time.
Perhaps you feel that you know why harm reduction is necessary. If so, we encourage you to use the space below to write down your ideas. It is also possible that after reading the previous section you still have doubts about Canada’s move towards implementing harm reduction strategies and legislation. That is okay too. If you are unsure, we invite you to write down any questions or arguments you might have against harm reduction in the space below. Be sure to return to them after reading the section, to see whether any of your views have changed.
Please also remember that this writing is for you to take stock of your knowledge and standpoint at the start of the section and you may write as much or as little as you would like.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=709#h5p-49
The answer to why harm reduction is a necessary approach rests with the explanation of what harm reduction is. We begin our discussion here with a brief animated video from the Harm Reduction Action Centre entitled, “Harm Reduction 101.”
Harm reduction is both a philosophical orientation and set of practices that aim to reduce the harm people experience associated with risky behaviours. This harm may be to themselves, to their family, friends, or society as a whole. As shown in the video, we use harm reduction in many areas of our lives, including the use of seatbelts to reduce harms associated with driving and applying sunscreen to prevent risks from sun exposure. The idea of harm reduction makes practical sense, yet as Dr. Bernie Pauly explains in the next video, it is not always embraced in the context of drug use because of long-standing biases and misconceptions rooted in prohibition.
In this video Dr. Bernadette [Bernie] Pauly discusses the broad scope of harm reduction interventions that have existed throughout history. She traces the early roots to the 1950s when physicians in the United Kingdom began prescribing their patients alternatives to the illicit drug market. In the 1980s harm reduction become more popular as a means of preventing HIV transmission, through the introduction of clean supplies, needle exchange, and supervised injection services. Currently, harm reduction efforts have been expanding through the distribution of Naloxone and calls for safer supply measures like decriminalization and regulation of the toxic drug supply. Dr. Pauly is clear to note that beyond the scope of interventions, it is important for people to understand harm reduction within the context of very criminalized use. This is because harm reduction provides a way of taking a non-judgmental, non-stigmatizing approach that acknowledges and accepts people where they are at. Through harm reduction, trusting relationships are formed that allow people to access services and get help without being judged for their substance use. Dr. Pauly cautions people who work in health care and/or harm reduction that there is a long-standing legacy of criminalization tied to prohibition that will have influenced them long before they entered the field. She calls for the decriminalization of drugs to help destigmatize drug use and enhance the potential for greater access to services. This video is 4:47 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: Why is a harm reduction approach necessary?
Harm reduction is necessary because it provides an empathetic person-centered approach that is lacking in alternative approaches like criminal enforcement and asking people to “just say no.” Professor Stephen Gaetz has written, “While not all people who experience homelessness have substance use disorders, many respond to experiences of trauma and exclusion through the use of substances, and in many cases this leads to problematic use. In a context where people who are homeless regularly experience the control and regulation of their lives through emergency services, harm reduction approaches provide a welcomed alternative through humane, respectful, effective and client centred approaches to addressing substance use disorders” (Gaetz, 2018, pg. S195).
We saw previously that addiction occurs for many complex and inter-related reasons like genetics, brain chemistry, social environment, mental health, and as a means of coping with stressors and trauma (CAMH, 2021). It is therefore unreasonable to expect that something that complicated could be resolved by telling people to stop using drugs or being addicted. That approach has been tried and has led to our current drug crisis situation. Rather than telling people to stop and then punishing them if they are unable to comply with an unreasonable demand, harm reduction approaches accept that substance use will occur and try to find ways to improve people’s quality of life without blame or judgement. Dr. Rebecca Schiff discusses these ideas further in the video that follows.
In this video, Dr. Rebecca Schiff explains that harm reduction is about human rights because housing is a human right and people should not be denied housing on the basis of using substances. She notes that harm reduction is necessary because the more traditional model of abstinence does not work for everyone. Dr. Schiff concludes that if we want to solve homelessness, we need to think in complex ways and address a range of interconnected challenges using different approaches for different people. This video is 2:37 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: Why is a harm reduction approach necessary?
Dr. Schiff reminds us that we have to think in very complex ways about how we implement harm reduction for different individuals. What works for one person might not work for another. For instance, researchers are actively investigating ways to adapt harm reduction to the needs of diverse populations, such as within Indigenous communities (Firestone et al., 2019; Victor et al., 2019; Young & Manion, 2017). Researchers have also considered the impact of harm reduction within the context of mental illness and/or Housing First programs (Maremmani et al., 2017; Urbanoski et al., 2018), and onthe experiences of women and gender-diverse individuals who use substances (Kitson & O’Byrne, 2020; Meyer et al., 2019; Scheim, Bauer, & Shokoohi, 2017). As we continue to look at why harm reduction is necessary, it is important to keep in mind that harm reduction is not one single or unitary approach, but that different people will benefit from different measures, based on their own unique set of needs.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=709#h5p-50
The application of harm reduction, as a practice, takes many different forms. Among the most common and effective approaches is substituting one substance for another, whether at the same frequency or varied. For instance, a person might be encouraged to reduce their use of injection drugs, even if it means they increase their use of non-injection drugs because it reduces risks such as infection. There is evidence that supports the substitution approach as an effective harm reduction approach. Youth, in particular, might choose to continue one type of drug while discontinuing another (Lake et al., 2018). For instance, in a study of 481 street involved youth in Vancouver, researchers found that those who reported daily cannabis use had lower rates of stimulant injection initiation, which challenges the notion of cannabis use as a gateway to harder and more addictive substances (Reddon et al., 2018). Likewise, use of the illicit drug MDMA (commonly referred to as ecstasy, E, or molly) has been linked to reductions in injection drug use amongst youth (Gaddis et al., 2018).
The substitution method encourages people to use less harmful substances, even if they use them at the same or higher rates. Does this logic make sense to you as a harm reduction strategy? Can you see the parallel if we suggested that a person with diabetes should eat two sugar-free chocolate bars rather than one regular bar, even if it means they consume more chocolate?
Substitution is one method of reducing the harms associated with problematic substance use. Another related approach involves replacing one substance with a medication that has similar pharmacological effects but without the same harms to the body. We see this approach taken with many different substances. Although we may not commonly think of tobacco as being amongst the most problematic drugs, it is frequently used and has harmful effects over time. In a study of 639 individuals who had a severe mental illness and were experiencing homelessness or housing instability, tobacco use was high among nearly three-quarters of respondents, including nearly half who smoked contraband cigarettes and a quarter who remade cigarettes from discarded butts (Pettey & Aubry, 2018). The same study found that smokers were more than 9 times more likely to have a co-occurring substance use disorder (Pettey & Aubry, 2018).
The PROMPT study (point-of-care for tobacco dependence) in Ottawa used community-based participatory action research to evaluate the effectiveness of recruiting 80 people who use drugs, providing them access to counselling, nicotine replacement therapy, and peer-support in a community setting (Pakhale et al., 2018). Results of this study indicated that over 6 months there were reported reductions in the use of cigarettes and illicit opioids such as heroin, fentanyl, and Oxycontin, as well as benefits like improved health, return to work, and greater community engagement (Pakhale et al., 2018). The success of this project demonstrates how replacing a substance with a medically supervised alternative can result in positive outcomes, particularly when combined with community supports.
Another pharmaceutical replacement method involves using synthetic opioid agonists, like methadone or suboxone, to replace heroin or painkiller use. These pharmaceuticals work to prevent the physical symptoms of heroin and other opiate withdrawal without producing the same mind-altering effects or mental high. Methadone maintenance treatment has had widespread uptake in many communities across Canada, being provided in clinics or pharmacies, as a way to reduce the harms associated with opioid addiction. Researchers examined the sociodemographic profiles of clients receiving methadone maintenance treatment in a clinic in western Canada and found that clients were 36 years old on average, had early exposure to drugs and alcohol, presented with complex health care needs, and had experiences of trauma that included poverty and homelessness (Maina, Crizzle, Maposa, & Fournier, 2019).
At this point, you might be thinking to yourself, “If methadone replaces opioids, why don’t we just give it everyone with an opioid addiction and solve the overdose crisis?” If this is indeed what you are thinking, you are on the right path to having a harm reduction mindset. At the same time, we come to the familiar book refrain that these seemingly simple kinds of questions often have rather complex answers. In short, methadone maintenance treatment is not a quick fix for the opioid crisis because not everyone wants to take it, and choice is a fundamental human right that is recognized as a core harm reduction principle.
There are many reasons people do not want to take methadone or that they discontinue its use after a period of time. In a Vancouver-based study researchers sought to identify factors associated with discontinuing methadone and found that discontinuation was more common among people who used heroin daily and those who were experiencing homelessness (Klimas et al., 2018). A study with a cohort of people who use drugs in Vancouver identified homelessness, daily heroin injection, daily prescription opioid use, recent incarceration, and not being on any form of income assistance as factors that were statistically linked to discontinuing methadone maintenance treatment (Lo et al., 2018). The authors of the study argue this demonstrates the need to reduce potential barriers by providing access to stable housing and preventing treatment interruptions during discharge from incarceration (Lo et al., 2018).
Research with participants from the Vancouver At Home / Chez Soi site investigated the effect of Housing First compared to Treatment as Usual, on methadone maintenance adherence but found no significant differences (Parpouchi et al., 2018), indicating that while housing is critical, it is not a direct pathway to methadone. It is promising to note that receiving other concurrent addiction treatment in addition to methadone maintenance has been found to help prevent discontinuation and promote adherence to the treatment (Klimas et al., 2018). Methadone is one harm reduction strategy that has gained a foothold within many communities, but it requires regular visits to get the medication and produces horrible withdrawal symptoms if not taken according to the schedule.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=709#h5p-51
Harm reduction strategies apply to a range of substances. Some people who experience homelessness have severe alcohol dependence, including the consumption of non-beverage alcohol like mouthwash and hand sanitizer (Crabtree et al., 2018). In a commentary published in the International Journal of Drug Policy, Ivsins et al., (2019) argue that there is a gap in harm reduction for individuals experiencing structural vulnerabilities like poverty and homelessness and have severe alcohol use disorder. They explain that because these individuals are doubly impacted by structural oppression and severe alcohol use disorder, conventional abstinence-based programs are largely ineffective. Rather, they point to Managed Alcohol Programs (MAPs) as a way to address these intersecting harms that has great potential but is not receiving enough attention within the broader harm reduction landscape (Ivsins et al., 2019).
Managed Alcohol Programs are a harm reduction approach that have been shown to be effective with this population. Using case study analysis from five Canadian cities, Dr. Bernie Pauly and her team (2019) found that prior to entering a MAP, participants in the study were often stuck in a revolving institutional cycle between health, justice, housing, and shelter use where abstinence is often required to qualify for services. The MAPs case study found that prior to entering the programs, most people were using alcohol while engaged in risky street-based environments characterized by criminalization, unmet health needs, stigma, a lack of safety, and disconnection from family and social supports (Pauly et al., 2019).
In contrast, MAPs reduce harms by providing people with access to safe spaces and a managed supply of alcohol (Pauly et al., 2019). They are a better harm reduction alternative because people may still use alcohol at high rates, but their safety, health, and social connections are likely to improve. MAPs can be offered in different ways, such as through residential live-in programs or as drop-in day programs. In Pauly et al.’s (2018) study there were six key dimensions that researchers found differentiated these programs from one another, including program goals and eligibility, food and accommodation, alcohol dispensing and administration, funding and money management, primary care services and clinical monitoring, and social and cultural connections.
We encourage you to read some of the most recent work that combines research into cannabis substitution and managed alcohol programs, both harm reduction approaches we have discussed above. In this section’s featured reading Professor Bernie Pauly and her team examine these inter-related strategies.
Pauly, B., Brown, M., Chow, C., Wettlaufer, A., East Side Illicit Drinkers Group for Education, … & Sutherland, C. (2021). “If I knew I could get that every hour instead of alcohol, I would take the cannabis”: Need and feasibility of cannabis substitution implementation in Canadian managed alcohol programs. Harm Reduction Journal, 18, 65.
Many of the harm reduction approaches we have considered, such as pharmaceutical replacements (like methadone) and supervised distributions (like managed alcohol programs) fall under the broader umbrella of “safe supply.” Particularly as drug poisonings and overdose deaths have risen during the COVID-19 pandemic, there have been calls to expand these efforts to provide safe supplies as an alternative. For instance, Fleming et al., (2020) have written a commentary piece arguing that much like methadone replaces street opioids, there are pharmaceuticals that could be used as substitutes for stimulants, such as cocaine and methamphetamine, that could be regulated to reduce the number of stimulant-related deaths.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=709#h5p-52
Safe supply is one harm reduction measure we can take to help reduce the number of drug overdoses that are occurring across our country. In this next video, Dr. Abe Oudshoorn explains this idea further.
In July 2021, British Columbia became the first Canadian province to introduce a safe supply alternative to a range of street drugs, including opioids and stimulants, as Fleming et al., (2020) advocated for. This approach, of providing a safe supply, is a public health measure that has the potential to reduce harm and save many lives. Consider this brief news clip from CBC Vancouver, in which advocates call for the safe supply strategy to go even further. We would like to caution you that this video shows images of injection drugs being prepared for use, and viewer discretion is advised.
At the Provincial level, British Columbia has implemented many progressive harm reduction approaches. Most notably Canada’s first sanctioned supervised injection facility, InSite, opened in Vancouver in 2003 as a place where people can go to use drugs under the supervision of medical, nursing, and social work professionals, reducing the risk of overdose and improving access to non-judgmental support services. Research from Vancouver has shown that people most likely to use supervised injection facilities over time include those who experience homelessness, inject heroin daily, engage in binge injection and/or injection in public, have experienced a nonfatal overdose, have had difficulty accessing addiction treatment, and have a history of incarceration (Kennedy et al., 2019). This research suggests that supervised injection facilities have success in retaining clients who are among the most at risk of negative, and potentially fatal, outcomes from injection drug use.
At this point in the chapter, we would like to invite you to step inside InSite and take a virtual tour as an interactive experience. You can use the controls on the top left side to change the camera angle and experience the organization through a 365-degree viewpoint. Again, we would like to caution you that there is a description of drug injection in this video and that you should use your discretion in choosing whether to view this media.
InSite opened after much advocacy and, although there is a large body of evidence highlighting its effectiveness in reducing social and physical harms associated with injection drug use, calls to expand these types of services nationwide require support at the Federal legislation level (Kerr, Mitra, Kennedy, & McNeil, 2017). In a commentary piece, published in 2018, Young and Fairbairn agreed that while InSite is supported by evidence that shows reductions in overdose mortality, infectious-related complications, and public disorder, expansion of these types of services across the country is at risk because Canada’s socio-demographic and political landscapes leave the application of supervised injection facilities a major uncertainty.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=709#h5p-53
In the years since these pieces were written, and within the context of rising overdose deaths during the COVID-19 pandemic, Canada has made national strides towards expanding access to these types of services across the country. We now call these “Supervised Consumptions Sites and Services,” which are offered in communities alongside other types of programs to support people who use drugs.
As we have seen, Canada’s national drug policies and strategies are re-integrating harm reduction as one of the central pillars. One practical application of this approach has been the development of Supervised Consumption Sites and Services in communities across the country. Have you noticed harm reduction services available where you live and, if so, are they effective? What other services do you think could be added to make your community safer for people who use drugs? To learn more, check out this Interactive map: Canada‘’s response to the opioid crisis
In response to the escalating drug poisonings, some supervised injection facilities have begun offering drug checking as a service. The brief video below, created by the Drug Policy Alliance, provides an overview of what drug checking is and why it is important.
In a study conducted at InSite from July 2016 to June 2017 only 1% of clients opted to test their urine for the presence of fentanyl, but among those who did 80% came back positive (Karamouzian et al., 2018). This suggests that exposure to fentanyl is considerably higher than people consuming it may even realize. Further results of this study indicated that a positive fentanyl result did not make people intend to dispose of the drug, but it did mean they were likely to reduce the dose they took, which could decrease the chances of overdose (Karamouzian et al., 2018). Kennedy et al., (2018) conducted a study to better understand the willingness of supervised injection facility clients to access these services and found that just under half (43%) would be willing to frequently check their drugs if the service was available and that this willingness was more common among those who were female-identified, experiencing homelessness, and/or dealing drugs (Kennedy et al., 2018).
These studies suggest that while drug checking may not be accessed by all individuals who use drugs, this is a valuable harm reduction service that has the potential to save lives for those who do. In the video that follows Dr. Nick Kerman explains the importance of expanding harm reduction capacity at the community level, through partnership building and collaboration.
In this video, Dr. Nick Kerman discusses the impact that the ongoing and worsening drug overdose and poisoning crisis in Canada is having on community programs, that often are the ones to intervene. Dr. Kerman argues we need to enhance capacity within the social service sector to address this issue, by strengthening relationships, partnerships, and collaboration between social service agencies that provide supports to people experiencing homelessness and harm reduction services, including those within the health care system. He concludes that with collaboration and integration we can position services to respond to overdoses more effectively and provide people with a safe place to use substances without feeling like they have to hide or do so in an unsafe way. This video is 1:30 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: Supporting harm reduction in communities
At the start of the section, we asked you to consider why harm reduction is a necessary approach for people who use drugs problematically. We encouraged you to take stock of your own position and see whether you agreed that it is important, had questions, or had arguments against. If you wrote down a response, please return to it now and see whether any of your ideas have changed throughout this section.
We have argued unequivocally that harm reduction is an important and necessary approach in Canada. We began by learning about the early roots of harm reduction and considering the importance of individual choice about which services and supports are needed. There are many different types of responses that fall under the harm reduction umbrella, and which one is the “right” one will vary for each individual. For instance, a person may choose to substitute substances for less harmful ones or seek pharmaceutical replacements like methadone maintenance treatment. As an extension, we discussed managed alcohol programs and invited you to read contemporary research on the impact these programs can have for people with severe alcohol dependence, including the consumption of non-beverage alcohol.
Calls for safe supply have been made across the country and during the COVID-19 pandemic British Columbia became the first province to implement a generalized safe supply initiative. It was in 2003 that British Columbia also opened Canada’s first supervised injection facility known as InSite. We invited you to take a virtual tour and to check out a map of how Canada has expanded Supervised Consumption Sites and Services across the country today. Finally, we discussed drug checking as an important, yet underutilized, service that is available in many of these locations. We ended with a consideration of how communities can, through collaboration and integration, support people who use drugs in safer and healthier ways.
Click the link below to listen to all of the researchers answer the question “Why is a harm reduction approach necessary?” in audio format on our podcast!
Listen to “Why is a harm reduction approach necessary?” on Spreaker
52
Stephan and Zane
So let us return to Stephan and Zane. Without an understanding of the systematic issues in our society, we might consider that shelters must be a safe place to “house” individuals, however, it is evident that this couple is facing a number of safety risks. As we learned from Dr. Hwang folks living in shelters have a higher risk of contracting COVID-19. Stephan and Zane have been exposed and now must “shelter at home” in a congregate setting where space is limited, residents are transient, and supplies and resources to prevent transmission are inadequate. In addition, both Stephan and Zane have substance use challenges. They are currently living in a shelter that has a “no tolerance” policy for drug use which increases their risk of seeking substances from a significantly questionable and unsafe supply of both equipment and drugs. This increases the risk of an overdose or poisoning by tainted supply – increasing the risk of harm to both. They are living with daily fear, frustration, guilt, and feelings of hopelessness.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1047#h5p-87
53
Public health related issues dominate the news cycle today, as evidenced by the volume of stories about the COVID-19 pandemic and rise in overdose deaths. We have argued that both of these public health issues are intricately related to a lack of affordable housing in Canada and the subsequent management of homelessness through emergency services like shelters.
At the start of the chapter, we introduced you to the composite characters Stephan and Zane, who were living in a shelter during the COVID-19 outbreak because they were having difficult obtaining employment and housing. The scenario was presented as an entry point into thinking about the complexity of homelessness and public health. We returned to these individual’s story again at the end to demonstrate how it can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada.
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “Why are people who experience homelessness at higher risk during a pandemic?” Here we considered the incongruity between public health messages, like asking people to stay at home, and the lived reality of homelessness. We considered research conducted during the H1N1 outbreak and saw that even with this knowledge many homelessness sectors were not able to adequately prepare because they were already dealing with the crisis of homelessness. The design of service agencies, like shelters, serves to increase the spread of disease and we saw this in the high rates of COVID-19 infection, hospitalizations, ICU admissions, and deaths among people experiencing homelessness. Many service providers continued to work through the pandemic, despite their own decreasing mental wellness, because clients needed their support, particularly in rural areas and in relation to domestic violence.
Next we asked, “How is drug use a public health issue?” As a nation Canada has undergone many shifts in drug policy and legislation, but currently harm reduction is a recognized pillar in our strategic approach. In this section we considered the relationship between drug policy and housing precarity, such as the unlawful evictions of people who use drugs because of discriminatory practices. People who use drugs are often isolated and may risk overdosing while alone or with others who are also using drugs at the time. In response, Canada has passed legislation that allows for people to call 9-1-1 and not be charged with being under the influence or having drugs in their possession. There have been calls to decriminalize drugs as a means of further protecting people from the harms they can pose, both medically and socially.
Finally we asked, “Why is harm reduction a necessary approach?” In this final section we made the argument that harm reduction is critical because it is an approach that treats people with compassion while also saving lives. There are many different harm reduction strategies that vary according to individual choice and need. People may substitute one substance for another, use pharmacological treatments like methadone, or engage with managed alcohol programs. These strategies are part of a larger call for safe supply, which was announced in British Columbia amidst critiques that it does not go far enough. In 2003 InSite, the first supervised injection facility, opened in Vancouver and in the time since we have seen the federal roll out of Supervised Consumption Sites and Services that include measures like drug checking. While these are positive steps towards normalizing harm reduction, there is still much work to do in communities across Canada.
54
Here are some additional resources you may want to check out!
55
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
56
Bardwell, G., Boyd, J., Kerr, T., & McNeil, R. (2018). Negotiating space & drug use in emergency shelters with peer witness injection programs within the context of an overdose crisis: A qualitative study. Health & Place, 53, 86–93. https://doi.org/10.1016/j.healthplace.2018.07.011
Bodkin, C., Mokashi, V., Beal, K., Wiwcharuk, J., Lennox, R., Guenter, D., … O’Shea, T. (2020). Pandemic planning in homeless shelters: A pilot study of a COVID-19 testing and support program to mitigate the risk of COVID-19 outbreaks in congregate settings. Clinical Infectious Diseases, 72(9), 1639-1641. https://doi.org/10.1093/cid/ciaa743
Buccieri, K. (2013). Back to the future for Canada’s national anti-drug strategy: Homeless youth and the need for harm reduction. In S. Gaetz, B. O’Grady, K. Buccieri, J. Karabanow, & A. Marsolais (Eds.), Youth homelessness in Canada: Implications for policy and practice (199-215). Toronto, ON: The Canadian Homelessness Research Network. Youth Homelessness in Canada (homelesshub.ca)
Buccieri, K. (2016). H1N1 and homelessness in Toronto: Identifying structural issues in the homelessness sector. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Buccieri, K. & Schiff, R. (Eds.). (2016). Pandemic preparedness and homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Buccieri, K. (2020). Pandemic planning: How can my agency prepare for the potential spread of Coronavirus? Toronto, ON: The Homeless Hub.
CAMH. (2021). Addiction. Centre for Addiction and Mental Health, Toronto. Addiction | CAMH
Cherner, R. A., Aubry, T., & Ecker, J. (2017). Predictors of the physical and psychological integration of homeless adults with problematic substance use. Journal of Community Psychology, 45(1), 65–80. https://doi.org/10.1002/jcop.21834
Crabtree, A., Latham, N., Morgan, R., Pauly, B., Bungay, V., & Buxton, J. A. (2018). Perceived harms and harm reduction strategies among people who drink non-beverage alcohol: Community-based qualitative research in Vancouver, Canada. The International Journal of Drug Policy, 59, 85–93. https://doi.org/10.1016/j.drugpo.2018.06.020
Dohoo, C., Stuart, R., Finkelstein, M., Bradley, K., & Gournis, E. (2020). Risk factors associated with group A Streptococcus acquisition in a large, urban homeless shelter outbreak. Canadian Journal of Public Health, 111(1), 117–124. https://doi.org/10.17269/s41997-019-00258-5
Firestone, M., Syrette, J., Jourdain, T., Recollet, V., & Smylie, J. (2019). “I feel safe just coming here because there are other Native brothers and sisters”: Findings from a community-based evaluation of the Niiwin Wendaanimak Four Winds Wellness Program. Canadian Journal of Public Health, 110(4), 404–413. https://doi.org/10.17269/s41997-019-00192-6
Fleming, T., Barker, A., Ivsins, A., Vakharia, S., & McNeil, R. (2020). Stimulant safe supply: a potential opportunity to respond to the overdose epidemic. Harm Reduction Journal, 17(1), 6–6. https://doi.org/10.1186/s12954-019-0351-1
Fleming, T., Damon, W., Collins, A. B., Czechaczek, S., Boyd, J., & McNeil, R. (2019). Housing in crisis: A qualitative study of the socio-legal contexts of residential evictions in Vancouver’s Downtown Eastside. The International Journal of Drug Policy, 71, 169–177. https://doi.org/10.1016/j.drugpo.2018.12.012
Gaddis, A., Lake, S., Tupper, K., Nosova, E., Blommaert, K., Wood, E., & DeBeck, K. (2018). Regular MDMA use is associated with decreased risk of drug injection among street-involved youth who use illicit drugs. Drug and Alcohol Dependence, 192, 112–117. https://doi.org/10.1016/j.drugalcdep.2018.07.035
Gaetz, S. (2018). Commentary: Harm reduction, managed alcohol programs and doing the right thing. Drug and Alcohol Review, 37(S1), S195–S196. https://doi.org/10.1111/dar.12652
Gaetz, S., & Buccieri, K. (2016). The challenges of pandemic planning in the context of homelessness. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Government of Canada. (2016). The new Canadian drugs and substances strategy. Canada. The New Canadian Drugs and Substances Strategy – Canada.ca
Government of Canada. (2021a). Cannabis legalization and regulation. Canada. Cannabis Legalization and Regulation (justice.gc.ca)
Government of Canada. (2021b). Controlled drugs and substances act. Canada. Controlled Drugs and Substances Act (justice.gc.ca)
Government of Canada. (2021c). Good Samaritan drug overdose act. Canada. Good Samaritan Drug Overdose Act (justice.gc.ca)
Ivsins, A., Pauly, B., Brown, M., Evans, J., Gray, E., Schiff, R., … Stockwell, T. (2019). On the outside looking in: Finding a place for managed alcohol programs in the harm reduction movement. The International Journal of Drug Policy, 67, 58–62. https://doi.org/10.1016/j.drugpo.2019.02.004
Karamouzian, M., Dohoo, C., Forsting, S., McNeil, R., Kerr, T., & Lysyshyn, M. (2018). Evaluation of a fentanyl drug checking service for clients of a supervised injection facility, Vancouver, Canada. Harm Reduction Journal, 15(1), 46–46. https://doi.org/10.1186/s12954-018-0252-8
Kennedy, M. C., Klassen, D. C., Dong, H., Milloy, M. J. S., Hayashi, K., & Kerr, T. H. (2019). Supervised injection facility utilization patterns: A prospective cohort study in Vancouver, Canada. American Journal of Preventive Medicine, 57(3), 330–337. https://doi.org/10.1016/j.amepre.2019.04.024
Kennedy, M. C., Scheim, A., Rachlis, B., Mitra, S., Bardwell, G., Rourke, S., & Kerr, T. (2018). Willingness to use drug checking within future supervised injection services among people who inject drugs in a mid-sized Canadian city. Drug and Alcohol Dependence, 185, 248–252. https://doi.org/10.1016/j.drugalcdep.2017.12.026
Kerman, N., Ecker, J., Gaetz, S., Tiderington, E., & Kidd, S. A. (2021). Mental health and wellness of service providers working with people experiencing homelessness in Canada: A national survey from the second wave of the COVID-19 Pandemic. The Canadian Journal of Psychiatry, 1-9. https://doi.org/10.1177/07067437211018782
Kerr, T., Mitra, S., Kennedy, M. C., & McNeil, R. (2017). Supervised injection facilities in Canada: past, present, and future. Harm reduction journal, 14(1), 28. https://doi.org/10.1186/s12954-017-0154-1
Kiran, T., Craig-Neil, A., Das, P., Lockwood, J., Wang, R., Nathanielsz, N., … Hwang, S. W. (2021). Factors associated with SARS-CoV-2 positivity in 20 homeless shelters in Toronto, Canada, from April to July 2020: a repeated cross-sectional study. CMAJ Open, 9(1), E302–E308. https://doi.org/10.9778/cmajo.20200253
Kitson, C., & O’Byrne, P. (2020). The experience of violence against women who use injection drugs: An exploratory qualitative study. Canadian Journal of Nursing Research, 53(4), 340-352. https://doi.org/10.1177/0844562120979577
Klimas, J., Nosova, E., Socías, E., Nolan, S., Brar, R., Hayashi, K., … Wood, E. (2018). Factors associated with discontinuation of methadone maintenance therapy (MMT) among persons who use alcohol in Vancouver, Canada. Drug and Alcohol Dependence, 186, 182–186. https://doi.org/10.1016/j.drugalcdep.2018.01.027
Lake, S., Kerr, T., Nosova, E., Milloy, M. J., Wood, E., & DeBeck, K. (2018). Patterns of non-injection drug use associated with injection cessation among street-involved youth in Vancouver, Canada. Journal of Urban Health, 95(2), 267–277. https://doi.org/10.1007/s11524-017-0225-3
Leger, P., Hamilton, A., Bahji, A., & Martell, D. on behalf of the CSAM Policy Committee. (2021). Policy brief: CSAM in support of the decriminalization of drug use and possession for personal use. The Canadian Journal of Addiction, 12(1), 13-15. Policy Brief: CSAM in Support of the Decriminalization of Dr… : Canadian Journal of Addiction (lww.com)
Lo, A., Kerr, T., Hayashi, K., Milloy, M. J., Nosova, E., Liu, Y., & Fairbairn, N. (2018). Factors associated with methadone maintenance therapy discontinuation among people who inject drugs. Journal of Substance Abuse Treatment, 94, 41–46. https://doi.org/10.1016/j.jsat.2018.08.009
Maina, G., Crizzle, A., Maposa, S., & Fournier, B. (2019). Sociodemographic profiles and clinical outcomes for clients on methadone maintenance treatment in a western Canadian clinic: Implications for practice. Journal of Forensic Nursing, 15(4), 231. 10.1097/JFN.0000000000000246
Maremmani, A. G., Bacciardi, S., Gehring, N. D., Cambioli, L., Schütz, C., Jang, K., & Krausz, M. (2017). Substance use among homeless individuals with schizophrenia and bipolar disorder. The Journal of Nervous and Mental Disease, 205(3), 173–177. https://doi.org/10.1097/NMD.0000000000000462
McNeil, R., Fleming, T., Collins, A. B., Czechaczek, S., Mayer, S., & Boyd, J. (2021). Navigating post-eviction drug use amidst a changing drug supply: A spatially-oriented qualitative study of overlapping housing and overdose crises in Vancouver, Canada. Drug and Alcohol Dependence, 222. https://doi.org/10.1016/j.drugalcdep.2021.108666
Meyer, J. P., Isaacs, K., El-Shahawy, O., Burlew, A. K., & Wechsberg, W. (2019). Research on women with substance use disorders: Reviewing progress and developing a research and implementation roadmap. Drug and Alcohol Dependence, 197, 158–163. https://doi.org/10.1016/j.drugalcdep.2019.01.017
Mills, C. W. (1967). The sociological imagination. London: Oxford University Press.
Nasmith, T. E., Gadermann, A., Jaworsky, D., Norena, M., To, M. J., Hwang, S. W., & Palepu, A. (2020). Clinically significant substance use and residential stability among homeless or vulnerably housed persons in Canada: a longitudinal cohort study. Journal of Public Health, 43(3), 532-540. https://doi.org/10.1093/pubmed/fdaa018
O’Shea, T., Mbuagbaw, L., Mokashi, V., Bulir, D., Gilchrist, J., Smieja, N., … Smieja, M. (2020). Comparison of four COVID-19 screening strategies to facilitate early case identification within the homeless shelter population: A structured summary of a study protocol for a randomised controlled trial. Trials, 21(1), 941–941. https://doi.org/10.1186/s13063-020-04890-2
Pakhale, S., Kaur, T., Charron, C., Florence, K., Rose, T., Jama, S., … Tyndall, M. (2018). Management and point-of-care for tobacco dependence (PROMPT): A feasibility mixed methods community-based participatory action research project in Ottawa, Canada. BMJ Open, 8(1), e018416–e018416. https://doi.org/10.1136/bmjopen-2017-018416
Parpouchi, M., Moniruzzaman, A., Rezansoff, S. N., Russolillo, A., & Somers, J. M. (2018). The effect of housing first on adherence to methadone maintenance treatment. The International Journal of Drug Policy, 56, 73–80. https://doi.org/10.1016/j.drugpo.2018.03.012
Pauly, B., Brown, M., Chow, C., Wettlaufer, A., East Side Illicit Drinkers Group for Education, … & Sutherland, C. (2021). “If I knew I could get that every hour instead of alcohol, I would take the cannabis”: Need and feasibility of cannabis substitution implementation in Canadian managed alcohol programs. Harm Reduction Journal, 18, 65. https://doi.org/10.1186/s12954-021-00512-5
Pauly, B., Brown, M., Evans, J., Gray, E., Schiff, R., Ivsins, A., Krysowaty, B., Vallance, K., & Stockwell, T. (2019). “There is a Place”: Impacts of managed alcohol programs for people experiencing severe alcohol dependence and homelessness. Harm Reduction Journal, 16(1), 70–70. https://doi.org/10.1186/s12954-019-0332-4
Pauly, B., Perkin, K., & Cross, G. (2016). The case of Victoria, BC. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Pauly, B., Vallance, K., Wettlaufer, A., Chow, C., Brown, R., Evans, J., … Stockwell, T. (2018). Community managed alcohol programs in Canada: Overview of key dimensions and implementation. Drug and Alcohol Review, 37(S1), S132–S139. https://doi.org/10.1111/dar.12681
Perri, M., Dosani, N., & Hwang, S. W. (2020). COVID-19 and people experiencing homelessness: challenges and mitigation strategies. Canadian Medical Association Journal (CMAJ), 192(26), E716–E719. https://doi.org/10.1503/cmaj.200834
Pettey, D., & Aubry, T. (2018). Tobacco use and smoking behaviors of individuals with a serious mental illness. Psychiatric Rehabilitation Journal, 41(4), 356–360. https://doi.org/10.1037/prj0000302
Reddon, H., DeBeck, K., Socias, M. E., Dong, H., Wood, E., Montaner, J., … Milloy, M. (2018). Cannabis use is associated with lower rates of initiation of injection drug use among street‐involved youth: A longitudinal analysis. Drug and Alcohol Review, 37(3), 421–428. https://doi.org/10.1111/dar.12667
Richard, L., Booth, R., Rayner, J., Clemens, K. K., Forchuk, C., & Shariff, S. Z. (2021). Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: A retrospective cohort study. CMAJ Open, 9(1), E1–E9. https://doi.org/10.9778/cmajo.20200287
Scheim, A. I., Bauer, G. R., & Shokoohi, M. (2017). Drug use among transgender people in Ontario, Canada: Disparities and associations with social exclusion. Addictive Behaviors, 72, 151–158. https://doi.org/10.1016/j.addbeh.2017.03.022
Schiff, R. (2016a). Conclusion. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Schiff, R. (2016b). Regina, Saskatchewan: The case of small, isolated urban centres. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Schiff, R., Buccieri, K., Waegemakers Schiff, J, Kauppi, C., & Riva, M. (2020). COVID-19 and pandemic planning in the context of rural and remote homelessness. Canadian Journal of Public Health, 111(6), 967–970. https://doi.org/10.17269/s41997-020-00415-1
Schwan, K., Dej, E. & Versteegh, A. (2020). Girls, homelessness, and COVID-19: The urgent need for research and action. Girlhood Studies, 13(3), 151-168. https://doi.org/10.3167/ghs.2020.130311
Selfridge, M., Greer, A., Card, K. G., Macdonald, S., & Pauly, B. (2020). “It’s like super structural” – Overdose experiences of youth who use drugs and police in three non-metropolitan cities across British Columbia. The International Journal of Drug Policy, 76, 102623–102623. https://doi.org/10.1016/j.drugpo.2019.102623
Urbanoski, K., Veldhuizen, S., Krausz, M., Schutz, C., Somers, J. M., Kirst, M., … Goering, P. (2018). Effects of comorbid substance use disorders on outcomes in a Housing First intervention for homeless people with mental illness. Addiction, 113(1), 137–145. https://doi.org/10.1111/add.13928
Victor, J., Shouting, M., DeGroot, C., Vonkeman, L., Brave Rock, M., & Hunt, R. (2019). I’taamohkanoohsin (everyone comes together): (Re)connecting Indigenous people experiencing homelessness and substance misuse to Blackfoot ways of knowing. International Journal of Indigenous Health, 14(1), 42–59. https://doi.org/10.32799/ijih.v14i1.31939
Waegemakers Schiff, J., & Lane, A. (2016). The Calgary response. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Waegemakers Schiff, J., Pauly, B., & Schiff, R. (2016). Health needs and analysis of pandemic planning in four Canadian cities. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Wu, H., & Karabanow, J. (2020). COVID-19 and beyond: Social work interventions for supporting homeless populations. International Social Work, 63(6), 790–794. https://doi.org/10.1177/0020872820949625
Young, S., & Fairbairn, N. (2018). Expanding supervised injection facilities across Canada: lessons from the Vancouver experience. Canadian Journal of Public Health, 109(2), 227–230. https://doi.org/10.17269/s41997-018-0089-7
Young, M. G., & Manion, K. (2017). Harm reduction through housing first: An assessment of the emergency warming centre in Inuvik, Canada. Harm Reduction Journal, 14(1), 8. https://doi.org/10.1186/s12954-016-0128-8
VI

Population Studies is a broad term used to describe the examination of how groups of people’s experiences are shaped by personal characteristics they share. Within this part of the book, we examine the impacts of gender, sexual orientation, and juvenile age on the causes and experiences of homelessness. We begin with a chapter on Gender and Queer Studies, followed by a chapter on Child and Youth Studies. As you work through these chapters, you are encouraged to critically reflect upon what these disciplines contribute to our knowledge and understanding of homelessness in Canada.
Perhaps as you read this, you are considering a career that relates to Population Studies, such as a Counselor, Teacher, or Child and Youth Advocate. The chapters in this section are designed to help you think critically about some of the questions you may encounter in these fields of employment. Understanding homelessness will help you navigate situations and choices you have to make. Consider, for example, a scenario in which a teenager self-identifies as being transgender but does not feel comfortable disclosing their gender to their family or peers and instead engages in self-harm behaviours. As a Counselor or Teacher, you may be situated within a school setting where you spend full days with the student. What signs might you want to look for to consider whether a student is at risk or oppressed within their home environment? As a Child and Youth Advocate, you may meet the young person only after they have had significant conflict and left their home. Likely, they have also left their school. How will you provide this young person with the support they need? How will you help to protect their human rights?
Before you begin, pause to consider how you would respond in each of the roles of the scenario above. With the knowledge you currently have about homelessness in Canada, why do you think one’s gender, sexual orientation, and/or age might impact the causes and experiences of homelessness? In the scenario, what might you do to reduce conflict within their family, discourage self-harm behaviour, and prevent the young person from leaving school and becoming homeless?
You are encouraged to keep this scenario in your mind as you read through the next two chapters and ask yourself whether any of your responses change, or are reaffirmed, after learning more about what Population Studies can teach us about homelessness in Canada.
VI
One of the authors of this book keeps a cardboard box in her office with black marker lettering that declares it the “Big Box-O-Gender Normativity.” In this box is a random assortment of objects that represent the mundane moments in everyday life where one is asked to declare their gender identity. The contents of this box routinely grow bigger, as colleagues and students contribute items they encounter along their way. One such item is a sign that hotel guests hang on the door to indicate they do not require room service and would prefer to have some privacy. On one side there is an image of a tie and on the other side is an image of a pearl necklace. Both sides have the same message, requesting privacy, but with different images arguably to identify the person requesting privacy as either a man or a woman, depending on which image of clothing is hung face-up.
There are literally countless times throughout our daily lives where we are asked to identify ourselves – as man or woman, masculine or feminine, straight or queer, tie or pearls – for reasons that often are not clear. The expectation that we define ourselves for others is so pervasive that we may not even take note of when or how frequently it occurs. The enactment and representation of gender and sexuality impact all aspects of our lives, and this is perhaps nowhere more clear than in the home. Ideas about gender and sexual orientation exist in the home and they reach beyond, to shape experiences of homelessness as well.
57
In this chapter, you are invited to open your own mental box-o-gender normativity and spend some time rooting around through it. Our investigation is directed by three key questions that guide this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind gender and sexual expression are felt at a very personal level, but there are demands placed upon us by social norms and expectations. When the way we feel and what others expect of us do not align, conflict can emerge. Read on to learn more about the multiple and complex ways in which gender and sexuality contribute to and shape experiences of homelessness in Canada.
58
We begin this chapter by presenting two composite scenarios that reflect real-world experiences of homelessness in Canada, as they pertain to Gender and Queer Studies. As you work through the scenarios, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenarios represent larger issues impacting people in our society.
After considering the real-world scenarios, we will endeavour to answer each question posed in the learning objectives. What is unique about the experience of homelessness for women? Do men and women have different needs when experiencing homelessness? Why is there a high rate of homelessness is the LGBTQ2S+ community? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenarios presented at the beginning and reconsider them in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
59
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with these real life composite scenarios. Take a moment here to pause and consider these people’s experiences.
Shruti
Shruti is a 23-year-old female who arrived in Canada from the US three years ago. She came to Canada originally to go to school. While in school, she was lonely and tried desperately to fit in with others. A young man, who helped her find an apartment, befriended her. He introduced her to alcohol and drugs. He played the role of devoted boyfriend for 4 months and then once she was completely dependent upon him for her drug supply, he started selling her to clients for sex. She became trapped in the sex trafficking trade. After a near fatal overdose, Shruti escaped from this man and disappeared to a new town. She is alone, frightened that he will find her, and has no resources or knowledge of the supports available to her.
Mia
Mia is a 17-year-old transgender woman fleeing an abusive relationship. She cannot go home to her parents, as they have disowned her for her “unacceptable behaviour,” with her father claiming that the “devil” was ruling her choices and that there is no place for the devil in his home. Mia goes to the local women’s shelter, whose mandate is to support women fleeing from sexual and domestic abuse. The intake worker indicates that they are very full. When pressed she tells Mia that they have a bed but that she doesn’t think they will fit in with the other residents (some of whom are children) and that there are no services tailored to their special needs. She is turned away.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to these scenarios again at the end of the chapter.
Reflection Questions
60
The real life composite scenarios introduced you to two women, one who was cisgender (having a gender-identity that aligns with her birth sex) and one who was transgender (having a gender-identity that is different than the male sex organs she was born with). Throughout this chapter we will refer to “women” and “men” with the recognition that one’s gender identity may or may not match the sex they were born into. We will explore this further in the third section of the chapter, but we feel it is important to step outside of that “gender normativity” box right from the start. While we have a section devoted to lesbian, gay, bisexual, transgender, queer and/or questioning, two-spirit, plus additional identities not named (LGBTQ2S+), we are not limiting our consideration of these individual’s experiences to just that one section.
As such, when we ask you here to consider what is unique about the experience of homelessness for women, we encourage you to consider this question in light of all women who represent a broad gender diversity. How might homelessness be different for cisgender women, transgender women, and gender diverse people compared to cisgender men, for instance? What additional considerations might women and feminine identified individuals have that are unique to their experiences? As you consider these questions, we encourage you to use the space below to record your answers. You may write as little or as much as you wish to explore your thoughts on this issue.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=718#h5p-69
We began this chapter by sharing the tale of a hotel door hanger that can be hung on either the tie or the pearls side to indicate the occupant – a man or a woman – does not wish to be disturbed. Why a person would need to make an outward declaration of their gender identity to the hotel cleaning staff remains unclear, but beyond that it is unsafe. When this item is discussed with students in a classroom setting, they often raise the point that people who identify as women (whether cisgender, transgender and/or gender diverse) may not be inclined to put the pearl necklace side up because it signals to passersby that there is a woman inside. Students suggest that even if a person identified as a woman, she would be more likely to put the tie side up for the sense of safety it provides. While a very simple example, this idea of which side to hang the sign on is actually rather informative about issues women face related to homelessness – namely, trying to remain hidden to increase a sense of safety and the risks of presenting with a female identity in a society that can often be quite predatory.
In this section, we consider what is unique about the experience of homelessness for cisgender women, transgender women, and gender diverse feminine individuals. What we see is that the issues are complex and intersecting. Research has shown that homelessness often begins early in life for women and gender diverse individuals, and that their subsequent experiences tend to be a chronic and chaotic cycle of moving in and out of precarious housing situations (Schwan, Vaccaro, Reid, Ali, & Baig, 2021b). Women are commonly amongst the hidden homeless population, moving between temporary accommodations rather than entering the emergency homelessness sector, because of gender inequity and a range of structural factors beyond their control (Andermann et al., 2021).
As we will see throughout this section, women’s experiences of homelessness tend to be directly related to gender-based violence and trauma. They often have children in their care that they try to protect from harm or from being removed by child welfare authorities. When children are removed, as we will see, the impact can be further trauma, isolation, and grief. Homelessness has a deeply negative impact on the health and well-being of cisgender and transgender women. Surviving homelessness requires a tremendous amount of strength to overcome these obstacles. Often the first obstacle is – much like the door sign dilemma – trying not to be noticed by people who may take advantage and exploit them. In the first video, Dr. Jacqueline Kennelly explains further.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Jacqueline Kennelly argues that unlike men, who tend to be visible on the streets and in emergency shelters, women’s homelessness is often more hidden. Because it is not safe for women to be on the streets, particularly at night, they are more likely to protect themselves by partnering with a man or group, couch surf, trade sex for a place to stay, and/or move around each night. This video is 1:39 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Women’s homelessness
Cisgender women, transgender women, and gender diverse individuals may avoid shelters for safety reasons and instead stay temporarily in someone else’s residence. They may stay with friends or family, they may stay with someone they are in a relationship with, or with someone who is accepting sexual favours in exchange for accommodations. Research has shown that women and gender diverse people face significant barriers in accessing emergency shelter beds when they need them (Schwan et al., 2021b). Consequently, many women in precarious housing situations are reliant on relationships to maintain their accommodations. Consider, for instance, the results of the Pan-Canadian Women’s Housing & Homelessness Survey, which indicated experiencing a breakup was the primary reason women and gender diverse individuals lost their most recent housing (Schwan et al., 2021b).
When a woman loses her housing, she often has limited resources and options available. In a study of how communities use a gender-based approach to homelessness prevention and planning, Dr. Abe Oudshoorn and his team (2021) found that cisgender and transgender women are under-recognized and underserved by a general lack of tailored interventions for this population. They further note that part of what is driving this lack of services is a gap in data about the diversity of women’s needs related to gender identity, sexual orientation, and ethnicity (Oudshoorn et al., 2021). In the next video, Dr. Abe Oudshoorn explains further how many of our current homelessness sector approaches were designed for cisgender men and the impact that has on women seeking to access these supports.
In this video, Dr. Abe Oudshoorn argues that our current homelessness systems and processes were designed around the needs of middle-aged white men, making them unintentionally exclusionary to cis and trans female-identified individuals. He notes that homelessness is a gendered experience, including the pathways in, experiences of, and exits from. Dr. Oudshoorn provides the example of prioritization, in which acuity assessments are given to people at shelters and through street outreach to determine their level of need. These efforts often fail to identify women, who are more likely to be experiencing hidden homelessness outside of these locations. Through this approach women go unnoticed, making them less able to access services and supports tied to the assessments. Further, when women are included, their acuity scores tend to be lower because the metrics are defined in a narrow way that does not account for the severity of their situations. Dr. Oudshoorn further notes that female-identified individuals are at high risk for sexual violence and exploitation, and that they comprise the majority of single-parent families within the shelter system. This video is 4:24 in length and has closed captions available in English.
Key Takeaways – Dr. Abe Oudshoorn: Exclusionary system responses for women experiencing homelessness
There are many reasons why women and gender diverse individuals lose their housing. However, experiences of violence and the resulting lack of safety are amongst the most prevalent. The Pan-Canadian survey, for instance, showed that safety issues are common concerns that threaten the housing stability of women and gender diverse individuals, and that 75% report being survivors of trauma or abuse (Schwan et al., 2021b). In the chapter on Public Health, we discussed the challenges of telling people who are without housing to “stay home” as a protective measure. Consider how this same message – to stay home – would sound equally distressing to a woman who might be housed but in a violent relationship. Yakubovich and Maki (2021) considered women’s experiences of gender-based violence during COVID-19 and noted that while the Federal government increased financial support to Violence Against Women (VAW) shelters, the nation still lacks a coordinated strategy, legislation, and funding framework to support coordinated interpersonal violence prevention efforts.
As Oudshoorn et al., (2021) noted previously, a major concern is that women and gender diverse individuals are at increased risk of gender-based violence, but they require interventions that are not just tailored to gender, but to sexual orientation and ethnicity as well. We encourage you to think about the different needs that cisgender women, transgender women, and gender diverse individuals may have to help prevent experiences of violence in their lives and promote recovery when it does occur. These next two videos provide further insight into the intersections of homelessness and domestic violence, as well as the critical need to incorporate anti-racist practices into our approaches.
Gender-based violence is a prevalent reason why many women and gender diverse individuals experience housing instability and loss. These experiences are not uniform, but rather require consideration of how structural factors, such as racism and discrimination, shape the rates and occurrences of gender-based violence related homelessness. Additional factors like substance use can also intersect with, and increase risks of, experiencing violence for women and gender diverse individuals (Kitson & O’Byrne, 2020; Meyer et al., 2019).
Structural factors of power and control can be deeply imbedded in these harmful relationships, leading to acts of violence being committed against women and gender diverse individuals. At the same time, power and control make it difficult to escape. Flynn et al., (2018) have conducted focus groups in Quebec City and identified two interconnected gendered pathways related to social exclusion and social control. They found that as women tried to overcome social exclusion in these relationships and fulfill their basic needs, they were vulnerable to social control by their abuser, and at the same time, this control increased their dependency and social exclusion (Flynn et al., 2018).
Women and gender diverse individuals are at risk of violence and trauma while housed and it continues through their experiences of homelessness. Leaving an abusive partner, while a positive step, does not protect the woman from violence and abuse she may experience in shelters or while seeking temporary housing with someone she knows. In the next video, Dr. Katrina Milaney explores the histories of trauma many women have and the continuation of these experiences through homelessness.
In this video Dr. Katrina Milaney argues that every person who experiences homelessness has had some trauma in their life, often dating back to childhood. For women, these traumas tend to be compounded by long histories of violence, exploitation, and victimization that have deeply negative implications for mental health, that get worse the longer a woman remains in homelessness. Yet, women’s homelessness can be difficult to identify as many avoid shelters for safety reasons, opting instead to couch surf or remain in unsafe housing situations. Dr. Milaney notes that a unique aspect of women’s homelessness is that of mothering and/or becoming pregnant. While caring for a child is a major consideration, she argues that many interventions are directed at single adults and youth, as opposed to the family unit. She concludes that more supports are needed to support women and families experiencing homelessness. This video is 2:18 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: What is unique about the experience of homelessness for women?
Dr. Milaney and her team (2020) have analyzed a subset of 81 women experiencing homelessness in Calgary to learn about how their experiences differ from those of men. They have found that women have greater mental health concerns, suicidal thoughts and attempts, and adverse childhood experiences. Based on their findings, they argue we must understand these factors as being highly interconnected and ensure women have access to appropriate services that are gender-specific and trauma-informed. We invite you now to read more about this study in this section’s featured reading.
Milaney, K., Williams, N., Lockerbie, S. L., Dutton, D. J., & Hyshka, E. (2020). Recognizing and responding to women experiencing homelessness with gendered and trauma-informed care. BMC Public Health, 20(1), 397.
Women and gender diverse individuals experience multiple forms of violence and victimization in their lives. When you think about this, you may think of domestic interpersonal violence that occurs within the home, but we also need to consider the prevalence of sexual trafficking that occurs across the country. When someone is without their own secure housing, their level of vulnerability increases. This creates a ‘no win’ situation, as women and gender diverse individuals who stay in emergency shelters may become known to predators through their presence, and those who try to remain hidden may encounter dangerous people in unmonitored spaces. Consider this issue, of sexual trafficking in Canada, as you watch the next video with Dr. Katrina Milaney, followed by a brief public awareness video created by Peel Regional Police in Ontario.
In this video, Dr. Katrina Milaney discusses human trafficking for sexual purposes as being a particular kind of trauma and violence that women experience. She notes that it can occur in all size communities, including those that are rural, and that by moving these women around those who exploit them are disconnecting them from social supports, such as friends and family, and emergency supports, such as the police. This video is 1:26 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: Women’s homelessness and rural trafficking
Researchers have evaluated interventions aimed at supporting individuals experiencing homelessness related to gender-based violence to learn more about what is effective. Young women who participated in a community-based, trauma-informed group intervention reported that they appreciated the program was safe, for women-only, allowed them to share lived experiences, and incorporated tailored psychoeducation to improve their confidence, coping skills, health, relationships, and future directions (Reid et al., 2020). Additional research has shown that these programs remain effective over time. After 12 months, in one study, there was a significant improvement to the quality-of-life reported by women in the community-based, trauma-informed group intervention (Bani-Fatemi et al., 2020). These findings indicate programs like this need to be securely funded, so that they have the ability and resources to offer ongoing supports on a consistent basis.
Another study that looked at an intervention for survivors of sexual exploitation, forced marriage, and “honour” crimes, found that in order to be effective approaches should focus on the service user’s needs, be flexible and accessible, and draw upon strong connections within the organization and beyond (Kahan, Lamanna, Rajakulendran, Noble, & Stergiopoulos, 2020). It is important that we think about the best way to offer support to women and gender diverse individuals coping with violence and trauma in their lives, including through evidence-based interventions like post-shelter advocacy counselling, case management, and permanent housing subsidies that offset the cost of housing (Andermann et al., 2021). Gender-based violence is a pressing issue that greatly impacts women and gender diverse individuals at higher proportions. In the next video, Dr. Katrina Milaney explains why “trauma-informed care” is not a buzzword, but rather a critically important approach for supporting survivors.
In this video, Dr. Katrina Milaney discusses the experience of violence as being a particularly gendered pathway into homelessness for women. She notes that service delivery has increasingly moved towards the recognition that safety must be a key consideration in finding housing and making policies that impact women. She further notes that many women who experience homelessness have children, who may or may not be in their care, and that the removal of children is a form of trauma that requires healing. Dr. Milaney concludes that trauma-informed care is not a buzzword, but rather critically important in acknowledging and responding to the histories of violence and exploitation that women have been through. This video is 2:20 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: Women’s homelessness and trauma-informed care
We have seen that women and gender diverse individuals are at an increased risk of gender-based violence, and that these risks are present whether housed, in a shelter, or seeking temporary accommodations with someone they know. We encourage you now to consider an aspect that has been noted previously but deserves independent consideration: women may not be alone in these situations. Many women who experience homelessness are also actively caring for children, while others may be coping with the loss of children who have been removed from their custody.
What additional considerations and challenges would a woman have if she were experiencing homelessness while caring for children?
If a woman’s children are in her care or she is trying to regain custody, securing affordable and appropriate housing is a particular challenge. Housing must meet the needs of the family and child welfare workers will consider the size, number of bedrooms, and sleeping arrangements in making their determinations about whether to return a child to parental care. Further, if a woman is in subsidized housing and has her children removed by the state, she will often be removed from her housing unit as well because she is considered “over-housed,” such as a single person living in a three-bedroom apartment. While one must wonder if being “over-housed” is really the issue to focus on, when that same woman seeks to regain custody of her children she is likely to be denied because she does not have housing suitable to her children’s needs. When we talk about systemic barriers that impact women’s access to housing, this is one such example of the gaps in the system.
We routinely ask you to put yourself in someone else’s shoes and here we do so again. The cards below are quotes from two women who at the time were mothering while experiencing homelessness. They demonstrate the challenges mothers go through in trying to care for their children while maintaining housing and looking after their own well-being. As you read these cards, we encourage you to continue to think about how women’s experiences of homelessness – and what they need – are often different than that of a single adult cisgender man, for whom most homelessness services are designed.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=718#h5p-70
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=718#h5p-71
Dr. Sarah Benbow and her team have explored the intersections of homelessness and mothering and found that these women have to navigate unsafe private and public spaces, related to exclusion from society and stigma resulting from public discrimination and surveillance (Benbow, Forchuk, Berman, Gorlick, & Ward-Griffin, 2019b). They further found that when these mothers sought support from the homelessness system, they received contradictory responses that were supposed to offer help but served to further perpetuate their experiences of exclusion (Benbow, Forchuk, Gorlick, Berman, & Ward-Griffin, 2019c). As a result, women who are mothering while experiencing homelessness may internalize the expectations and regulations upon them while also pushing back as a source of resilience and resistance (Benbow, Forchuk, Berman, Gorlick, & Ward-Griffin, 2019a). According to Benbow et al., (2019a) women in these situations have demonstrated a keen sense of agency, by working and advocating for safety and housing for themselves and their children.
Research has shown that ecologically based treatment (EBT) is particularly effective for helping mothers with children in their care become securely housed, by helping them develop life skills, connect with services in the community, engage in therapeutic dialogue, and process trauma and victimization they may have experienced (Murnan, Zhang, & Slesnick, 2018). Processing trauma, as we have seen, is critical for many women experiencing homelessness, whether they are parenting or not. In the following video, Dr. Naomi Thulien explains how parenting and trauma are two prominent gendered aspects of homelessness, that can often go hand-in-hand.
In this video, Dr. Naomi Thulien identifies two unique aspects of women’s homelessness. First, she notes, women may have children or become pregnant. Caring for a child is an added responsibility that makes it more challenging to move through social systems, increases vulnerabilities associated with living in poverty, and often results in the mother putting her own needs after those of her children. Secondly, Dr. Thulien argues that women who experience homelessness are at increased risk of sexual exploitation, through trafficking and assault. This video is 1:00 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: What is unique about the experience of homelessness for women?
Dr. Thulien identifies an important consideration when she says that cisgender women may become pregnant while experiencing homelessness. This is a unique aspect of women’s homelessness that can have an impact on how she views her body and her safety. Further, women who become pregnant may have to navigate issues such as whether to take or discontinue medications, whether to use drugs and/or alcohol, and even whether accessing harm reduction supports like methadone maintenance therapy are advisable. Given these circumstances, cisgender women’s experiences and choices while experiencing homelessness are unique. On the reserve side, when a woman is not pregnant she is likely to menstruate at some point during her time experiencing homelessness. Menstruating in a shelter or on the street, without reliable access to private washrooms or sanitary products, and without the comforts of a bed or couch, are quite simply a pain. We invite you to watch the video, “How do homeless women cope with their periods?” to learn more.
Women’s experiences of homelessness are indeed unique in many ways. Throughout this section, we have regularly cited results from the Pan-Canadian Women’s Housing & Homelessness Survey. This survey identified many key challenges that women and gender diverse individuals face in Canada including, but not limited to, living in deep poverty, needing to undertake financial management strategies such as skipping bills or taking out additional credit cards that are harmful and often increase debt, and being evicted or losing housing due to many forms of discrimination (Schwan et al., 2021b). In the final video of this section, the report’s lead author Dr. Kaitlin Schwan addresses the question of what is unique about the experience of homelessness for women. We have chosen to present this video as the last in the series because Dr. Schwan identifies 4 key aspects that align perfectly with the themes of this section and serve as an excellent summary and review for you to reflect upon.
In this video, Dr. Kaitlin Schwan argues that women experiencing homelessness have unique causes, conditions, and consequences of being on the streets, experiencing core housing need, and experiencing homelessness. She identifies four particular considerations that relate to women’s homelessness. First, women are more likely to experience hidden homelessness and are subsequently less likely to come to the attention of policymakers and politicians. This invisibility results in lower prioritization and funding for gender-based services. Second, Dr. Schwan argues that violence is a presence in women’s lives before becoming homeless, once on the street, in the shelter system, and once they have transitioned out of homelessness. She notes that these experiences create tremendous harm and that the kinds of responses we have around women’s homelessness need to be proportionate to the level of violence that this group experiences. Third, she argues that women are more likely to be caregivers for children and other family members. This adds an additional responsibility on top of earning an income and results in single mothers being over-represented among those living in poverty. Additionally, women in poverty often have their children removed from their care and our child welfare, housing, and homelessness systems operate in ways that create tremendous challenges for women trying to reunite with their children. These systems form particular barriers for racialized women and Indigenous women experiencing homelessness. Finally, Dr. Schwan concludes that there are unique health circumstances for women, gender diverse, and transgender individuals experiencing homelessness which include pregnancy, access to period supplies, and access to sexual health services. This video is 6:02 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: What is unique about the experience of homelessness for women?
In this section, we asked you to consider how women might experience homelessness in ways that are unique. We noted that our discussion was intentionally inclusionary of the range of ways a person can identify as a woman, whether cisgender, transgender, or gender diverse. Throughout our discussion, we saw that women are often amongst the hidden homeless population as a means of avoiding shelters and trying to protect themselves. We also, unfortunately, saw that gender-based violence and trafficking were common for women regardless of whether they stay in shelters or not. These experiences are so common amongst women and gender diverse individuals that a national survey showed 75% of respondents reported being a survivor of trauma or abuse (Schwan et al., 2021b). The need for gender-based and trauma-informed supports is undeniable for this population.
After considering the hidden nature and high rates of violence associated with women’s homelessness, we asked you to think about the additional layer of also being a mother. We saw that some women have children in their care, while others have had children removed. For all of these women, obtaining safe, secure, and affordable housing is key to being able to parent without the added stress and hardship of homelessness. As Canada moves forward with the National Housing Strategy and National Housing Strategy Act (Government of Canada, 2017, 2019), it will be imperative that the right to housing be implemented strategically for women and gender diverse individuals (Schwan, Vaccaro, Reid, & Ali, 2021a).
Women’s unique needs, related to insecure housing, violence and trauma, mothering, and reproductive health all contribute to the need for gender-specific approaches to addressing homelessness for this population. We must remember that not every woman’s experience is the same, and so these approaches also need to be representative of women’s diverse gender, sexual, and ethnic identities. As Van Berkum and Oudshoorn (2019) have argued, it is imperative that we create new programs with a diverse set of women in mind – reflecting their needs for affordable housing, safety, and to be supported by people trained in trauma- and violence- informed care.
Click the link below to listen to all of the researchers answer the question “What is unique about the experience of homelessness for women?” in audio format on our podcast!
61
There is sometimes a mistaken tendency to assume that “gender” means “women.” This does a great disservice to men and women alike. While we have been considering the experiences of cisgender and transgender women, we also need to recognize that this is not the extent of gender studies. Now that you have learned more about women’s experiences of homelessness, we encourage you to pause and consider how these experiences might differ from those of men. Again, we encourage you to think about people who identify as cisgender and transgender in your response. Do you think men and women have different needs when experiencing homelessness? Before you continue through the section, take a moment to record your thoughts in the space below.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=720#h5p-72
As you probably have guessed by now, this question is not as straightforward as it seems. Just as we asked you to take on a gender-inclusive perspective when considering what is unique about women’s homelessness, we are going to encourage you to do the same here. We set out to see whether men and women have different needs when experiencing homelessness, with the stated recognition that these are not dichotomous categories. When we ask about men’s needs, we are considering cisgender men, who were born with genitalia that matches their gender-identity, but we also include transgender men and the range of gender diverse identities people may have that align with different forms and representations of masculinity. In the same way, we ask that you keep in mind that when we refer to women, we are talking about cisgender women but also transgender women and gender-diverse individuals whose identity may align with femininity in a range of different ways. Gender is, and never has been, as straight forward as a blue or pink nursery would have us believe.
With this caveat in mind, we set out to see whether the needs of men and women are different. If you are coming to this section after having read the one before, you will know that part of the answer must be ‘yes’ because we saw that women have unique needs. However, part of the answer is also ‘no’ because what people fundamentally need as basic human rights remain the same. Consider this starting point of the discussion as you watch this video of Dr. Naomi Thulien in which she explains further.
In this video, Dr. Naomi Thulien argues that while they may have different experiences, men and women fundamentally have the same needs. These include the need for a safe place to be, a living wage income, and to feel a sense of belonging. This video is 0:48 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: Do men and women have different needs, when experiencing homelessness?
If we approach the question of whether men and women have different needs when experiencing homelessness from a human rights perspective – as we must – it is simple to see that people’s fundamental needs are the same. Everyone, regardless of their gender identity, needs safe and secure housing, equitable access to health care, a livable income, and to feel that they belong within their community. Where we see some differences arise is when we look at how to ensure men and women have their needs met.
In recent years, authors in a couple of studies, have examined quality of life variables for men and women experiencing homelessness and begun to pinpoint some of the areas where gender differences emerge. For instance, Gentil, Grenier, Bamvita, Dorvil, and Fleury (2019) conducted a study with 455 people who had current or previous experience of homelessness in Quebec. They found there were four clusters that emerged. Those with the highest reported quality of life were older women who had low functional disability and relatively few episodes of homelessness. A second cluster that emerged in the data with high quality of life scores were individuals living in temporary housing with relatively few mental health or substance use disorders. Lower quality of life was reported by the third cluster, comprised of middle-aged women living in temporary housing, with criminal records, personality disorders, and substance use disorders. Finally, the fourth cluster, who also reported low quality of life scores, were individuals with multiple homeless episodes, complex health problems, and frequent service use. Gentil et al., (2019) conclude from their data that the findings served to reinforce the need for programs that are adapted and tailored to the unique needs of individuals within these different groups. It is clear from this study that gender is a factor that intersects with quality of life variables, such as having housing, being in good physical and mental health, and having stability in one’s life.
In another study, Buccieri, Oudshoorn, Waegemakers Schiff, Pauly, Schiff, and Gaetz (2020) conducted a regression analysis of 343 people experiencing homelessness in Toronto, Victoria, Calgary, and Regina. They examined multiple variables that could contribute to positive or negative quality of life for men and women, as divided by self-reported gender. Some of the results were the same regardless of a person’s stated gender. For instance, men and women both reported that poor sleep quality and duration decreased their mental well-being. However, the results also clearly showed that there was some variability in quality of life reported by gender. In this study, it was found that having poor health led women to feel stressed and unsafe. The men who reported being in poor health reported having higher levels of depression, but also that improved health contributed to enjoyment of life, feeling relaxed, and being happy. These same links were not found for women, which suggests that physical health may be an underlying factor in negative mental well-being for women and men but in different ways (Buccieri et al., 2020).
Additional results from the Buccieri et al., (2020) study found that having regular access to food was particularly important to the emotional well-being of men and that going without it led to stress, loneliness, decreased life enjoyment, and feeling unsafe. Men also reported that when they were able to drink clean water and eat breakfast, lunch, dinner, and a snack throughout the day their mental health would improve. Access to food was a major quality of life issue for men, but not nearly as pressing for women, who reported that eating dinner was the only significant food-related factor leading to greater enjoyment of life. Clearly food is an important gendered variable. This is not to suggest that women do not need food as much as men do, but rather that women might be more used to going without and prioritizing the needs of others (such as their children) before their own. Men, particularly if cisgender or taking testosterone, might also require higher caloric intake and need a higher quantity of food to meet their daily goal.
An interesting finding that came out of the Buccieri et al., (2020) study was the direct relation between men feeling good and the absence of variables that made them feel bad. This may seem obvious, that a person would feel good if there was nothing making them feel bad. Yet, this same finding did not emerge for women. For women, there had to be components in their life that made them actively feel good, whereas men felt good if there was nothing making them feel bad. This finding suggests that one approach to improving men’s emotional well-being while experiencing homelessness, is to address the factors that are bothering them. Conversely, women may need strategies that not only remove factors making them feel bad, but also have approaches that actively make them feel good.
It is clear from these studies that women and men have the same fundamental needs – such as for housing, equitable access to health care, a livable income, and community inclusion – but that how (or whether) they get these needs met differs by their identified gender. We encourage you to keep this idea in mind – that the fundamental needs are the same, but the approach differs – as you watch this video from CBC that follows four men experiencing homelessness through their daily lives in Toronto. How might the video be different if they followed women as well?
This video shows the lives of four men in Toronto, living in shelters and in tent encampments. What the men say they need is simple. They want their own housing. They want to get a good night’s sleep. They want to work and be part of society. They want to be treated with respect. They don’t want to be eaten by rats. We asked you to watch the video while considering how the needs expressed might be different for men and women. We can take a leap of faith and say that women would also want housing, sleep, income, inclusion, respect, and to be free from infestations. Yet, we can also think about where some key differences might emerge. One of the key differences is that of safety. Whereas Frenchie said he felt safe living under a bridge in a tent, we know that many women seek accommodations inside even if in unsafe places. Whereas these were single men, women often are in mothering roles with their children in their care. The housing they need is very different than the housing a single adult man would need. This is not to suggest that men do not also parent while experiencing homelessness, but that much less is known about those who do.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=720#h5p-73
If we think about the video of the four men in Toronto, we can also see an example of what Buccieri et al., (2020) found about men’s wellness. For men, improved mental wellness results from taking away the things that are wrong. For Frenchie, removal of the rats would likely go a long way to increasing his well-being. Although, this is certainly not enough. Research on what men need has shown that they benefit from mental health programs that are community-based, flexible to allow for continuity of daily routines, offered in a secure environment, and incorporate mental health and social supports (Voisard, Whitley, Latimer, Looper, & Laliberté, 2021). Men may face barriers to housing and service use related to mental health challenges, drugs or alcohol use, unaddressed trauma, and physical health limitations (COH & Blue Door, 2021). Certainly, these barriers also apply to many women experiencing homelessness, but the way they impact men and women are often different. Research has shown that having a social network is important for men, such as in managing chronic health conditions (Merdsoy, Lambert, & Sherman, 2020), yet developing these social networks may be challenging amidst the isolation of homelessness. We saw this in the video, as one man explained his friends do not know he lives in a shelter. It is difficult to seek support when you do not feel comfortable sharing this level of personal information.
Gender expression is a key factor here. Whether a person identifies as feminine, masculine, or anywhere along a gender spectrum has an impact on how they view themselves as well as on how others treat them. This is an unfortunate aspect that may lead men to resist showing vulnerability, women to hide as a means of self-protection, and everyone’s quality of life to be impacted by negative stereotypes and stigmas. In the next video, Dr. Kaitlin Schwan speaks about discrimination that people experiencing homelessness face, and why we need to approach solutions through a gender-based equity lens.
In this video, Dr. Kaitlin Schwan discusses the gender specific needs of men, women, and gender diverse individuals, such as those who are transgender and/or two spirit. She notes that gender diverse individuals experience systemic discrimination in health care, education, and the criminal justice system, along with higher levels of violence, exclusions, and marginalization that make the needs of this group extremely urgent to address. Dr. Schwan further notes that gender specific supports and interventions need to be defined by the communities that use them, in line with seeing themselves as experts in their own lives and integrated into program and policy design. She argues that housing is a solution to all homelessness, but that we must also consider gender-specific factors. She cites findings from the 2021 Women’s National Housing and Homelessness Survey, which indicated that the break-up of a romantic relationship was the most common reason women reported losing their housing, as an example of the need for gender specific policies and program interventions. Dr. Schwan concludes by calling for an increase in Indigenous led and controlled community supports, particularly for Indigenous women, girls, and gender diverse individuals. This video is 3:30 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: Do men and women have different needs when experiencing homelessness?
When experiencing homelessness, all people have the same fundamental needs for housing, health, income, and inclusion but the particulars will be shaped by a person’s identity, including by their gender, sexuality, ethnicity, and ancestry. These factors will interact in ways that lead to different expressions and representations of gender on the street. What it means to be “a man” has traditionally been very narrowly defined as being associated with power, dominance, and strength without space for expressions of vulnerability, emotions, or need for support. What it means traditionally to be “a woman” has been similarly narrow and defined in opposition to men. This traditional structure leaves very little room for a person to express gender in complex ways. However, as we have tried to challenge you to consider throughout this chapter, these limited gender expressions are not how people actually engage with gender, nor do they capture the extent of gender identities. When we speak about the needs of women, we must consider the range of ways feminine gender is expressed, and when we speak about the needs of men, we must also consider the range of ways masculine gender is expressed.
Julia Wardhaugh (1999) has written that the streets are the quintessential male space, where men have freedom to make their presence known. Do you think this is true of all men or are some forms of masculinity given more privilege than others in the context of the street? What might make a man feel less comfortable within spaces associated with the street – like shelters and tent encampments?
As you consider this question, of how masculinity is expressed and whether some forms are more privileged than others, we invite you to read this section’s featured reading. The authors of this article examine sexual exploitation of homeless and street-involved boys living in Western Canada. As you read this article, we encourage you to reflect on what you have learned about the needs of women and men, and the diversity of gender identities and expressions that exist amongst people experiencing homelessness.
Saewyc, E. M., Shankar, S., Pearce, L. A., & Smith, A. (2021). Challenging the stereotypes: Unexpected features of sexual exploitation among homeless and street-involved boys in western Canada. International Journal of Environmental Research and Public Health, 18(11), 5898.
Just as women each have their own individual experiences of homelessness that are shaped but not determined by gender, so too do men. In a three-year ethnographic study of a weekly floor hockey program in Edmonton, Koch, Scherer, and Holt (2018) observed that while the program was largely funded to reproduce a particular kind of traditional masculinity, what they actually observed was how participants use the program in diverse and sometimes contradictory ways to express themselves. We can see how there are gendered expectations placed on people experiencing homelessness, and how people may respond in ways that at times reaffirm them and at times challenge and resist them.
Dr. Jacqueline Kennelly (2020) has written about young men’s navigation of urban spaces, noting that while there is an internal logic to their practices under the conditions of extreme inequality that neoliberalism produces, they are also caught in a cycle of reinforcing their marginal positions through exposure to violence and criminalization by the state. In the next video, Dr. Kennelly explains that one reason she came to reflect upon expressions of masculinity stemmed from research she conducted with youth experiencing homelessness in Ottawa. She and her team were creating videos with these young people as part of a project entitled, “Encountering Democracy.” We first share a video of Dr. Kennelly speaking about the project and then invite you to watch the piece on youth and policing that was created during the study. We would like you here to think about the gendered aspects as you watch this film. We will explore policing and the criminalization of homelessness further in the chapter on Sociology & Crimino-Legal Studies.
In this video, Dr. Jacqueline Kennelly shares a story a young man told her about entering a courthouse in Ottawa and being asked to remove his hat by the guard at the door. This story is used to demonstrate the ways in which gender expectations are taken up and enforced in public spaces in ways that are often different for men and women. While the same guard likely would not have asked a woman to remove her hat, the attention this young man received shows an additional level of policing that is more common of men’s experiences. This video is 5:19 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Do men and women have different needs, when experiencing homelessness?
In this section, we asked you to consider whether men and women have different needs when experiencing homelessness. Keeping with the theme of the book, this is a seemingly simple question with a rather complex answer. At the root of the question, we can see how men and women have the same very fundamental needs. Everyone, regardless of their gender identity, needs a safe and secure place to live, an income to support themselves and their dependents, to have access to health and mental health supports so they can be well, and to feel included and accepted by their society without facing discrimination. These are the same needs, and the same basic human rights, people of all gender identities are entitled to.
Where we see differences arise, is when we start to look more closely at how people express their needs and seek to have them met. We saw, for instance, that quality of life was impacted by gendered variables, particularly related to health, hygiene, and regular access to food. Whereas men reported feeling better when the things that bothered them were taken away, women needed targeted supports to help them feel good. These indicate very different approaches to meeting men’s and women’s needs, despite having the same ultimate needs overall.
We invited you to watch a video of four men’s experiences in Toronto and challenged you to consider how the video might be different had women also been included. We saw through this section that gender expectations are a key determinant in shaping people’s experiences of homelessness, but that we cannot (nor should not) rely on outdated and narrow definitions of what gender means. When we do so, we limit our ability to understand people’s experiences, self-expression, and basic needs. We concluded this chapter by asking you to rethink traditional notions of hegemonic masculinity that are harmful to cisgender and transgender men, gender diverse individuals, and society as a whole. If we want to understand how the needs of men and women are different when experiencing homelessness, we must discard outdated notions of gender and open our minds to a broader, more inclusive, and more accurate spectrum of gender possibilities.
Click the link below to listen to all of the researchers answer the question “Do men and women have different needs, when experiencing homelessness?” in audio format on our podcast!
62
Throughout this chapter, on Gender & Queer Studies, we have encouraged you to think about the experiences of cisgender and transgender individuals. Here we dive further into explorations of how gender identity, sex, and sexual orientation impact a person’s experience of homelessness. We have chosen to use the acronym “LGBTQ2S+” throughout this book but recognize that there are different iterations of terms that are included (or not) in other versions. For instance, you may have heard “LGBT” or “LGBTQ,” which are also commonly used. We have selected to use the longer acronym as an attempt to represent as many identities as possible, including, Lesbian, Gay, Bisexual, Transgender, Queer and/or Questioning, 2-Spirit, + other identities not captured by the previous letters.
It is an undisputed fact that there is a high rate of homelessness amongst people who identify as LGBTQ2S+. For this reason, we did not ask the question of whether they are more likely to experience homelessness, but instead chose the more complex question of why the rates are so high. Before continuing to the material in this section, we invite you to pause here and consider this question on your own first. You may use the space below to record your thoughts. Feel free to write as little or much as you would like to answer this question.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=722#h5p-74
We began the Introduction chapter by asking the question, “What is homelessness?” This was intentionally done so that we started our discussion with a shared definition and understanding of what we meant by homelessness. In much the same way, we begin this section on LGBTQ2S+ homelessness with a review of definitions and key terms. Whether you are keenly familiar with this acronym, you have heard it but are unsure what it means, or this is your first introduction, we invite you to watch this brief explanatory video created by the TASCC AHS Sexual & Reproductive Health Calgary Zone.
While Canada prides itself (yes, pun intended) on being an inclusive nation, we are still far from being an equitable and egalitarian society in practice. It is important that we recognize the experience of gender and sexually diverse individuals as a standalone chapter, but also throughout this book as issues of gender and sexuality intersect with all aspects of homelessness. Structural issues, like homophobia and transphobia, create enormous barriers for people in all sectors across our society. We see these barriers in housing, health care, mental health care, and education, among many others. We can see in the quote below, how a person’s LGBTQ2S+ identity may be a source of discrimination in their lives, such as when at school.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=722#h5p-75
Much of what we know about LGBTQ2S+ homelessness comes from research on youth who have been forced to leave home and are experiencing homelessness or housing instability as a result. It can be difficult to know exactly how many young people there are that fit this description in Canada. LGBTQ2S+ youth may be reluctant to identify themselves, for fear of discrimination or violence, and may be more likely to find alternatives to staying in shelters. For these reasons, we do not have an exact figure. However, estimates suggest that 20-40% of young people experiencing homelessness are LGBTQ2S+, which is largely over-representative of the estimated 5-10% of the housed youth LGBTQ2S+ population (Abramovich & Shelton, 2017b). This tells us that although these youth make up a small percentage of the population, many of them become homeless. Consider this figure as you watch the video below of Dr. Naomi Thulien speaking about the high percentages.
In this video, Dr. Naomi Thulien explains that 20-40% of young people who experience homelessness identify as LGBTQ2S+. They often are forced to leave home because their families do not accept them but that some might find a sense of community among other LGBTQ2S+ youth who are also experiencing homelessness. This video is 0:46 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: Why is there a high rate of homelessness in the LGBTQ2S+ community?
In this video, Dr. Alex Abramovich states that up to 40% of young people experiencing homelessness in Canada identify as LGBTQ2S+, which means they are disproportionately over-represented. He argues that while family conflict is a leading cause of youth homelessness in general, for LGBTQ2S+ youth, this conflict is often specifically tied to the young person’s identity. He notes that this conflict might arise after a youth has disclosed their sexual orientation, and either has been forced out of the home directly or has found the environment to be so unsafe and unsupportive that they feel they have no choice but to leave. This video is 1:51 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Why is there a high rate of homelessness in the LGBTQ2S+ community?
In a study with 16 LGBTQ2S+ youth experiencing homelessness, Côté and Blais (2021) found that all of their participants reported having lived in a family environment that was neglectful and led to decreased self-confidence and trust in their families. They identified this family neglect as a starting point for three trajectories toward homelessness. These included being evicted by families that perpetuate heterocisnormative victimization, aging out of youth protection services without supports in place, and fleeing form bullying at school as an attempt to gain freedom and support. Reflecting on their findings, Côté and Blais (2021) note that it is important to develop homelessness prevention strategies for LGBTQ2S+ youth that consider the heterocisnormativity they experience in different life environments.
Heterocisnormativity is a big word that you may not have previously heard. That’s okay. Part of the work of preventing and ending LGBTQ2S+ homelessness is recognizing shortcomings in our collective knowledge. Even in writing this chapter, it becomes apparent to us as authors (although you will not see it as readers) that words like heterocisnormative and heterocisnormativity are so uncommonly used in daily language that they are underlined in squiggly red by our word processor, suggesting we are using a word that does not exist (although it most certainly does). Let’s break it down. Hetero / cis refers to the pairing of a cisgender man and a cisgender woman (i.e. two people whose gender identity matches the sex organs they were born with). When two such people partner, we can consider it a hetero cisgender relationship. Normative means that this kind of relationship is what society deems to be the normal or the accepted way of forming partnerships. What this normative aspect means is that our society shuts down pairings or relationships that fall outside this single view. Again, we bump into the problem of traditionally narrow gender and sexual ideas not being broad enough to account for the reality of people’s self-identities.
Perhaps a concrete example would be beneficial here. Young LGBTQ2S+ people who have left home often have few places they can go for support. They may have to resign themselves to using homelessness agencies to meet their basic needs for shelter and food, despite the heterocisnormative cultures that often exist within them (Côté & Blais, 2019). Sometimes the societal privileging of cisgender and heterosexual people is overtly acted upon as LGBTQ2S+ persons may be abused physically, sexually, and mentally within these spaces. At other times, the heterocisnormative violence may be less obvious to those who are not impacted by it. In the video that follows, we see an example of this as the young transgender person seeking support is asked to check a box indicating whether they are male or female and then to proceed to a room in the area designated for people of that biological sex. This act of assuming the person checking a box is cisgender, determining which area they sleep in on the basis of that assumption, and then not offering tailored supports if they resist the cisgender assumptions is just one example of the challenges these young people face in seeking support.
Dr. Alex Abramovich (2016) has written about the cyclical nature of the challenges young LGBTQ2S+ people face when seeking to access supports in heterocisnormative shelter systems. He explains that the lack of LGBTQ2S+ training in the shelter system leaves staff unprepared to intervene in situations of homophobia and transphobia that arise, which then increases homophobia and transphobia in the shelter system, reducing the chances LGBTQ2S+ youths’ needs are met, causing them to avoid the shelter system, meaning shelter staff know even less about these young people, and back to the beginning of the cycle with the lack of LGBTQ2S+ training in the shelter system (Abramovich, 2016). In a subsequent study Dr. Abramovich (2017) triangulated data from interviews, focus groups, observations, and document analysis for 33 LGBTQ2S+ youth and found that the systemic enactment of homophobia, transphobia, and hegemonic / traditional forms of masculinity are often normalized in shelters and create significant barriers to these youth accessing safe and supportive services.
LGBTQ2S+ individuals are discriminated against in many homelessness agencies that are not designed to offer inclusive supports. What do you think it would feel like to be a person who identifies as transgender, is young, and has to seek support from a shelter that is not designed for LGBTQ2S+ persons?
Throughout this section, we often cite research conducted by Dr. Alex Abramovich, whose work has been widely influential in drawing people’s attention to the need for LGBTQ2S+ specific supports, and in advocating for their implementation across Canada. Here we invite you to watch some of his earlier work entitled, “Teal’s Story” which is a digital storytelling project in which Teal shares their experience of navigating hostile shelter environments as a young person who was in the process of transitioning.
Society’s long-held narrow views on gender and sexual identities are prevalent in many homes and within the shelter system. This leaves young LGBTQ2S+ people with few options for support. The longer a young person is without housing, the more trauma they will face related to homelessness and the more difficult it will be to get them securely rehoused. For this reason, early intervention strategies that rapidly move LGBTQ2S+ youth back into housing are critically important. Abramovich and Pang (2020) have noted that despite the high rates of family conflict and estrangement, many of these young people continue to have regular contact with at least one supportive family member. Engaging the families of LGBTQ2S+ youth provides opportunities for reunification or extended family support, but only if it is safe. Dr. Abramovich explains in the next video why getting supportive family engagement is challenging, but also why it has the potential to be life– saving.
In this video, Dr. Alex Abramovich argues that prevention and early intervention of LGBTQ2S+ youth begin with educating and working with families of these young people. He notes the startling statistic that LGBTQ2S+ youth who come from families that reject them are 8 times more likely to attempt suicide than those who receive familial support. Dr. Abramovich states that there are programs and interventions to help the families of these young people better understand, but that they must be willing and open to engage with them. This video is 2:20 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Working with families to support LGBTQ2S+ youth
LGBTQ2S+ youth often have poor mental health. Abramovich and Pang (2020) found in their study that 75% of participants had self-harmed in the past year and that 1 in 3 had attempted suicide in the same time frame. Transgender individuals, in particular, have been found to have higher rates of drug use (Scheim, Bauer, & Shokoohi, 2017) and higher rates of mental and physical comorbidities compared to cisgender individuals (Abramovich, Lam, & Chowdhury, 2020). Clearly these are patterns, but what they point to is structural deficiencies rather than individual failings. When we see these trends – of greater self harm, mental illness, drug use, and suicide – we have to stop and ask why. Why are there higher rates in this population of people? To be clear, these outcomes are not the by-product of people’s gender identities and/or sexual orientations. Rather, it is a response to being continually and systematically shut out of society. Think back to the example of the youth trying to access support at a shelter and facing discrimination. This is just one brief moment of harm among many compounding harms, both large and small.
If people who identify as transgender and in other non-heterocisnormative ways experience high rates of mental illness, substance use, and self-harm – as they do – it is because society creates the conditions for this to occur. What if we stopped? Imagine for a moment that instead of viewing gender and sexual orientation in narrow ways that miss (or obliterate) the experiences of a large proportion of our society, we instead redefined a new normal. How would Canada be a better place to live, a place where we could have pride (yes, again intended) in knowing people have equitable access to the care and support they need no matter how they identify as a person? We encourage you to consider these questions as you watch the next video about Dr. James Makokis, who is an Indigenous two-spirit Doctor who works with transgender youth in Alberta. Before you begin watching, we have two points of note: yes, it is the same Dr. Makokis who was a contestant on The Amazing Race Canada, and more importantly this video discusses suicide and viewers should use discretion in deciding whether watching it is right for them.
It is important to consider not only the need for LGBTQ2S+ supports, but the ways in which they should be tailored to different populations. We have seen this already, in the first section about women’s needs. In much the same way, there are intersecting factors that need to be considered so that we do not put forth a misguided “one size fits all” model. We have seen in the video above that culturally- appropriate supports are beneficial for Indigenous youth. This is key because research has shown that LGBTQ2S+ Indigenous youth are more likely to engage in self-harm, to have seriously considered suicide, or to have attempted suicide (Saewyc et al., 2017). While this study found that 51% of the Indigenous LGBTQ2S+ youth in the study attempted suicide in the preceding year, compared to 22% of heterosexual cisgender Indigenous youth, they also found positive health outcomes amongst LGBTQ2S+ Indigenous youth who were involved in traditional or cultural activities (Saewyc et al., 2017). These findings demonstrate the pressing nature of the issue, while also directing us towards some potential solutions.
Connecting with culturally appropriate supports is an important approach for other groups of LGBTQ2S+ youth as well. For instance, although there are some organizations and spaces, like the Black Queer Youth initiative that are exclusively for Black and queer-identified young people (Benn, 2017), we are lacking a clear understanding of how the combination of being a young person of racial, gender, and sexual minority might interact with experiences of homelessness (Gattis & Larson, 2017). It is essential that we learn more about the experiences of different LGBTQ2S+ youth, such as those who are racialized, in order to offer tailored interventions that meet their needs, as they define them. Notably, in one study of racialized LGBTQ2S+ youth, they spoke about demands placed upon them by support services that they define themselves either as a racial minority or a sexual minority, without recognition of how to support them in being both (McCready, 2017).
Supporting people who identify as LGBTQ2S+ and are experiencing homelessness requires that we understand their intersecting identity markers. We have seen, for instance, how this might include an Indigenous identity and/or a racialized identity. What we also must consider is that not all people who are LGBTQ2S+ and experience homelessness are youth. There are adults and seniors who are gender or sexual minorities and experience homelessness in somewhat similar and somewhat different ways than their youth counterparts. Bardwell (2019) cautions that older LGBTQ2S+ individuals experiencing homelessness also face discrimination, harassment, exclusionary policies, and limited accommodations in shelters, but that we cannot allow the emphasis on youth to render the experiences of these adults invisible.
At this point, we invite you to pause and read about LGBTQ2S+ adult homelessness. Redden et al., (2021) conducted focus groups in five Canadian cities in which participants spoke about their experiences and perceptions of safe, affordable, and affirming housing for older LGBTQ2S+ people. As you read, we encourage you to consider how these experiences are similar or different from what you have learned about youth.
Redden, M., Gahagan, J., Kia, H., Humble, Á. M., Stinchcombe, A., Manning, E., Ecker, J., de Vries, B., Gambold, L. L., Oliver, B., & Thomas, R. (2021). Housing as a determinant of health for older LGBT Canadians: Focus group findings from a national housing study. Housing and Society, 1–25.
In this article, the authors identified many considerations around homelessness for older LGBTQ2S+ persons, such as the lifelong reality and fear of discrimination, need to recognize diversity within this population, operationalize inclusive housing philosophies, address isolation and exclusion, and provide these individuals with access to appropriate housing and supports (Redden et al., 2021). Dr. John Ecker is a co-author on this article and has studied adult LGBTQ2S+ homelessness for several years. In one analysis of 143 articles, his team found that LGBTQ2S+ adults who experience homelessness have unique physical and mental health challenges, in part related to HIV and substance use, and that transgender and non-conforming adults face challenges to their safety in the homelessness system (Ecker, Aubry, & Sylvestre, 2019). There are many structural barriers related to these adults’ homelessness, such as sexual minority wage gaps and exclusion from the labour market (Waite, Ecker, & Ross, 2019). There also exists structural pathways into homelessness for these individuals, related to discrimination and sexual/gender–based victimization, as well as interpersonal pathways often linked to substance use (Ecker, Aubry, & Sylvestre, 2020). When residing in emergency shelters, LGBTQ2S+ adults report engaging in various identity management strategies as a form of protection (Ecker, Aubry, & Sylvestre, 2021). In the video that follows, Dr. John Ecker speaks about his research on adult LGBTQ2S+ homelessness in Canada.
In this video, Dr. John Ecker argues that LGBTQ2S+ young people are a dramatically over-represented group among individuals experiencing homelessness, largely due to homophobia, biphobia, and transphobia within the home. He states that once a young person who identifies as LGBTQ2S+ becomes homeless there are often few services available that are tailored specifically to this group’s needs, and that as a result of discrimination within shelters and agencies, many of these youth will avoid seeking out services. Dr. Ecker further notes that while we have some research on young people, less is known about LGBTQ2S+ adults and seniors experiencing homelessness. There is some preliminary data that suggests these individuals may face discrimination by landlords and employers, prefer LGBTQ2S+ services tailored to adults and seniors, and benefit from community building practices. Dr. Ecker concludes that more research needs to be done on LGBTQ2S+ homelessness, which researchers can undertake by regularly asking questions about gender and sexual orientation and doing so in a way that is informed by diverse categories rather than binaries. This video is 6:19 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: Why is there a high rate of homelessness in the LGBTQ2S+ community?
Dr. Ecker notes that research on gender-identity and sexual orientation is limited because many studies on homelessness do not contain questions that explore these characteristics in depth. This is certainly interesting to consider from a researcher’s perspective, but it also has implications for policy and practice. How do we know what services and supports are needed, if we do not have a keen understanding of the populations themselves? We have seen that there are a range of ways a person can identify their gender and sexual orientation, as well as how these intersect with race, ethnicity, Indigeneity, and age (among arguably many more demographic factors). We have also seen quite clearly that early intervention is key to preventing people from falling into long-term, chronic homelessness and all the harms that brings. Here we must ask ourselves, what can we do to learn more about the diversity of LGBTQ2S+ persons experiencing homelessness, to better tailor our responses? The next video was produced by our partners at the Homeless Hub to help communities better understand how to collect data on who is experiencing homelessness where they live in ways that are inclusive, affirming, and safe for LGBTQ2S+ individuals. Here Dr. Alex Abramovich explains.
Data gathering, whether through research or community counts, is done with the intention of learning more about a population and being able to implement evidence-informed solutions tailored for them. Dr. Abramovich (2018) has written about the intervention components that he has found to be important based on his own research with LGBTQ2S+ youth experiencing homelessness. These include creating policies and standards that are affirming and culturally inclusive of people’s diverse identities. This can be done through mandatory staff training, development of a standardized intake process that accurately reflects people’s diverse identities, creating a welcoming physical environment with representative images in clear view, establishing a formal and safe grievance procedure, developing an integrated approach to mental health services that are trauma-informed, affirming, and accessible, involving youth in planning for their needs, offering programs that recognize the intersectionality of people’s backgrounds, and preventing chronic homelessness by reuniting youth with their families when safe, and rapidly rehousing them elsewhere when not (Abramovich, 2018).
There are many steps that organizations can take to make their services more inclusive for all LGBTQ2S+ persons. There are also some organizations that have emerged exclusively to address the unique needs of this population. In the next video, Dr. Abramovich speaks about the need to advocate for services and how we are beginning to see progress towards the realization of dedicated LGBTQ2S+ transitional housing and support programs in Canada.
In this video, Dr. Alex Abramovich discusses how advocacy can be used to provide government officials with evidence supporting the need for LGBTQ2S+ population-specific programs. He notes that we are starting to see an increase in these types of support services across Canada, citing the opening of two LGBTQ2S+ transitional housing programs for youth in Toronto. Dr. Abramovich says that research shows these population-specific programs are successful and necessary, but that there is still more to learn and work to be done. This video is 1:59 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Transitional housing for LGBTQ2S youth
The YMCA Sprott House opened in February 2016, as Canada’s first transitional housing program with 25 beds for LGBTQ2S+ youth between the ages of 16 and 24 (Abramovich & Kimura, 2019). The goal of the program is to create a safe and affirming space for these youth while also supporting them as they increase their independence and ability to find affordable and stable housing of their own within the community (Abramovich & Kimura, 2019). Reflecting on their time living at YMCA Sprott House, Morgan has written, “I’ve been able to do some soul-searching through feeling comfortable enough in a positive space to reflect and grow as a person. It has helped me to become true to myself by being around those who are accepting of my identity – staff and youth. The fact that the staff at Sprott House aren’t cis and straight has made such a difference for me. I’ve been able to see positive examples of trans men and non-binary people, and positive examples of masculinity in general” (Miller, Bissoondial, & Morgan, 2017, pg. 179).
An evaluation of the YMCA Sprott House has similarly found that the young residents feel safer, gain exposure to staff and other residents who help to normalize gender and sexually diverse identities, explore their true and authentic selves, and move forward with an improved sense of mental wellness (Abramovich & Kimura, 2019). Notably one of the biggest challenges is the time restriction, which is needed to open spaces for more youth but can also serve as a ticking clock for those who are already residing there (Miller et al., 2017). Fortunately, there have been developments with new LGBTQ2S+ programs, including additional transitional housing, opening since the Sprott House. Programs that help LGBTQ2S+ youth are life- saving but they in themselves are not enough – they must be part of a comprehensive strategy that is coordinated and seeks to prevent homelessness before it occurs (Abramovich & Shelton, 2017a). These efforts must be considered not as a piecemeal assemblage of services located across the country, but rather as a systems-wide approach with governmental funding and support (French, 2017).

Visit the 519 website for a complete set of LGBTQ2S+ youth homelessness in Canada infographics that you can print and post for others to read.

If you want to learn more about homelessness among women and gender diverse people, sign up for this free online Homelessness Learning Hub training course that contains six lessons and gives a certificate of completion to those who complete them successfully.
The rates of homelessness are high for people who identify as LGBTQ2S+ in Canada, and we have asked you to consider why this occurs. We have seen estimates that 20-40% of youth who experience homelessness are amongst this population, which largely results from familial rejection of their gender and/or sexual identity. There are certainly many pathways into homelessness for these youth, such as related to child welfare involvement and institutional discrimination, but family conflict remains a pressing factor. We saw that limited notions of gender and sexuality within our society shape the discriminatory responses these individuals face in their homes and across society. This results from heterocisnormativity, which the word processor still does not understand (cue the red squiggles) but by now we hope has become clearer to you. Recall the experience of Teal who sought help from an emergency shelter only to be forced back into a gender identity that was not authentic and a physical environment that was outwardly hostile.
We learned that people who identify as LGBTQ2S+ have higher rates of mental illness, substance use, self-harm, and suicide. This is not because of their gender or sexual orientation, but rather because society prevents them from being able to freely express it. Recall the video of the Indigenous youth who attempted suicide and the depth of impact receiving treatment from someone who understood had on their well-being. People who identify as LGBTQ2S+ have many intersecting identities. Indigenous identity, being a racialized person, and/or being an adult or senior are just some of the identities that overlap with gender and sexual identity, and that need tailored responses.
We may be reluctant to ask questions about people’s gender and sexual identities, but by not doing so we miss the opportunity to gain a deeper understanding. It is possible to conduct research and engage in counts in ways that are inclusive, safe, and respectful of people’s diverse and intersecting identities. This information is critical for helping us design and implement programs that meet people’s unique needs. Tailored supports, like the YMCA Sprott House, are critically important but we must also realize that real change will take dedication, effort, and a coordinated approach that reflects commitment to inclusive change across the country.
Click the link below to listen to all of the researchers answer the question “Why is there a high rate of homelessness in the LGBTQ2S+ community?” in audio format on our podcast!
63
Shruti and Mia
At the beginning of this chapter, we introduced you to Shruti, a 23-year-old female who moved to Canada from the US and became trapped in sex trafficking, and Mia, a 17-year-old transgender woman fleeing an abusive relationship.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1184#h5p-87
64
We began this chapter on Gender & Queer Studies with a story about a hotel door hanger that can be used to ask for privacy, with pearls on one side and a tie on the other. We used this to set the stage for our discussion about the complexity of gender and sexual identities that cannot be adequately captured or expressed in an object with only two sides.
At the start of the chapter, we introduced you to the composite characters Shruti and Mia, who were each experiencing homelessness in their own unique way. The scenarios were presented as an entry point into thinking about the complexity of homelessness. We returned to these individuals’ stories again at the end to demonstrate how they can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada
We asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “What is unique about the experience of homelessness for women?” Here we considered the experience of cisgender women, transgender women, and gender diverse individuals. We saw that they often try to remain hidden as a means of protection and seek emergency supports only when other options run out. They are often the victims of gender-based violence and experience considerable trauma throughout their lives. When women experience homelessness, they often do so within the context of mothering as either active caregivers or in grief over having their children removed from their custody. Cisgender women also have to navigate reproductive issues, such as pregnancy or menstruation.
Next we asked, “Do men and women have different needs, when experiencing homelessness?” This question had both a simple and more complex response. On the one hand, the fundamental needs are the same. Everyone needs safe housing, good health care, a livable income, and to feel included. How these needs are expressed and obtained are what differ between men, women, and gender diverse individuals. We saw this emerge through quality of life studies that identified different factors that contributed to well-being for women and for men. Gender expression is complex, and we considered how notions of traditional masculinity are both challenged and reproduced on the streets.
Finally, we asked, “Why is there a high rate of homelessness in the LGBTQ2S+ community?” We began this section by considering the term itself and learning that 20-40% of youth experiencing homelessness are estimated to identify this way. These young people may have multiple pathways to the street, but identity-based family conflict is a primary reason this rate is so high. Prevailing notions of heterocisnormativity can be found in many homes, as well as in homelessness sector agencies. These youth face high rates of discrimination and consequently have poor mental health and high rates of substance use, self-harm, and suicide. Supporting these individuals requires tailored supports that are safe, inclusive, and reflective of their intersecting identities. We must also remember that while there are many young people who experience homelessness and identify as LGBTQ2S+, there are also many adults and seniors in this population who are discriminated against and under-served as well. Efforts towards creating LGBTQ2S+ services, like the YMCA Sprott House, are encouraging but need to be part of a coordinated effort to create widespread and sustained change.
65
Here are some additional resources you may want to check out!
66
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
67
Abramovich, A. (2016). Preventing, reducing and ending LGBTQ2S youth homelessness: The need for targeted strategies. Social Inclusion, 4 (4).
Abramovich, A. (2017). Understanding how policy and culture create oppressive conditions for LGBTQ2S youth in the shelter system. Journal of Homosexuality, 64(11), 1484–1501. https://doi.org/10.1080/00918369.2016.1244449
Abramovich, A. (2018). Responding to the needs of LGBTQ2S youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Abramovich, A., Lam, J. S. H., & Chowdhury, M. (2020). A transgender refugee woman experiencing posttraumatic stress disorder symptoms and homelessness. Canadian Medical Association Journal (CMAJ), 192(1), E9–E11. https://pubmed.ncbi.nlm.nih.gov/31907229/
Abramovich, A., & Pang, N. (2020) Understanding LGBTQ2S youth homelessness in York Region. Toronto, ON. Report LGBTQ2S Youth in York Region
Abramovich, A., & Shelton, J. (2017a). Conclusion: The way forward. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Abramovich, A., & Shelton, J. (2017b). Introduction: Where are we now?. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Andermann, A., Mott, S., Mathew, C. M., Kendall, C., Mendonca, O., Harriott, D., … Pottie, K. (2021). Evidence-informed interventions and best practices for supporting women experiencing or at risk of homelessness: a scoping review with gender and equity analysis. Health Promotion and Chronic Disease Prevention in Canada, 41(1), 1–13. https://doi.org/10.24095/hpcdp.41.1.01
Bani-Fatemi, A., Malta, M., Noble, A., Wang, W., Rajakulendran, T., Kahan, D., & Stergiopoulos, V. (2020). Supporting female survivors of gender-based violence experiencing homelessness: Outcomes of a health promotion psychoeducation group intervention. Frontiers in Psychiatry, 11, 601540–601540. 10.3389/fpsyt.2020.601540
Bardwell, G. (2019). The impact of risk environments on LGBTQ2S adults experiencing homelessness in a midsized Canadian city. Journal of Gay & Lesbian Social Services, 31(1), 53-64. https://doi.org/10.1080/10538720.2019.1548327
Barrow, S. K. (2018). Scholarship review of queer youth homelessness in Canada and the United States. The American Review of Canadian Studies, 48(4), 415–431. https://doi.org/10.1080/02722011.2018.1531603
Benbow, S., Forchuk, C., Berman, H., Gorlick, C., & Ward-Griffin, C. (2019a). Mothering without a home: Internalized impacts of social exclusion. Canadian Journal of Nursing Research, 51(2), 105–115. https://doi.org/10.1177/0844562118818948
Benbow, S., Forchuk, C., Berman, H., Gorlick, C., & Ward-Griffin, C. (2019b). Spaces of exclusion: Safety, stigma, and surveillance of mothers experiencing homelessness. Canadian Journal of Nursing Research, 51(3), 202–213. https://doi.org/10.1177/0844562119859138
Benbow, S., Forchuk, C., Gorlick, C., Berman, H., & Ward-Griffin, C. (2019c). “Until You hit rock bottom there’s no support”: Contradictory sources and systems of support for mothers experiencing homelessness in southwestern Ontario. Canadian Journal of Nursing Research, 51(3), 179–190. https://doi.org/10.1177/0844562119840910
Benn, A. (2017). The Black queer youth initiative: Challenging racism, stigma & exclusion. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Buccieri, K., Oudshoorn, A., Waegemakers Schiff, J., Pauly, B., Schiff, R., & Gaetz, S. (2020). Quality of life and mental well-being: A gendered analysis of persons experiencing homelessness in Canada. Community Mental Health Journal, 56(8), 1496–1503. 10.1007/s10597-020-00596-6
COH and Blue Door. (2021). The future of men’s supportive housing in York Region: An exploratory study. Ontario: Canadian Observatory on Homelessness and Blue Door. Blue Door Executive Summary
Côté, P. B., & Blais, M. (2019). Between resignation, resistance and recognition: A qualitative analysis of LGBTQ+ youth profiles of homelessness agencies utilization. Children and Youth Services Review, 100, 437–443. https://doi.org/10.1016/j.childyouth.2019.03.024
Côté, P. B., & Blais, M. (2021). “The least loved, that’s what I was”: A qualitative analysis of the pathways to homelessness by LGBTQ+ youth. Journal of Gay & Lesbian Social Services, 33(2), 137-156. https://doi.org/10.1080/10538720.2020.1850388
Ecker, J., Aubry, T., & Sylvestre, J. (2019). A review of the literature on LGBTQ adults who experience homelessness. Journal of Homosexuality, 66, 297-323. https://doi.org/10.1080/00918369.2017.1413277
Ecker, J., Aubry, T., & Sylvestre, J. (2020). Pathways into homelessness among LGBTQ2S adults. Journal of Homosexuality, 67(11), 1625–1643. https://doi.org/10.1080/00918369.2019.1600902
Ecker, J., Aubry, T., & Sylvestre, J. (2021). Experiences of LGBTQ adults who have accessed emergency shelters in a large urban city in Canada. Social Work in Public Health. https://doi.org/10.1080/19371918.2021.1976345
Flynn, C., Damant, D., Lapierre, S., Lessard, G., Gagnon, C., Couturier, V., & Couturier, P. (2018). When structural violences create a context that facilitates sexual assault and intimate partner violence against street-involved young women. Women’s Studies International Forum, 68, 94–103. https://doi.org/10.1016/j.wsif.2018.01.004
French, D. (2017). A Provincial response to LGBTQ2S youth homelessness. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Gattis, M., & Larson, A. (2017). Discrimination & mental health outcomes of Black youth experiencing homelessness. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Gentil, L., Grenier, G., Bamvita, J. M., Dorvil, H., & Fleury, M. J. (2019). Profiles of quality of life in a homeless population. Frontiers in Psychiatry, 10, 10. https://doi.org/10.3389/fpsyt.2019.00010
Government of Canada. (2017). A place to call home: Canada’s national housing strategy. Government of Canada, Ottawa. Canada’s National Housing Strategy (placetocallhome.ca)
Government of Canada. (2019). National housing strategy act. Government of Canada, Ottawa. National Housing Strategy Act (justice.gc.ca)
Kahan, D., Lamanna, D., Rajakulendran, T., Noble, A., & Stergiopoulos, V. (2020). Implementing a trauma‐informed intervention for homeless female survivors of gender‐based violence: Lessons learned in a large Canadian urban centre. Health & Social Care in the Community, 28(3), 823–832. https://doi.org/10.1111/hsc.12913
Kennelly, J. (2020). Urban masculinity, contested spaces, and classed subcultures: young homeless men navigating downtown Ottawa, Canada. Gender, Place and Culture: A Journal of Feminist Geography, 27(2), 281–300. https://doi.org/10.1080/0966369X.2019.1650724
Koch, J., Scherer, J., & Holt, N. (2018). Slap shot! Sport, masculinities, and homelessness in the downtown core of a divided western Canadian inner city. Journal of Sport and Social Issues, 42(4), 270–294. https://doi.org/10.1177/0193723518773280
Kitson, C., & O’Byrne, P. (2020). The experience of violence against women who use injection drugs: An exploratory qualitative study. Canadian Journal of Nursing Research, 340-352. https://doi.org/10.1177/0844562120979577
McCready, L. T. (2017). Black queer youth, unstable housing and homelessness: Understanding the impact of family conflict, school and community-based violence on racialized LGBTQ2S youth. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Merdsoy, L., Lambert, S., & Sherman, J. (2020). Perceptions, needs and preferences of chronic disease self‐management support among men experiencing homelessness in Montreal. Health Expectations: An International Journal of Public Participation in Health Care and Health Policy, 23(6), 1420–1430. https://doi.org/10.1111/hex.13106
Meyer, J. P., Isaacs, K., El-Shahawy, O., Burlew, A. K., & Wechsberg, W. (2019). Research on women with substance use disorders: Reviewing progress and developing a research and implementation roadmap. Drug and Alcohol Dependence, 197, 158–163. https://doi.org/10.1016/j.drugalcdep.2019.01.017
Milaney, K., Williams, N., Lockerbie, S. L., Dutton, D. J., & Hyshka, E. (2020). Recognizing and responding to women experiencing homelessness with gendered and trauma-informed care. BMC Public Health, 20(1), 397–397. https://doi.org/10.1186/s12889-020-8353-1
Miller, K., Bissoondial, K., & Morgan. (2017). YMCA Sprott House: Creating a better space for LGBTQ2S youth in Toronto. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Murnan, A., Zhang, J., & Slesnick, N. (2018). Ecologically based treatment for mothers experiencing homelessness who have children in their care. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Oudshoorn, A., May, K., Van Berkum, A., Schwan, K., Nelson, A., Eiboff, F., K., Begun, S., Nichols, N., & Parsons, C. (2021). Exploring the presence of gender-based approaches to women’s homelessness in Canadian communities. Gender Based Approaches Report
Redden, M., Gahagan, J., Kia, H., Humble, Á. M., Stinchcombe, A., Manning, E., … Thomas, R. (2021). Housing as a determinant of health for older LGBT Canadians: Focus group findings from a national housing study. Housing and Society, 1–25. https://doi.org/10.1080/08882746.2021.1905996
Reid, N., Kron, A., Rajakulendran, T., Kahan, D., Noble, A., & Stergiopoulos, V. (2020). Promoting wellness and recovery of young women experiencing gender-based violence and homelessness: The role of trauma-informed health promotion interventions. Violence Against Women, 27(9). https://doi.org/10.1177/1077801220923748
Saewyc, E., Mounsey, B., Tourand, J., Brunanski, D., Kirk, D., McNeil-Seymour, J., Shaughnessy, K., Tsuruda, S., & Clark, N. (2017). Homeless & street-involved Indigenous LGBTQ2S youth in British Columbia: Intersectionality, challenges, resilience & cues for action. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Saewyc, E. M., Shankar, S., Pearce, L. A., & Smith, A. (2021). Challenging the stereotypes: unexpected features of sexual exploitation among homeless and street-involved boys in western Canada. International Journal of Environmental Research and Public Health, 18(11), 5898–. https://doi.org/10.3390/ijerph18115898
Scheim, A. I., Bauer, G. R., & Shokoohi, M. (2017). Drug use among transgender people in Ontario, Canada: Disparities and associations with social exclusion. Addictive Behaviors, 72, 151–158. https://doi.org/10.1016/j.addbeh.2017.03.022
Schwan, K., Vaccaro, M. E., Reid, L., & Ali, N. (2021a). Implementation of the right to housing for women, girls, and gender diverse people in Canada. Canada: The National Right to Housing Network. Microsoft Word – EN_CHRC_13.docx (housingrights.ca)
Schwan, K., Vaccaro, M., Reid, L., Ali, N., & Baig, K. (2021b). The pan-Canadian women’s housing & homelessness survey. Toronto, ON: Canadian Observatory on Homelessness. Pan-Canadian-Womens-Housing-Homelessness-Survey
Van Berkum, A., & Oudshoorn, A. (2019). “Where to now?” Understanding the landscape of health and social services for homeless women in London, Ontario, Canada. Journal of Social Inclusion, 10(1), 41. https://doi.org/10.36251/josi.158
Voisard, B., Whitley, R., Latimer, E., Looper, K., & Laliberté, V. (2021). Insights from homeless men about PRISM, an innovative shelter-based mental health service. PloS One, 16(4), e0250341–e0250341. https://doi.org/10.1371/journal.pone.0250341
Waite, S., Ecker, J., & Ross, L. E. (2019). A systematic review and thematic synthesis of Canada’s LGBTQ2S+ employment, labour market and earnings literature. PloS One, 14(10), e0223372–e0223372. https://doi.org/10.1371/journal.pone.0223372
Wardhaugh, J. (1999). The unaccommodated woman: Home, homelessness and identity. The Sociological Review, 47(1): 91-109. https://doi.org/10.1111/1467-954X.00164
Wheeler, C., Price, C., & Ellasante, I. (2017). Pathways into and out of homelessness for LGBTQ2S youth. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Yakubovich, A. R., & Maki, K. (2021). Preventing gender-based homelessness in Canada during the COVID-19 pandemic and beyond: The need to account for violence against women. Violence Against Women, 1-13. DOI: 10.1177/10778012211034202
VII
In all societies there are rites of passage that mark the passing of time. Leaving one’s family of origin and claiming independence is one such marker. Commonly we may think of a young person leaving their parents’ home because they are entering college or university, they have rented or purchased a place of their own, and/or because they have started their own family through marriage or the birth of a child. When a young person leaves their home under these circumstances they are celebrated, even if met with mixed emotions. Yet, there are many young people who leave home under very different – and not celebratory – circumstances.
Consider for instance a young person who leaves an abusive or oppressive household, a young person who feels unwelcome in their home due to their sexual orientation or gender expression, or a young person who struggles with emotional or cognitive disabilities and does not receive the support they need to succeed in traditional educational settings. These young people may all leave home out of necessity or be pushed out by family who does not accept them. When they leave home, they are not met with the same celebration as those who leave for socially approved reasons. Rather, they are left without vital support networks to help them navigate education, housing, and employment on their own. Finding stability without these supports is a long and uphill battle.
68
In this chapter, you are invited to learn and think critically about the experience of being both young and homeless in Canada. While considering homelessness as an issue that impacts young persons, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that young people who become homeless rarely do so unless it is a necessity. The decision to leave home – or being asked to leave home – is a traumatic life circumstance for any young person to go through. Just as leaving one’s home is often a process rather than a single event, so too does permanently exiting homelessness take time to achieve. Read on to learn more about the reasons some youth become homeless, the challenges these young people face, the remarkable strength it takes to achieve long-term stability, and what we as a society can do to better support these young people before homelessness occurs.
69
We begin this chapter by presenting three composite scenarios that reflect real-world experiences of homelessness in Canada, as they pertain to Child and Youth Studies. As you work through these scenarios, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenarios, and a critical perspective, to think about how the scenarios represent larger issues impacting people in our society.
After considering the real-world scenarios, we will endeavour to answer each question posed in the learning objectives. Why do some young people become homeless? What are the challenges these young people face? How can young people be supported to exit homelessness permanently? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenarios presented at the beginning and reconsider them in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
70
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with these real life composite scenarios. Take a moment here to pause and consider these people’s experiences.
Enzo
Enzo is a 14-year-old male who is currently staying at the youth shelter. He was kicked out of his parents’ house again for hanging out with friends from the neighbourhood who his parents believe are local gang members. He has been lying, breaking curfew, stealing his mother’s prescription drugs, and has had a number of minor interactions with the local police. His parents have said they will not take him back this time. His parents feel that he needs to learn about how “good he has had it at home” by being forced to “fend for himself.” He feels they are overly strict, “lame,” and embarrassing to be seen with. He left thinking any place would be better than his family home. At the shelter he is disrespectful to the workers, bullying to the other residents and withdrawn when not engaged in altercations. He has been warned that his behaviour will lead to being removed from the shelter, leaving him with few options left.
Jake
Jake is a 19-year-old youth who has been on and off of the streets since he was 16 years old. He left his family home following abuse by his stepfather and indifference shown by his mother. He accessed the adult shelter in his local town five to six times over two years. He is known about town as somewhat of a trouble-maker and local police have followed his activities fairly closely. He would start a job and then be picked on by local youths and end up missing shifts and being fired. He has left the shelter various times over the years as he was victimized by other residents. Recently his support workers have found him an affordable place to live. His new apartment is small and is in a town 10 kilometers away from his home town. He has connected with a local Art Hive where he spends his time embracing his love of creativity through painting. He has also connected with the local community group and attends weekly dinners and other events. He is starting to feel as though he belongs to the community and has begun volunteering with the agency that hosts the dinners. He is hoping to take high school classes through the local alternative program in the fall. He is beginning to have hope.
Miriam
Miriam is a six-year-old student at a local elementary school. She started at the school this fall and has had spotty attendance. She is a very quiet and painfully shy child who does not run on the playground or get involved in the high-energy events of the day. She often comes to school in obviously soiled clothing and without a lunch. The teacher is aware that her family are recent immigrants from Ghana. Miriam’s mother indicates that the transition has been fine. She has had a few challenges with the washing facilities at their apartment building and Miriam is forgetful in her hurry to get to school on time. She declines a meeting with the Social Worker. From the small amount of information that Miriam shares reluctantly the teacher is beginning to think that the family may be living in their car.
With these scenarios fresh in your mind, consider the following reflection questions. You may wish to record your answers before moving on to the next section. We will return to the scenarios again at the end of the chapter.
Reflection Questions
71
The reasons why people experience homelessness are always complicated. For adults, homelessness often results from one or more factors such as mental illness, addictions, unemployment, and/or disability. When we think about what contributes to youth homelessness, however, we see that there are very different causes. While young people may also experience mental illness, addictions, a lack of employment, and/or disability, these are not the factors that we commonly point to in order to explain why they lose their housing. One key difference between adults and youth is the ownership and control of property. Whereas adults may lose housing they own or rent due to these factors, young people often flee or are pushed out of housing controlled by adults in their lives, such as their parents.
When young people are visibly living on the street, we may hear people ask why they do not just return home. While this question may be asked with good intentions, it assumes that the home was a good place to live, and the youth is at fault for leaving it. We know from the research that the homelives of young people who become homeless are often challenging, but that these experiences also must be located within broader social and structural contexts. Throughout this section, we will consider the interpersonal, structural, and systemic causes of youth homelessness. Before you continue through the material, we invite you now to take a moment and record your own thoughts on why some young people become homeless.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=731#h5p-106
One day in the summer of 2005, one of the authors of this book was volunteering at an urban drop-in centre for young people experiencing homelessness. There was a local television station located around the corner, that would donate the left-over craft services spread (such as donuts and muffins) after the morning broadcast. As she walked the two blocks to pick up the donation, people along the way nodded and said hello to this smiling clean-cut woman in her early 20s. On her way back, she ran into a young man who frequented the drop-in centre and he accompanied her back (eager to get first dibs on the donuts). This man was also in his early 20s but was severely malnourished from an intravenous drug addiction, slept outside in a rock garden under a nearby bridge, and had not bathed for several weeks, if not months. Along the way, an interesting thing happened. Where people had been smiling at her on the way to get the food, now beside this young man, they would not meet her eye. People shuffled past, noticeably clutching their bags and possessions close to their bodies. When one or two did meet her eye, it was only to silently project the message “I know you’re in trouble, but I’m not stepping in to help you.”
The thing was, she was not in trouble. She was actually having a rather pleasant conversation with this man whom she had come to know fairly well. Yet, what people saw – what they focused on – was the malnourishment, the results of the addiction, the dishevelled clothing, and the smell of sweat and grime that comes from not bathing in the summer. The reasons young people become homeless are generally not well understood in society. As a result of this, these youth frequently face stigma and discrimination. Often they are viewed as individuals to be feared. However, to understand the complexity of youth homelessness we must look beyond the clothing and hygiene. We begin this section with videos of Dr. Kaitlin Schwan and Dr. David Firang each respectively explaining why it is essential we locate the individual within broader social and structural contexts, to grasp why some young people become homeless.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Kaitlin Schwan argues that we can use the image of a pie chart to think about the three main factors that contribute to youth experiencing homelessness. First, structural causes are the societal pieces that create conditions of inequity and discrimination in society. Second, systemic causes are related to policy failings, such as the lack of transitional planning from public systems. Finally, interpersonal causes are underpinned by the preceding causes and relate to a young person’s own experiences in their home and community. Dr. Schwan notes that young people who come from wealthier backgrounds often have more access to supports and resources to prevent homelessness, in the event they have a crisis and/or lose their housing. This video is 3:07 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: Why do some young people become homeless?
In this video, Dr. David Firang argues that young people do not have to become homeless but in our society some people will experience poverty and homelessness based on life circumstances. He explains that we need to consider this issue from a ‘person in environment’ perspective which entails the micro environment of the family one is born into, the mezzo environment of the neighbourhood one is raised in, and the macro environment of societal policies, cultures, values, and norms. Dr. Firang concludes that people do not choose to be homeless but rather, through their environments, society pushes them to become homeless. This video is 3:40 in length and has closed captions available in English.
Key Takeaways – Dr. David Firang: Why do some young people become homeless?
Despite using different terms, Dr. Schwan and Dr. Firang both explain that youth homelessness is not about individual choices but rather is the product of intersecting domains. We must consider the role of relationships within the family and, more broadly, within the community – this is the interpersonal or micro domain. We must consider issues of equity and whether these young people have opportunities in their lives – this is the structural or mezzo domain. Finally, we must consider how society and public institutions function (or fail to function) is ways that support young people – this is what we call the systemic or macro domain. What the people on the street saw, in the story above, was a disheveled young man. What they failed to see was the interpersonal struggles within his home and community, the inequity within society that resulted in limited opportunities, and the systemic failures that did not provide a safety net and prevent his homelessness from occurring. In the next video Dr. Sean Kidd explains that youth homelessness is not a binary experience (of being homeless or not), but that it is often a process and regardless of why a young person is on the streets, we must consider them a person in need of support.
In this video, Dr. Sean Kidd explains that there is a range of reasons young people experience homelessness in high-income countries, like Canada. Notably, they may have faced adversity or abuse in the home, their family may be experiencing economic crisis, they may be discriminated against in public institutions, such as criminal justice and child welfare systems, and they may have been bullied or under-accommodated in school. Dr. Kidd clarifies that youth homelessness is not a binary experience, but rather a trajectory of episodes that become longer and more frequent over time. He notes that some young people are pushed out of their homes because of economic hardship or their family’s rejection of their gender or sexual identity. Dr. Kidd argues that a minority of young people experience homelessness because of bad choices they have made but that, regardless of the reasons, once a young person is unhoused they are at risk of victimization, poor physical and mental health, and premature death, making them a young person in need of support. This video is 5:43 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: Why do some young people become homeless?
In the Introduction chapter we reviewed the Canadian Definition of Homelessness. A separate document, also led by the Canadian Observatory on Homelessness (2016), was created to define the unique experience of youth homelessness. It states:
“Youth homelessness refers to the situation and experience of young people between the ages of 13 and 24 who are living independently of parents and/or caregivers, but do not have the means or ability to acquire a stable, safe, or consistent residence. Youth homelessness is a complex social issue because as a society we have failed to provide young people and their families with the necessary and adequate supports that will enable them to move forward with their lives in a safe and planned way. In addition to experiencing economic deprivation and a lack of secure housing, many young people who are homeless lack the personal experience of living independently and at the same time may be in the throes of significant developmental (social, physical, emotional, and cognitive) changes. As a result, they may not have the resources, resilience, education, social supports or life skills necessary to foster a safe and nurturing transition to adulthood and independence. Few young people choose to be homeless, nor wish to be defined by their homelessness, and the experience is generally negative and stressful. Youth homelessness is the denial of basic human rights and once identified as such, it must be remedied. All young people have the right to the essentials of life, including adequate housing, food, safety, education, and justice” (COH, 2016, pg.1).
You can read the full Canadian Definition of Youth Homelessness here:
The reasons some young people become homeless, while others do not, is largely an outcome of these three intersecting factors – the interpersonal, structural, and systemic domains. As Dr. Kidd explained, and as we will hear repeated throughout this section, there is no single reason young people become homeless but rather it is the result of multiple factors. These young people often have cumulative shorter episodes, where they leave or are thrown out for a brief time before returning home again. They may stay in an emergency shelter, but also commonly couch-surf and reside with friends or extended family. These episodes grow longer and more frequent, leading to longer-term youth homelessness. In the next video, current and former residents of “Youth Without Shelter,” an emergency shelter for young people in the Greater Toronto Area, speak about the reasons why they became homeless. As you watch this video, we encourage you to look beyond individual factors and listen for the interpersonal, structural, and systemic factors that emerge in their narratives.
We have noted that there are three levels or domains that contribute to youth homelessness, often in overlapping and intersecting ways. As we take a closer look at each of these three domains, we ask that you pay careful attention to the ways they interact with one another. We begin here with the interpersonal factors that contribute to youth homelessness, by showcasing segments in which researchers discuss family and community relationships. However, while the videos we show here all touch on interpersonal issues, the domains are so interconnected that you will also hear them speak about structural and systemic issues as well. We cannot – nor would not want to – tease these issues apart and present them solely in isolation. In fact, it is their intertwined nature that is what gives rise to youth homelessness. In the next set of videos, Dr. Naomi Thulien, Dr. Tyler Frederick, and Dr. Jeff Karabanow each explain further.
In this video, Dr. Naomi Thulien explains that youth homelessness is nearly always related to some sort of family dysfunction, such as physical, sexual, and/or emotional abuse. She notes that it is also often related to child welfare involvement, such as monitoring in the home or removal and placement into foster care or group homes. This video is 0:39 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: Why do some young people become homeless?
In this video, Dr. Tyler Frederick explains that there are many different reasons young people become homeless but that histories of abuse and parental conflict within the home are common. He notes that exiting the child welfare system without transitional planning is also a recognized pathway for many young people. Dr. Frederick concludes that youth homelessness is rarely the result of a single event, but rather is the culmination of multiple stressors that occur over time within complex home environments. This video is 2:56 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: Why do some young people become homeless?
In this video, Dr. Jeff Karabanow identifies three core interrelated dynamics that contribute to youth homelessness. First, there may be deep family dysfunction such as addictions, mental illness, or parental lack of acceptance of one’s sexual orientation that makes the home an unsafe environment. Second, young people may experience deep abuse within their family systems, including physical, emotional, spiritual, and psychological traumas. Third, youth may come from family units struggling for basic survival while living in deep poverty. Dr. Karabanow notes that when young people leave home it is a rational and deliberate process, where they consider how they will get through a situation, think deeply about it, and weigh their options. He concludes that these young people do not want to be homeless but rather leave complicated and dangerous situations. This video is 4:06 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: Why do some young people become homeless?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=731#h5p-107
Family conflict is a key driver within the interpersonal domain. Young people may be living in abusive environments, struggling to complete school or other obligations (often as the result of undiagnosed learning disorders and/or mental illness), and may be using substances in problematic ways. Conflict within the family may occur with parents or even with siblings, if they are perceived to be getting preferential treatment (Buccieri, 2019). Young people who identify as lesbian, gay, bisexual, transgender, queer or questioning, or two-spirit [LGBTQ2S+] may also face identity-based conflict within their families and communities that can contribute to homelessness, often in complex and non-linear ways (Barrow, 2018). For instance, in a study of LGBTQ2S+ youth homelessness in the Toronto region, Abramovich and Pang (2020) found that on average these young people left home at age 18, but that 28% had left when they were 16 or younger. In the next two videos, Dr. Jacqueline Kennelly and Dr. Alex Abramovich speak about how the intersection of interpersonal and other factors contribute to LGBTQ2S+ youth homelessness. To learn more about LGBTQ2S+ individuals’ experiences of homelessness, we also encourage you to read the chapter on Gender & Queer Studies.
In this video, Dr. Jacqueline Kennelly explains that while every pathway into homelessness is unique, there are common factors such as poverty and the lack of affordable housing. She notes that middle class and more affluent youth may experience homelessness because of stress and mental health challenges within the family. Dr. Kennelly concludes by noting that LGBTQ2S+ youth are amongst the highest risk group for youth homelessness. This video is 2:00 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Why do some young people become homeless?
In this video, Dr. Alex Abramovich explains that the primary cause of youth homelessness is family conflict, and for LGBTQ2S+ youth this is often related to identity-based conflict and discrimination. He notes that there are other reasons youth experience homelessness as well, such as institutional discharges, unstable and insufficient employment, poverty, and racism. This video is 1:16 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Why do some young people become homeless?
We presented the series of videos above to highlight the interpersonal domain that contributes to youth homelessness, yet at the same time noted they also demonstrate intersections between structural and systemic levels as well. We can see, for instance, that interpersonal conflict within families may be the result of a young person’s struggles in schools. However, if the struggles result from an undiagnosed learning disorder or mental illness, there are structural and systemic failures involved. We can also see how conflict over a young person’s gender or sexual identity may intersect with structural conditions, such as racism and discrimination, and may result from inadequate social supports within society.
Structural or macro factors that contribute to homelessness are rooted in the ways our society functions and the relations that develop as a result. If our society was equitable, each person would have what they need to be well. However, the large number of young people experiencing homelessness across the country tells us quite clearly that not all young people are getting what they need. This is not only the product of their home environments, but rather an outcome of structural factors inherent in the way our society operates. When we see patterns arise, we have to question why. In the next video, Dr. Stephen Gaetz identifies some patterns that arise in the reasons some youth become homeless and situates these within the structure of our society.
In this video, Dr. Stephen Gaetz notes that the causes and conditions of youth homelessness are different than adults because most young people become homeless without having been in charge of their own housing. He explains that while each person will have their own experience, the research shows high rates of family conflict and abuse. Dr. Gaetz indicates that 40% of youth who are currently homeless had their first episode before the age of 16, which makes them more likely to have had adverse childhood experiences, histories of housing instability, and experiences of bullying at school. Dr. Gaetz argues that to answer the question of why youth become homeless we have to say it is because society allows them to become homeless rather than putting supports in place to help young people and their families. Dr. Gaetz concludes that it is a horrible statement about our society that we allow youth homelessness to occur. This video is 3:17 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: Why do some young people become homeless?
Dr. Gaetz explains that young people become homeless because society fails to stop it from happening. The Canadian definition of youth homelessness establishes that youth homelessness is the denial of basic human rights and that once it is identified as such, it must be remedied (COH, 2016). In the Introduction chapter, we considered the question of why prevention matters. For youth, as for adults, preventing homelessness from occurring would mean that people do not have to experience the traumas that go along with it. As youth homelessness is society’s problem, borne of structural inequities, it is society’s obligation to fix.
Our society’s current response to youth homelessness is primarily emergency-based and implemented after a person is already in crisis and experiencing homelessness (Gaetz, O’Grady, Kidd, & Schwan, 2016). As a way to reframe society’s approach, Gaetz, Schwan, Redman, French, and Dej (2018) have created a roadmap for the prevention of youth homelessness. We invite you now to familiarize yourself with this roadmap as this section’s featured reading. First, we present an infographic, created by the Canadian Observatory on Homelessness and A Way Home Canada, that highlights the six key aspects and how they can be realized. We then present the Executive Summary as the featured reading below (although we encourage you to use the links within the document to read the report in its entirety to learn even more).
Click the image below to open a new window and view the full infographic “The Roadmap for the Prevention of YOUTH HOMELESSNESS” on the Homeless Hub.
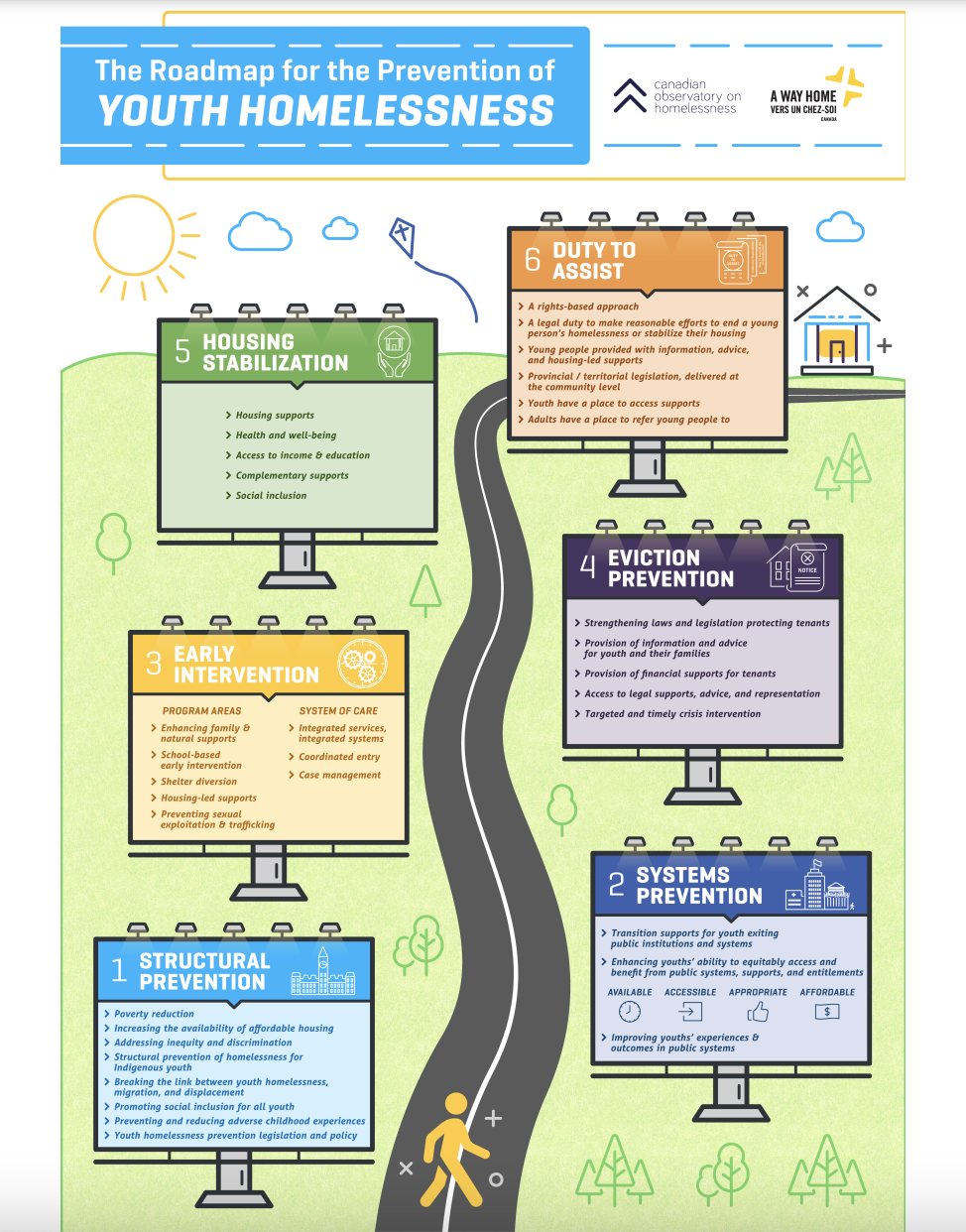
Gaetz, S., Schwan, K., Redman, M., French, D., & Dej, E. (2018). The Roadmap for the Prevention of Youth Homelessness – Executive Summary. A. Buchnea (Ed.). Toronto, ON: Canadian Observatory on Homelessness Press.
Young people become homeless for many reasons, including because society fails to prevent it from occurring. The risk factors that contribute to youth homelessness are clear and can be addressed with early intervention. For instance, in a sample of 974 young people who were street involved and using substances, 76% had not completed high school, with analysis showing these were related to childhood maltreatment, such as physical abuse, emotional abuse, physical neglect, and emotional neglect (Barker, Kerr, Dong, Wood, & DeBeck, 2017). Multivariate analysis from this study indicated that there was a cumulative effect, such that the greater the number of different forms of childhood maltreatment, the greater the chance of not completing high school (Barker et al., 2017). It is societal failures that allow young people to be victimized, experience trauma, and subsequently fall through the proverbial cracks like not completing high school.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=731#h5p-108
In this video, Dr. Katrina Milaney explains that young people who become homeless have often experienced higher rates of adverse childhood events (ACEs) and involvement with the child welfare system. She argues that if we can figure out how to intervene at the right time, we can help prevent youth homelessness from occurring. This video is 0:31 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: Early trauma and homelessness prevention
Creating a shift towards prevention is important because people who experience homelessness as adults also have histories of youth homelessness, suggesting that interrupting this cycle early can help prevent chronic homelessness throughout a person’s life (Parpouchi, Moniruzzaman, & Somers, 2021). However, while prevention makes good sense, it is easier said than done. There are deeply rooted structural inequities in the way our society operates including, but not limited to, poverty, racism, and discrimination. In the next video, Dr. Naomi Nichols reflects on the structural barriers that contribute to youth homelessness, with the recognition that they are also intertwined with the interpersonal and systemic challenges.
In this video, Dr. Naomi Nichols explains that there are many reasons some young people become homeless and that their experiences may be episodic or longer-term and more pronounced. She notes that prior to experiencing homelessness a young person might have precipitating events, such as family conflict related to identity-based prejudices that make leaving a safer option than remaining at home. Dr. Nichols argues that when young people try to seek housing, they encounter a rental market that is expensive and often discriminatory towards young people. She identifies institutional pathways leading to youth homelessness as well, such as inadequate planning for young people exiting child welfare, corrections, and in-patient mental health facilities. Dr. Nichols concludes by arguing that COVID-19 has increased family stress levels in unprecedented ways, which has negatively impacted young people’s mental health and ability to rely on strategies and supports that might have been available to them prior to the pandemic. This video is 5:03 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Why do some young people become homeless?
Dr. Nichols has extensively researched institutional responses to youth homelessness and is the author of the book, “Youth, school, and community: Participatory institutional ethnographies” (Nichols, 2019). Ideally, schools should be places where young people feel safe and included. For some youth, however, they are places of exclusion and marginalization. Particularly for a young person who is having interpersonal struggles, such as conflict with their parents, school may become an extension of these challenges. They may have additional conflict with teachers or peers, they may struggle with understanding or completing the coursework, or they may choose to stop attending altogether. When robust supports are in place, the school can be a site of youth homelessness prevention work, but without these supports we see systems-level failure.
A review of pre-service teacher certification standards in the United States and Canada found that there are few requirements for teacher candidates to obtain training in mental health-relevant interventions, despite teachers’ unique positionality and ability to promote student social and emotional well-being (Brown, Phillippo, Weston, & Rodger, 2019). When we ask why young people become homeless, we must consider that it is because our systems and institutions fail to prevent it from occurring. We see these gaps across sectors, including education, child welfare, health care, mental health care, and youth justice. When young people are not well-served by these systems, they risk falling into homelessness.
Among the most commonly identified systems-level pathways into youth homeless is that of child welfare, such as residing in foster care. Dr. Nichols and her team (2017) led an analysis of the child welfare data from the first national survey of youth homelessness in Canada and found that 58% were involved with the child welfare system at some point in their life. This figure is striking in itself, but even more so when we consider that only 0.3% of the general population has had contact – meaning that youth experiencing homelessness are 193 times more likely to have been through child welfare systems (Nichols et al., 2017). In the next video, Dr. Naomi Nichols reflects on how systemic failures in the education and child welfare systems can contribute to youth homelessness.
In this video, Dr. Naomi Nichols argues that youth experiencing homelessness are invisibilized in public systems that are not well equipped to facilitate positive referrals between their institutions. She identifies schools and child welfare as a particular gap. Dr. Nichols explains that school officials have a duty to report a student who is 16 or under and experiencing homelessness to child welfare officials. However, the child welfare system pivots on parental abuse and neglect, so if this is not the cause for the report, the child welfare worker can say the youth is not eligible for protection. This video is 1:16 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Child welfare, schools, and youth
Young people who experience homelessness have significantly higher rates of involvement with the child welfare system. This is a systemic failure. When young people are removed from their family it may be for legitimate reasons, such as neglect or abuse, but it is the child welfare authority’s obligation to then act in the role of their parent. Many young people continue to struggle with the effects of the trauma incurred before they were taken into custody. While in care, some young people choose to leave before they reach the official age at which care ends. In these instances, they may engage in couch-surfing, use emergency shelters, or sleep outside in public spaces. Alternatively, some young people continue in care until they reach the age at which it ends, and they may not have the support or ability to live independently. In the next two videos, Dr. Jeff Karabanow and Dr. Bill O’Grady reflect on child welfare as one of many interrelated pathways into youth homelessness.
In this video, Dr. Jeff Karabanow explains that half of the young people experiencing homelessness have come through the child welfare system. He notes that this figure is indicative of the level of trauma these youth experience even prior to care, and how it is not resolved within the system. Dr. Karabanow concludes by arguing that if 1 in 2 people on the streets is coming from child welfare, we need to look more closely at what is happening in that world. This video is 0:32 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: Child welfare and youth homelessness
In this video, Dr. William [Bill] O’Grady explains that every young person has their own story, but that there are commonalities in why youth experience homelessness. He identifies histories of conflict and abuse as primary factors. Dr. O’Grady notes that approximately half of the young people accessing services for homeless youth have had contact with the child welfare system, indicating early experiences of neglect. He explains that within Ontario the age of support has been extended recently, but that it should be raised even higher to support young people until the age of 21. Dr. O’Grady explains that there is an over-representation of LGBTQ2S+ youth who experience homelessness, compared to the general population. He concludes by noting that youth homelessness needs to be understood as unique from adult homelessness. This video is 3:31 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: Why do some young people become homeless?
While child welfare involvement is a systemic pathway into homelessness for many young people in Canada, it is even more so for Indigenous youth. Analysis of national survey data shows that Indigenous individuals are nearly four times more likely to be involved with the child welfare system than non-Indigenous persons, which demonstrates that at the population level, Indigenous peoples are at far greater risk of having been involved in the child welfare system, and consequently experiencing homelessness than non-Indigenous peoples (Alberton, Angell, Gorey, & Grenier, 2020). In the next video, Dr. Jacqueline Kennelly speaks about the disproportionate number of Indigenous youth who are in the child welfare system. Following this video, we present a brief documentary from CBC that features Adrianna sharing her personal story. As you watch it, we encourage you to reflect on what you have learned throughout this section on the complex and intersecting reasons some young people become homeless.
In this video, Dr. Jacqueline Kennelly explains that young people who experience homelessness often leave school, which has long-term consequences for obtaining employment. She notes that youth leaving child welfare is a major category of young people experiencing homelessness, and that recent advocacy by former foster care children and their supporters has helped extend the period in which they receive financial supports. Dr. Kennelly concludes by noting that there are a disproportionate number of Indigenous youth in the child welfare system because of Canada’s history of colonialism and displacement, leading to inter-generational trauma and entrenchment in poverty. This video is 1:56 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Child welfare involvement and youth homelessness
How do you think Adrianna’s story demonstrates the complexity of why some young people become homeless? In what ways did you see interpersonal, structural, and systemic factors contribute? Take a moment to reflect back on the featured reading detailing a pathway to preventing youth homelessness. What could have been done to prevent Adrianna from experiencing the trauma and hardships she went through?
Adrianna’s story is heart-breaking, as are many young people’s who experience homelessness, because they result from circumstances beyond their control. Throughout this section, we have seen the many hardships that lead young people into homelessness, but also how they use resourceful means to remove themselves from difficult and dangerous situations. This section opened with a story about one of the authors walking along with a young man who had been sleeping rough, using intravenous drugs, not eating well, and not bathing. The public response indicated a lack of understanding about the multiple reasons this young man was homeless, focusing instead on seeing his individual shortcomings. This event occurred nearly 20 years ago before we had a definition of youth homelessness (COH, 2016), and public awareness campaigns such as through Raising the Roof and Home Depot’s “The Orange Door Campaign.” We wondered whether there has been a change in public perception and understanding about youth homelessness over the years. Would people still look away today? We conclude this section with a video of Dr. Jeff Karabanow speaking about research he conducted on public perceptions. While it was in a different city than the story we began with, we would like to hope that it represents a shift towards a more inclusive and supportive direction overall.
In this video, Dr. Jeff Karabanow discusses the results of a survey he conducted on public perceptions about youth homelessness in Halifax. He notes that while we tend to have stereotypes and biases pertaining to homelessness in general, the small majority of respondents were deeply compassionate and empathetic towards these young people. Dr. Karabanow shares that the research showed many people felt that it was unconscionable to have young people on the streets and that if families could not support this population, then we need to have deeper interventions as a society. This video is 0:57 in length and has closed captions available in English.
Key Takeaways
The reasons young people become homeless are complicated and not binary in nature. It is rarely the case that a young person is housed one day and homeless the next – rather, it is often the result of ongoing conflicts and struggles in the young person’s life. These may occur at the interpersonal level, as challenges arise in relationships with parents, siblings, teachers, and peers, and may be a response to the youth’s gender or sexual identity. When interpersonal struggles arise, they are often also located within a context of structural factors such as inequity, poverty, and discrimination. We heard that youth homelessness occurs because society allows it to occur, and that when the problem is identified it is the government’s obligation to step in and make changes. The best change would be a shift towards prevention, which we saw outlined in the roadmap infographic and featured reading.
At the systemic level, there are many institutions that are implicated in youth becoming homeless, such as education, health care, mental health care, and youth justice. However, the most commonly cited was the child welfare system. Not only are youth who experience homelessness 193 times more likely to be involved (Nichols et al., 2017) but those who are Indigenous are even more disproportionately represented. The reasons young people become homeless are complex, but they are also well documented. We know why young people become homeless. Since we know, it is our obligation to prevent it from happening before they face the traumas of a young life spent on the street.
Click the link below to listen to all of the researchers answer the question “Why do some young people become homeless?” in audio format on our podcast!
72
In the previous section, we looked at the many complex and intersecting pathways that lead young people into homelessness. Once a young person has left home, been thrown out, or left the child welfare system, they may find themselves couch-surfing, residing in an emergency shelter, or they may be unsheltered, sleeping outside in public places. We began the last section with a story about a young man who was sleeping in a rock garden, and noted that he was also malnourished, using intravenous drugs, and not engaging in hygienic practices like bathing. These are just some of the challenges that young people face while experiencing homelessness in Canada. The author who knew this young man does not know what happened to him, as it is fairly common for these young people to move around. We would like to believe he is alive and well, but the severity of challenges associated with street life are indisputable. Before you continue through the material of this section, we invite you to pause and reflect here on this young man. What challenges do you think he and other youth face as a result of experiencing homelessness? You may use the space below to record your thoughts.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=733#h5p-109
The need for prevention becomes evident when we look closely at the challenges and risks young people face when experiencing homelessness. While they must be recognized as strong and independent for navigating these challenges, we cannot forget that they are fundamentally young adults who are placed in dangerous environments and asked to engage in tasks, like finding independent housing, that are not generally asked of housed youth who are the same age. For instance, when a 16–year–old leaves an abusive home they may go to a friend’s house or shelter, but the ultimate expectation is that they obtain housing of their own. Securing housing – and having the income to pay for it – is not something we would expect of most people this age. Although these young people may be living independently, it does not necessarily mean they have the social, emotional, and life skill preparation required to do so. We begin with a video of Dr. Jeff Karabanow discussing how young people may initially view the street as a safer place than the one they left, but how it quickly becomes an exploitative place that they need to be supported in order to move rapidly away from.
In this video Dr. Jeff Karabanow shares that many young people believe the street is a better option than the place they left. He notes that this is a problematic notion because, while the streets can offer some initial respite and social connections, it is a deeply exploitative environment that forces young people to constantly be in survival mode. Dr. Karabanow explains that while on the street young people have to navigate the general public, changing weather conditions, and a sense of boredom. He notes that young people experiencing homelessness are at high risk for abuse and exploitation, and that there are drug dynamics on the street that can amplify mental health and addiction challenges. Dr. Karabanow concludes that although the street might offer some short-term crisis relief for youth leaving home, it is imperative that they be moved off the streets and into safe and secure housing as quickly as possible. This video is 3:49 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: What are the challenges these young people face?
Living in survival mode is characteristic of homelessness, whether as a youth or an adult. However, the developmental stage of young people means they are often more dependent on others for this survival, which can place them in a vulnerable position. For instance, peer relationships play a central role in these young people’s lives and part of the work of navigating shelters and other street-based environments is developing strategies for managing their influence (Alschech, Taiwo-Hanna, & Shier, 2020). Likewise, romantic relationships amongst youth experiencing homelessness can also have a contradictory nature including positive aspects such as connection, support, validation, and encouragement, but also negative experiences such as interpersonal violence and the stress of managing street-life (Joly & Connolly, 2019). The reliance on others, including those who are also street-involved, can lead to violence and exploitation. In the next video, Dr. Stephen Gaetz explains further.
In this video, Dr. Stephen Gaetz states that many of the challenges adults who experience homelessness face also apply to young people, but that there are some youth-specific challenges as well. Notably, he points to the negative impacts homelessness has on young people’s health, mental health, well-being, and nutrition at a time when they are still developing. Dr. Gaetz explains that youth experiencing homelessness are exposed to high rates of crime and violence, in large part because we create institutional structures, such as shelters, that serve as recruitment sites for predators like sex traffickers. He notes that prolonged homelessness can have lifelong impacts on youth and potentially lead to chronic homelessness when they are adults. Dr. Gaetz concludes by arguing we need to seriously prioritize youth homelessness prevention because it is the pipeline into adult homelessness. This video is 2:59 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: What are the challenges these young people face?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=733#h5p-110
The first national survey of homeless youth clearly demonstrated the range of suffering that young people experience while homeless, including housing precarity, violence, marginalization, health challenges, and social exclusion (Gaetz, O’Grady, Kidd, & Schwan, 2016). The second national survey that followed reconfirmed that exposure to violence and victimization are common for young people experiencing homelessness, with negative outcomes such as 35% reporting at least 1 suicide attempt and 33% reporting drug overdose that required hospitalization (Kidd et al., 2021). Although the public perception may be that young people who are unhoused present a sense of danger – such as the young man in the story at the beginning – the reality is that these young people are much more likely to be the victims of crime than perpetrators.
There are several reasons why these young people are frequently victimized. For instance, without the security of a place to keep their possessions safe many young people carry their belongings with them at all times, increasing their vulnerability to robbery. Many of these young people have limited support networks, meaning there are few people who are looking out for them and/or whom they could turn to for help. Finally, because these young people are more frequently perceived to be criminally involved than as victims, they have poor relations with police and are less likely to report being victimized. You can read more about this in the chapter on Sociology & Crimino-Legal Studies. In the next video, Dr. Jacqueline Kennelly explains further.
In this video, Dr. Jacqueline Kennelly notes that the challenges young people face vary somewhat depending on where they live and the kinds of supports they have. For instance, youth in rural settings may experience hidden homelessness and need to leave behind their support networks to seek services in larger cities. She discusses the risks youth experience once becoming homeless, such as being vulnerable to street-based violence, robbery, and trafficking. Dr. Kennelly argues that while these young people are in need of protection, they are often targeted by police and seen as perpetrators of crime. Consequently, many do not feel comfortable reporting their victimization. This video is 2:07 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: What are the challenges these young people face?
There is a cycle in which youth who experience homelessness are victimized but do not report it to the police because of poor relationships. However, because they do not report these incidences, police do not generally view them as being victimized. What can be done to disrupt this cycle, so that police see these young people as needing protection, and these young people see the police as sources of that protection?
A young person’s perception of their own vulnerability may be connected to the length of time they have experienced homelessness. Analysis from a national survey of youth experiencing homelessness showed, for instance, that not every young person considers themselves to be homeless, but that past trauma and the intensity of the day-to-day hardships contribute to adopting this identity (O’Grady, Kidd, & Gaetz, 2020). Among other factors, O’Grady et al., (2020) found that when a person reported being the victim of crime in the preceding 12 months, they were more likely to consider themselves homeless and take on homelessness as a part of their self-identity. This research is important because it helps us understand the connection between being victimized and adopting a homeless identity, which can make it more difficult to transition off the streets. By extension, we need to consider the impact being victimized has on young people’s chances and opportunities to become securely housed. In the next video, Dr. Bill O’Grady speaks about his team’s research and the dire impacts victimization can have on these young people.
In this video, Dr. William [Bill] O’Grady explains that there are some general challenges youth experiencing homelessness face, but that they are impacted by layers of marginality related to ethnicity, gender, and/or sexual orientation. He notes that these common challenges include a lack of income, no high school diploma, and not having lived independently before. Dr. O’Grady discusses his research, which shows youth who experience homelessness are at high risk of multiple victimization episodes, including being robbed, physically and/or sexually assaulted, and recruited into sex trafficking. While there is a public perception that these youth commit crimes, Dr. O’Grady concludes they are much more likely to be the victims. This video is 4:11 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: What are the challenges these young people face?
In the preceding video, Dr. O’Grady spoke about the layers of marginality that shape young people’s experiences of homelessness and that contribute to the challenges they face. Being a young adult is one such layer that interacts with others. For instance, among individuals who are Indigenous, the strongest predictor of experiencing visible (i.e. unsheltered) homelessness has been found to be child welfare involvement (Alberton et al., 2020). This shows us a connection between Indigeneity and child welfare involvement as additional layers of marginality for some young people.
Researchers have also pointed to the ways in which youth who experience homelessness have a much higher prevalence of disabilities than the general public (Baker Collins & Fudge Schormans, 2021). A chart review of intake data for 494 clients enrolled in a community-based inner-city mental health program in Vancouver, for instance, identified a subsample of 44 individuals who were referred for neurophysiological evaluation (Barone et al., 2019). Findings of this analysis revealed that 80% of the referred clients showed cognitive impairment, primarily related to attention and processing speed, 51% of clients referred for testing did not have more than a grade ten education, and only 5% received government support intended for individuals who have significant disabilities (Barone et al., 2019). The invisibility of disability means that young people with cognitive and other disabilities experiencing homelessness are particularly vulnerable and may face significant barriers gaining access to the tailored supports they need (Baker Collins, Schormans, Watt, Idems, & Wilson, 2018).
There are many layers of marginality that serve to shape a young person’s experiences of homelessness and the challenges they face. The results of the second national survey of 1,375 youth experiencing homelessness emphasized that while all these young people are vulnerable, there is heightened adversity for Indigenous persons, young women, and young people who identify as LGBTQ2S+ (Kidd et al., 2021). In the next video, Dr. Alex Abramovich speaks about the unique challenges unhoused LGBTQ2S+ youth face and the resulting risks to their safety.
In this video, Dr. Alex Abramovich explains that for LGBTQ2S+ youth who experience homelessness, safety is an ongoing challenge and source of daily anxiety. He notes that most spaces these young people navigate are unsafe and that they often have to choose between unsafe alternatives. Dr. Abramovich provides the example of a trans youth deciding between staying in a shelter where their gender identity will be discriminated against or sleeping outside where they will face unknown physical dangers. He concludes by noting that navigating unsafe spaces also makes it more difficult for LGBTQ2S+ youth experiencing homelessness to access supports where they feel they can be honest about their identity. This video is 2:19 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: What are the challenges these young people face?
Being a young person who identifies as an LGBTQ2S+ individual poses additional challenges while experiencing homelessness. In this section’s featured reading we share the results of a study Dr. Abramovich and his team conducted, to learn more about the experiences of LGBTQ2S+ youth experiencing homelessness in Toronto and its surrounding areas during the COVID-19 pandemic. Through surveys and interviews, they found that these young people reported poor mental health, such as suicidality, depression, anxiety, and increased substance use, compounded by a lack of access to health care and social services (Abramovich et al., 2021). Although these issues were not created by the pandemic (i.e. they already existed), these young people felt they had been exacerbated by pandemic conditions. We invite you now to learn more about this study’s outcomes, through the featured reading presented below. While you are reading, we encourage you to reflect on how the discrimination LGBTQ2S+ youth experience is a layer of marginality.
Abramovich, A., Pang, N., Moss, A., Logie, C. H., Chaiton, M., Kidd, S. A., & Hamilton, H. A. (2021). Investigating the impacts of COVID-19 among LGBTQ2S youth experiencing homelessness. PLOS ONE, 16(9): e0257693.
Throughout this section, we have considered the numerous challenges that young people face while experiencing homelessness. We have seen that although they may initially see the streets as a respite from the homelife they left, it soon becomes a space of violence and exploitation. Because they lack private spaces, have limited social support, and generally poor relations with the police, these young people are at high risk of victimization. Indeed, our current emergency response – which places these young people together in shelter settings – serves as a recruitment ground for sexual predators. In addition to being young, these individuals’ experiences of homelessness are shaped by identity markers, such as their Indigeneity, ethnicity, level of abilities, gender, and/or sexuality.
While experiencing homelessness, young people often spend much of their time trying to meet their basic survival needs, like obtaining food and shelter. In the “At-Risk Youth Study” conducted with 1,066 street-involved young people who use drugs, 68% reported some degree of food insufficiency, defined as being hungry but not having enough money to buy food, and 53% met the criteria for depression (Goldman-Hasbun, Nosova, DeBeck, Dahlby, & Kerr, 2019). When these researchers looked to see if a relationship existed between these two variables, they found that the youth who reported often experiencing food insufficiency also had a higher likelihood of reporting depression, suggesting the lack of food may negatively impact these young people’s mental well-being on the street (Goldman-Hasbun et al., 2019). Food insecurity has also been found to exacerbate body image concerns and lead to higher rates of compensatory substance use amongst youth experiencing homelessness (Luongo, 2018).
We see from these research studies, that the success of young people’s survival activities – like whether they are able to secure adequate levels of nutritious food – has an impact on their well-being and self-esteem. Youth who experience homelessness often perceive themselves to be devalued in society, with research linking this to outcomes such as engaging in higher rates of unprotected sex, increased alcohol use, and daily heroin use (Karamouzian et al., 2019). These risk factors are not always well addressed either, such as through their differential use of sexual health care services (Côté, 2019). In the next video, Dr. Sean Kidd explains how these negative self-images are particularly detrimental for a young person who is still developing and reiterates that navigating supports and peer relations on the street can be a primary challenge these young people face.
In this video, Dr. Sean Kidd notes that young people experiencing homelessness are also in a developmental period, where they are forming their brains and identities, and that an episode of homelessness can make it difficult for them to sustain a positive sense of self. He explains that there are basic survival challenges, such as obtaining food, shelter, and safety, and that these young people experience a profound level of violence on the street. Dr. Kidd relays research findings that show violence on the street, whether daily intimidation or life-threatening events, carries tremendous weight in relation to suicidal ideation, drug overdoses, and being in a general state of distress. He further notes that young people may face challenges finding supports that offer the kind of tangible and emotional help they need, as their friends may not provide the best advice and they may resist seeking out support workers based on previous negative encounters with authority figures in their lives. Dr. Kidd concludes by discussing the challenges young people face in transitioning out of homelessness, such as wanting to return to school but finding their former peers have moved on. This video is 4:34 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: What are the challenges these young people face?
Young people have to navigate the street through conscious decisions about who they feel they are as a person, and how they can best survive within that physical and social environment (Frederick, 2019). However, as they work towards exiting homelessness, they may find that the barriers they encountered on the streets continue to be challenges. The effects of trauma and violence on the street can be long-lasting, and young people who have spent formative years in unstable living conditions may not have developed independent living skills. This means that even as they try to secure housing, they may find they do not have the income or the means to secure a job needed to pay rent. They may also find that even if housing is secured, they have limited knowledge of how to manage household responsibilities, like grocery shopping, cooking, and budgeting their money. Young people may encounter on-going interpersonal challenges, such as with roommates or landlords that they are unsure how to navigate. We see that the challenges that arise while a young person is homeless do not necessarily get resolved just because they seek housing. In the next video, Dr. Tyler Frederick reviews the challenges these young people face and explains how they can continue even once the young person is housed.
In this video, Dr. Tyler Frederick argues that homelessness can be an extremely stressful experience for young people, as they may not know where to go, what to do, how to get help, or whom to trust. He notes that when a young person is already struggling, such as with depression or anxiety, and they are placed in a stressful environment like a shelter, there will be negative outcomes for their mental health and/or substance use. Dr. Frederick warns that young people experiencing homelessness are at high risk for victimization, like violence and sex trafficking, and that they face systemic vulnerabilities, such as being over-policed. Dr. Frederick concludes that exiting homelessness is a challenge for these youth as well, who have to balance daily stressors of life with finding affordable housing, a landlord who is willing to rent to them, and a reliable source of income. This video is 4:24 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: What are the challenges these young people face?
Being able to move out of homelessness and into secure housing is itself a primary challenge young people face. Consider the many barriers we have discussed throughout this section. They often have left homelives that were not supportive only to find themselves in dangerous and exploitative environments. Many young people are victimized and face daily stressors just to meet their basic needs. Throughout all of this, they are discriminated against and commonly suffer from poor self-esteem, trauma, and diminished mental health. They are at an age where they are still developing, and securely housed youth of the same age are not met with the same expectations. Yet, despite these conditions and through their own personal strength, these young people seek to find housing and security in their lives. In a study of formerly homeless youth in Toronto, researchers found that the primary barriers they encounter are related to unaffordable housing, having limited education, inadequate employment opportunities, living in poverty, and having a lack of social capital (Thulien, Gastaldo, Hwang, & McCay, 2018). In the next video, lead author Dr. Naomi Thulien speaks about the findings of this study and what it can tell us about how to help improve the situation for these young people.
In this video, Dr. Naomi Thulien argues that young people experiencing homelessness face the clear challenge of not having anywhere to live, as well as additional challenges related to incomplete education, inability to find employment, and a lack of connections within the community. Dr. Thulien explains that these youth experience homelessness during a period in which they are still developing, and that this is particularly challenging as Canadian youth, in general, are staying home longer and delaying living independently. She notes that obtaining housing in a competitive market may be even more difficult for these youth, as a result of stigma, poor credit, and not having a surety in place. Dr. Thulien encourages landlords to make an intentional decision to rent to these young people as a way to help them exit homelessness. This video is 4:14 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: What are the challenges these young people face?
There are many challenges young people face when they experience homelessness. We have seen throughout this section that while they may think about leaving home as a respite, they soon realize that the street is not a safe environment. Rather, they are exposed to considerable violence, victimization, and trauma at a time in their life when they are still developing mentally, emotionally, physically, and socially. The impacts of this violence and trauma can last throughout their lives.
When a young person becomes homeless, they may stay temporarily with friends or extended family, reside in an emergency shelter, or sleep outside in public places. We began this section by returning to one young man, who was sleeping outside, using substances, and facing considerable public discrimination as a result. The perception of these young people is often that they are dangerous and/or criminals, yet what the research shows is that they are much more likely to be the victims. Our current emergency response increases these chances, by placing young people together and increasing their visibility and vulnerability to predators. Indeed, sexual victimization and trafficking are common outcomes for young people who become homeless.
While all young people are vulnerable when in street environments, we learned that there are additional layers of marginality that can serve to make some even more at-risk. In particular, young people who are Indigenous, racialized, living with disabilities, female, and/or who identify as LGBTQ2S+ are among the highest risk for additional harms associated with homelessness. While in a developmental stage, and navigating risks of violence and trauma, these young people also must function in survival mode just to meet their basic needs. The demand to always be searching for safety, food, and shelter creates a physiological state of stress that can also have life-long consequences.
If a young person is able to find some stability and begin to transition out of homelessness, they may find that the challenges persist. As many young people leave school prior to graduating, they often are not able to obtain a job that is high paying enough to cover the costs of market rent. Returning to school, getting a job, and finding secure and affordable housing are considerable tasks that take time. Exiting homelessness, and recovering from the trauma of the experience, is a process that requires a great deal of personal strength and social support.
Click the link below to listen to all of the researchers answer the question “What are the challenges these young people face?” in audio format on our podcast!
73
Let’s imagine it is a bright sunny day back in July 2005. The same author is volunteering at a drop-in centre for youth and takes a walk to pick up the muffins and donuts from the local news station. On this particular day, as she walks back, she encounters the same young man. Rather than walking back with her, he stops to say hello and tell her about the changes in his life. In the time since she last saw him, he has been enrolled in a program designed to help young people transition out of homelessness. A team of support workers has helped him find housing, provided subsidies to cover the cost of rent, and connected him with a harm reduction program within the community. He says he cannot stop to talk long because he is on his way to an adult education centre, where he is working on credits toward his high school equivalency.
This is not a storybook ending. The challenges he faced on the street – violence and trauma in his early years, mental health struggles, addictions, malnutrition, and the physical effects on his body – have not magically disappeared. The key difference is that he has received the support he needs to begin the difficult process of transitioning out of homelessness. This is not a linear path, and his support workers know that his risk of falling back into homelessness again is high. Their role is to help him maintain his housing and to help connect him with the supports he needs to be well. On the very best of days, this work remains two steps forward, one step back. Throughout this section we will take a closer look at the work young people undertake to exit homelessness, and what can be done to support them on their journey. Before you continue through the material, we invite you to pause now and record your thoughts about how we can best support young people throughout this process.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=735#h5p-111
Becoming securely housed is not a linear event where young people exit the street and become permanently housed. Exiting youth homelessness does not happen immediately, but rather takes place as a series of stages that include a turning point, housing, acceptance, and achievement (Karabanow, Hughes, Kidd, & Frederick, 2018). Karabanow et al., (2018) note that in their study of young people exiting homelessness, what stood out was that even among the successes these youth achieved, they still struggled on a daily basis to maintain their stability while reconstructing their sense of self-identity. This identity-struggle is often characteristic of adults exiting homelessness as well, as they continue to face barriers related to poverty, social marginalization, inadequate and unaffordable housing, violence, and lack of access to services to meet their personal needs (Sylvestre et al., 2018).
For many young people who transition off the streets, the ability to formulate and realize long-term plans remains marked by their need to focus on day-to-day existence, which can be characterized as a precarious path marked by structural gaps (Thulien et al., 2018). Young people need rent subsidies and affordable housing, but it is also important to consider what social support and meaningful social integration looks like in their lives (Thulien et al., 2019b). As youth become more stable, they often want to distance themselves from their previous identity as a person experiencing homelessness, and need to cultivate new identity capital (Thulien, Gastaldo, McCay, & Hwang, 2019a). We begin this section by returning to our conversation with Dr. Naomi Thulien, who speaks about the importance of helping young people with their financial, support, and identity needs in order to help them successfully make the transition and find long-term stability.
In this video, Dr. Naomi Thulien identifies three key factors young people need to successfully exit homelessness. These include financial supports, such as rent subsidies and a living wage, social supports through community connections in education, employment, and faith-based places, and identity-based supports to foster a sense of purpose and control upon which these youth can draw. This video is 1:26 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: How can young people be supported to exit homelessness permanently?
Housing is the first step in supporting young people exiting homelessness – but it is not the last step. Even as young people become housed, they often still struggle with the effects of having been homeless, and the trauma and stress that goes along with that experience. Research shows that even amongst young adults residing in single room occupancy housing, there are still high mortality rates, multi-morbid illnesses, unmet mental health needs, and extreme poverty (Barbic et al., 2018). Young people may also have on-going sexual health considerations, such as whether to continue with a pregnancy and/or intimate relationships (Begun, 2019). In addition to on-going physical and mental health effects, young people may have acquired legal challenges that can complicate leaving the street and that need to be identified and addressed or risk being barriers to long-term housing security (Chan & Huys, 2017). As we examine more closely in the chapter on Sociology & Crimino-Legal Studies, ticketing the money-making activities of people experiencing homelessness (such as panhandling and squeegeeing) can create barriers to moving out of homelessness, as they often go unpaid and can count against a person’s credit score, which makes it difficult to qualify for housing.
We can see even from this brief discussion, that it is not a simple task for young people to become housed. Gaetz, Ward, and Kimura (2019) argue that when considering what it means to successfully exit homelessness, we must take a holistic approach that recognizes a range of positive outcomes related to housing, but also to safety and security, health and well-being, social connections and integration, and the pursuit of goals that are meaningful to the individual. Having housing is an important place to begin, but to assist young in permanently exiting homelessness, we also must ensure they have access to a range of wrap-around supports that are tailored to their self-identified needs. In the next two videos, Dr. Kaitlin Schwan and Dr. Jacqueline Kennelly respectively discuss the need for affordable housing with wrap-around supports. If you would like to learn more about these kinds of supports, we encourage you to read the chapters on Mental Health and Social Work, where we examine case management and different support styles in more detail.
In this video, Dr. Kaitlin Schwan argues that in Canada we need to expand housing for young people who are experiencing homelessness or at risk, by enforcing the development of affordable housing that reflects the actual level of income these young people have access to. She notes that these youth need wrap-around supports and services to help them with life skills, such as money-management and cooking, and that these youth need to be supported in learning about their tenant rights. Dr. Schwan states that we need to ensure there is legal infrastructure in place to protect young people’s right to housing. She concludes by explaining that many young people experiencing homelessness wish to reconnect with family members, and that programs that help them do so in a safe way can provide an additional layer of support as they transition into secure housing. This video is 4:45 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: How can young people be supported to exit homelessness permanently?
In this video, Dr. Jacqueline Kennelly argues that we need affordable housing for young people and their families. She notes that once housing is secured, young people need wrap-around supports, including Intensive Case Managers, to help them navigate complex structures, such as signing up for government financial assistance, obtaining mental health supports, and learning how to register for and finance schooling. Dr. Kennelly explains that youth exiting homelessness need help, guidance, and people who care about them, the same as all young people need. She concludes that since this important work is often undertaken by non-profit organizations, they need to receive increased funding. This video is 3:24 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: How can young people be supported to exit homelessness permanently?
Housing First, as discussed in the chapter on Politics, Policy, & Housing in Canada, is an intervention that prioritizes getting people housed and then providing them with the kinds of supports they need, according to principles such as client choice and self-determination. For young people, Housing First may look different than it does for adults. As teenagers or young adults, transitional housing with peers and on-site support may be preferrable to independent housing where the young person is expected to manage on their own. Results from “Without a Home,” the first national youth homelessness survey, showed that we need to prioritize prevention-focused approaches, like Housing First that are adapted for the unique needs of youth (Gaetz, O’Grady, Kidd, & Schwan, 2016).
Based on what you have learned about the reasons young people become homeless and the challenges they face, what unique needs do you think they might have related to housing? How might Housing First be different for a teenager or young adult than for someone who is older?
A critical component of Housing First initiatives for young people is helping ensure they feel a sense of social inclusion. When a young person becomes homeless, they often lose their connection to family, friends, and the general community. As we have seen, this can have a detrimental impact on their sense of identity and well-being. Young people need to engage in meaningful pursuits as they progress towards greater stability, and a key part of this is connecting them with supportive and reliable adults they can turn to. Social service providers can play an important role in helping young people to feel connected, by reassuring them that they are supported and will not be abandoned (Kozloff, Bergmans, Snider, Langley, & Stergiopoulos, 2018).
Young people’s own subjective sense of their stability is one of the key indicators of long-term housing stability (Frederick, Vitopoulos, Leon, & Kidd, 2021) and the more these young people access services, the less likely they are to return to homelessness (Barker, Shoveller, Grant, Kerr, & DeBeck, 2020). These findings suggest that connecting youth with services, and helping them feel stable in their housing, is critically important for increasing the chances they permanently exit homelessness. In the next two videos, Dr. Jeff Karabanow and Dr. Tyler Frederick speak about the importance of Housing First and having supportive people in the lives of young people transitioning out of homelessness.
In this video, Dr. Jeff Karabanow explains that there are different best-practice approaches for supporting youth exiting homelessness but that Housing First is critical for providing a safe sanctuary as a basic initial step. He notes that some young people may wish to return home, if it is safe, and that there are programs that can assist with this. Dr. Karabanow expresses that housing is an important step but that once the youth is housed we need to consider the types of wrap-around supports they might need, including feeling part of the community, returning to school, and/or finding employment. He notes that youth need circles of care that help them deal with trauma, and issues such as addiction and/or mental illness using harm reduction approaches and philosophies of compassion, choice, and gradual change. Dr. Karabanow identifies different intervention approaches that have shown positive results for youth, but also notes that what is most critical is that the young person has at least one person in their life they feel connected to, and who will support them. This video is 4:50 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: How can young people be supported to exit homelessness permanently?
In this video, Dr. Tyler Frederick explains that the first step in helping young people exit homelessness is improving their access to affordable housing, but that addressing permanency is more difficult. He notes that many young people struggle to remain housed due to a range of complex issues, such as only being able to afford poor quality housing, difficulties with landlords, and challenges with roommates. Dr. Frederick argues that young people exiting homelessness may lack a critical safety net to help them navigate these issues and that having at least one person they can count on, whether a friend or case manager, is essential for achieving longer-term stability. He cautions that young people may become stuck after getting housed and that they often benefit from bridging support to help them return to school, find employment, and learn independent living skills. Dr. Frederick concludes that as youth transition out of homelessness, it is critical they feel a sense of belonging in the community and have mental health and wellness supports to help them navigate the stress that these life changes may bring. This video is 8:29 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: How can young people be supported to exit homelessness permanently?
Karabanow, Hughes, Kidd, and Frederick (2018) have published a book entitled, “Homeless youth and the search for stability” detailing the outcomes of a multi-year study on supporting youth exiting homelessness. In the book they write, “… the majority of these young people remain in a fragile state throughout their transitions to ‘non-street’ life. This fragility has much to do with their in-between status. Not certain they have indeed been removed from street life, and by no means comfortable or accepted within mainstream civil society, these young people struggle with their sense of self – of who they are, what they desire, where they are going, and what they need. Given that for most youth living on the street, their memories of home were filled with trauma and upheaval, it is not surprising that while they would dream of leaving the streets and living in a stable environment, they were not sure how to do it” (Karabanow et al., 2018, pg.16).
As part of this project a group of young people, Layla Sunshine, Baby T, Orlando Foster, and Sarafin, worked together to create a truly remarkable comic-style book about the challenges of exiting homelessness.
We encourage you to take a moment and learn more.
Dr. Sean Kidd was a lead researcher on this project as well and has studied young people’s transitions out of homelessness for many years. In the next video, he reflects on this extensive research, identifying several programmatic interventions and the need for tailored mental health and addictions support for young people. Here he explains further.
In this video, Dr. Sean Kidd promotes Family Reconnect as a programmatic intervention that can be used to identify young people experiencing homelessness, quickly assess whether there are any positive familial relationships that exist, and re-establish housing and supports through that relationship. He notes that these programs are helpful in identifying extended family member supports and serving as early intervention to keep young people from living in predacious and violent street environments. Dr. Kidd explains that we need to improve our ability to rapidly house young people leaving institutions, such as child welfare and the criminal justice system. He sites Housing First as an important strategy but notes that youth may require different models than adults, including a focus on congregate living with shared common spaces, life skills training, peer-support, harm reduction or abstinence programming, and ongoing assessment of their changing needs. Dr. Kidd observes that for many young people exiting homelessness, tailored mental health and addiction help is key and that young people must have choice and flexibility in their treatment. They must also have skillful engagers who can help with common factors such as making them feel understood, hopeful, cared for, and like they have someone they can trust. Dr. Kidd concludes by arguing that as part of our efforts to support young people exiting homelessness, it is essential to have reasonable funding and evidence to inform what programs and supports work best for whom. This video is 9:39 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: How can young people be supported to exit homelessness permanently?
In the preceding video, Dr. Kidd explains that programs and interventions should be evidence-informed through the most recent evaluations. In much the same way, Malla et al., (2019) have also argued that youth mental health services are most effective when they involve detailed and carefully orchestrated processes guided by a set of values and principles, clear objectives, training, and evaluation. The research shows that there are innovative programs to help young people cope with mental illness and/or addictions as part of their pathway out of homelessness.
For instance, in Montreal, a team of service providers offers intensive outreach intervention for youth experiencing homelessness and suffering from first episode psychosis and addiction (Doré-Gauthier, Côté, Jutras-Aswad, Ouellet-Plamondon, & Abdel-Baki, 2019). Analysis of this program shows that when the team first meets with youth, they often have poor prognostic factors, such as one of the Cluster B personality disorders, substance use disorders, legal problems, childhood trauma, and lower educational attainment, but that after a period of 6 months the majority have been able to achieve housing stability and improved functionality (Doré-Gauthier et al., 2019). Providers can work together to support the mental health needs of youth experiencing homelessness, as evidenced by the development and growth of the Montreal Homeless Youth Network (Morisseau-Guillot et al., 2020). As an outcome of this collaborative work, a clinic was created for youth to ensure they had timely access to appropriate services, using an approach that engaged young people in service planning and design (Abdel-Baki et al., 2019).
In the preceding video, Dr. Kidd spoke about the need for mental health and addictions support for young people transitioning out of homelessness. He and his team have led a multi-agency and interdisciplinary collaboration, known as the Housing Outreach Program – Collaboration [HOP-C], which is comprised of transitional outreach-based case management, individual and group mental health supports, and peer support (Kidd et al., 2019a, 2019b). These wrap-around supports, built on collaboration, mental health support, and peer support, have been linked to positive outcomes for young people (Vitopoulos et al., 2018b). Ongoing analysis of the HOP-C initiative demonstrates that there is potential benefit in fostering city-level, multi-disciplinary teams that work together across organizations to support young people who are transitioning out of homelessness (Kidd et al., 2020). We invite you now to learn more about the HOP-C project in this section’s featured reading entitled, “Developing a trauma-informed mental health group intervention for youth transitioning out of homelessness” presented below.
Vitopoulos, N., Cerswell Kielburger, L., Frederick, T., & Kidd, S. (2018). Developing a trauma-informed mental health group intervention for youth transitioning out of homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
While young people demonstrate remarkable personal strength in exiting homelessness, they require support as they make these transitions. We have seen that the reasons young people become homeless are complicated, and that while on the street they experience a range of challenges including exposure to violence and trauma, stress, poor mental and physical health, addictions issues, and malnutrition. It is unrealistic to expect young people to recover from these experiences without sustained support and assistance. There is a recurring theme that runs throughout this chapter (and throughout the book as a whole) that argues for prevention and early intervention. If we can stop young people from becoming homeless, they will not have to go through the hardships and recovery period.
In the past, Canada has looked to the United States for solutions on how to address homelessness, such as through Housing First, but Gaetz (2018) notes that we are increasingly seeing international solutions arise. Upstream Canada is one such example, that is adapted from an Australian program and is put in place to identify youth who are at risk of homelessness and school disengagement by implementing a universal screening tool known as the Student Needs Assessment (Sohn & Gaetz, 2020). The values of Upstream Canada are to be collaborative, equitable, integrative, and longitudinal in identifying youth at risk, validating the findings with a trained Upstream Social Worker, and then connecting the youth to coordinated services and supports (Sohn & Gaetz, 2020). In the next video, Dr. Stephen Gaetz speaks about the importance of preventive programs, like Upstream Canada, in identifying young people before they become homeless and intervening to keep them connected and engaged with social supports, such as education.
In this video, Dr. Stephen Gaetz argues that early intervention and prevention programs like Upstream and Family Reconnect are the best place to start supporting young people, so they do not experience homelessness. He notes that thinking about exiting homelessness draws our attention to the damage it causes, and that young people often continue to struggle with malnutrition, poverty, a lack of education and employment, and social exclusion even after they are housed. Dr. Gaetz explains that evidence-based approaches, like Housing First for Youth, are key in supporting the changing needs of developing adolescents and young adults. He states that there are different approaches, such as reconnecting with families if they are safe, obtaining youth-specific transitional housing, and including Indigenous-led housing programs that focus on cultural reconnection. Dr. Gaetz concludes that in addition to housing stabilization, support models must address elements of young people’s well-being using trauma-informed care. This video is 4:35 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Gaetz: How can young people be supported to exit homelessness permanently?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=735#h5p-112
The Upstream model is an important approach for addressing the gap that currently exists in mental health awareness training among pre-service teacher candidates (Brown et al., 2019). Rogers and Shafer (2018) have argued that when teachers are empowered with knowledge to reject the deficit model commonly attached to marginalized youth, they can become advocates for these young people. Teachers are well-situated to identify young people who are at risk of homelessness and help connect them with services and supports. However, it is essential that teachers themselves be educated in trauma and violence-informed care practices (Rodger et al., 2020).
While implementing prevention programs such as Upstream Canada are best-practice approaches, it is still possible that some young people will not be identified through these measures. In these instances, programs such as Family Reconnect can be implemented as early-interventions. Throughout this section, several researchers have identified three core interventions used to help young people, which come into effect at different stages. Upstream Canada has not yet been widely adopted but could help to identify young people in schools, before they become homeless. Family Reconnect is used once a young person has recently become homeless and may have the chance to return to their home (if safe for them to do so) or to live with another family member, such as a grandparent or aunt / uncle. Housing First is the most commonly used of the three programs, and it comes into effect after a young person has been homeless for a period of time and needs help securing housing arrangements and wrap-around supports.
In the next set of videos, Dr. Bill O’Grady and Dr. Alex Abramovich speak about the importance of these programs for young people. However, they also remind us of another common theme throughout this book, which is that there is no one-size-fits-all solution to homelessness. While having contact with supportive family members can help buffer risks on the street (Kidd et al., 2021) and there are therapies that can help families reconcile (Cully, Wu, & Slesnick, 2018), approaches like Family Reconnect might look very different for some youth. In particular, young people who left home or were thrown out over LGBTQ2S+ identity conflicts might not be welcome back home. In these instances, we may need to redefine who counts as family. Here Dr. O’Grady and Dr. Abramovich each respectively explain further.
In this video, Dr. William [Bill] O’Grady explains that in recent years we have expanded our understanding to consider ways of supporting youth exiting homelessness. He notes that school-based early interventions are important because teachers often have a keen sense of which students are at risk, but often do not have the resources to help. Dr. O’Grady advocates for the use of programs like Family Reconnect to help youth re-establish positive relationships, where possible, with members of their family. He argues that targeted approaches are needed, such as for LGBTQ2S+ individuals and youth aging out of state care. Dr. O’Grady notes that since many young people experiencing homelessness have had to prioritize survival over school, it is important to support them in returning to education as a basic human right. He concludes by discussing Housing First for Youth as a key strategy that prioritizes housing and addresses young people’s unique and changing needs. This video is 5:14 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: How can young people be supported to exit homelessness permanently?
In this video, Dr. Alex Abramovich explains that LGBTQ2S+ youth experience homelessness at younger ages than heterosexual and cisgender youth, resulting in longer episodes, higher accumulation of traumas, and making it more difficult to exit. For this reason, he notes, it is critically important to focus on prevention and early intervention efforts, such as through school-based programs. Dr. Abramovich argues that focusing on protective factors is key and that for LGBTQ2S+ youth this often involves peer groups and other supportive people in their lives. He explains that within LGBTQ2S+ communities, the meaning of family may be redefined and this needs to be respected in programs like Family Reconnect to ensure young people’s relationships with supportive people are respected. Dr. Abramovich concludes that these young people benefit from population-based programs that have supportive case managers, and that allow them to be themselves and connect with others who identify in similar ways. This video is 3:10 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: How can young people be supported to exit homelessness permanently?
Family reconciliation work may be more difficult within families where rejection of a young person’s LGBTQ2S+ status is an issue, but there are models of this work that have shown some promising outcomes, such as the Ruth Ellis Centre in Michigan (Jones & Ellis, 2017). As Dr. Abramovich noted in the preceding video, it may be that we need to expand our definition of what family means. If Family Reconnect programs are to be effective with LGBTQ2S+ youth, who constitute a particularly high-risk and marginalized group, then we must first ask whom the young people consider to be their family. Relationships that are supportive, stable, and empowering should be cultivated if in the best interest of the young person involved.
At the heart of this issue, is a young person’s right to make decisions and to choose what is best for them. As young people exit the streets, they are expected to address the challenges of emerging adulthood, independence, and overcoming the trauma that often contributed to their homelessness in the first place (Karabanow et al., 2018). One key way to help support young people permanently exit homelessness is to listen to them and respect that they understand what they need. We must also consider what the research tells us about the pathways into youth homelessness, the immense traumas young people experience as a result, and how to best support them to become safely and securely rehoused as quickly as possible.
Gaetz, O’Grady, Kidd, and Schwan (2016) have written that society’s failure to implement more effective strategies to address youth homelessness undermines these young people’s basic human rights. We need to work from an evidence-based framework that prioritizes human rights and equity while making changes to the way our social systems and institutions function (Nichols et al., 2017). Making this kind of change does not simply happen, but rather requires on-going and active commitment from people working in roles across society (Nichols, Schwan, Gaetz, & Redman, 2021). We conclude this section with a video of Dr. Naomi Nichols advocating for the rights of young people, as knowledgeable and autonomous decision makers.
In this video, Dr. Naomi Nichols argues that for a permanent solution to help youth exit homelessness we need policy and structural changes. She explains that factors such as long waitlists, a lack of affordable housing, and housing that does not match young people’s income levels all serve as barriers to successfully transitioning out of homelessness. Dr. Nichols concludes that we need better non-paternalistic systems for listening to young people, understanding their role as autonomous decision-makers who have rights, and working with them to define the most appropriate interventions. This video is 5:35 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: How can young people be supported to exit homelessness?
Want to learn more about how to support young people exiting homelessness? Check out the Homelessness Learning Hub links below!
Young people become homeless for very complex reasons, and experience considerable trauma while on the streets. Throughout this section, we looked at some of the ways to help support these youth as they transition out of homelessness and into secure housing. We saw that this is not something that happens overnight, but rather is a process marked by both progress forward and steps backward. What matters in this process, is that they be given the support they need to achieve financial security, social inclusion, and a redefined sense of identity that highlights their self-worth. We heard from multiple researchers that while housing is an important place to start, it must be accompanied by wrap-around supports such as through Housing First for youth. Which supports a young person receives will vary depending on their self-identified needs, but commonly include interventions aimed at improving mental health and/or issues with addictions. Here we learned about coordinated efforts that are being implemented in different cities to help young people address these issues as they transition out of homelessness.
There were three programmatic interventions that were routinely identified throughout this section. Upstream Canada is a preventive measure that is used to identify young people at risk of homelessness through school settings. However, while this program has shown promising outcomes, it is not yet widely implemented across the country. Family Reconnect is an early intervention program that is used to help repair family discord, where safe and possible, or rehouse a young person with extended family. We saw that while this intervention is effective, it may need to be broadened in scope, particularly for young people who identify as LGBTQ2S+. Finally, we have considered Housing First as a tailored intervention for helping young people become housed and have wrap-around supports based on choice and self-determination.
The foundation of success for all of these programs and interventions is that they consider young people to be rights-holders who are capable of making their own autonomous decisions. The best way we can support young people is to design our society in a way that prevents homelessness from occurring. When prevention fails, we must shift towards early intervention to get young people returned to family where safe to do so. As a very last resort, we should move young people into Housing First programs where they have wrap-around supports to meet their needs. Our current approach – of allowing young people to become homeless, experience trauma after trauma, and then wait to get them housed until after they are in crisis – is the worst possible scenario.
We began each section of this chapter with a story about a young man sleeping outside, using intravenous drugs, and living a difficult life in the summer of 2005. Unfortunately, we do not know what happened to him, but we like to believe the narrative that he got support, secured housing, and returned to school with the help of community agencies. While he may be out there today – living in a house, married with children, working a full-time job – he would still carry with him the scars of having been homeless as a young man. Let’s imagine instead that Upstream interventions were in place in his school, he was identified early, given support, and never was on the street to meet the author carrying the donuts. That would be the happy ending he deserves.
Click the link below to listen to all of the researchers answer the question “How can young people be supported to exit homelessness permanently?” in audio format on our podcast!
74
Enzo
At the beginning of the chapter, we met Enzo. He had been kicked out of his home following ongoing family disputes and disagreements. His acting out behaviour has provided challenges both in the home and in the youth shelter.
We need to ask ourselves:
Jake
We met Jake who is in the process, once again, of transitioning out of homelessness. He has a wrap around team working with him to increase his odds of success.
We need to ask ourselves:
Miriam
Miriam is a grade one student who teachers believe is living in a car with her family. Dr. Nichols discusses the “duty to report” obligation of the teachers and also speaks to the fact that the child welfare system in Canada needs to be fixed. Dr. Nichols discusses the link between time spent in the child welfare system and the probability of experiencing youth homelessness.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1186#h5p-87
75
We began this chapter on Child & Youth Studies by noting that leaving home is often a rite of passage that is celebrated in our society. Young adults leave home to attend school, get married, and/or purchase a home of their own. These are all milestone achievements. However, some youth leave or are pushed out of their homes in ways that are traumatic and have potentially life-altering implications.
At the start of the chapter, we introduced you to the composite characters Enzo, Jake, and Miriam, who were each young people experiencing homelessness in their own way. The scenarios were presented as an entry point into thinking about the complexity of youth homelessness. We returned to these individuals’ stories again at the end to demonstrate how they can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada.
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “Why do some young people become homeless?” Here we learned that the reasons are complex and often develop over a period of time. We considered the three different, yet inter-related aspects, that contribute to youth homelessness. These include interpersonal factors, such as discord within a young person’s family or school, structural issues that create inequities and discrimination, and systemic failures within institutions. It was clearly argued in this section that young people become homeless because society allows them to, such as through involvement with the child welfare system that acts as a common pathway onto the street. Rather than focusing on individual causes, we need to see the bigger picture of how our society creates the conditions that allow youth homelessness to occur.
Next we asked, “What are the challenges these young people face?” While the street may initially seem like a respite from a difficult environment, it soon reveals itself to be an extremely dangerous and exploitative place. Young people are often mistakenly thought to be dangerous and/or criminal offenders yet are actually at much higher risk of being victimized themselves. This risk is increased for some groups of youth based on factors such as being Indigenous, racialized, living with a disability, female-identified, and/or identifying as LGBTQ2S+. For young people, homelessness is a traumatic and stressful experience that forces them to constantly operate in survival mode. As they attempt to move off the streets and find stability, they often encourage barriers such as a lack of education, employment opportunities, and life skills needed for living independently. While they show remarkable personal strength, transitioning out of homelessness is a challenging process that takes time and hard work.
Finally, we asked, “How can young people be supported to exit homelessness permanently?” In this final section, we looked at ways to help these young people as they undertake this challenging work. We learned that rather than becoming instantly housed, it is often a process in which a youth moves back and forth, progressing towards increased independence and stability. Programmatic interventions, such as Upstream Canada can help to identify youth at risk of homelessness while they are in a school setting, but this has not yet been widely adopted. Family Reconnect can be used to help young people and their families work through challenges, but only if safe to do so. Housing First helps move young people into secure and appropriate housing, with wrap-around supports based on their self-identified needs. These interventions have all shown promising outcomes, based on the foundation that young people are rights-holders who are capable of making autonomous decisions regarding their own lives.
76
Here are some additional resources you may want to check out!
77
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
78
Abdel‐Baki, A., Aubin, D., Morisseau‐Guillot, R., Lal, S., Dupont, M., Bauco, P., … Iyer, S. N. (2019). Improving mental health services for homeless youth in downtown Montreal, Canada: Partnership between a local network and ACCESS Esprits ouverts (Open Minds), a national services transformation research initiative. Early Intervention in Psychiatry, 13(S1), 20–28. https://doi.org/10.1111/eip.12814
Abramovich, A., & Pang, N. (2020) Understanding LGBTQ2S youth homelessness in York Region. Toronto, ON. Report LGBTQ2S Youth in York Region
Abramovich, A., Pang, N., Moss, A., Logie, C. H., Chaiton, M., Kidd, S. A., & Hamilton, H. A. (2021). Investigating the impacts of COVID-19 among LGBTQ2S youth experiencing homelessness. PLOS ONE, 16(9): e0257693. https://doi.org/10.1371/journal.pone.0257693
Alberton, A. M., Angell, G. B., Gorey, K. M., & Grenier, S. (2020). Homelessness among Indigenous peoples in Canada: The impacts of child welfare involvement and educational achievement. Children and Youth Services Review, 111, 104846–. https://doi.org/10.1016/j.childyouth.2020.104846
Alschech, J., Taiwo-Hanna, T., & Shier, M. L. (2020). Navigating peer-influences in a large youth homeless shelter in North America. Children and Youth Services Review, 108, 104665–. https://doi.org/10.1016/j.childyouth.2019.104665
Baker Collins, S., Schormans, A. F., Watt, L., Idems, B., & Wilson, T. (2018). The invisibility of disability for homeless youth. Journal of Social Distress and the Homeless, 27(2), 99–109. https://doi.org/10.1080/10530789.2018.1480892
Baker Collins, S., & Fudge Schormans, A. (2021). Making visible the prevalence of self-identified disability among youth experiencing homelessness. Journal of Social Distress and Homelessness. https://doi.org/10.1080/10530789.2021.1940719
Barbic, S. P., Jones, A. A., Woodward, M., Piercy, M., Mathias, S., Vila-Rodriguez, F., … Honer, W. G. (2018). Clinical and functional characteristics of young adults living in single room occupancy housing: preliminary findings from a 10-year longitudinal study. Canadian Journal of Public Health, 109(2), 204–214. https://doi.org/10.17269/s41997-018-0087-9
Barker, B., Kerr, T., Dong, H., Wood, E., & DeBeck, K. (2017). High school incompletion and childhood maltreatment among street‐involved young people in Vancouver, Canada. Health & Social Care in the Community, 25(2), 378–384. https://doi.org/10.1111/hsc.12314
Barker, B., Shoveller, J., Grant, C., Kerr, T., & DeBeck, K. (2020). Long-term benefits of providing transitional services to youth aging-out of the child welfare system: Evidence from a cohort of young people who use drugs in Vancouver, Canada. The International Journal of Drug Policy, 85, 102912–102912. https://doi.org/10.1016/j.drugpo.2020.102912
Barone, C., Yamamoto, A., Richardson, C. G., Zivanovic, R., Lin, D., & Mathias, S. (2019). Examining patterns of cognitive impairment among homeless and precariously housed urban youth. Journal of Adolescence, 72, 64–69. https://doi.org/10.1016/j.adolescence.2019.02.011
Barrow, S. K. (2018). Scholarship review of queer youth homelessness in Canada and the United States. The American Review of Canadian Studies, 48(4), 415–431. https://doi.org/10.1080/02722011.2018.1531603
Begun, S. (2019). The association between social capital and pregnancy attitudes among youth experiencing homelessness. Journal of Obstetrics and Gynaecology Canada, 41(5), 710–710. https://doi.org/10.1016/j.jogc.2019.02.159
Brown, E. L., Phillippo, K. L., Weston, K., & Rodger, S. (2019). United States and Canada pre-service teacher certification standards for student mental health: A comparative case study. Teaching and Teacher Education, 80, 71–82. https://doi.org/10.1016/j.tate.2018.12.015
Buccieri, K. (2019). “My brother was his little angel; I was the problem child”: Perceived sibling favoritism in the narratives of youth who become homeless. Journal of Family Issues, 40(11), 1419–1437. https://doi.org/10.1177/0192513X19839748
Canadian Observatory on Homelessness. (2016). Canadian Definition of Youth Homelessness. Canada: Canadian Observatory on Homelessness.
Chan, E., & Huys, J. (2017). Addressing the legal needs of LGBTQ2S youth experiencing homelessness. In A. Abramovich, & J. Shelton (eds.), Where Am I Going to Go? Intersectional Approaches to Ending LGBTQ2S Youth Homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Côté, P.-B. (2019). Sexual health services for homeless youth: A qualitative analysis of their experiences. Journal of Social Service Research, 45(3), 429–443. https://doi.org/10.1080/01488376.2018.1480568
Cully, L., Wu, Q., & Slesnick, N. (2018). Ecologically based family therapy for adolescents who have left home. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Doré-Gauthier, V., Côté, H., Jutras-Aswad, D., Ouellet-Plamondon, C., & Abdel-Baki, A. (2019). How to help homeless youth suffering from first episode psychosis and substance use disorders? The creation of a new intensive outreach intervention team. Psychiatry Research, 273, 603–612. https://doi.org/10.1016/j.psychres.2019.01.076
Frederick, T. (2019). ‘A person like me’: identity narratives, dual process theories, and subsistence related decision-making among young people experiencing homelessness, Journal of Youth Studies, 22(8), 1083-1100. 10.1080/13676261.2018.1563674
Frederick, T., Vitopoulos, N., Leon, S., & Kidd, S. (2021). Subjective housing stability in the transition away from homelessness. Journal of Community Psychology. Early view. https://doi.org/10.1002/jcop.22702
Gaetz, S. (2018). Reflections from Canada: Can research contribute to better responses to youth homelessness? Cityscape, 20(3), 139–146. Cityscape – Volume 20 Number 3 (huduser.gov)
Gaetz, S., O’Grady, B., Kidd, S., & Schwan, K. (2016). Without a home: The national youth homelessness survey. Toronto: Canadian Observatory on Homelessness Press
Gaetz, S., Schwan, K., Redman, M., French, D., & Dej, E. (2018). The roadmap for the prevention of youth homelessness – executive summary. A. Buchnea (Ed.). Toronto, ON: Canadian Observatory on Homelessness Press.
Gaetz, S., Ward, A., & Kimura, L. (2019). Youth homelessness and housing stability: What outcomes should we be looking for? Healthcare Management Forum, 32(2), 73–77. https://doi.org/10.1177/0840470418817333
Goldman-Hasbun, J., Nosova, E., DeBeck, K., Dahlby, L., & Kerr, T. (2019). Food insufficiency is associated with depression among street-involved youth in a Canadian setting. Public Health Nutrition, 22(1), 115–121. https://doi.org/10.1017/S1368980018002574
Joly, L. E., & Connolly, J. (2019). It can be beautiful or destructive: Street-involved youth’s perceptions of their romantic relationships and resilience. Journal of Adolescence, 70, 43–52. https://doi.org/10.1016/j.adolescence.2018.11.006
Jones, T., & Ellis, J. (2017). It’s a kiki…. In A. Abramovich, & J. Shelton (eds.), Where Am I Going to Go? Intersectional Approaches to Ending LGBTQ2S Youth Homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Karabanow, J., Hughes, J., Kidd, S., & Frederick, T. (2018). Homeless youth and the search for stability. Wilfrid Laurier University Press. Project MUSE
Karamouzian, M., Cheng, T., Nosova, E., Sedgemore, K., Shoveller, J., Kerr, T., & Debeck, K. (2019). Perceived devaluation among a cohort of street-involved youth in Vancouver, Canada. Substance Use & Misuse, 54(2), 324–330. https://doi.org/10.1080/10826084.2018.1523193
Kidd, S. A., Gaetz, S., O’Grady, B., Schwan, K., Zhao, H., Lopes, K., & Wang, W. (2021). The second national Canadian homeless youth survey: Mental health and addiction findings. Canadian Journal of Psychiatry. https://doi.org/10.1177/0706743721990310
Kidd, S. A., Vitopoulos, N., Frederick, T., Daley, M., Peters, K., Clarc, K., … McKenzie, K. (2019a). Peer support in the homeless youth context: Requirements, design, and outcomes. Child & Adolescent Social Work Journal, 36(6), 641–654. https://doi.org/10.1007/s10560-019-00610-1
Kidd, S. A., Vitopoulos, N., Frederick, T., Leon, S., Karabanow, J., & McKenzie, K. (2019b). More than four walls and a roof needed: A complex tertiary prevention approach for recently homeless youth. American Journal of Orthopsychiatry, 89(2), 248–257. https://doi.org/10.1037/ort0000335
Kidd, S. A., Vitopoulos, N., Frederick, T., Leon, S., Wang, W., Mushquash, C., & McKenzie, K. (2020). Trialing the feasibility of a critical time intervention for youth transitioning out of homelessness. American Journal of Orthopsychiatry, 90(5), 535–545. https://doi.org/10.1037/ort0000454
Kozloff, N., Bergmans, Y., Snider, C., Langley, J., & Stergiopoulos, V. (2018). Crisis response with street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Luongo, N. M. (2018). Disappearing in plain sight: An exploratory study of co-occurring eating and substance abuse dis/orders among homeless youth in Vancouver, Canada. Women’s Studies International Forum, 67, 38–44. https://doi.org/10.1016/j.wsif.2018.01.003
Malla, A., Iyer, S., Shah, J., Joober, R., Boksa, P., Lal, S., … Vallianatos, H. (2019). Canadian response to need for transformation of youth mental health services: ACCESS Open Minds (Esprits ouverts). Early Intervention in Psychiatry, 13(3), 697–706. https://doi.org/10.1111/eip.12772
Morisseau-Guillot, R., Aubin, D., Deschênes, J.-M., Gioia, M., Malla, A., Bauco, P., … Abdel-Baki, A. (2020). A promising route towards improvement of homeless young people’s access to mental health services: The creation and evolution of an outreach service network in Montréal. Community Mental Health Journal, 56(2), 258–270. https://doi.org/10.1007/s10597-019-00456-y
Nichols, N. (2019). Youth, school, and community: Participatory institutional ethnographies. Toronto: University of Toronto Press. https://doi.org/10.3138/9781487517724
Nichols, N., Schwan, K., Gaetz, S., & Redman, M. (2021). Enabling evidence-led collaborative systems-change efforts: An adaption of the collective impact approach. Community Development Journal. https://doi.org/10.1093/cdj/bsab011
Nichols, N., Schwan, K., Gaetz, S., Redman, M., French, D., Kidd, S., O’Grady, B. (2017). Child welfare and youth homelessness in Canada: A proposal for action. Toronto: Canadian Observatory on Homelessness Press.
O’Grady, B., Kidd, S., & Gaetz, S. (2020). Youth homelessness and self identity: a view from Canada. Journal of Youth Studies, 23(4), 499–510. https://doi.org/10.1080/13676261.2019.1621997
Parpouchi, M., Moniruzzaman, A., & Somers, J. M. (2021). The association between experiencing homelessness in childhood or youth and adult housing stability in housing first. BMC Psychiatry, 21(1), 138–138. https://doi.org/10.1186/s12888-021-03142-0
Rodger, S., Bird, R., Hibbert, K., Johnson, A. M., Specht, J., & Wathen, C. N. (2020). Initial teacher education and trauma and violence informed care in the classroom: Preliminary results from an online teacher education course. Psychology in the Schools, 57(12), 1798–1814. https://doi.org/10.1002/pits.22373
Rogers, T., & Shafer, R. (2018). Addressing homelessness in our schools and language arts classrooms. Language Arts, 96(2), 102–112. National Council of Teachers of English (ncte.org)
Sohn, J. & Gaetz, S. (2020). Upstream Canada: An early intervention strategy to prevent youth homelessness & school disengagement. Toronto: Canadian Observatory on Homelessness Press.
Sylvestre, J., Klodawsky, F., Gogosis, E., Ecker, J., Polillo, A., Czechowski, K., … Hwang, S. (2018). Perceptions of housing and shelter among people with histories of unstable housing in three cities in Canada: A qualitative study. American Journal of Community Psychology, 61(3-4), 445–458. https://doi.org/10.1002/ajcp.12243
Thulien, N. S., Gastaldo, D., Hwang, S. W., & McCay, E. (2018). The elusive goal of social integration: A critical examination of the socio-economic and psychosocial consequences experienced by homeless young people who obtain housing. Canadian Journal of Public Health, 109(1), 89–98. https://doi.org/10.17269/s41997-018-0029-6
Thulien, N. S., Gastaldo, D., McCay, E., & Hwang, S. W. (2019a). “I want to be able to show everyone that it is possible to go from being nothing in the world to being something”: Identity as a determinant of social integration. Children and Youth Services Review, 96, 118–126. https://doi.org/10.1016/j.childyouth.2018.11.005
Thulien, N. S., Kozloff, N., McCay, E., Nisenbaum, R., Wang, A., & Hwang, S. W. (2019b). Evaluating the effects of a rent subsidy and mentoring intervention for youth transitioning out of homelessness: Protocol for a mixed methods, community-based pilot randomized controlled trial. JMIR Research Protocols, 8(12), e15557–e15557. https://doi.org/10.2196/15557
Vitopoulos, N., Cerswell Kielburger, L., Frederick, T., & Kidd, S. (2018a). Developing a trauma-informed mental health group intervention for youth transitioning out of homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Vitopoulos, N. A., Frederick, T. J., Leon, S., Daley, M., McDonald, C., Morales, S., … Kidd, S. A. (2018b). Development of a complex tertiary prevention intervention for the transition out of youth homelessness. Children and Youth Services Review, 94, 579–588. https://doi.org/10.1016/j.childyouth.2018.08.038
VIII

Social Sciences help us understand the various roles and impacts of people in society. While there are many subjects within the Social Sciences, this part contains chapters on Sociology & Crimino-Legal Studies, and Social Work. As you work through these chapters you are encouraged to think about what these disciplines can add to our understanding of homelessness in Canada.
Perhaps as you read this, you are considering a career that relates to the Social Sciences, such as a Social Policy Analyst, Police Officer, Lawyer, or Social Worker. The chapters in this section are designed to help you think critically about some of the questions you may encounter in these fields of employment. Understanding homelessness will help you navigate situations and choices you may have to make. Consider for example a scenario in which you are a Social Policy Analyst who must decide whether to recommend implementing a by-law that bans sleeping in a public park after 10pm. The choice you make will be influenced by your understanding of the by-law’s impact. This choice will also influence decisions that have to be made by Police Officers [such as whether to use discretion not to issue a ticket under the by-law], Lawyers [such as whether to take the case of a client who faces jail time for not paying these tickets and does not have money to pay for representation], and Social Workers [such as how to help the client navigate the legal and justice systems].
Before you begin, pause to consider how you would respond in each of the roles of the scenario above. With the knowledge you currently have about homelessness in Canada, would you recommend implementing a by-law that bans sleeping in the park at night? Would you issue a ticket if you were a Police Officer who came across someone sleeping in the park? Would you take their case, if you were a Lawyer and a person who was ticketed came to you for help but could not pay for your services? If you were a Social Worker and had limited resources, where would you go to connect your client with community legal supports?
You are encouraged to keep this scenario in your mind as you read through the next two chapters and ask yourself whether any of your responses change, or are reaffirmed, after learning more about what the Social Sciences can teach us about homelessness in Canada.
VIII

On the evening of July 29, 2015, CBS New York broke an ‘exclusive’ story. According to the journalists covering the event, “It was a shocking scene at one of the city’s most visited landmarks” (CBSNewYork, 2015). A reporter was on scene to interview witnesses and report live updates, relaying details to the anchors sitting in shock at the studio’s news desk. The reason for the exclusive news story?
Take a moment to stop and reflect on what you just watched. How did it make you feel? Was there anything about it that you found shocking? The story, “Exclusive: Photos show homeless man taking bath in Columbus Circle fountain” is indeed shocking, but not for the reasons the journalists think. What this video shows us is a man who is in need of basic necessities of life – privacy, bathing facilities, and compassion. While quality of life is made out to be an issue, this story fails to ask the question “whose quality of life is at stake?”
79
In this chapter, you are invited to think about how homelessness is a social issue that plays out in public. Like the man in the fountain, homelessness is often on display because people lack a private space in which to bathe, eat, sleep, and generally just live. While considering homelessness as a public social issue, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind people who experience homelessness often engage in private acts in public not because they want to, but because they lack a private space in which to go. Punishing people for bathing in public is essentially punishing them for not having a home. Read on to learn more about street-involvement, the resulting criminalization of homelessness, and alternate measures that we can take up within communities to improve quality of life for all residents.
80
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to Sociology and Crimino-Legal Studies. As you work through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After considering the real-world scenario, we will endeavour to answer each question posed in the learning objectives. Are all people who experience homelessness street-involved? What is the criminalization of homelessness? How can communities implement better support programs? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
81
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider this person’s experience.
Susan
Susan is a 32-year-old who has been living in a boarding house in a small town with five other women. She is not close to any of the other residents and has kept very much to herself trying to stay “under the radar.” She has not felt safe in the residence due to the level of discord among the women and the rowdy traffic in and out of the apartment building next door which is a known drug house. There have been frequent visits from the local police who have continuously stopped her to ask her what she is doing and where she is going. In the last few weeks, a cruiser has been parked on the street outside the boarding house for numerous days in a row.Prior to living in the boarding house, Susan was incarcerated for eight months after being convicted of theft. She was released from the local corrections centre 4 months ago to the community. She left the facility with nothing. She is not from this community and does not have the means to get back to her hometown. Living in a shelter was not an option as there simply isn’t one available.
She is currently on probation and must meet with her probation officer weekly. She has been ill, and without access to a reliable phone to let her work know, she was fired from her job at a local coffee shop. In addition, she was unable to let the court officials know about her illness and now is in breach of a request to be fingerprinted, has missed a court appearance, and has missed one probation meeting. There is now a bench warrant out for her arrest. She has had no idea what type of legal support there might be for her in this small town. Susan recently lost her room due to unpaid rent. She has been forced to sleep in garages and sheds. She has been contemplating sex trade work to survive. Last night she was arrested for breaking and entering having sought shelter from a driving rain.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to the scenario again at the end of the chapter.
Reflection Questions
82
Our understanding of the “street” as a social space has been greatly influenced by the Chicago School of Sociology. Prevalent in the early 1900s, researchers at the University of Chicago like W. I. Thomas, Ernest Burgess, and Robert Park undertook a unique approach now commonly called urban ethnography. These researchers were interested in documenting the daily activities of people deemed to be transgressive in public spaces. They would watch and record what they saw occurring within groups such as people living in extreme poverty, those who were new immigrants, and/or those involved in gangs.
Among the most influential of the Chicago School researchers was Nels Anderson (1923), whose research on hobos provided early insight into how the street can become a shared space for people without secure housing. His work on hobos, people who would ride the railways in search of work, provides a rich and detailed description of what life was like for these individuals in the early 1900s. We can still see some similarities today, with modern tent encampments serving as a modern version of the hobo jungles. However, much has also changed in the time since Nels Anderson was writing. Before you continue through the material in this section, we encourage you to pause and reflect on the question of whether all people who experience homelessness are street-involved and what “the street” even means. You may write your responses in the space below.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=744#h5p-76
When we write about the street, we are referring to a shared urban landscape made up of marginal spaces that exist outside the mainstream and are guided by a set of social practices. For instance, we might think of a downtown core in a city as being part of a street landscape that has spaces such as emergency shelters, drop-in centres, food banks, and a community health centre. While these services are commonly located in busy areas of a city, they are not often visited by the general public. In this way, we can consider them to be part of the street that have their own cultures and social practices that occur within. As people within these spaces move between them and into other public places, like sidewalks and city parks, a street network develops.
The question of whether all people who experience homelessness are part of this street network (i.e. street-involved) requires that we return to the very first question posed within this book and reconsider what homelessness means. In the Introduction chapter we discussed the Canadian Definition of Homelessness as being a four-part typology in which people can be unsheltered, emergency sheltered, provisionally accommodated, or at-risk of homelessness (Gaetz et al., 2012). This definition is important to return to here because it helps us see that not everyone who experiences homelessness lives in public spaces, accesses emergency shelters, or is part of the urban street landscape. In the next two videos, Dr. Erin Dej and Dr. Bernie Pauly explain further.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Erin Dej argues that not everyone who experiences homelessness is street-involved. She points to the Canadian definition of homelessness as a four-part typology that offers a broader understanding of homelessness, with people who are visibly unsheltered being the tip of the iceberg. Dr. Dej notes that while we need to ensure unsheltered individuals are supported and safe, we must also remember to attend to the full spectrum of experiences and focus on homelessness prevention. This video is 1:50 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: Are all people who experience homelessness street-involved?
In this video Dr. Bernadette [Bernie] Pauly explains that there is a diverse range of ways in which people experience homelessness, with some being more visible than others. She draws upon the Canadian definition of homelessness, which includes people who are unsheltered and visibly sleeping in public places like doorways, alleys, and parks, as well as people who may be in emergency shelters, provisional accommodations, or at-risk of homelessness. Dr. Pauly concludes by noting that media depictions are part of the issue. They commonly portray narrow stereotypes of homelessness as someone sleeping on a sidewalk, rather than showing more complex circumstances such as someone living in a shelter and going to work every day. This video is 2:41 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: Are all people who experience homelessness street-involved?
Consider the images of homelessness you have seen represented in the media. What comes to mind? Do you think these images show the diversity of people’s experiences of homelessness in Canada? If not, what is missing?
The street is commonly thought of as an urban space, meaning it is constituted by people located in cities. Homelessness looks very different outside of the city. When we ask ourselves whether all people who experience homelessness are street-involved, we have to consider the definition of homelessness and we also have to consider the geographic context. Many people experience homelessness in rural communities where the idea of the street is less applicable. Homelessness is often invisible in rural settings (MacDonald & Gaulin, 2020) as people may move between temporary accommodations and/or sleep in remote areas that are not well travelled. People living in urban areas are more likely to see individuals experiencing homelessness on a frequent basis, compared to those in rural and suburban areas (Doberstein & Smith, 2019a) which may result in rural homelessness being overlooked as a pressing social issue. We encourage you to consider the similarities and differences between rural and urban homelessness as you watch this brief video about people living in Wetaskiwin Alberta.
The research presents an alarming picture of rural homelessness. For instance, Pijl and Belanger (2021) conducted a study in a small Alberta prairie town and found that Indigenous participants were particularly likely to report couch-surfing, 88% of female participants had left their home at least once as the result of intimate partner violence, and over half reported having great difficulty paying the previous year’s housing costs. Homelessness exists in both urban and rural environments, but the experience is often different in each setting. Dr. Bill O’Grady has researched rural homelessness in Canada. In the next video he explains further the importance of context.
In this video Dr. William [Bill] O’Grady argues that to understand whether people who experience homelessness are street-involved, it is helpful to consider the different types of homelessness that exist. He notes that we must think about people who are at-risk of homelessness, couch surfing, and staying in shelters or outside, to understand why some people are street-involved while others are not. Dr. O’Grady explains that when we talk about street-involvement often we are referring to urban homelessness, but that being street-involved looks very different in rural communities. He shares an analysis of the 2014 General Social Survey which found people in rural communities report higher levels of lifetime homelessness than those living in larger cities. Dr. O’Grady concludes that we must consider the types of homelessness and the context to understand street-involvement. This video is 3:57 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: Are all people who experience homelessness street-involved?
The move between rural and urban areas has been described as a constant push and pull by Pijl and Belanger (2021) who found that Indigenous participants within their study were hyper-mobile between the reserve and larger neighbouring towns. In the next video Dr. Rebecca Schiff (2021), co-editor of “Health and health care in northern Canada,” discusses the challenges of rural homelessness and how we need to think about supporting people where they are, so they do not have to engage in this migratory cycle.
In this video, Dr. Rebecca Schiff argues that rural homelessness is under-recognized in Canada and is a much more significant issue than many people realize. She explains that rates of homelessness are higher in rural communities and that they face additional challenges, such as high costs of energy, heating, and food in addition to housing. Dr. Schiff notes that we need to consider how policy and funding approaches are currently designed toward the bias of urban homelessness, and that it is critical we identify ways to support people’s diverse needs in rural communities, so they do not have to migrate back and forth between rural and urban centres. Dr. Schiff concludes by advocating for prevention and early intervention for youth in rural communities, so they do not experience recurrent episodes of homelessness throughout their lives. This video is 7:10 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: Homelessness in rural communities
Research on rural homelessness has shown that the lack of privacy in small communities, limited support services, and a generally limited housing stock creates unique challenges for overcoming homelessness (Buck-McFadyen, 2021). There also may be less willingness to invest in supporting and expanding homelessness investments in rural areas compared to medium sized and large cities (Doberstein & Smith, 2019a). The unique challenges and lack of financial investments make rural homelessness a distinct experience from urban street-involved homelessness. We saw these clear challenges arise in rural areas during the COVID-19 pandemic. In this section’s featured reading Dr. Rebecca Schiff and her team (2020) explore the impact of COVID-19 on people experiencing homelessness in rural and remote communities.
Schiff, R., Buccieri, K., Waegemakers Schiff, J., Kauppi, C., & Riva, M. (2020). COVID-19 and pandemic planning in the context of rural and remote homelessness. Canadian Journal of Public Health, 111, 967-970.
When we consider the question of whether all people who experience homelessness are street-involved, it is important that we recognize the different types of homelessness and locations in which it occurs. Sometimes, as we have seen, people in rural communities will migrate into urban settings for services and opportunities that are not available where they live. They may then also return back to the rural community again. People who experience homelessness are often mobile and their departures may at times seem abrupt, as though they were a missing person (Huey & Ferguson, 2020). The idea of mobility being associated with homelessness traces back a long time, even before the hobos riding the rails that Nels Anderson wrote about in 1923. People who experience homelessness may move between regions for a diverse number of reasons, including for interpersonal opportunities, seeking health care and social services, and for personal security (Kaufman et al., 2020a). In the next video, Dr. Jacqueline Kennelly explains how these moves lead to fluid experiences of street-involvement.
In this video, Dr. Jacqueline Kennelly argues that not every person who experiences homelessness is street-involved and that even those who are, tend to move in and out of street-involvement fluidly. She notes that men are more likely to be visible on the streets, whether panhandling or sleeping outside, while women, girls, and families often remain more hidden. This video is 1:22 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Are all people who experience homelessness street-involved?
In urban settings, street involvement is often organized around access to services and economic activities. People find creative and intentional strategies for navigating street life, including recognizing opportunities, mobilizing their resources, using social connections and skills, and engaging in entrepreneurial processes (Isaak, Reynolds, Sareen, & Distasio, 2019). Within the context of urban settings, people who are street-involved may use informal money–making strategies like panhandling or squeegeeing car windshields in exchange for payment. These income strategies are more likely to be used in large cities, like Vancouver and Toronto, where daily encounters with people experiencing homelessness are much more common than in rural and suburban settings (Doberstein & Smith, 2019a). In the next video, Dr. Jeff Karabanow discusses rural homelessness, urban street involvement, and the youth cultures that can develop on the street.
In this video, Dr. Jeff Karabanow explains that street involvement denotes engagement with activities such as panhandling, squeegeeing, and living rough. He notes that a core response to youth homelessness has been to create youth shelters that are distinct from adult-serving ones, but that many young people still remain connected to the street, where they must navigate day-to-day encounters with others. Dr. Karabanow explains that in rural communities there is less street-involvement, as couch surfing and hidden homelessness are more common. He concludes that in recent years a shift towards prevention has occurred in which the emphasis is on keeping people off the streets and out of homelessness. This video is 3:14 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: Are all people who experience homelessness street-involved?
Just as people who experience homelessness may move between geographic locations, they also often have to move around throughout the day as emergency shelters and social services open and close. This kind of movement creates a social geography of the street. One of the authors of this book has conducted research on the social and spatial dimensions of homelessness using time geography mapping to see how young people without secure housing move through the street over a 24–hour period. While it may seem to the general public that people who experience homelessness are sitting on the sidewalk, in the park, or outside of an agency with nowhere to go, this mapping activity actually demonstrates their movements are rather controlled. They must attune their actions to the service agencies they depend upon.
Consider how you spent the past 24–hours and create a mental map of where you went, the times, and the modes of transportation you used. How do you think this activity might look for a young person who is couch–surfing in the suburbs while using services in the downtown core of Toronto? How might this activity look for a person couch–surfing in a rural community?
We encourage you to keep these questions in mind as you watch this brief video created by the Public Visualization Studio. This video was created based on the 24–hour map of “Anna” a real woman (although not her real name) who was experiencing homelessness in Toronto. They created a visual representation of this research as part of the “In the Air Tonight” month-long interactive architecture installation by projecting it on the side of a building in downtown Toronto on a continuous loop. There is no sound in the video, so we invite you to use the quiet time to reflect on how being street-involved requires spatial work and coordination.
Some people experience homelessness in a way that brings them into the street environment, such as accessing shelters and social services. Dr. Tyler Frederick (2019) has conducted interviews with 39 young people to learn about their experiences within these environments and the cultures that develop within the spaces. His research shows that by spending time on the street, young people develop strategies for navigating the rules, opportunities, and social politics of the different spaces they access, while still struggling to meet their basic needs. In the next video, Dr. Frederick speaks about the different ways the street is conceptualized and the social world that develops around it.
In this video, Dr. Tyler Frederick explains that the term street-involved is sometimes used broadly to refer to people experiencing homelessness, but that it is important to remember not everyone who experiences homelessness is involved in street-based activities. He clarifies that more narrowly, street-involvement refers to people who are sleeping rough, living in an encampment or their car, and are involved in a wider social network of other street-involved individuals. Dr. Frederick notes that shelters and drop-in services are often surrounded by a social world where people form relationships, whether positive or risky, that may continue after they are housed. This video is 3:00 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: Are all people who experience homelessness street-involved?
People commonly equate homelessness with living on the street, but the two are not necessarily synonymous. We began this section by tracing research about homelessness in Sociology to the Chicago School and Nels Anderson’s work on hobos in the 1920s. This is important to note because it set the stage for the urban ethnography style of research that followed, in which people were observed living their lives in public spaces. This tradition has continued to the modern day but has also been expanded to allow for broader understandings of homelessness.
We heard from researchers that the Canadian definition of homelessness is important because it provides a conceptualization of homelessness as being a continuum rather than an ‘either / or’ occurrence (Gaetz et al., 2012). We noted that some people, such as those who are unsheltered or emergency sheltered, might be more visible and likely to engage in street culture to meet their needs. Those in rural settings are more removed from the street, as these communities generally lack the centralized infrastructure to create a hub of services. People in these communities may migrate in a cyclical form back and forth between rural and urban settings, in an attempt to improve their economic, housing, and/or social situations.
Just as people move between rural and urban settings, so too do people move on and off the street based on their personal circumstances. We heard that it is not uncommon for people to move fluidly through the street, as they experience different forms of homelessness, and that they may move in and out of services throughout the day. This movement creates a geography of the street that shows how constraining street-involvement can actually be. We concluded this section by discussing some of the economic activities, like panhandling and squeegeeing, that are more common in urban than rural environments and the street cultures that are produced by the people who engage in them.
Click the link below to listen to all of the researchers answer the question “Are all people who experience homelessness street involved?” in audio format on our podcast!
83
We opened this chapter with a news clip of a man bathing in a public fountain and receiving media attention for disturbing the wealthier people who lived nearby. In this incident, police were called and there were mayoral promises to remove “emotionally disturbed” people from the streets. This news clip is a clear example of the transgressive nature of engaging in private behaviour in public spaces, that elicits a strong reaction. On the one hand, we can think of a response that is grounded in human rights and social justice-based practices. A response of this nature would entail speaking to the man as a human being, treating him with respect, asking him what he needs, and helping to connect him with supports in the community. The opposite response is the criminalization of homelessness. This is what we saw in the news video, as bathing in the fountain was not understood as an expression of need (for housing, privacy, and hygiene facilities) but rather as an act that needed to be “corrected” with legal measures. Based on this understanding, what you do think is meant by the criminalization of homelessness? Use the space below to record your thoughts before continuing through the material in this section.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=746#h5p-77
The government can respond to homelessness in a supportive way or in a punitive way. We have seen, for instance, in the chapter on Politics, Policy, & Housing in Canadathat Housing First was introduced as a person-centered approach that focuses on housing people and then providing wrap-around supports based on what the person themselves identifies needing. Conversely, governments sometimes implement policies and laws that penalize people for their lack of housing through measures like ticketing them for panhandling or being in a park late at night. We begin this section with a video in which Dr. Jonathan Greene discusses the two contrasting approaches and argues it is the government’s legal obligation to recognize and protect human rights.
In this video, Dr. Jonathan Greene explores the two approaches states use for dealing with homelessness. One way, he notes, is through providing supports and programs such as Housing First. The other way is by enforcing state mechanisms to move people who are visibly experiencing homelessness out of public view. Dr. Greene argues that removing these individuals from public view affects how we as a society understand homelessness. He explains that we need to consider issues of enforcement, such as tearing down encampments, in relation to human rights. These include the right to use public space in ways that may not be socially approved, and the right to be homeless in the way one chooses in the absence of safe, adequate, and secure housing alternatives. Dr. Greene concludes by discussing a legal decision from the United States that says if a city cannot provide shelter for people experiencing homelessness, they do not have the right to subsequently criminalize them. This video is 5:10 in length and has closed captions available in English.
Key Takeaways – Dr. Jonathan Greene: The different ways of managing homelessness
There are many common stereotypes associated with people experiencing homelessness, such as that they are mentally ill, dangerous, and/or commit high rates of crime. While there is some research that shows a connection between childhood trauma and violence (Baron & Forde, 2020) and increased rates of property crime around shelters (Faraji, Ridgeway, & Wu, 2018) there is also research that shows people who experience homelessness with complex psychosocial histories do not have many criminal charges against them (Lemieux, Leclair, Roy, Nicholls, & Crocker, 2020). It may (or may not) surprise you to learn that people who experience homelessness are actually much more likely to be victims of crime, in large part because they tend to be socially and physically isolated from others. However, despite being a population at risk of victimization, people who experience homelessness are much more likely to be treated as criminals. In the next video Dr. Sean Kidd explains further.
In this video, Dr. Sean Kidd argues that criminalizing homelessness is the outcome of our society’s tendency to stigmatize and label people who experience homelessness as being dangerous. He notes that there are policies and laws that serve to formally criminalize people, such as provincial Safe Streets Acts, that allow for ticketing people who are panhandling in public. Dr. Kidd explains that there are also informal methods of criminalization, such as through the additional attention people experiencing homelessness receive from police and security guards. He notes that these encounters may result in charges for loitering, vagrancy, or trespass. Dr. Kidd concludes that the long-term outcomes of criminalization can serve as barriers to exiting homelessness, such as by limiting access to housing and employment, and producing a record of incarceration that emerges in job searches. This video is 3:13 in length and has closed captions available in English.
Key Takeaways – Dr. Sean Kidd: What is the criminalization of homelessness?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=746#h5p-78
The criminalization of homelessness occurs in many ways. The slides below provide a brief summary of the six facets identified by O’Grady, Gaetz, & Buccieri (2011) in the report, “Can I see your ID? The policing of youth homelessness in Toronto.” This report was created in partnership with the organization Justice for Children and Youth and the slides help set the stage for the remainder of this section, as we explore what the criminalization of homelessness means and how it is enacted.
Click the forward arrow to view all 5 slides in the course presentation below.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=746#h5p-43
One of the most prominent examples of criminalizing homelessness is the increased attention people receive from police when they are visible on the street. We saw this, for instance, with the video of the man in the fountain. Police targeting or profiling occurs primarily for those who are more street-involved than hidden. Recall from the previous section that not all individuals who experience homelessness are street-involved but that those who are, tend to be visible and engaging in money making activities like panhandling and squeegeeing in highly populated urban spaces. The visible nature of this kind of homelessness draws increased police attention and response.
People who are visibly homeless receive increased police attention not because of their actions, but because of where they are doing them. For instance, bathing is not an action that draws police notice but bathing in a fountain does. Drinking beer with friends in a private residence does not generally attract police attention but drinking in a public park does. In a study of 547 adults who were experiencing homelessness and had mental illness, Kouyoumdjian et al., (2019) found that in the year before the study 56% of the participants had police interactions and that the odds of interacting with the police was 47% higher for people who were homeless than housed. Further, the reasons for these police interactions were for acts of daily living (like showering), being victimized, mental health assessments, and suicidal behaviour (Kouyoumdjian et al., 2019). These findings show that there are increased police encounters and that they are not related to criminal behaviours.
Increased police interactions can have negative implications for people who experience homelessness. For instance, they may fear calling the police or emergency services if they are a person who uses drugs and are experiencing, or with someone experiencing, a drug overdose (Collins et al., 2019). For young people, in particular, coming into contact with the law has long-term repercussions that continue even after they have left the streets (Quirouette, Frederick, Hughes, Karabanow, & Kidd, 2016). Young people may find themselves trapped by circumstances that are created by the state’s response of criminalizing homelessness and increasing police enforcement (Fast & Cunningham, 2018). In the next two videos we see this clearly as Dr. Jacqueline Kennelly and Dr. Tyler Frederick, both researchers who focus on youth homelessness, each independently discuss the snowball effect police interactions have on these young people.
In this video, Dr. Jacqueline Kennelly argues that people experiencing homelessness, such as youth, are disproportionately targeted by police because they are visible on the streets. She notes that these individuals often get an accumulation of minor charges that convert into criminal sentences, records, and jail time. Dr. Kennelly warns that young people leaving correctional institutions are vulnerable to getting caught in a snowball effect, in that they are imprisoned and then released with no housing or money and end up continuing their experience of homelessness. This video is 1:11 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: What is the criminalization of homelessness?
In this video, Dr. Tyler Frederick explains that social profiling, like racial profiling, is the idea that certain people have visible markers or characteristics that increase police attention and interest in them. He notes these individuals have higher rates of police contact, not because they commit crime but because they are deemed to be out of place, such as youth congregating in the park or a person who appears to use drugs. Dr. Frederick argues that once a person is criminalized there is a snowball effect that can result in them receiving charges and having their liberty taken away even before they are found guilty of any offense. As a result, some people who are street-involved in urban settings develop a skill for blending in and not attracting police attention. This video is 6:13 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: Criminalization through social profiling
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=746#h5p-79
Police interactions with people who appear visibly homeless and/or experiencing mental illness need to be framed within larger structural issues related to the lack of affordable housing, people living in extreme poverty, and the associated stigmas that they face (Frederick, O’Connor, & Koziarski, 2018). Additionally, factors such as race, gender, and class intersect in ways that may diminish a person’s belief that the police are fair and equitable in their practices (Nichols, 2018). The police are often used as a tool for regulating people’s behaviours in public spaces, with some activities being deemed acceptable and others resulting in sanctions. While laws do not explicitly prohibit people from being unhoused, they are used indirectly to punish the behaviours that are more commonly undertaken by people who are street-involved.
We see a clear example of this with the criminalization of people engaged in sex trade work, particularly when it is street-based in nature. Sex trade work is often stigmatized (Benoit et al., 2018, 2020) and people who engage in it are at increased risk of being victimized as a result of the work they do (Baumann et al., 2019). Safety and well-being are pressing concerns for these workers (Magnan-Tremblay, Lanctôt, & Couvrette, 2020) and they use different strategies for navigating violence and stigma (Orchard et al., 2019), but these strategies do not generally involve going to the police. Research conducted with sex workers in five Canadian cities showed that of those who had experienced violence or confinement while working, only 17% reported it to the police, choosing instead to turn to peers for support (Crago, Bruckert, Braschel, & Shannon, 2021). Krüsi et al., (2016) who have studied sex trade work in Canada write that despite police rhetoric of protecting sex workers and prioritizing their safety, they have found people are commonly denied their citizenship rights for police protection by virtue of being in a “risky” occupation. Sibley (2020) further notes that the Protection of Communities and Exploited Persons Act [Bill C-36] demonstrates Canada’s part in a global trend that shifts the state’s attention away from regulating sex work and instead puts forth a carceral agenda.
In much the same way that sex trade work is criminalized, so too are the behaviours that many people who are unhoused and street-involved engage in. We see this through legislation that punishes behaviours like panhandling and squeegeeing as money-making activities. Ontario has the reprehensible title of being the first province to adopt the Safe Streets Act in 1999, followed by British Columbia in 2004 (Chesnay, Bellot, & Sylvestre, 2013). These provincial pieces of legislation are used to ticket people who engage in aggressive panhandling, solicitation of a captive audience (such as people waiting in line for a bus or at an ATM), and the seldom enforced unsafe disposal of glass, needles, and used condoms. Tickets are given out under these laws and if they are not paid, subsequent fines go up and people may face imprisonment for a term not more than six months. In the next two videos, Dr. Tyler Frederick and Dr. Erin Dej discuss the Safe Streets Act as a form of criminalizing homelessness.
In this video, Dr. Tyler Frederick defines criminalization as a policy choice to address a particular social issue, such as substance use, sex trade work, or homelessness, by using the criminal justice system as a primary response. He explains that the criminalization of homelessness often results in policies and laws that target practices associated with homelessness, such as Safe Streets Act legislation that is used to ticket people for panhandling with the potential of jail for accumulated unpaid fines. Dr. Frederick compares these to historical vagrancy laws that gave police authority over people who they deemed to be out of place. He notes that we are currently also seeing more subtle forms of criminalization, through the banishment of people from public places like parks and transit, through selective enforcement of trespass laws that move people along. This video is 4:43 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: What is the criminalization of homelessness?
In this video, Dr. Erin Dej explains that the criminalization of homelessness refers to the ways that people who are experiencing homelessness become involved in the criminal justice system, largely for activities that housed people would not, because they receive more attention from the police. She provides examples such as standing on the sidewalk, being intoxicated, or urinating in public after being denied entry into a public washroom. Dr. Dej argues that the criminal justice system is an inefficient and unethical tool for managing homelessness. She points to the absurdity of legislation, such as Safe Streets Acts, that ticket people for being so poor that they have to ask others for money. She notes that receiving multiple tickets can have detrimental long-term outcomes that keep people entrenched in homelessness. Dr. Dej concludes that criminalization efforts are led by vocal members of the public whose intention is not to solve homelessness, but rather to remove it from public sight. This video is 6:29 in length and has closed captions available in English.
Key Takeaways – Dr. Erin Dej: What is the criminalization of homelessness?
Safe Streets Act legislation is enforced as a means of displacing people from public spaces, on the basis that their behaviour is not acceptable to the general (housed) population. We can consider this act expulsion, as certain people are socially excluded at the same time they are displaced spatially (Kaufman, 2020b). We heard this noted in the previous video from Dr. Erin Dej (2020), author of “A complex exile: Homelessness and social exclusion in Canada.” The Safe Streets Acts were introduced under the premise they would protect people from aggressive panhandling, but research led by Dr. Bill O’Grady and his team (2013) showed that in the 10 years after it was passed ticketing not only rose by 2000% in Toronto but that nearly all the tickets were given out for soliciting a captive audience. This strongly suggests that this legislation is being applied not to protect people from aggressive behaviour, but rather to protect them from having to think about homelessness while going about their daily business.
The Safe Streets Acts in Ontario and British Columbia are discriminatory pieces of legislation. They are used to ticket people who express publicly to others that they are living in extreme poverty. When people cannot pay the tickets, they either get higher tickets or go to jail. Can you think of literally any better response to helping people experiencing homelessness than ticketing and sending them to jail for expressing their needs?
Dr. Bill O’Grady led early analyses of the Ontario Safe Streets Act implementation. In the next video, he explains how discussions about criminalizing homelessness began 20 years ago and are still ongoing today.
In this video Dr. William [Bill] O’Grady notes that we have begun talking about the criminalization of homelessness within the past 20 years. He explains that criminalization entails using laws to target the activities of people experiencing homelessness and to punish them through tickets, arrests, or removal from public spaces. Dr. O’Grady notes that sometimes existing laws are used, such as enforcing bylaws against camping in parks to remove encampments during the COVID-19 outbreak, and sometimes new laws are passed with the intention of targeting behaviours commonly associated with homelessness. Dr. O’Grady points to the Safe Streets Acts in Ontario and British Columbia, under which people can be ticketed for panhandling or squeegeeing near roadways, bus stops, and ATMs. He explains that most tickets are not paid, which can result in higher fines, jail time, and implications for housing and employment that make exiting homelessness more difficult. Dr. O’Grady concludes by drawing our attention to ongoing initiatives to challenge these pieces of legislation and inform the government that they are not working in the best interest of people experiencing homelessness or the general public. This video is 5:17 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: What is the criminalization of homelessness?
Increased police attention, social and spatial displacement, and the enforcement of Safe Streets Act legislation are all examples of the criminalization of homelessness. The extension of this increased policing and ticketing is that people who experience homelessness are more likely to be incarcerated as a result. Much like the snowball effect, we heard about with youth and police involvement, being incarcerated has a snowball effect on one’s subsequent lack of opportunities. Research from three Canadian cities supports this statement, with the finding that being incarcerated in the 12 months preceding the study decreased a person’s likelihood of being housed in the two years that followed (To et al., 2016). Incarceration also increases the risk of relapse for people who use drugs (Goldman-Hasbun, Nosova, Kerr, Wood, & DeBeck, 2019).
When people go to jail, they often lose whatever social support and housing they may have had, such as a shelter bed or access to a friend’s couch. Even if a person is only in jail because they were panhandling and accrued too many unpaid tickets, they are subject to criminal sanctions and the stigma that goes along with them. Ideally, institutional discharge planning would occur so that while a person was incarcerated and nearing their release date workers would help them to secure housing and supports. Consider, for instance, applying a Housing First approach to help people transition directly out of jail and into housing. While this would be a logical approach, the coordination and lack of involvement in systems planning from the corrections sector are considerable barriers (Roy et al., 2020). What we see instead, in most cases, is that people are released from jail without anywhere to go. In the next video, Dr. Bill O’Grady explains further.
In this video Dr. William [Bill] O’Grady argues that people are often released from correctional facilities without a discharge plan in place, which increases their risk of experiencing homelessness. He notes that in the 1990s in Ontario provincial halfway houses were abolished, leaving people with no transitional accommodations upon their release. Dr. O’Grady explains that while some organizations, like the John Howard Society, work in this area more needs to be done to support people in finding housing as they exit jails. In the absence of community supports, there is a revolving door between homelessness and incarceration. Dr. O’Grady concludes that more needs to be done to coordinate and integrate services across public systems, such as corrections, health care, and social services. This video is 2:20 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: The need for better discharge planning out of corrections
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=746#h5p-80
When people are discharged from corrections, they have to find housing and social supports while having the additional stigma and challenges associated with being a person with a criminal record. There are also often conditions placed on people who are released, such as checking in with a parole officer and/or not leaving the city, which puts additional pressure on people to secure housing within a limited geographic area. Institutions often set people up to fail. In the next video, Dr. Naomi Nichols identifies institutional failures as a contributing factor to the criminalization of homelessness and poses an important question. She notes that homelessness shelters are often at capacity and laws prevent people from being able to live freely in public spaces. Given this, she wonders, “Where do people go?” We encourage you to consider this question too as Dr. Nichols explains further.
In this video, Dr. Naomi Nichols argues that there are many institutions that contribute to the criminalization of young people who spend time on the street because they have nowhere else to go. She notes that most cities have bylaws banning people from sleeping or forming encampments in public places, like parks, and encourages us to ask ourselves where people go when shelters are full. Dr. Nichols concludes that sometimes people are given no choice, and are arrested and sent to jail, which she explains is costly, harmful, and not a solution to the problem. This video is 1:19 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: The criminalization of encampments
Where do people live, if there is no affordable housing, shelters are full, and being in public risks being ticketed or sent to jail? As a means of securing their own protection and building community, many people who are unsheltered create encampments in public places. You may have seen these encampments in your own community, such as tents set up around City Hall, in public parks, or less conspicuously under bridges. It is also likely you have seen these removed – at times rather violently – by police acting on government orders.
The COVID-19 period demonstrated gaps in our emergency homelessness response, such as shelters being full and unequipped to manage the public health requirements of physical distancing. To protect themselves from the spread of disease and to increase their own safety, many unsheltered and emergency sheltered people opted instead to set up their own temporary housing with others in the same situation. When these encampments are torn down, it is usually justified under the guise of existing by-laws that ban activities like camping in a public park. We see here again the criminalization of homelessness by focusing on the behaviours people engage in publicly, like sleeping, because they have no alternative private spaces.
Dej, Sanders, and Braimoh (2021) write, “Law enforcement (e.g., police and by-law) is often brought in to respond to encampments. When this happens, there is a tendency for the political nature of encampments and the conditions that produce homelessness to be overlooked. Such interventions and attempts at managing encampments can create a critical divide and, at times divisive relationship, between the city and law enforcement that negatively impacts community resilience” (pg. 6). In the next video, Dr. Jeff Karabanow reflects on the tent encampments that arose and were subsequently torn down during COVID-19.
In this video, Dr. Jeff Karabanow explains that the criminalization of homelessness is a perspective of equating the poverty of homelessness with something delinquent, deviant, or criminal. He notes that this often occurs through legislation and bylaws that target people living on the streets and engaging in private acts in public, because they have nowhere else to go. Dr. Karabanow argues that criminalization practices are part of a broader effort to make people who live in public spaces uncomfortable. He points to the removal of tent encampments across the country during the COVID-19 pandemic as one such example where people were made out to be deviant for sleeping outside. Dr. Karabanow concludes by arguing that the only time these encampments should be removed, especially during a pandemic, is when there are immediate and sustainable housing options available. This video is 2:43 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: What is the criminalization of homelessness?
Treating people as deviant because they lack housing is a form of criminalizing homelessness in much the same way as ticketing and incarcerating people for expressing their poverty in public. People who experience homelessness are regulated in different ways than the housed population, which speaks to the state’s power and leads to many harms being committed against them (Skolnik, 2018). Among the most pressing harms is the disregard for people’s basic human rights to occupy space in public and to speak openly about their needs. We invite you now to engage with this section’s featured reading about homelessness encampments, public health, and human rights. Dr. Bernie Pauly is a co-author of this paper and she speaks more about these issues in the video that follows the reading.
Olson, N., & Pauly, B. (2021). Homeless encampments: Connecting public health and human rights. Canadian Journal of Public Health, 112, 988-991.
In this video Dr. Bernadette [Bernie] Pauly explains that the criminalization of homelessness means being subject to surveillance by policing or bylaw for actions that would be considered activities of daily living, such as sitting or sleeping in public, because a person has no private place to go. She provides the example of people being ticketed for sleeping outside during the COVID-19 pandemic, despite not having a home in which to isolate. Dr. Pauly notes there is a high financial cost to criminalizing homelessness, as funds go towards policing rather than housing, and that it takes a toll on people’s mental health, ability to sleep, and stress levels. She advocates for alternative responses that connect people to the system, particularly for mental health crises and homelessness, in a way that are non-policing based. Dr. Pauly concludes by explaining that displacing people from encampments is a form of criminalization that portrays people who are trying to survive as being a threat to public safety, and that removing them without housing options is neither a human rights nor health-based approach. This video is 9:31 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: What is the criminalization of homelessness?
As Olson and Pauly (2021) note, encampments are a visible form of homelessness that identify the governmental failures to protect citizens through meeting their basic rights to housing, income, and supports. Tearing these communities down, by enforcing city by-laws, is arguably easier than admitting there is a problem – because if the government admits there is a problem, they are legally obligated to solve it. We need to shift the dialogue away from criminalization and towards the enactment of human rights frameworks. This shift is demonstrated in the National Protocol for Homeless Encampments in Canada, authored by Farha and Schwan (2020). In this document, they discuss the eight principles of recognizing residents of encampments as rights holders, engaging with the residents in a meaningful and participatory way, prohibiting forced evictions, exploring alternatives to eviction, relocating people when needed in a way that is human rights compliant, ensuring encampments are set up to provide basic needs like water and toilets, preserving people’s dignity, and respecting and protecting the distinct rights of Indigenous peoples within encampments (Farha & Schwan, 2020).
The criminalization of homelessness is a violation of human rights committed against people because they lack housing. When we talk about people experiencing homelessness and crime, there may be a tendency to assume these individuals are the ones committing crime. Yet, what the research shows is that people who experience homelessness are at greatly increased risk of being the victims of crime, in large part because they are socially excluded and pushed into unsafe physical spaces. The criminalization of homelessness takes many forms including increased police attention, ticketing as the result of asking people for money, being jailed for not being able to pay fines, and then being released back into the community without proper planning and with limitations that make it more difficult to find housing and employment. Does that seem fair to you?
We can see the criminalization of homelessness at work when we turn on the news and see tent encampments being torn down with government explanations that they pose a risk to public safety. What they fail to mention, is that not having those safe spaces is a much bigger risk to the safety of those living within them. We began and ended this section with discussions about human rights. This seemed to us a necessary thing to do, as human rights are left out of the criminalization approach. We have said before – and will continue to say – that homelessness is not a criminal offense, nor will it be solved with police and handcuffs.
Click the link below to listen to all of the researchers answer the question “What is the criminalization of homelessness?” in audio format on our podcast!
84
We can approach homelessness as a social issue that impacts people who have basic human rights and help them get supports or we criminalize people who do not have housing and throw them in jail. If you are reading this chapter in order, you know by now the criminalization approach does not work. Not only does it not work, but it makes no logical sense. We would like to believe that our society is made up of caring, compassionate, and reasonable people. If criminalization is not the way to help people experiencing homelessness (and we cannot stress enough that it is not!), what then would be a better approach? Before you continue through the material in this section we encourage you to pause here and consider how communities can implement better – human centered – support programs to address homelessness at the local level?
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=748#h5p-77
True engagement with human rights practices requires communities commit to really listening to people with lived experience of homelessness and acting on their recommendations. In the previous section, we tried to make clear that criminalizing homelessness is not a rights-based approach. Communities can – and must – do better than to punish, relocate, and/or put people in jail for not having housing and resources. We begin this section again arguing the critical need for human rights approaches that prioritize respect, dignity, and inclusion of diverse peoples and viewpoints. Dr. Kaitlin Schwan, who is the Lead Researcher for the UN Special Rapporteur on the Right to Housing, explains this further in the video that follows.
In this video, Dr. Kaitlin Schwan identifies three things that communities can do to improve their support for people experiencing homelessness. First, they can look towards the evidence base of what programs, policies, and supports have been successful in other countries and in communities across Canada. Second, they must deeply engage people with lived experience in designing and planning supports, in a way that provides them with resources and decision-making power. Finally, communities must expand their affordable housing by building new housing and thinking creatively about how to repurpose existing spaces. Dr. Schwan concludes that municipalities must undertake this work from a rights-based place in accordance with federal legislation. This video is 3:17 in length and has closed captions available in English.
Key Takeaways – Dr. Kaitlin Schwan: How can communities implement better support programs?
The idea of including people who have lived experience in conversations about homelessness makes a great deal of sense but is not always the case when communities are undertaking planning initiatives. There is often an underlying ideology of neoliberalism in service provision (Johnstone, Lee, & Connelly, 2017) which can prioritize budgets and minimal government oversight instead of providing services that are specially designed to meet clients’ needs. We will see the recommendation that people with lived experience be authentically engaged throughout this chapter and, even more broadly, throughout this book. This message is recurring because authentic inclusion and civic engagement are key to a human rights–based approach. In the last section, we encouraged you to read Dr. Bernie Pauly’s work connecting tent encampments to public health and human rights. Here we continue the conversation, as Dr. Pauly speaks about community building as the alternative approach.
In this video Dr. Bernadette [Bernie] Pauly argues that we need to look at how available and affordable housing is within communities, which begins with all levels of government recognizing that housing is a human right. She notes that community organizations can offer support to individuals by meeting them where they are, to help them achieve the goals they establish for themselves. Dr. Pauly explains the importance of community-building as a key social determinant of mental and physical health, that also increases safety. She notes that belonging and inclusion are particularly important for the health and well-being of people who might be experiencing high rates of stigma and discrimination. Dr. Pauly concludes by noting that despite our tendency to medicalize substance use, we need to understand that public health measures like harm reduction are critical for increasing people’s access to social determinants such as housing, food, income, and community supports. This video is 5:17 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: How can communities implement better support programs?
We can look to people who have experienced (or are experiencing) homelessness as the experts. This just makes good sense. If a community wants to understand how well their homelessness services work, who better to ask than people who have accessed them (or equally important, not accessed them despite needing assistance)? People who have lived experience of homelessness are able to offer perspectives on the services and help with evaluations of how effective different programs are. In the next video, Dr. John Ecker discusses the need for ongoing program evaluation and why it is imperative that people who have lived experience be part of the evaluation team.
In this video, Dr. John Ecker argues that communities are doing a good job of offering diverse services for people experiencing homelessness. He notes that while many communities have adopted Housing First, such as in their ten-year plans, it is important that they routinely conduct fidelity assessments to ensure the standards are being met. Dr. Ecker states that communities need to focus on evaluation, with attention to holistic outcome measures that include housing, income, well-being, community integration, and social inclusion. He notes that it is important for community programs to assess staffing ratios, so that they can ensure meaningful programming while avoiding staff burnout. Dr. Ecker concludes that it is important to have service users and people with lived experience of homelessness contribute to program evaluation and design, such as through paid positions in which they have a real opportunity to share their knowledge. This video is 2:56 in length and has closed captions available in English.
Key Takeaways – Dr. John Ecker: How can communities implement better support programs?
Seeking guidance from people with lived experience is a step communities can take to improve their support systems. Part of this work requires that communities take stock of, and evaluate, the programs and services they currently provide, such as through mapping housing-related supports (Canham, Fang, Battersby, & Wada, 2019). It is important not only to identify what services exist, but also to consider how they coordinate with one another. Service hubs are one increasingly used community approach, in which different agencies and supports are located together in the same physical space. This can be thought of as an assemblage of the voluntary sector, private organizations, and government sectors (Evans, Collins, & Chai, 2019) with the intention of making services more accessible by removing barriers. In the video that follows Dr. Tyler Frederick discusses steps communities can take to identify their services, consider the range of supports offered, and tailor them to meet their community members’ diverse needs.
In this video, Dr. Tyler Frederick argues that while there is no magic bullet, there are steps communities can take to help address homelessness at the local level. He notes that we need more affordable housing and housing stability measures, as well as the coordination of services in a way that facilitates easy access for clients in a timely manner. Dr. Frederick encourages communities to conduct a scan of the supports they have in place, particularly in rural areas where services may be more limited. He explains that in these scans, it is important for communities to consider the diversity of clients and what can be done to enhance supports, such as for LGBTQ2S+ youth, racialized communities, and individuals with disabilities. Dr. Frederick notes that communities can also help by focusing on prevention initiatives, greater emphasis on trauma-informed care practices, and programs that help support people feel integrated into the community as they transition out of homelessness. This video is 7:49 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: How can communities implement better support programs?
Mapping the services that are available and assessing whether they meet people’s diverse needs is important for ensuring that community members feel supported and included. Additionally, if communities do not offer tailored supports – or do not promote them – individuals may not be well served. The key to this is addressing the needs of special populations who are at increased risk of homelessness. We have discussed these populations at different points throughout this book, such as in the chapters on Social Work, Indigenous Studies, Child & Youth Studies, and Gender & Queer Studies.
When we asked what communities could do to implement better support programs, many of the researchers’ responses related to tailored population interventions. We encourage you to think about how different people might need different programs and types of support from their communities as you watch the next set of videos. First, Dr. Jacqueline Kennelly and Dr. Jeff Karabanow share insight into how communities can improve youth services. You can learn more in the chapter on Child & Youth Studies.
In this video, Dr. Jacqueline Kennelly explains that within many communities there are great services that exist for youth. However, if they are not aware of them, they may turn to adult services which are not always safe alternatives. This video is 0:36 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: Youth seeking services
In this video, Dr. Jeff Karabanow argues that communities need to have youth at the table for any policy and programming decisions that impact them, because youth know best what works for them. He explains that communities need to adopt Housing First and harm reduction as trauma-informed care philosophies and interventions that prioritize choice and work well for young people. Dr. Karabanow notes that the responses that have been the most helpful have historically come from the non-profit and community-based sector, and that these organizations have expertise that we should be working with. This video is 3:00 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: How can communities implement better support programs?
Young people have particular needs within their community. In the video that follows Dr. Alex Abramovich discusses what communities can do to support youth who identify as lesbian, gay, bisexual, transgender, queer or questioning, and/or two-spirit [LGBTQ2S+]. You can learn more in the chapter on Gender & Queer Studies.
In this video, Dr. Alex Abramovich identifies the need for communities to build more awareness and understanding of diverse identities. He notes that there is a lack of support for LGBTQ2S+ youth experiencing homelessness across the country. Dr. Abramovich explains that communities can help by standardizing the model of care they offer to create service environments that are more accepting and affirming. This step is important for communities to implement for all LGBTQ2S+ persons, as entering a service without knowing what questions will be asked, what types of bathrooms are available, and whether the staff will be respectful can cause high levels of stress. This video is 3:10 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: How can communities implement better support programs?
Communities can best support people by listening to them and providing supports tailored to their specific needs. We have heard that youth and LGBTQ2S+ individuals benefit from approaches that are inclusive and designed with their guidance. In the chapters on Indigenous Studies, Social Work, and Gender & Queer Studies, we variously consider the unique needs of Indigenous persons, racialized individuals, families, and women. Here Dr. Katrina Milaney considers how communities can use targeted approaches to assist each of these populations.
In this video, Dr. Katrina Milaney discusses the need to fund housing programs onsite in shelters for women and families. She notes that within these shelters there are high rates of Indigenous, racialized, and equity-seeking groups and that the system is designed as a crisis response, rather than being equipped to offer culturally appropriate supports. Dr. Milaney concludes that cultivating community partnerships is an important step to help create this supportive capacity within organizations. This video is 1:58 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: How can communities implement better support programs?
Although people who experience homelessness in general benefit from access to services, there are additional measures communities can take to support specific populations. We have seen that young people, those who identify as LGBTQ2S+, Indigenous persons, racialized persons, families, and women are all special populations that benefit from tailored supports. There is an additional special population that we have not yet discussed but needs to be represented here. That is, communities need to support people experiencing homelessness who have pets. The idea that people can be unhoused and have pets, particularly if street-involved and sleeping rough, is unsettling to some people. They wonder: how can people care for animals if they cannot provide themselves with a home and other necessities of life? We pose the alternative question: how could a person survive the trauma of homelessness without the companionship of an animal?
We wrote this book during the COVID-19 pandemic, with virtual team meetings held weekly. It never took long before the cats crawled into laps and started batting at headphone chords. The dogs would sleep nearby or sit (not so) patiently by our feet waiting for a ball to be thrown. On one memorable occasion, a visiting “grand dog” grabbed a printed document out of the recycling bin and ran off with much self-satisfaction over the treat that had been won. As you read this, you may also have a furry, feathery, or scaly friend nearby. It is estimated that 5 – 25% of people experiencing homelessness have pets (Kerman, Gran-Ruaz, & Lem, 2019). While these individuals do not constitute a special population, they do require special consideration at the community level to keep their friends healthy and well.
What do you think the benefits of having a pet while experiencing homelessness are? What do you think the challenges might be? How can communities help these individuals, and their pets, move into stable and secure housing and gain supports? Consider these questions as you watch this brief video about a veterinarian who offers outreach to people experiencing homelessness in California.
Veterinarians can serve as an entry point into reaching people experiencing homelessness who have animals. Outreach in this regard is critically important because many service agencies have ‘no pet’ policies making them inaccessible to these individuals. Instead of sleeping in shelters, they may choose to live in a tent or public space where they can have their animal with them for comfort and companionship. The One Health model of care is a promising approach in which veterinary care is used as part of a holistic wellness program aimed at improving the health, mental health, and well–being of people and their pets (Lem, 2019). Dr. Nick Kerman and his team (2019) have conducted a scoping review to see what is known about homelessness among people with pets and found that there are both benefits and challenges. We invite you now to learn more about the One Health approach for people experiencing homelessness with pets in this section’s featured reading. In the video that follows, Dr. Nick Kerman speaks about his research in this field.
Kerman, N., Lem, M., Witte, M., Kim, C., & Rhoades, H. (2020). A multilevel intervention framework for supporting people experiencing homelessness with pets. Animals (Basel), 10(10), 1869.
In this video, Dr. Nick Kerman explains that pets can be a source of unconditional support, love, and connection for people experiencing homelessness. He notes that the homelessness sector needs to enact pet-friendly organizational policies and practices to support people with pets, as they often fall through the cracks if they are turned away. Dr. Kerman discusses the additional challenges people with pets have in securing housing, particularly if they are looking to rent in a building with a ‘no pet’ policy. Although this is a grey area, not all individuals will feel comfortable advocating for their rights and may not proceed with housing that can create problems and result in a future episode of homelessness. Dr. Kerman concludes by correcting the common misconception that pets of people experiencing homelessness are not well cared for. Rather, he explains, the research shows they are just as healthy as housed pets and may be better socially adjusted around strangers. This video is 6:10 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: Supporting pet owners experiencing homelessness
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=748#h5p-82
There are many steps communities can take to support individuals experiencing homelessness. We have seen that listening to people with lived experience, evaluating and taking stock of existing programs, creating services for specialized populations, and helping people continue to care for their pets are all aspects that communities should embrace. For all of this to happen, we must address the elephant in the virtual room. That is, taking a community-building approach requires that we recognize the prevalence of “not in my backyard” [NIMBY] attitudes that arise surrounding supports for people experiencing homelessness. Dr. Bill O’Grady speaks about NIMBY in the video that follows.
In this video Dr. William [Bill] O’Grady discusses the need for school-based interventions for youth, such as family reconnect programs and supports for those transitioning out of care. He notes that at the community level it is also important to increase public education to combat ‘not in my backyard’ [NIMBY] attitudes that might arise in resistance to shelters or supportive housing initiatives being built. This video is 1:42 in length and has closed captions available in English
Key Takeaways – Dr. Bill O’Grady: How can communities implement better support programs?
Public education is critical in combatting NIMBY attitudes, which are often embedded in a criminalization of homelessness mindset. Rather than embracing human rights–based approaches that see housing and support as necessary for ensuring the well-being of all citizens, some members of society are more inclined to think of policing as the solution. We have seen already why this is problematic. Dr. Naomi Nichols speaks about the need to build greater public empathy, in the next video.
In this video, Dr. Naomi Nichols explains that we need to think about the general public’s response to homelessness and how we can build greater empathic understanding. She provides the example of someone calling police to report an encampment in a public park. Dr. Nichols notes that this action starts a criminalization process that results in evicting the person from the only safe place they could find to sleep. She concludes that we must push harder to implement solutions such as affordable housing, rent subsidies, and different supported housing models. This video is 2:19 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: How can communities implement better support programs?
Perhaps the most important approach communities can take to support people experiencing homelessness, is to be inclusive. Sometimes when new projects are proposed, such as a housing development for people experiencing homelessness, it is met with public resistance and conflict (Ranasinghe & Valverde, 2006). In fact, research has shown there are notable differences in the willingness of citizens in different locations to invest in homelessness programs (Doberstein & Smith, 2019a) and that there can be deep contention over the need for diverse services located within a given community (Dej, Sanders, & Braimoh, 2021). Part of what gives rise to NIMBY responses is the notion of “deservingness,” which factors into citizens’ support for investing in homelessness initiatives (Doberstein & Smith, 2019b). Although gaining access to services often requires a person demonstrate that they are “appropriately homeless and needy” (Cook & Hole, 2020), this creates a power dynamic that is contrary to human rights approaches. What if instead of fighting against new homelessness services, people embraced them as a necessary part of building capacity within the community? In the next video, Dr. Nick Kerman explains why advocating for these kinds of community programs is important.
In this video, Dr. Nick Kerman explains that whether located in urban or rural areas, community programs face a number of challenges. First and foremost, he notes, these organizations are underfunded to provide the supports and services clients need. Dr. Kerman argues that in addition to providing more funding we must also address societal stigma and ‘not in my backyard’ [NIMBY] attitudes that sometimes arise in resistance to new community programs. Dr. Kerman concludes that it is important to advocate for community services, promote the positive outcomes they can have for all community members, and dispel any myths that might exist. This video is 3:07 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: How can communities implement better support programs?
When new initiatives are proposed in a community they may be met with resistance, but people can find satisfaction if they are given the opportunity to discuss them, particularly with others who have different viewpoints than their own (Doberstein, 2020). Despite their challenges, public housing projects can be good places to live (van Ingen, Sharpe, & Lashua, 2018) and communities can support their residents by promoting inclusion and ensuring all members have safe and high-quality housing (Ecker & Aubry, 2017). The quality of a person’s living space has been shown to impact their quality-of-life (Magee et al., 2019), although further research is needed to know whether there is also a relationship between the quality of the neighbourhood and a person’s long-term housing stability (Distasio et al., 2021).
Importantly, communities need to focus on inclusion, providing safe and high-quality housing, and ensuring that supports continue to be made available continuously. Research from Kingston Ontario shows that even after becoming securely housed, people may still experience food insecurity and be heavily dependent on charitable food programs (Hainstock & Masuda, 2019). In the final video of this section, Dr. Jacqueline Kennelly explains why NIMBY is problematic, the value of ongoing community supports, and why community members need to hold their public representatives accountable for upholding human rights.
In this video, Dr. Jacqueline Kennelly argues that there are many things communities can do to help support people experiencing homelessness, such as becoming more knowledgeable about the complexity of homelessness and not engaging in ‘not in my backyard’ [NIMBY] politics. She notes that there are some wonderful community resources that exist, but more needs to be done to offer affordable housing, financial supports, and adequate health care. Dr. Kennelly points to a food bank in her city that offers a warm and welcoming environment, as demonstrating how organizations should operate to support rather than demoralize or stigmatize people. Dr. Kennelly argues, however, that while communities can do many things, the duty belongs to government and elected officials to ensure everyone has their human rights met. This video is 3:26 in length and has closed captions available in English.
Key Takeaways – Dr. Jacqueline Kennelly: How can communities implement better support programs?
Communities can support all of their citizens by rejecting the criminalization of homelessness and instead implementing a human rights-based approach. To accomplish this, they need to ensure they have mechanisms for listening to people who have lived experience, such as inclusion on planning committees, and that they follow through on implementing their recommendations. Listening to people who have been clients of the services can help to identify and address gaps that exist. Additionally, communities should consider the diversity of their population and review how to make their services more inclusive for everyone. This may involve establishing supports for special populations, such as women, youth, LGBTQ2S+ individuals, Indigenous persons, and families, among others. We saw in this chapter that many people who experience homelessness have pets with them, who provide a critical source of companionship. Communities can help increase wellness by providing outreach veterinary care for people’s pets as part of a holistic approach.
While there are many steps communities can take to increase the well-being of all their members, the largest hurdle is that of NIMBYism which reflects the “not in my backyard” resistance to new supports being created. When housing developments or other services are proposed, they may be met with resistance from some members of the community. Public education and advocacy are important for addressing the stigma and misconceptions that fuel these attitudes. What all people need is a safe place to live – by adopting a human rights mindset, communities can cultivate the support needed to turn this into a reality.
Click the link below to listen to all of the researchers answer the question “How can communities implement better support programs?” in audio format on our podcast!
85
Susan
Let’s return to the scenario involving Susan. There is a rather inevitable quality to her story that plays itself out over and over again across Canada. If we use a pet analogy, it is like that small mouse running all day in the wheel in its cage. The fact that she was released from jail with nothing, to a community that she was unfamiliar with, and with no connections to family or social support – sets her up to fail and inevitably be re-arrested. It is hard to know the impact of the social profiling that she experienced with the police outside her residence on a continuous basis asking her what she was doing. Can you imagine if every time you left your house this happened to you?
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1188#h5p-87
86
We began this chapter on Sociology and Crimino-Legal Studies by sharing a video of a man bathing in a public fountain and receiving news media coverage for the impact this was having on the quality-of-life of the housed citizens who lived nearby. We began with this story as a way of highlighting how police are often called into situations that are better addressed by considering the bigger picture of whose quality-of-life is really at stake.
At the start of the chapter, we introduced you to the composite character Susan who has had negative experiences with police and the justice system that have impacted her housing stability. The scenario was presented as an entry point into thinking about the complexity of homelessness. We returned to her story again at the end to demonstrate how it can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada.
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked,“Are all people who experience homelessness street-involved?” Here we considered how the sociology of homelessness has been shaped around urban ethnography of the street, tracing back to the Chicago School and Nels Anderson’s research on hobo culture. We noted that while this work is important, we also must recognize that not all people who experience homelessness are involved with the street. Most notably, people who live in rural and remote areas often do not have access to a critical mass of infrastructure that would constitute a street environment. Within urban settings, the street is often made up of social service agencies but also has a social element as well. People may move between the network of organizations and arrange their time around their hours of operation.
Next we asked, “What is the criminalization of homelessness?” This led us to consider how people who experience homelessness – and in particular visible homelessness – are subject to sanctions for being in public spaces. This criminalization occurs in multiple ways, such as through additional police attention and profiling, ticketing under Safe Streets Act legislation, and incarceration for not paying fines. We further saw that when people get released from custody they are often subject to conditions that make finding housing and employment more difficult, without the support of appropriate discharge planning. The criminalization of homelessness has also led to enforcement of by-laws, such as prohibiting camping in parks, which resulted in encampments being torn down, as highly evident during the COVID-19 lockdowns. The criminalization of homelessness has many long-lasting harmful outcomes and does nothing to actually address the problem of homelessness.
Finally, we asked, “How can communities implement better support programs?” In this final section, we turned away from criminalization and considered how communities can use human rights-based approaches to support their citizens. We saw that it is critically important to include people with lived experience in decision-making and to implement their recommendations. While communities may have existing programs, we saw that they are encouraged to evaluate these programs and review their diversity for meeting the needs of special populations, including for youth, women, LGBTQ2S+ persons, Indigenous persons, families, and people who have pets. Additional community education may be needed to counter NIMBY attitudes and ensure safe and affordable housing, as well as ongoing supports, are available for all members of the community.
87
Here are some additional resources you may want to check out!
88
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
89
Anderson, N. (1923). The hobo: The Sociology of the homeless man. Chicago: The University of Chicago Press.
Baron, S. W., & Forde, D. R. (2020). Childhood trauma, criminogenic social schemas, and violent crime. Deviant Behavior, 41(8), 991–1004. https://doi.org/10.1080/01639625.2019.1596534
Baumann, R. M., Hamilton-Wright, S., Riley, D. L., Brown, K., Hunt, C., Michalak, A., & Matheson, F. I. (2019). Experiences of violence and head injury among women and transgender women sex workers. Sexuality Research & Social Policy, 16(3), 278–288. https://doi.org/10.1007/s13178-018-0334-0
Benoit, C., Jansson, S. M., Smith, M., & Flagg, J. (2018). Prostitution stigma and its effect on the working conditions, personal lives, and health of sex workers. The Journal of Sex Research, 55(4-5), 457–471. https://doi.org/10.1080/00224499.2017.1393652
Benoit, C., Maurice, R., Abel, G., Smith, M., Jansson, M., Healey, P., & Magnuson, D. (2020). “I dodged the stigma bullet”: Canadian sex workers’ situated responses to occupational stigma. Culture, Health & Sexuality, 22(1), 81–95. https://doi.org/10.1080/13691058.2019.1576226
Buck-McFadyen, E. (2021). Competing perspectives on rural homelessness: Findings from a qualitative study in Ontario, Canada. Health & Social Care in the Community. https://doi.org/10.1111/hsc.13633
Canham, S. L., Fang, M. L., Battersby, L., & Wada, M. (2019). Understanding the functionality of housing-related support services through mapping methods and dialogue. Evaluation and Program Planning, 72, 33–39. https://doi.org/10.1016/j.evalprogplan.2018.09.008
Chesnay, C. T., Bellot, C., & Sylvestre, M. E. (2013). Taming disorderly people one ticket at a time: The penalization of homelessness in Ontario and British Columbia. Canadian Journal of Criminology and Criminal Justice, 55(2), 161–185. https://doi.org/10.3138/cjccj.2011-E-46
Collins, A. B., Boyd, J., Mayer, S., Fowler, A., Kennedy, M. C., Bluthenthal, R. N., … McNeil, R. (2019). Policing space in the overdose crisis: A rapid ethnographic study of the impact of law enforcement practices on the effectiveness of overdose prevention sites. The International Journal of Drug Policy, 73, 199–207. https://doi.org/10.1016/j.drugpo.2019.08.002
Cook, S., & Hole, R. (2020). “Appropriately homeless and needy:” Examining street homeless survival through the lens of Bourdieusian social capital theory. Journal of Human Behavior in the Social Environment, 30(7), 816–834. https://doi.org/10.1080/10911359.2020.1747585
Crago, A. L., Bruckert, C., Braschel, M., & Shannon, K. (2021). Sex workers’ access to police assistance in safety emergencies and means of escape from situations of violence and confinement under an “end demand” criminalization model: A five city study in Canada. Social Sciences (Basel), 10(1), 13–. https://doi.org/10.3390/socsci10010013
Dej, E. (2020). A complex exile: Homelessness and social exclusion in Canada. BC: UBC Press.
Dej, E., Sanders, C., & Braimoh, J. (2021). Rewriting the narrative on homelessness in mid-size Canadian cities. Ontario: Centre for Research on Security Practices, Laurier University. Brokering a Counter-Narrative on Homelessness (homelesshub.ca)
Distasio, J., Adair, C. E., Hwang, S., Hinds, A., Kopp, B. C., Aubry, T., … Kaufman, A. F. (2021). Exploring the relationship between neighbourhood quality (NQ) and housing stability among formerly homeless individuals with mental illness in housing first. Wellbeing, Space and Society, 2, 100008–. https://doi.org/10.1016/j.wss.2020.100008
Doberstein, C. (2020). Role-playing in public engagement for housing for vulnerable populations: An experiment exploring its possibilities and limitations. Land Use Policy, 99, 105032–. https://doi.org/10.1016/j.landusepol.2020.105032
Doberstein, C., & Smith, A. (2019a). Citizen support for spending to reduce homelessness in Canada’s largest urban centres. Housing Studies, 34(7), 1140–1162. https://doi.org/10.1080/02673037.2018.1520820
Doberstein, C., & Smith, A. (2019b). When political values and perceptions of deservingness collide: Evaluating public support for homelessness investments in Canada. International Journal of Social Welfare, 28(3), 282–292. https://doi.org/10.1111/ijsw.12353
Ecker, J., & Aubry, T. (2017). A mixed methods analysis of housing and neighbourhood impacts on community integration among vulnerably housed and homeless individuals. Journal of Community Psychology, 45(4), 528–542. https://doi.org/10.1002/jcop.21864
Evans, J., Collins, D., & Chai, C. (2019). On thin ice: Assembling a resilient service hub. Area (London 1969), 51(3), 451–460. https://doi.org/10.1111/area.12448
Faraji, S. L., Ridgeway, G., & Wu, Y. (2018). Effect of emergency winter homeless shelters on property crime. Journal of Experimental Criminology, 14(2), 129–140. https://doi.org/10.1007/s11292-017-9320-4
Farha, L., & Schwan, K. (2020). A national protocol for homeless encampments in Canada. Canada: UN Special Rapporteur on the Right to Housing. Tent Encampment Protocol (make-the-shift.org)
Fast, D., & Cunningham, D. (2018). “We don’t belong there”: New geographies of homelessness, addiction, and social control in Vancouver’s inner city. City & Society, 30(2), 237–262. https://doi.org/10.1111/ciso.12177
Frederick, T. (2019). Conceptualizing the social and cultural organization of street life among young people experiencing homelessness. Journal of Youth Studies, 22(8), 1133–1149. https://doi.org/10.1080/13676261.2019.1569214
Frederick, T., O’Connor, C., & Koziarski, J. (2018). Police interactions with people perceived to have a mental health problem: A critical review of frames, terminology, and definitions. Victims & Offenders, 13(8), 1037-1054. 10.1080/15564886.2018.1512024
Gaetz, S., Barr, C., Friesen, A., Harris, B., Hill, C., Kovacs-Burns, K., Pauly, B., Pearce, B., Turner, A., & Marsolais, A. (2012) Canadian definition of homelessness. Toronto: Canadian Observatory on Homelessness Press. Canadian Definition of Homelessness | The Homeless Hub
Goldman‐Hasbun, J., Nosova, E., Kerr, T., Wood, E., & DeBeck, K. (2019). Homelessness and incarceration associated with relapse into stimulant and opioid use among youth who are street‐involved in Vancouver, Canada. Drug and Alcohol Review, 38(4), 428–434. https://doi.org/10.1111/dar.12921
Hainstock, M., & Masuda, J. R. (2019). “We have a roof over our head, but we have to eat too:” Exploring shifting foodscapes from homelessness into Housing First in Kingston, Ontario. Health & Place, 59, 102197–102197. https://doi.org/10.1016/j.healthplace.2019.102197
Huey, L., & Ferguson, L. (2020). “Did not return in time for curfew”: A descriptive analysis of homeless missing persons cases. International Criminal Justice Review, 105756772091864–. https://doi.org/10.1177/1057567720918640
Isaak, C. A., Reynolds, K., Sareen, J., & Distasio, J. (2019). The entrepreneurship of survival among urban adults experiencing homelessness and mental illness. Journal of Community Psychology, 47(6), 1548–1562. https://doi.org/10.1002/jcop.22204
Johnstone, M., Lee, E., & Connelly, J. (2017). Understanding the meta-discourse driving homeless policies and programs in Toronto, Canada: The neoliberal management of social service delivery. International Social Work, 60(6), 1443–1456. https://doi.org/10.1177/0020872817706406
Kaufman, D. F. (2020a). Canadian homeless mobilities: Tracing the inter-regional movements of at home / chez soi participants. The Canadian Geographer, 65(3), 292-305. https://doi.org/10.1111/cag.12658
Kaufman, D. (2020b). Expulsion: A type of forced mobility experienced by homeless people in Canada. Urban Geography, 1–23. https://doi.org/10.1080/02723638.2020.1853919
Kerman, N., Gran-Ruaz, S., & Lem, M. (2019). Pet ownership and homelessness: a scoping review. Journal of Social Distress and the Homeless, 28(2), 106–114. https://doi.org/10.1080/10530789.2019.1650325
Kerman, N., Lem, M., Witte, M., Kim, C., & Rhoades, H. (2020). A Multilevel Intervention Framework for Supporting People Experiencing Homelessness with Pets. Animals (Basel), 10(10), 1869. https://doi.org/10.3390/ani10101869
Kouyoumdjian, F. G., Wang R., Mejia-Lancheros, C., Owusu-Bempah, A., Nisenbaum, R., O’Campo, P., Stergiopoulos, V., & Hwang, S. W. (2019). Interactions between police and persons who experience homelessness and mental illness in Toronto, Canada: Findings from a prospective study. The Canadian Journal of Psychiatry, 64(10),718-725. 10.1177/0706743719861386
Krüsi, A., Kerr, T., Taylor, C., Rhodes, T., & Shannon, K. (2016). “They won’t change it back in their heads that we’re trash’: The intersection of sex work‐related stigma and evolving policing strategies. Sociology of Health & Illness, 38(7), 1137–1150. https://doi.org/10.1111/1467-9566.12436
Lem, M. (2019). Serving homeless populations through a one health approach. Canadian Veterinary Journal, 60(10), 1119–1120. https://europepmc.org/article/PMC/PMC6741821
Lemieux, A. J., Leclair, M. C., Roy, L., Nicholls, T. L., & Crocker, A. G. (2020). A typology of lifetime criminal justice involvement among homeless individuals with mental illness: Identifying needs to better target intervention. Criminal Justice and Behavior, 47(7), 790–807. https://doi.org/10.1177/0093854819900305
MacDonald, S. A., & Gaulin, D. (2020). The invisibility of rural homelessness in a Canadian context. Journal of Social Distress and Homelessness, 29(2), 169-183. 10.1080/10530789.2019.1688540
Magee, C., Norena, M., Hubley, A. M., Palepu, A., Hwang, S. W., Nisenbaum, R., … Gadermann, A. (2019). Longitudinal associations between perceived quality of living spaces and health-related quality of life among homeless and vulnerably housed individuals living in three Canadian cities. International Journal of Environmental Research and Public Health, 16(23), 4808. https://doi.org/10.3390/ijerph16234808
Magnan‐Tremblay, L., Lanctôt, N., & Couvrette, A. (2020). The hopelessness effect: Counsellors’ perceptions of their female clients involved in sex work in Canada. Health & Social Care in the Community, 28(5), 1430–1437. https://doi.org/10.1111/hsc.12993
Nichols, N. (2018). The social organization of access to justice for youth in “unsafe” urban neighbourhoods. Social & Legal Studies, 27(1), 79–96. https://doi.org/10.1177/0964663917703179
O’Grady, B., Gaetz, S., & Buccieri, K. (2011). Can I see your ID? The policing of youth homelessness in Toronto. Toronto: JFCY & Homeless Hub. CanISeeYourID_nov9.pdf (homelesshub.ca)
O’Grady, B., Gaetz, S., & Buccieri, K. (2013). Tickets… and more tickets: A case study of the Enforcement of the Ontario Safe Streets Act. Canadian Public Policy, 39(4), 541-558. https://www.muse.jhu.edu/article/534407
Olson, N., & Pauly, B. (2021). Homeless encampments: Connecting public health and human rights. Canadian Journal of Public Health, 112, 988-991. https://doi.org/10.17269/s41997-021-00581-w
Orchard, T., Murie, A., Elash, H. L., Bunch, M., Middleton, C., Sadakhom, D., … Benoit, C. (2019). “People like us”: Spatialised notions of health, stigma, power and subjectivity among women in street sex work. Culture, Health & Sexuality, 21(4), 478–494. https://doi.org/10.1080/13691058.2018.1490455
Pijl, E. M., & Belanger, Y.D. (2021). Lost in transition: Entering the liminal space of rural homelessness in a small prairie town. Journal of Social Distress and Homelessness, 30(2), 126-134. 10.1080/10530789.2020.1763575
Quirouette, M., Frederick, T., Hughes, J., Karabanow, J., & Kidd, S. (2016). “Conflict with the law”: Regulation & homeless youth trajectories toward stability. Canadian Journal of Law and Society, 31(3), 383–404. https://doi.org/10.1017/cls.2016.26
Ranasinghe, P. & Valverde, M. (2006). Governing homelessness through land-use: A sociolegal study of the Toronto shelter zoning by-law. Canadian Journal of Sociology, 31(3), 325-349. https://www.jstor.org/stable/20058713
Roy, L., Crocker, A., Hurtubise, R., Latimer, E., Côté, M., Billette, I., & Boissy, F. (2020). Reducing criminal justice involvement of individuals experiencing homelessness and mental illness: Perspectives of frontline practitioners. Canadian Journal of Criminology and Criminal Justice, 62(2), 1–21. https://doi.org/10.3138/cjccj.2019-0056
Schiff, R., Buccieri, K., Waegemakers Schiff, J., Kauppi, C., & Riva, M. (2020). COVID-19 and pandemic planning in the context of rural and remote homelessness. Canadian Journal of Public Health, 111, 967-970. https://doi.org/10.17269/s41997-020-00415-1
Schiff, R., & Møller, H. (Eds.). (2021). Health and health care in northern Canada. Toronto: University of Toronto Press.
Sibley, M. A. (2020). Attachments to victimhood: Anti-trafficking narratives and the criminalization of the sex trade. Social & Legal Studies, 29(5), 699–717. https://doi.org/10.1177/0964663919897970
Skolnik, T. (2018). How and why homeless people are regulated differently. Queen’s Law Journal, 43(1), 297. https://ssrn.com/abstract=3219919
To, M. J., Palepu, A., Matheson, F. I., Ecker, J., Farrell, S., Hwang, S. W., & Werb, D. (2016). The effect of incarceration on housing stability among homeless and vulnerably housed individuals in three Canadian cities: A prospective cohort study. Canadian Journal of Public Health, 107(6), e550–e555. https://doi.org/10.17269/CJPH.107.5607
van Ingen, C., Sharpe, E., & Lashua, B. (2018). Neighborhood stigma and the sporting lives of young people in public housing. International Review for the Sociology of Sport, 53(2), 197–212. https://doi.org/10.1177/1012690216641146
IX

Social Work is not easy work. Yet, Social Workers play a critical role within the homelessness sector, particularly in relation to supporting individuals who have complex needs. Often when an individual experiences chronic homelessness, that is ongoing over time without resolution, it is related in some way to challenges in their lives. These challenges may be related to mental health and/or addictions, an inability to hold consistent employment, or difficulty carrying out the tasks of maintaining housing, such as paying rent. Social Workers often constitute the support network for people who may otherwise be dissociated from family and friends. Although they deal in the mundane – providing help with meeting the basic necessities of life – the importance of their roles cannot be overstated.
90
In this chapter, you are invited to think about the important role that Social Workers undertake in supporting individuals who experience homelessness. While learning more about this kind of work, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that Social Workers are a critical part of the daily support networks for many people who experience chronic homelessness. This work, while essential, can also be emotionally and physically draining. Read on to learn more about Social Work within the homelessness sector.
91
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to Social Work. As you read through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After pausing to respond to reflection questions, we will endeavour to answer each question posed in the learning objectives. What is the role of case management in Social Work? Which special populations are at high risk of homelessness? How can support workers prevent becoming burned out? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
92
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider this person’s experience.
Liam
Liam is a 59-year-old male who has come into the community centre in the downtown area of a large city. The centre is a place where folks who live homeless can drop in for a meal, wash their clothes, and find toiletries, extra clothing, and bedding. Liam has frequented the centre for 3 years off and on. When he comes in, he meets with one of the Social Workers, Tanya. The Social Worker’s role is to provide case management: assessing Liam’s needs and arranging, coordinating, monitoring, and evaluating his connections to various services to determine if his needs are being met. Tanya has found her work with Liam very challenging over the past year as he has moved around a significant amount and attends the centre for a bit and then disappears for weeks on end. In the past 6 months he has lived under a local overpass, stayed with a friend for a month and has been in and out of one of the local shelters during the winter months. Liam hasn’t had access to phone/internet connection and his identification has expired. Tanya has set Liam up with free legal assistance, a Nurse Practitioner, government income assistance, and a local housing organization. All of the case workers at these agencies have connected with Tanya to see if she can find him, as he has missed appointments and they have lost track of him. As she sees Liam come in, she knows she needs to make a positive connection today to try and re-establish assistance.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to this scenario again at the end of the chapter.
Reflection Questions
93
Social Work is a helping profession. The people who enter into this field often do so because they are motivated to assist others who are in some form of need. As it pertains to homelessness, Social Work plays a vital role in helping people establish connections within the community, such as to housing, food, employment, and health and wellness supports. Case management is a particular skill set of Social Workers that uses established protocols to identify clients in need of assistance and work with them over a period of time to help them access the services they need to obtain stability and security.
Before we take a more in-depth look at the role of case management within Social Work, we encourage you to pause and consider how you think it might be useful as a method for supporting people experiencing homelessness. You may use the space below to write your response.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=757#h5p-83
Recently a team of health care providers, researchers, community members, and people with lived experience of homelessness worked together to develop a document entitled, “Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience” (Pottie et al., 2020). You will have the opportunity to read this document and learn more about it in the chapter on Primary Care & Nursing. However, we introduce it here because it also has relevance to the field of Social Work. The authors of these clinical guidelines write that having case management interventions, with access to psychiatric support, is recommended as an initial step to support the primary health care of people experiencing homelessness or housing vulnerability, particularly as a means to address mental illness and/or addictions issues that might complicate one’s medical care (Pottie et al., 2020).
Case management is a critical piece in helping people experiencing homelessness to connect with supports, such as health care, within their community. This raises the questions of what exactly case management is and how we can understand it as being situated within Social Work. The Canadian Observatory on Homelessness has prepared a brief overview that discusses the definition, goals, and conditions of case management in relation to homelessness. We invite you now to flip through this document below.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=757#h5p-21
The Global Social Service Workforce Alliance (2018) further expands upon the definition of case management. They write that case management is a process practiced by Social Workers, that guides the delivery of social service support to vulnerable individuals in need. It begins when a person or family is identified as being in a difficult situation requiring support or assistance. They further indicate that case management involves a Social Worker who collaboratively assesses the needs of a client (and when appropriate the client unit) and arranges, coordinates, monitors, evaluates and advocates for a package of services to meet the client’s specific needs. (Global Social Service Workforce Alliance, 2018).
The Global Social Service Workforce Alliance (2018) document identifies 9 key principles that underpin the case management process. These include: [1] increasing resiliency and improving quality of life, [2] collaboration and partnership, [3] doing no harm, [4] respect and promotion of client strengths, [5] respect for diversity, culture, and tradition, [6] respect for, and reflection of, a human rights-based approach, [7] consent to participate in case management, [8] confidentiality, and [9] assurance of quality in case management, such as through clear job descriptions, supervision, and monitoring and evaluation.
These principles are important because they establish the criteria for “good case management,” which is an idea that re-emerged throughout the researcher interviews conducted for this book. For instance, we spoke to Dr. Jeannette Waegemakers Schiff, who is the author of “Working with homeless and vulnerable people: Basic skills and practice,” a text that prepares frontline workers through offering knowledge and understanding of homelessness and vulnerability from a lived perspective, as well as from professional practice considerations (Waegemakers Schiff, 2015). Dr. Waegemakers Schiff explained the history of case management and why it is important that it be done properly.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Jeannette Waegemakers Schiff likens good case management to a form of preventative medicine, that supports people from falling through the cracks of long-term and intractable problems in their lives. She traces the two roots of case management, including in hospitals through discharge nursing, and in Social Work where there is a comprehensive consideration of people’s psychosocial, physical, and behavioural needs. Dr. Waegemakers Schiff argues that good Social Work is not about providing clients with a checklist of what they need to do, but rather walking alongside them and continually returning to check in on them over time. This video is 3:44 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: What is the role of case management in social work?
Professional helping relationships are a distinct part of interventions designed to support people who are highly disadvantaged, such as those experiencing homelessness (Sandu, Anyan, & Stergiopoulos, 2021). It is important to understand that there are different types of interventions, and that case managers play a role in helping their clients navigate through them. For instance, considering different profiles of people’s need when they are experiencing homelessness, researchers have found that increased assertive or intensive case management may be particularly beneficial for those who have multiple and complex health problems and high frequency of service use (Fleury, Grenier, Cao, & Meng, 2020). Family systems therapy has been found to be an effective intervention for addressing youth homelessness, because it is an approach that includes the whole family in an effort to help them reconnect and see problems as resulting from the relational system rather than individual deficiencies (Cully, Wu, & Slesnick, 2018). Even after a client is housed, case managers play an important role in continuing to provide support for a period of time, to help reduce the risk of homelessness reoccurring (Kaltsidis, Grenier, Cao, & Fleury, 2020).
How the case manager operates – such as which organizations or individuals they reach out to and connect with – will be determined by the individual needs of their client, as identified by the client themselves. A systemic review of the literature on youth homelessness, for instance, has found that the effectiveness of interventions varies according to the issue that needs to be addressed (Wang et al., 2019). Most notably, cognitive behavioural therapy was shown to be promising for addressing depression, family-based therapy was successful for improving substance use outcomes, and housing programs were effective for achieving greater housing stability (Wang et al., 2019). While the case manager themselves would not be providing the interventions, such as cognitive behavioural therapy, their role would be to help the person identify what kind of support they need and then connect to the right program or service. It is essential that Social Workers come to their roles with an open and inclusive mindset that respects the unique histories, experiences, and needs of their clients so that they can offer the right kinds of support. Consider this as you watch a brief video entitled, “Indigenous Social Work” created by the Alberta College of Social Workers.
We invite you to learn more about Indigenous-based Social Work in this section’s featured reading published in the International Journal of Indigenous Health. You can also learn more in the chapter on Indigenous Studies.
Firestone, M., Syrette, J., Brant, T., Laing, M., & Teekens, S. (2021). Findings from a process evaluation of an Indigenous holistic housing support and mental health case management program in downtown Toronto. International Journal of Indigenous Health, 16(2), 139-150.
Kozloff et al., (2018) emphasize the important role of Social Workers walking beside a person as they work through their crisis situation and identify their strengths. They explain that a crisis can be an opportunity for a client and service provider to deepen their relationship and establish a foundation of trust (Kozloff et al., 2018). This notion of walking alongside one’s client was discussed by Dr. Waegemakers Schiff in the preceding video, and it also emerged in our conversation with Dr. David Firang in the video that follows.
In this video, Dr. David Firang identifies the three foundational elements of case management. The first element is engagement, which means establishing rapport, a therapeutical alliance relationship, warmth, and general care to create the conditions where the client feels comfortable and supported in sharing personal information. The second element of case management is assessment, in which the client and case manager discuss the presenting issues and come to an understanding, much like a medical doctor making a diagnosis. The final element of case management Dr. Firang identifies is jointly creating an intervention plan with the client by empowering them to access supports but also advocating for and organizing referrals to services in the community. These elements are the essence of case management in Social Work. This video is 6:08 in length and has closed captions available in English.
Key Takeaways – Dr. David Firang: What is the role of case management in social work?
Dr. Firang says that case management is about establishing rapport and relationships, rather than being Hercules or Superman. What personal traits or characteristics do you think Social Workers need to have to be successful in case management roles?
As you consider your response to the question above, we invite you to watch this video from Homeless Link, located in the United Kingdom, in which individuals with lived experience of homelessness share what they feel are important qualities for support workers to have. How does your response compare to the ones given in the video?
Through the process of case management, Social Workers can help people navigate through complex systems and institutions within society. In the next video, Dr. Jeff Karabanow explains that it is critically important for case managers to undertake this kind of work with a deep commitment to social justice and anti-oppressive dynamics, and by applying an accompaniment approach.
In this video, Dr. Jeff Karabanow discusses how the formal and bureaucratic nature of our social systems can make them difficult and overwhelming for people to navigate. He argues that good casement management is about connecting with clients to help them broker, negotiate, and navigate complex systems in society, by using a practice that is deeply grounded in the principles of social justice, a critical engagement with anti-oppressive dynamics, and an accompaniment style. This video is 2:24 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: What is the role of case management in social work?
As Dr. Karabanow points out, Social Workers who undertake case management need to have a keen sense of how to provide support in a way that is respectful of a person’s unique needs and personal history. People who experience homelessness are often deeply impacted by trauma, both through their homelessness experience and as a precipitating factor. The three principles Dr. Karabanow identifies – of working with a social justice, anti-oppressive, and accompaniment style – are all situated within a trauma-informed framework of care. Engaging in trauma-informed care work means treating clients with respect, honouring individual differences, providing an emotionally safe caregiving environment, using an empowerment framework to support self-efficacy, facilitating access to trauma-specific services, and considering individuals within their larger social environments (Hopper, Olivet, & Bassuk, 2018).
Professional Social Workers play an important role, but increasingly interventions designed to support people experiencing homelessness are also integrating peer support. While peers are generally not formally credentialed, such as having an undergraduate or graduate degree, they do work alongside case managers to provide individualized supports to clients in need. It has only been in recent years that researchers have begun to study the role of peer support in-depth. For instance, Parkes et al., (2019) note that peer-delivered approaches seem to have particular promise, but there is limited evidence regarding peer interventions that are both acceptable to, and effective for, people who are experiencing homelessness and using drugs and/or alcohol. Likewise, Kidd et al., (2019) have pointed out there has been limited research conducted on peer support work for young people, but the research that does exist suggests peer support has the potential for positive outcomes, provided the peer support is a robust part of the programming in a way that benefits clients and peer workers alike.
The importance of peer support is evident across many types of interventions for people experiencing homelessness, including tobacco reduction programs (Charron et al., 2018), decreasing traumatic brain injury rates among cisgender and transgender women involved in sex trade work (Baumann et al., 2019), and normalizing drug use in shelters as part of harm reduction interventions (Bardwell, Boyd, Kerr, & McNeil, 2018). In this last study, researchers examined the perspectives of people who use drugs residing in two emergency shelters and found peer support was related to relationship-building and trust, that people felt increased safety using drugs in front of peer support workers, and that the dynamics between worker and client felt more equitable and balanced (Bardwell et al., 2018).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=757#h5p-84
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=757#h5p-85
Community-based research that looked at why peer support workers engage in these positions found three key motivators, including obtaining a sense of purpose from helping others, being an inspiration for others, and feeling a sense of belonging (Pauly et al., 2021). These sources of motivation were important in giving meaning to the work and helped to provide a buffer against the stressors that go along with these roles (Pauly et al., 2021). Having a buffering effect is important, as peer work has also been found to have common challenges related to inadequate financial compensation, lack of respect and recognition at work, having their own housing challenges, an inability to access or refer clients to other resources, and constant exposure to death and trauma related to the work (Mamdani et al., 2021).
When researchers study peer support work they often describe it in complicated ways, identifying the positive benefits for clients but also the toll it takes on peer support workers themselves. For instance, Kenney et al., (2019) have noted that peer workers, such as at overdose prevention sites, provide expertise that can enable communication, foster harm reduction practices, and promote health benefits, yet these positions are often not well compensated and can result in grief, trauma, and burnout over time. Likewise, Greer, Buxton, Pauly, and Bungay (2021) note that peer harm reduction work is complex and demanding because they are at the forefront of support and that, while these roles can be rewarding, they also tend to lack definition and clarity within organizational structures.
Moving beyond peer support work can also be a challenge. In the video below, from the Ontario Harm Reduction Network, Stephanie explains the stigma that surrounds the word “peer” on a resume. While she discusses this in relation to harm reduction, the same stigmas would likely apply to peers working in fields related to mental illness and/or sex trade work. As you watch this video, we encourage you to consider what could be done to reduce this stigma.
In the preceding video, Stephanie explained that peer work is not always highly regarded in the labour force. Consider for a moment that you are on a hiring committee at work. Someone who is highly qualified applies and has harm reduction and sex trade peer support work on their resume. Your fellow hiring committee member argues they should not be considered for an interview because of their history with drug use and sex trade work. What could you say to persuade them to give the person a chance? How could you convince them that peer support work is valuable?
In this section we examined the role of case management in Social Work, beginning with a brief definition from the Canadian Observatory on Homelessness and a longer featured reading from the Global Social Service Workforce Alliance (2018). We traced the early roots of case management and considered the qualities that make someone a good case manager. We posed this section’s guiding question, “What is the role of case management in Social Work?” to three researchers, all professors in the field of Social Work, and they each independently distinguished case management from “good” case management.
What, then, is the role of good case management in Social Work?
Good case managers help their clients to identify what kinds of supports they need and then make connections to them. These support interventions may take many different forms, and what works for one client will be different than what works for another. Good case management requires flexibility and a commitment to providing on-going support for clients.
We concluded this section by shifting to consider the important, yet under-recognized, role of peer support as an affiliated helping profession. While peer support workers generally do not have the education and credentials of Social Workers, they offer a uniquely positioned set of skills. Notably, peer support workers are increasingly being used in harm reduction, sex trade, and mental health programs. This work is complex in that it can offer many benefits but also has many associated challenges as well.
Ultimately, good case management is about recognizing it cannot be done alone. As Dr. Firang said, no Social Worker is expected to be Hercules or Superman. Rather they must reach out to other agencies, case managers, and peer support workers in the community to best support their clients.
Click the link below to listen to all of the researchers answer the question “What is the role of case management?” in audio format on our podcast!
94
The public perception of homelessness is often that of an unkempt adult man sleeping on the sidewalk, with a paper cup next to him for collecting coins. It is true that many people who experience homelessness – and particularly visible forms of homelessness – are single adult cisgender men. Their experiences and needs are important for Social Workers to understand and consider. However, beyond that, there are other special populations that require consideration.
The use of the word “special” here is not to connote a sense that they are more important but rather that their experiences and needs are unique and cannot be addressed using the standard models and approaches that have been created for single adult men. In other chapters, we consider some of these special populations, such as youth, Indigenous persons, women, and LGBTQ2S+ persons. We can see that for these groups, who are at increased risk of homelessness, their needs differ from single men. For instance, youth may not be able to live independently, Indigenous persons might need cultural supports related to intergenerational trauma, women might have additional childcare responsibilities or risk factors, and LGBTQ2S+ persons might be threatened and discriminated against in social service settings. These special populations are discussed further in the chapters on Child & Youth Studies, Indigenous Studies, and Gender & Queer Studies, respectively.
However, there are additional special populations who are at high risk of homelessness and whose experiences and needs will vary. Before you continue, we encourage you to pause here and reflect on the role of Social Workers in supporting a diverse range of people experiencing homelessness. What special populations might Social Workers encounter, and what makes their experiences separate or distinct from others?
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=759#h5p-86
We would like to begin this section with a note about the importance of intersectionality. This means that people may fall into multiple overlapping categories at the same time. Consider the special populations above, for instance. A person may be young, identify as a transgender woman, and be of Indigenous ancestry. Rather than thinking of these identity markers as simply being layered on top of one another, we need to consider how they interact in dynamic ways that shape a person’s experiences of homelessness. In this brief video, American Civil Rights advocate and UCLA Professor Kimberlé Crenshaw explains intersectionality further.
In the first video, Dr. Cheryl Forchuk explains that many special populations are among the hidden homeless and that it is essential we understand how their unique experiences require specialized and tailored responses. When providing support for people experiencing homelessness, there is no “one size fits all” approach.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk speaks about her research identifying hidden homeless populations. Dr. Forchuk argues that hidden homelessness is always contextual but that some groups are more commonly reported to be in this category than others, such as Indigenous peoples, youth, and women or families fleeing domestic violence. She discusses the increasing rates of first-time homelessness in rural communities, resulting from pandemic job losses and the rising cost of the housing market. While it may be tempting to try to find one solution to homelessness that meets the needs of all individuals, Dr. Forchuk cautions that it is often more effective to tailor our responses to the needs of communities, subpopulations, and individuals. This video is 2:30 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Which special populations are at high risk of homelessness?
Social Workers can best support their clients by understanding that their unique characteristics require equally unique responses. As Dr. Forchuk noted, what works for one group will not necessarily work for another. This is evident with the rise in family homelessness that has occurred throughout Canada in recent years. Factors such as a lack of affordable housing, increasing housing and rent costs, and job losses due to COVID-19 all have the potential to create housing instability for families. Low-income families, in particular, are often precariously housed or at risk of homelessness because of the disparities between their income and the costs of living (Paradis, Wilson, & Logan, 2014). Family homelessness is not often the result of addiction, but poor mental health and high levels of stress have been found to be prevalent amongst family members residing in shelters (Sylvestre et al., 2017). There are also gendered pathways into family homelessness, such as for single mothers caring for children (Milaney, Lockerbie, Fang, & Ramage, 2019).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=759#h5p-88
Sylvestre et al., (2018) have interviewed people experiencing family homelessness and found that their experiences prior to residing in a shelter were characterized by vulnerability, instability, and isolation. Their research further showed that once residing in an emergency shelter, these families faced new challenges related to living in an environment that was restrictive, noisy, chaotic, and lacking in privacy. These family members described disruptions in their lives, relationships, and routines but also had hope about the future.
Emergency shelters offer an important service but are not ideal locations for families to live in long-term, in part because they are stressful places (Polillo et al., 2018). If you were a Social Worker who was supporting a family experiencing homelessness, what steps could you take to help them move into stable and secure affordable housing of their own? What challenges do you think you might encounter in connecting families (and individual members) with supports in the community? How might working with a family be different than working with a single adult?
As you consider the questions above, we invite you to watch this brief video from “The Columbian” about a woman and her children residing in an emergency shelter in Vancouver. We encourage you to think critically from the perspective of the individual family members, as well as from the perspective of a Social Worker who may be asked to offer support through case management.
Family homelessness may be the result of a specific incident, such as a job loss or eviction, or it may be rooted in intergenerational experiences of deep poverty. Families may access social assistance, such as governmental income support programs, across multiple generations within a family (Baker Collins, Smith-Carrier, Gazso, & Smith, 2020). It is important to understand that what Gazso et al., (2019) call the “generationing” of social assistance interacts within broader contexts of gender, race, Indigeneity, and class. We see this in the next video in which Dr. Nick Kerman discusses findings from research he and his colleagues have conducted about families experiencing homelessness.
In this video, Dr. Nick Kerman discusses the characteristics associated with family homelessness in Canada. Among Canadian-born families there is a high rate of single-mothers with children, which comprises one of the groups at highest risk of homelessness in terms of the family unit. Among newcomer and immigrant families, it is more common to see two-parent headed families that may have been initially supported in the process but were not connected with housing that would remain affordable and stable over time. This video is 1:59 and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: Which special populations are at high risk of homelessness?
Compared to other populations, Jadidzadeh and Falvo (2019) have found that families exiting Calgary’s homeless system of care required support for the least amount of time. The length and types of support that families need will differ from other populations, such as single adults, and what one family needs will be different than what another family needs. This becomes apparent when we consider the experiences of immigrant and refugee families. In a study of 75 families experiencing homelessness in Ottawa, researchers found a large number of newcomer families, who were larger and more likely to have two-parent structures compared to Canadian-born families experiencing homelessness (Sylvestre et al., 2017). An ethnographic participatory action research study, also conducted in Ontario, explored the experiences of 11 immigrant families with housing challenges and found five key themes emerged, related to life challenges, lack of understanding of the system, difficulty with conflict resolution, escaping as a solution for hardship, and the need to reduce family homelessness amongst immigrants (Forchuk et al., 2021b).
To study pathways for refugees’ descent into homelessness in Edmonton, St. Arnault and Merali (2019a) conducted interviews with 19 adult refugees from various countries who experienced homelessness after their arrival and also conducted focus groups with housing providers in the area. They found that there were several key critical incidents that could contribute to homelessness after arrival, such as interpersonal conflicts with their sponsor, service provision interruptions with their case worker, or housing issues such as increased rent, discrimination from landlords or the community, and inhabitable housing conditions. The authors note that these critical incidents are exacerbated by the lack of available affordable housing, language barriers, and limited knowledge about housing systems in Canada which compound the critical incident, resulting in homelessness (St. Arnault & Merali, 2019a).
Findings from a Toronto-based study found that newcomer youth were diverse in country of origin, racial and ethnic background, sexual orientation, level of education, and pathways into homelessness (Ratnam, Fitzpatrick, & Thang, 2018). Yet, despite this diversity there are many negative stereotypes and generalized discrimination that immigrants and refugees face within Canada. Researchers who undertook a systematic review of the literature found that refugees’ well-being is negatively impacted by societal discrimination, leading to feelings of helplessness, mistrust, and anger, which may lead to avoiding health care and social services even when needed (da Silva Rebelo, Fernández, & Achotegui, 2018).
The struggles of immigrants and refugees often overlap with the challenges of other racialized populations within Canada. For instance, institutional ethnography shows that growing up in social housing (re)produces conditions of oppression that can exacerbate housing precariousness and exclusion, including a belief among economically marginalized and racialized youth that the state is not invested in their safety (Nichols & Braimoh, 2018). In the next video, Dr. David Firang discusses challenges of racialized and newcomer Canadians as they pertain to housing precarity.
In this video, Dr. David Firang discusses the increased risk of homelessness among Northern-located Indigenous communities and racialized or newcomer Canadians. He cautions that the way we understand the concept of being ‘at-risk’ depends on the definition of homelessness that we use. This video is 3:06 in length and has closed captions available in English.
Key Takeaways – Dr. David Firang: Which special populations are at high risk of homelessness?
Immigrants, refugees, and racialized Canadians are at increased risk of homelessness. If you were a Social Worker whose role involved supporting clients within these populations, how could you use a culturally informed approach to identify and connect them with appropriate, respectful, and inclusive services? What would you do if there were no culturally specific services located in your community? What tools and resources could you turn to for guidance?
Social Workers are well-positioned to support immigrant, refugee, and racialized Canadians in identifying and accessing supports within their communities and more broadly through resource networks. Dr. Firang, for instance, has studied the impact COVID-19 has had on the financial and emotional stability of international students in Canada and argues that Social Workers can improve the situation by serving as strategist / brokers (to identify underlying structures that marginalize international students and help connect them with community supports), advocate / activist (to provide leadership and help create compassionate institutional arrangements), and educator / coordinator (to provide information and resources to raise awareness about international student challenges, such as the risk of housing loss) (Firang, 2020).
The needs of racialized and newcomer Canadians will differ from non-racialized Canadian-born citizens. Whether at risk of losing housing due to pandemic closures or residing in a shelter after fleeing violence in one’s homeland, these differences require tailored responses from Social Workers. Ratnam et al., (2018) encourage people in helping professions to engage the voices and experiences of their newcomer clients at all stages of the service continuum including casework, program planning, and systems planning. Hasford, Amponsah, and Hylton (2018) have similarly written that when working with African Canadian young people, service providers need to engage with critical reflexivity and praxis as a means of connecting with young people and helping them access culturally relevant resources while advocating for structural and systems level change.
Social Workers have an important role to play, not only in advocating and supporting racialized and newcomer clients, but also in recognizing the strengths and resourcefulness they bring to challenging circumstances. Researchers examining how people cope with the compounding stressors of racial discrimination, homelessness, and mental illness found that participants described hope, optimism, self-esteem, confidence, insight into their challenges, and spirituality as being instrumental in overcoming their challenges (Paul et al., 2018). St. Arnault and Merali (2019b) also similarly found four interrelated pathways refugees in Canada use for exiting the cycle of homelessness, including drawing on religiosity and spirituality, using creative problem-solving, asking for help, and engaging in self-advocacy.
As professionals working with refugees and immigrants, in particular, Social Workers should use social justice orientated approaches to help their clients realize their fundamental human right to safe and secure housing (St. Arnault & Merali, 2019b). As much as possible, Social Workers should develop their expertise in working with refugee and new Canadians, as research has demonstrated this promotes better experiences for clients, in their migration journey (Oudshoorn et al., 2020). Key to this work is understanding how the range of issues these individuals face put them at higher risk of homelessness. We must consider their housing career, such as the places they have lived, beginning with their experiences in their homeland (Firang, 2019). We must also remember the importance of intersectionality. In the video that follows Dr. Katrina Milaney further explores the connections between people at risk of homelessness, including racialized individuals and other potentially vulnerable groups.
In this video, Dr. Katrina Milaney urges us to consider the common threads that connect groups of people who are at high-risk of homelessness, such as racialized individuals, people with mental health issues, people living in poverty, women, children and youth, and people with disabilities. Notably, the themes that cross-sect these groups are higher rates of trauma, limited access to social supports, potentially unhealthy relationships, and a lack of access to affordable housing. Dr. Milaney identifies seniors as a high-risk group, whose vulnerability to homelessness can be increased or decreased in accordance with their level of social support and community involvement. This video is 2:14 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: Which special populations are at high risk of homelessness?
As Dr. Milaney explained, older adults have specific shelter and housing needs (Humphries & Canham, 2021). We encourage you here to pause for a moment and consider two questions. First, what specific needs do you think older adults might have related to their housing? Second, what do you think qualifies as the age of an “older” adult? Researchers examining the first question – of what needs exist – have tended to use 50 as the age at which a person experiencing homelessness is considered an older adult. The reason for this, as discussed in more detail in the chapter on Primary Care & Nursing, is that homelessness impacts people’s health in such a negative way that many experience chronic illness at a much younger age than the housed population and tend to have significantly shorter life expectancies (Hwang et al., 2009). Experiencing homelessness at age 50 is comparable to being an advanced age.
In the preceding video, Dr. Milaney spoke about the reasons seniors are a high-risk group that require special consideration. She and her team recruited 300 participants from a Calgary-based shelter, of whom 142 were 50 or older and 158 were under 50 (Milaney, Kamran, & Williams, 2020). They found that older participants reported complex health issues and faced significant barriers to accessing care, such as pertaining to waitlists, insufficient finances, and not receiving help even after asking. Dr. Milaney and her colleagues (2020) further found that older respondents reported trauma in their childhoods at rates 2 ½ times the general population and required culturally appropriate and trauma-informed interventions to address the diversity of their needs.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=759#h5p-89
In another study, Burns and Sussman (2019) conducted in-depth interviews with 15 adults who were 50 or older to learn about the pathways into late-life homelessness. Through this research they identified two divergent pathways. In the first pathway, some people had a gradual entry into homelessness in which they endured many years of struggle related to poor housing, a lack of social support, and social distress. The authors note that these individuals have often reached out for support but had limited success, indicating these adults’ risk of homelessness may be reduced by strengthening social supports. The second pathway was a rapid entry into homelessness, in which people reported that multiple unanticipated losses threatened their economic and social resources with little warning. While these individuals reported having social networks that could help buffer the effects of loss, they resisted asking for help to protect their independence.
Social Workers play a vital role in supporting older people who are experiencing homelessness to connect with supports within their community. Consider the gradual and rapid pathways (Burns & Sussman, 2019) as you watch this video entitled, “Beyond Housing” about seniors experiencing homelessness. Again, we encourage you to consider this video from the perspective of the individuals experiencing homelessness, as well as from the perspective of a Social Worker who might be advocating and facilitating connections on their behalf.
Experiencing homelessness later in life can evoke feelings of grief, shock, despair, and anger which must be acknowledged and validated for the person to address and move beyond them (Burns, Sussman, & Bourgeois-Guérin, 2018). When people experience homelessness at the age of 50 or beyond, their primary needs are for accessible housing that can be adapted to their health challenges, income supports, access to health care and/or homecare, reliable transportation, and non-discriminatory support services (Canham et al., 2018).
Accessible housing and supports are important for people over the age of 50, but they also are needed for people of all ages with disabilities as well. Government financial assistance programs may not adequately meet the cost of living for people with disabilities (Roy et al., 2020), even though they may be the sole source of income for those who are unable to work. When people do not have adequate access to income supports, their risk of homelessness increases. It is noteworthy that in a study of 172 adults with mental illness residing in a Toronto-based emergency shelter, the 16% whose standardized test scores indicated borderline or lower intellectual functioning also had lifetime homelessness lengths that were nearly double those in the study with higher intellectual functioning (Durbin et al., 2018). Social Workers can support people living with disabilities by connecting with Housing First programs. Research has shown that for adults living with intellectual and developmental disabilities, participating in cross-sector interventions that offer immediate access to housing and supports results in housing stability and increased quality of life (Reid et al., 2021).
Access to secure and affordable housing is critical to the wellness of all persons experiencing homelessness, but the special populations discussed in this section require housing that is tailored to their specific needs. We have seen how families, racialized and newcomer Canadians, seniors, and persons with disabilities have different pathways into homelessness, experiences in the system, and needs for transitioning out of homelessness. The final special population that Social Workers might engage with, through case management or other frontline activities, are Veterans. Analysis of the physical health of Veterans enrolled in the At Home / Chez Soi study found that they presented with 5 physical health problems on average, including dental problems, head injuries, musculoskeletal injuries, and foot problems (Bourque et al., 2017). In the next video, Dr. Cheryl Forchuk discusses her team’s work implementing Housing First interventions for Veterans, and the lessons they learned.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk discusses her ground-breaking research on Veterans who experience homelessness. While research out of the United States often cites PTSD as a contributing factor, in Canada homelessness is more often linked to alcoholism that develops over time as a part of socializing within the military. When Canadian Veterans experiencing homelessness are asked what supports they need, they identify structure, re-establishing a sense of self-concept, and peer-support from others who have similar experiences. As Dr. Forchuk’s research shows, when Canadian Veterans are listened to, and the supports they identify are put in place, they can successfully exit homelessness. This video is 7:13 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Canadian Veterans experiencing homelessness
After hearing Dr. Forchuk discuss her team’s work with Veterans, we invite you to learn more about the project in this section’s featured reading from the Journal of Military, Veteran and Family Health.
Forchuk, C., Richardson, J., Atyeo, H., & Serrato, J. (2021a). Qualitative findings from a housing first evaluation project for homeless veterans in Canada. Journal of Military, Veteran and Family Health. Advance Access Article.
Veterans are a special population who have unique experiences that require tailored responses. Dr. Forchuk and her team (2021a) have evaluated the effectiveness of Housing First, with different types of supports, over a two-year study in Toronto, London, Calgary, and Victoria. They have found that along with permanent housing, the Veterans who participated identified a need for harm reduction support, more mental health programming, and peer support from others with military experience (Forchuk et al., 2021a). Additional analysis of the data from this study further indicated that Veterans prefer regimented structures in support agencies and want services that are located close enough to access but not in an area associated with known substance use (Marsella, Forchuk, & Oudshoorn, 2020).
When engaging Veterans in case management, such as aligning services and housing supports, it is important that Social Workers understand and incorporate their preferences into the support plans. Consider this as you watch the next video, “Functional Zero Veteran Homelessness” from the Canadian Alliance to End Homelessness.
We began this section by asking you to consider what special populations are at higher risk of homelessness. This question is important to consider because Social Workers need to be able to adjust their approach to individual clients to offer tailored support. We noted that the common perception of a single adult cisgender man experiencing homelessness is perfectly valid. However, what works for him will not work for everyone. A common theme throughout this book – that emerged clearly in this section – is that there is no “one size fits all” approach for supporting people who are experiencing homelessness. Rather, we need to think about their individual needs and what will help them personally.
We considered families as a special population and saw that family homelessness is often the result of factors like job loss and financial strain that overwhelms the family’s ability to maintain stable housing. We learned that there are a high percentage of refugee and immigrant families experiencing homelessness, and that they are best served when Social Workers use culturally sensitive approaches that connect them to meaningful services and supports within the community. We then considered the needs of older adults, which in relation to this population means those 50 and above and saw that there are different pathways that lead to later life homelessness, requiring different solutions or pathways back out. Similarly, we discussed how people with disabilities are an over-represented group amongst people experiencing homelessness, in large part because of an inability to work and limited financial assistance. Finally, we considered Veterans as a special population who benefit from Housing First approaches augmented with harm reduction and peer support.
There are additional special populations discussed throughout this book as well, including youth, Indigenous persons, LGBTQ2S+ persons, and women. A key takeaway message here is that people who experience homelessness in Canada are diverse. Social Workers can help these individuals best by recognizing their diversity of backgrounds, experiences, and unique needs.
Click the link below to listen to all of the researchers answer the question “Which special populations are at high risk of homelessness?” in audio format on our podcast!
95
If you have ever had a job, it is likely you have experienced some degree of stress related to your employment. Perhaps you have had to respond to upset customers, deal with a micro-manager boss always checking up on you, or clean up a super gross spill in aisle 3. Whatever the position, stress is a common part of having a job. However, feeling burned out goes beyond normal levels of stress one would expect to have at work.
When you hear the term “burnout,” what comes to mind? Why do you think it is more common in helping professions, such as Social Work, Emergency Response, and Health Care? Do you think it is an inevitable outcome of working in these fields, or are there approaches we can use to help support workers avoid it? Before you continue through this section, we invite you to respond to these questions using the space below. You may write as little or as much as you wish.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=761#h5p-90
How can support workers prevent becoming burned out? This question could have been situated in multiple chapters of this book. Working in the homelessness sector, whether related to housing, mental health, physical health, emergency medicine, addictions, or frontline support work, can have a negative effect on service providers’ well-being over time. People often enter these professions with the goal of wanting to help make a difference in other people’s lives and they bring a great deal of enthusiasm and passion to the work. However, homelessness results from negative life circumstances and trauma which require on-going investments and support from professional care providers. The level of commitment required of support workers can be incredibly high and take a toll on their own sense of wellness. In the first video of this section, Dr. David Firang explains why he chose a career as a Social Worker and how reflexivity helps him manage the challenging aspects of the profession.
In this video, Dr. David Firang argues that despite being a difficult and stressful career, Social Work can also be thought of as a helping profession. Social Workers may come from different cultures and backgrounds, and hold different values and beliefs than the clients they work with. To prepare their students for this, those who teach Social Work can provide training in anti-oppressive practice, diversity, equity, and inclusion. Once in the field, good social workers will reflect upon this education to better understand their own social location, identity, values, and beliefs, and to try to draw the deficit gap in order to relate with all their clients. This video is 2:43 in length and has closed captions available in English.
Key Takeaways – Dr. David Firang: How can support workers prevent becoming burned out?
Social Workers, and others in frontline homelessness related professions, provide care and support for people with complex needs. At the same time, we must consider what they themselves need in order to be able to undertake this demanding and important work. We invite you now to read the blog post written by Justine Levesque, Research and Evaluation Officer at the Canadian Observatory on Homelessness entitled, “What are the needs of frontline workers in the homelessness support sector?” This is the first in a series of 3 blog posts that report on findings from a recent evaluation. We encourage you to read the report that is linked to this blog as well, to learn more about the study and its findings.
Click the image below to open a new window and read the full blog post, “What Are the Needs of Frontline Worker in the Homelessness Support Sector?” by Justine Levesque.
While working in the homelessness sector can be very rewarding, it also can lead to post-traumatic stress disorder (PTSD), burnout, and discrimination as we saw in the blog post above. These feelings can emerge as support workers listen to the stories of their clients, make outreach visits to people in marginal spaces within the community, or lose clients to premature deaths related to poor health, drug overdose, or violence committed against them. The accumulation of stress from these circumstances can take a toll on support workers, who often care deeply about the people they support. Dr. Kelli Stajduhar explains this further in the next video.
In this video, Dr. Kelli Stajduhar tells the story of walking into a colleague’s office to find her visibly upset. As a front-line worker she had experienced numerous losses. Although brief, Dr. Stajduhar’s impactful message in this video is that workers must recognize the impact of the loss they experience and understand it within the context of grieving. This video is 0:34 in length and has closed captions available in English.
Key Takeaways – Dr. Kelli Stajduhar: Workers, loss, and grieving
Suffering continual losses can create feelings of grief in people working in frontline helping positions within homelessness sectors. Dr. Jeannette Waegemakers Schiff, who has extensively studied the impact of frontline work on service providers, argues in the next video that the term “burnout” is not sufficient to capture the severity. Rather, she notes that we should think of workers as having sustained a workplace injury.
In this video, Dr. Jeannette Waegemakers Schiff argues that workers deal with tremendous psychological and moral injury on a regular basis. Rather than referring to it as burnout, she suggests we should reframe the issue to see people having been injured as a result of the work they do. This would shift not only our understanding of the issue, but our responses to it as well. This video is 0:41 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: Let’s change the way we think about burnout
The impacts of support work are complex and have to be understood in a dynamic way. For instance, Waegemakers Schiff and Lane (2019) have noted that while support workers may experience vicarious trauma, compassion fatigue, or burnout, researchers have not widely considered how they might be experienced collectively altogether. To address this, they undertook a survey of 472 frontline workers in homelessness agencies and found high rates of post-traumatic stress disorder (PTSD) related to their work directly with clients. We invite you to learn more about the study and its findings in the featured reading below. In the video that follows, lead author Dr. Jeannette Waegemakers Schiff, speaks about her follow-up study on support worker wellness in homelessness sectors during COVID-19.
Waegemakers Schiff, J., & Lane, A. M. (2019). PTSD Symptoms, Vicarious Traumatization, and Burnout in Front Line Workers in the Homeless Sector. Community Mental Health Journal, 55(3), 454–462.
In this video, Dr. Jeannette Waegemakers Schiff clarifies that burnout is not the issue, but rather it is traumatic stress that is harming frontline workers. She notes that current research indicates over half of homelessness sector workers across the country suffer from rates of traumatic stress that would qualify for a Post Traumatic Stress Disorder (PTSD) diagnosis. Dr. Waegemakers Schiff explains that with burnout people are disenchanted, lose compassion, and no longer care about helping people. In contrast, people suffering from traumatic stress continue to care but are unable to help because they suffer from psychological injury and high levels of depletion and stress. Having in-person contact with colleagues and supervisors can help lessen the effects of stressful working conditions, and research has shown service providers who worked remotely during COVID-19 particularly felt the effects of traumatic stress. In the absence of personal contact, Dr. Waegemakers Schiff argues it is important for workers to identify self-care strategies, such as meditation, that work for them. Managers and supervisors must recognize the signs of traumatic stress in their employees and implement approaches to help them. Dr. Waegemakers Schiff concludes that trauma-informed care is not just about how service providers look at their clients, it is also about how they look at themselves. This video is 6:33 in length and has closed captions available in English.
Key Takeaways – Dr. Jeannette Waegemakers Schiff: How can support workers prevent becoming burned out?
Dr. Waegemakers Schiff explained that traumatic stress is a more pressing issue than burnout, because with burnout people no longer care. With traumatic stress, they still care but are unable to accomplish what they feel they need to do. In our everyday language as a society, we tend to use “burnout” as a catch-all for people who are feeling overwhelmed and over-burdened at work. Do you agree with Dr. Waegemakers Schiff that we should be more precise with the language we use to describe people’s experiences? Why do you think “burnout” has become the collectively preferred term over the more accurate “traumatic stress?”
In this section, we use the term “burnout” because of its widespread recognition, but we are also very aware that it does not capture the complexity of people’s experiences. For that reason, we also refer to traumatic stress, compassion fatigue, and grief as well. We encourage you to note when these different terms arise and the meanings behind them. Burnout, compassion fatigue, and traumatic stress are all prevalent experiences for people working in frontline support roles with individuals experiencing homelessness. This was particularly evident during COVID-19, as homelessness sector workers self-reported rates of mental health problems that were similar to those of health care practitioners (Kerman, Ecker, Gaetz, Tiderington, & Kidd, 2021). When service providers do experience these mental health issues it is important to note it is not because they lack individual coping skills. Rather, these issues arise from the structure of the work itself and not having institutionalized practices aimed at identifying and reducing these problems amongst workers.
Malenfant, Nichols, and Schwan (2019) have written about the emotional and relational work that occurs within homelessness sectors and argue that whether people’s work is recognized and valued within an organization is critically important. In the concluding section of this article, they write, “It is the valuation of the work within organizations that contributes to shifts in social policies, practices, and people’s experience and pushing back against the erasure of connections between the daily work of people – that work that goes into maintaining all the moving pieces of an organization – that should be recognized as a key part in the process of contributing to social change” (Malenfant et al., 2019, pg.53). In this next video, Dr. Naomi Nichols, co-author of this study, discusses how these mental health challenges are structural issues that have been exacerbated during the COVID-19 pandemic.
In this video Dr. Naomi Nichols argues that burnout occurs in care sectors when people try to do their jobs without adequate resources, leading them to have to work in ways that conflict with their values. For instance, during the COVID-19 pandemic the need for services rose while the provision decreased, causing social workers to shift towards planning rather than doing. Dr. Nichols argues that while burnout is a structural issue, it is felt as an adjustment disorder at the level of the individual body. People who work in frontline services may themselves have previous experiences of homelessness, be paid low wages for the work they do, and be under economic pressures that exacerbate the work-related stress they experience. This video is 6:38 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: How can support workers prevent becoming burned out?
It is clearly evident that frontline support work is challenging. This does not mean that people should not undertake this kind of employment, but rather that when they do they need to have appropriate supports in place for themselves. Researchers have written, “Stress and trauma are often side effects of front-line youth work. While these issues cannot be totally eliminated, strategies and practices are emerging to deal with them. Interventions that have been shown to reduce stress, burnout, compassion fatigue, and vicarious trauma are psychoeducational and skill-based, and involve training in mindfulness, cognitive behavioural therapy, and psychological first aid. Mental fitness, self-care practices, and robust social supports serve as protective factors” (Cerswell Kielburger, Rockman, & Baranek, 2018, pg. 171).
As the guiding question for this section, we asked you to consider how support workers can prevent becoming burned out. There are many steps that support workers, and their supervisors, can take to reduce burnout, compassion fatigue, and traumatic stress related to frontline work within the homelessness sector. Consider this TEDx talk entitled, “How to manage compassion fatigue in caregiving” by Patricia Smith. While this video is not about working in the homelessness sector, the key points are highly relevant. We encourage you to think about how the concepts could be used to improve the well-being of Social Workers and others who undertake support roles related to homelessness.
We have heard from different people discussing issues related to burnout, compassion fatigue, and traumatic stress. Have you ever experienced these in your own life? What strategies have you used to cope with these feelings?
There are many specific approaches that can be used to reduce the risks of support workers becoming burned out, feeling compassion fatigue, or experiencing traumatic stress. These approaches exist at both the individual and workplace levels. In the two videos that follow Dr. Jeff Karabanow and Dr. Nick Kerman both discuss steps that support workers and managers can take within homelessness sector agencies to reduce the negative mental health burdens on employees.
In this video, Dr. Jeff Karabanow explains that frontline service provision entails emotional labour and that while people enter the field because they care deeply, they are faced with discriminatory and oppressive structures that can lead to compassion fatigue. He notes that while there are some strategies individuals can use, such as exercising and eating well, preventing burnout should not be left to individuals. Rather, Dr. Karabanow argues that organizations should support their staff by being deeply intentional about check-ins, time off, holding team meetings, offering training and educational leaves, and offering supports that help workers feel connected. Burnout can come on quickly, particularly with the stresses of COVID-19, and organizational leaders can help by engaging with staff to show they are listening and willing to work together to identify and implement solutions. This video is 5:13 in length and has closed captions available in English.
Key Takeaways – Dr. Jeff Karabanow: How can support workers prevent becoming burned out?
In this video Dr. Nick Kerman explains the importance of boundary-setting for service providers, to avoid burnout. He notes that good boundary setting means not taking calls or emails while off work and trusting that a team member who is on duty will be able to handle situations that arise. Dr. Kerman notes that boundary setting allows service providers to rest and recharge. He argues that organizations have a role to play in supporting workers avoid burnout. Strategies they can use include offering flexible time off, increasing wages to reflect the importance of the work, and ensuring supervisors are prepared to recognize and respond to stress and trauma in their employees. This video is 4:47 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: How can support workers prevent becoming burned out?
Identifying resources and champions within an organization can increase awareness of the need for mental health promotion and strategies for reducing burnout and its associated challenges (Cerswell Kielburger et al., 2018). This brief video from the National Alliance to End Homelessness shows the measures that three homelessness sector agencies implemented to protect their frontline support workers through the COVID-19 pandemic.
There are many different approaches that support workers and their managers can take to reduce the impact of burnout, traumatic stress, and compassion fatigue. As we have heard, it is best to select the ones that resonate and it can be useful to start small (Cerswell Kielburger et al., 2018). We end this section with a hopeful message from Dr. Nick Kerman, about the importance of recognizing and celebrating the small wins in frontline support work.
In this video, Dr. Nick Kerman argues that working in the homelessness and supportive housing sectors can be stressful and demanding, because service providers are often helping clients work towards achieving long-term goals. He notes that one of the best, yet overlooked, approaches for service providers to avoid burnout is to focus on the small wins. These are moments that occur daily, such as when a client smiles despite usually being withdrawn, shows up for an appointment despite competing obligations, and/or fills out an application for housing or employment. Dr. Kerman encourages service providers to be mindful of small wins because they show a client feels supported, has formed a trusting relationship, and is making progress. This video is 2:38 in length and has closed captions available in English.
Key Takeaways – Dr. Nick Kerman: Recognizing the small wins

Check out these wellness resources and toolkits:
In this section, we explored the question, “How can support workers prevent becoming burned out?” We began by considering the challenging nature of support work with people experiencing homelessness, and saw that people enter this profession with a sense of passion and purpose. Over time, the accumulation of stress and loss can lead to feelings of grief which is akin to a workplace injury. We heard that the term “burnout” – while commonly used to describe a wide array of feelings – does not capture the full extent of what support workers experience. Rather, traumatic stress and compassion fatigue were emphasized as being terms that better capture the mental health impacts that can result from this kind of support work.
While these mental health outcomes may be felt at the individual level – by workers themselves – we emphasized that this is not an individual level deficiency. Rather, we heard from researchers that burnout, traumatic stress, and compassion fatigue are rooted in organizational practices. This suggests that workers may suffer more in workplaces where they feel undervalued, but also that employers can implement practices to help buffer these effects faced by their staff. We heard from a number of researchers that there are many strategies individuals can use, such as journaling, exercising, and boundary setting, as well as strategies managers can take to reduce mental health burdens, such as through team debriefings and regular check-ins with staff. The key is to find the approach that works for the individual and/or their team. Taking time to notice and appreciate the small wins is where we ended the chapter, but it is a great place to start one’s wellness journey.
Click the link below to listen to all of the researchers answer the question “How can support workers prevent becoming burned out?” in audio format on our podcast!
96
Liam
Let’s return to the scenario that involves Liam and his Social Worker. Tanya entered the profession to make a difference in the lives of others. She is very committed to getting the services that Liam needs and feels a professional obligation to the other service providers as well. As Liam enters the centre Tanya approaches him with a smile and acknowledges that she is happy to see him. He appears a bit startled but returns the smile and engages in conversation. Tanya invites him to share a cup of coffee as they move to one of the tables.
This scenario, about Tanya needing to make a connection today, brings to mind Dr. Kerman’s video about taking time to appreciate the small wins. He says even minor acts like having a person smile at you or show up for a scheduled meeting can show you are making an impact. Liam feels ‘seen’ as a person and is pulled into a context where he can begin to engage with support services again, hopefully, with more consistency.
As front-line workers, Social Workers need to embrace small wins even while desiring a big change. Frustrations can build up when the small wins do not seem to be enough. Tanya takes the time to reflect on the small wins as well as consider the big picture for Liam. Tanya may also acknowledge for herself that Liam may be person who needs help but who may not be able to organize the support pieces for themselves. She uses mindfulness exercises when she is feeling overwhelmed and stays in close contact with other care providers for her own well-being. Social Workers and other front-line care providers can learn a lesson from the airline industry who remind us on every flight, that when the oxygen mask drops down in a time of crisis, to put our own on first before assisting others.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1190#h5p-87
97
We began this chapter on Social Work by discussing the challenging nature of the work. Even after reading that, you made it this far! We appreciate you continuing through, even with that warning, because although frontline support work is difficult, it is also a tremendously important role in the homelessness sector.
At the start of the chapter, we introduced you to the composite character Liam, who had many complex issues but was having difficulty connecting with services. The scenario was presented as an entry point into thinking about the complexity of frontline support work with people experiencing homelessness. We returned to Liam’s story again at the end to demonstrate how it can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada.
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “What is the role of case management in Social Work?” Here we learned about the roots and definition, and importantly that it is not enough to talk about the role of case management – we need to talk about good case management. Good case managers walk alongside their clients, advocate for them, and help them identify and connect to services they need within the community. As a critical part of the team, peer support workers offer an important, yet under-recognized, set of skills that can help people navigate programs for harm reduction, sex trade work, and mental health. Support workers do not need to be Hercules or Superman, but they do need to work with others to offer their clients the best care possible.
Next we asked, “What special populations are at high risk of homelessness?” We noted at the beginning of this section that they were special because of the unique needs and experiences that differentiated them from single adult cisgender men, for whom many programs are designed. In this section, we considered families, refugees and racialized new Canadians, adults over 50, persons with disabilities, and Veterans. Each of these populations is at higher risk of homelessness and benefit from support interventions that are tailored to them, rather than designed to be “one size fits all.”
Finally, we asked, “How can support workers prevent becoming burned out?” In this final section, we looked at the mental health challenges of burnout, traumatic stress, and compassion fatigue that can arise from repeated losses and stress related to frontline support work. While we noted that this question could have been situated in many different chapters, we felt it was important to recognize the impact these issues have on those within the Social Work profession. We learned that these issues result from institutional practices and that individuals and managers can undertake many different approaches to reduce the impacts. Finding the right strategy and recognizing small gains is key to long-term success in this field.
98
Here are some additional resources you may want to check out!
99
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
100
Baker Collins, S., Smith-Carrier, T., Gazso, A., & Smith, C. (2020). Resisting the culture of poverty narrative: Perspectives of social assistance recipients. Journal of Poverty, 24(1), 72–93. https://doi.org/10.1080/10875549.2019.1678551
Bardwell, G., Kerr, T., Boyd, J., & McNeil, R. (2018). Characterizing peer roles in an overdose crisis: Preferences for peer workers in overdose response programs in emergency shelters. Drug and Alcohol Dependence, 190, 6–8. https://doi.org/10.1016/j.drugalcdep.2018.05.023
Baumann, R. M., Hamilton-Wright, S., Riley, D. L., Brown, K., Hunt, C., Michalak, A., & Matheson, F. I. (2019). Experiences of violence and head injury among women and transgender women sex workers. Sexuality Research & Social Policy, 16(3), 278–288. https://doi.org/10.1007/s13178-018-0334-0
Bourque, J., VanTil, L., Nadeau, J., LeBlanc, S. R., Ebner-Daigle, J., Gibbons, C., & Darte, K. (2017). Physical health status of homeless Veterans in Canada: A cross-sectional study. Journal of Military, Veteran and Family Health, 3(2), 4–11. https://doi.org/10.3138/jmvfh.4251
Burns, V. F., & Sussman, T. (2019). Homeless for the first time in later life: Uncovering more than one pathway. The Gerontologist, 59(2), 251–259. https://doi.org/10.1093/geront/gnx212
Burns, V. F., Sussman, T., & Bourgeois-Guérin, V. (2018). Later-life homelessness as disenfranchised grief. Canadian Journal on Aging, 37(2), 171–184. https://doi.org/10.1017/S0714980818000090
Canham, S. L., Battersby, L., Fang, M. L., Wada, M., Barnes, R., & Sixsmith, A. (2018). Senior services that support housing first in metro Vancouver. Journal of Gerontological Social Work, 61(1), 104–125. https://doi.org/10.1080/01634372.2017.1391919
Cerswell Kielburger, L., Rockman, P., & Baranek, P. (2018). Preventing burnout among service providers. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Charron, C. B., Hudani, A., Kaur, T., Rose, T., Florence, K., Jama, S., & Pakhalé, S. (2018). Assessing community (peer) researcher’s experiences with conducting spirometry and being engaged in the “Participatory research in Ottawa: Management and point-of-care for tobacco-dependence” (PROMPT) project. Research Involvement and Engagement, 4(1), 43–43. https://doi.org/10.1186/s40900-018-0125-z
Cully, L., Wu, Q., & Slesnick, N. (2018). Ecologically based family therapy for adolescents who have left home. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
da Silva Rebelo, M. J., Fernández, M., & Achotegui, J. (2018). Mistrust, anger, and hostility in refugees, asylum seekers, and immigrants: A systematic review. Canadian Psychology, 59(3), 239–251. https://doi.org/10.1037/cap0000131
Durbin, A., Lunsky, Y., Wang, R., Nisenbaum, R., Hwang, S. W., O’Campo, P., & Stergiopoulos, V. (2018). Borderline intellectual functioning and lifetime duration of homelessness among homeless adults with mental illness. Healthcare Policy, 14(2), 40–46. https://doi.org/10.12927/hcpol.2018.25687
Firang, D. (2019). Exploring housing careers among Ghanaians in Toronto, Canada. Housing Studies, 34(5), 868–891. https://doi.org/10.1080/02673037.2018.1489527
Firang, D. (2020). The impact of COVID-19 pandemic on international students in Canada. International Social Work, 63(6), 820–824. https://doi.org/10.1177/0020872820940030
Firestone, M., Syrette, J., Brant, T., Laing, M., & Teekens, S. (2021). Findings from a process evaluation of an Indigenous holistic housing support and mental health case management program in downtown Toronto. International Journal of Indigenous Health, 16(2), 139-150. https://doi.org/10.32799/ijih.v16i2.33173
Fleury, M. J., Grenier, G., Cao, Z., & Meng, X. (2020). Typology of currently or formerly homeless individuals based on their use of health and social services. Community Mental Health Journal. https://doi.org/10.1007/s10597-020-00693-6
Forchuk, C., Richardson, J., Atyeo, H., & Serrato, J. (2021a). Qualitative findings from a housing first evaluation project for homeless veterans in Canada. Journal of Military, Veteran and Family Health. Advance Access Article. https://doi.org/10.3138/jmvfh-2021-0052
Forchuk, C., Russell, G., Richardson, J., Perreault, C., Hassan, H., Lucyk, B., & Gyamfi, S. (2021b). Family matters in Ontario: Understanding and addressing homelessness among newcomer families in Canada. Canadian Journal of Nursing Research. https://doi.org/10.1177/0844562121998206
Gazso, A., Baker Collins, S., Smith-Carrier, T., & Smith, C. (2019). The generationing of social assistance receipt and “welfare dependency” in Ontario, Canada. Social Problems. https://doi.org/10.1093/socpro/spz032
Global Social Service Workforce Alliance Case Management Interest Group. (2018). Core concepts and principles of effective case management: Approaches for the social service workforce. 1st Edition. Global Social Service Workforce Alliance. Core concepts and principles of effective case management
Greer, A., Buxton, J. A., Pauly, B., & Bungay, V. (2021). Organizational support for frontline harm reduction and systems navigation work among workers with living and lived experience: qualitative findings from British Columbia, Canada. Harm Reduction Journal, 18(1), 60. https://doi.org/10.1186/s12954-021-00507-2
Hasford, J., Amponsah, P., & Hylton, T. (2018). (2018). Anti-racist praxis with street-involved African Canadian youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Hopper, E. K., Olivet, J., & Bassuk, E. L. (2018). Trauma-informed care for street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Humphries, J., & Canham, S. L. (2021). Conceptualizing the shelter and housing needs and solutions of homeless older adults. Housing Studies, 36(2), 157–179. https://doi.org/10.1080/02673037.2019.1687854
Hwang, S. W., Wilkins, R., Tjepkema, M., O’Campo, P. J., & Dunn, J. R. (2009). Mortality among residents of shelters, rooming houses, and hotels in Canada: 11 year follow-up study. BMJ, 339. https://doi.org/10.1136/bmj.b4036
Jadidzadeh, A., & Falvo, N. (2019). Patterns of exits from housing in a homelessness system of care: the case of Calgary, Alberta. Housing Studies, 34(1), 66–91. https://doi.org/10.1080/02673037.2018.1432755
Kaltsidis, G., Grenier, G., Cao, Z., & Fleury, M. J. (2020). Change in housing status among homeless and formerly homeless individuals in Quebec, Canada: A profile study. International Journal of Environmental Research and Public Health, 17(17), 6254. https://doi.org/10.3390/ijerph17176254
Kennedy, M. C., Boyd, J., Mayer, S., Collins, A., Kerr, T., & McNeil, R. (2019). Peer worker involvement in low-threshold supervised consumption facilities in the context of an overdose epidemic in Vancouver, Canada. Social Science & Medicine (1982), 225, 60–68. https://doi.org/10.1016/j.socscimed.2019.02.014
Kerman, N., Ecker, J., Gaetz, S., Tiderington, E., & Kidd, S. A. (2021). Mental health and wellness of service providers working with people experiencing homelessness in Canada: A national survey from the second wave of the COVID-19 pandemic. Canadian Journal of Psychiatry. https://doi.org/10.1177/07067437211018782
Kidd, S. A., Vitopoulos, N., Frederick, T., Daley, M., Peters, K., Clarc, K., … McKenzie, K. (2019). Peer support in the homeless youth context: Requirements, design, and outcomes. Child & Adolescent Social Work Journal, 36(6), 641–654. https://doi.org/10.1007/s10560-019-00610-1
Kozloff, N., Bergmans, Y., Snider, C., Langley, J., & Stergiopoulos, V. (2018). Crisis response with street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Malenfant, J. A., Nichols, N., & Schwan, K. (2019). Chasing funding “to eat our own tail”: The invisible emotional work of making social change. Canadian Journal of Nonprofit and Social Economy Research, 10(2). https://doi.org/10.29173/cjnser.2019v10n2a307
Mamdani, Z., McKenzie, S., Pauly, B., Cameron, F., Conway-Brown, J., Edwards, D., Howell, A., Scott, T., Seguin, R., Woodrow, P., & Buxton, J. A. (2021). “Running myself ragged”: stressors faced by peer workers in overdose response settings. Harm Reduction Journal, 18(1), 18. https://doi.org/10.1186/s12954-020-00449-1
Marsella, O., Forchuk, C., & Oudshoorn, A. (2020). Exploring harm reduction among Canadian Veterans experiencing homelessness. Journal of Military, Veteran and Family Health, 6(2), 17–25. https://doi.org/10.3138/jmvfh-2019-0042
Milaney, K., Kamran, H., & Williams, N. (2020). A portrait of late life homelessness in Calgary, Alberta. Canadian Journal on Aging, 39(1), 42–51. https://doi.org/10.1017/S0714980819000229
Milaney, K., Lockerbie, S. L., Fang, X. Y., & Ramage, K. (2019). The role of structural violence in family homelessness. Canadian Journal of Public Health, 110(5), 554–562. https://doi.org/10.17269/s41997-019-00219-y
Nichols, N., & Braimoh, J. (2018). Community safety, housing precariousness and processes of exclusion: An institutional ethnography from the standpoints of youth in an “unsafe” urban neighbourhood. Critical Sociology, 44(1), 157–172. https://doi.org/10.1177/0896920516658941
Oudshoorn, A., Benbow, S., Esses, V., Baker, L., Annor, B., Coplan, I., Shantz, J., & Ezukuse, V. (2020). Homelessness prevention for refugees: Results from an analysis of pathways to shelter. European Journal of Homelessness; 14(2), 189-205. EJH_14-2_WEB.pdf (feantsaresearch.org)
Paradis, E., Wilson, R. M., & Logan, J. (2014). Nowhere else to go: Inadequate housing & risk of homelessness among families in Toronto’s aging rental buildings. Toronto, Ontario: Cities Centre, University of Toronto.
Parkes, T., Matheson, C., Carver, H., Budd, J., Liddell, D., Wallace, J., … Foster, R. (2019). Supporting harm reduction through peer support (SHARPS): Testing the feasibility and acceptability of a peer-delivered, relational intervention for people with problem substance use who are homeless, to improve health outcomes, quality of life and social functioning and reduce: study protocol. Pilot and Feasibility Studies, 5(1), 64–64. https://doi.org/10.1186/s40814-019-0447-0
Paul, S., Corneau, S., Boozary, T., & Stergiopoulos, V. (2018). Coping and resilience among ethnoracial individuals experiencing homelessness and mental illness. International Journal of Social Psychiatry, 64(2), 189–197. https://doi.org/10.1177/0020764017748986
Pauly, B., Mamdani, Z., Mesley, L., McKenzie, S., Cameron, F., Edwards, D., Howell, A., Knott, M., Scott, T., Seguin, R., Greer, A. M., & Buxton, J. A. (2021). “It’s an emotional roller coaster… But sometimes it’s fucking awesome”: Meaning and motivation of work for peers in overdose response environments in British Columbia. The International Journal on Drug Policy, 88, 103015. https://doi.org/10.1016/j.drugpo.2020.103015
Polillo, A., Sylvestre, J., Kerman, N., Lee, C. M., Aubry, T., & Czechowski, K. (2018). The experiences of adolescents and young adults residing with their families in emergency shelters in Canada. Journal of Children & Poverty, 24(2), 89–107. https://doi.org/10.1080/10796126.2018.1470438
Pottie, K., Kendall, C. E., Aubry, T., Magwood, O., Andermann, A., Salvalaggio, G., … Hwang, S. W., Stergiopoulos, V., & Tugwell, P. (2020). Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience. Canadian Medical Association Journal (CMAJ), 192(10), E240–E254. https://doi.org/10.1503/cmaj.190777
Ratnam, C., Fitzpatrick, A., & Thang, H. (2018). Engaging with newcomer youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Reid, N., Kron, A., Lamanna, D., Wen, S., Durbin, A., Rajakulendran, T., … Stergiopoulos, V. (2021). Building bridges to housing for homeless adults with intellectual and developmental disabilities: Outcomes of a cross‐sector intervention. Journal of Applied Research in Intellectual Disabilities, 34(1), 16–27. https://doi.org/10.1111/jar.12779
Roy, S., Svoboda, T., Issacs, B., Budin, R., Sidhu, A., Biss, R. K., … Connelly, J. (2020). Examining the cognitive and mental health related disability rates among the homeless: Policy implications of changing the definition of disability in Ontario. Canadian Psychology = Psychologie Canadienne, 61(2), 118–126. https://doi.org/10.1037/cap0000211
Sandu, R. D., Anyan, F., & Stergiopoulos, V. (2021). Housing first, connection second: the impact of professional helping relationships on the trajectories of housing stability for people facing severe and multiple disadvantage. BMC Public Health, 21(1), 249–249. https://doi.org/10.1186/s12889-021-10281-2
St. Arnault, D., & Merali, N. (2019a). Pathways for refugees’ descent into homelessness in Edmonton, Alberta: The urgent need for policy and procedural change. Journal of International Migration and Integration, 20(4), 1161–1179. https://doi.org/10.1007/s12134-019-00652-5
St. Arnault, D., & Merali, N. (2019b). Refugee pathways out of homelessness in urban Alberta, Canada: implications for social justice-oriented counselling. Counselling Psychology Quarterly, 32(2), 227–245. https://doi.org/10.1080/09515070.2018.1437540
Sylvestre, J., Kerman, N., Polillo, A., Lee, C. M., & Aubry, T. (2017). A profile of families in the emergency family homeless shelter system in Ottawa, Ontario, Canada. Canadian Journal of Urban Research, 26(1), 40–51. Canadian Journal of Urban Research
Sylvestre, J., Kerman, N., Polillo, A., Lee, C. M., Aubry, T., & Czechowski, K. (2018). A Qualitative study of the pathways into and impacts of family homelessness. Journal of Family Issues, 39(8), 2265–2285. https://doi.org/10.1177/0192513X17746709
Waegemakers Schiff, J. (2015). Working with homeless and vulnerable people: Basic skills and practices. UK: Oxford University Press.
Waegemakers Schiff, J., & Lane, A. M. (2019). PTSD symptoms, vicarious traumatization, and burnout in front line workers in the homeless sector. Community Mental Health Journal, 55(3), 454–462. https://doi.org/10.1007/s10597-018-00364-7
Wang, J. Z., Mott, S., Magwood, O., Mathew, C., Mclellan, A., Kpade, V., … Andermann, A. (2019). The impact of interventions for youth experiencing homelessness on housing, mental health, substance use, and family cohesion: a systematic review. BMC Public Health, 19(1), 1528–1528. https://doi.org/10.1186/s12889-019-7856-0
X
Health Sciences encompasses many different medical fields. Within this part of the book, we focus on how two of these fields can be framed within a social determinants of health lens, through chapters on Primary Care and Nursing, and Emergency Medicine. As you work through these chapters, you are encouraged to think about the fields of health and medicine as fundamentally being about ensuring human rights through health care equity. You are also encouraged to consider how health care and medical professionals can serve as points-of-contact for a population who may otherwise be difficult to reach.
Perhaps as you read this, you are considering undertaking a career in the Health Sciences, such as a Primary Care Physician, Emergency Nurse, or Emergency Physician. The chapters in this section are designed to help you think critically about some of the questions you may encounter in these fields of employment. Understanding homelessness will help you navigate situations and choices you have to make. Consider, for example, a scenario in which a man seeks medical care at a walk-in clinic for falling off a ladder at work. He admits to being intoxicated at the time and says he has lost both his employment and his housing as a result. He is seeking medication to treat the pain. As a Primary Care Physician, the choice you make will have implications for this man’s health and well-being. The choice not to treat him may result in an Emergency Room visit and potential hospitalization. If you are working in the Emergency Room, you will need to make the same choice. How do you provide this man the best possible care, without being influenced by potential bias?
Before you begin, pause to consider how you would respond in each of the roles of the scenario above. With the knowledge you currently have about homelessness in Canada, why do you think people who experience homelessness tend to have poor health? What could be done to improve their access to health care? In the scenario above, what is the best-case outcome and the worst-case outcome for the man who is seeking care?
You are encouraged to keep this scenario in your mind as you read through the next two chapters and ask yourself whether any of your responses change, or are reaffirmed, after learning more about what Health Sciences can teach us about homelessness in Canada.
X
Health and housing security are positively correlated variables. This consistent research outcome tells us the simple fact that people who have stable housing tend to be in better health than those who do not. The flipside of this is also true. As housing security decreases – as a person becomes at risk of losing their housing or becomes homeless – their health gets worse. When people experience homelessness, they tend to also experience a range of chronic conditions that go along with it. These include diabetes, chronic lung issues such as COPD and emphysema, fatigue, skin conditions, dental problems, and foot problems.
Yet, despite having generally poorer health than housed individuals, people who experience homelessness also are more likely to report they do not have a primary care provider, such as a Family Physician or Nurse Practitioner. Accessing mainstream healthcare in this way often requires that a person have a valid health card, address where they can receive mailings, and a phone number where they can be contacted to book appointments and follow-ups. These requirements are not always conducive to the realities of being homeless, andnot havingan address, phone, or proper documentation. Canada has a highly regarded health care system, but it does not work as well as it could (and should) for our most vulnerable citizens.
101
In this chapter, you are invited to learn more about the health and primary health care needs of people experiencing homelessness in Canada. While thinking critically to uncover the strengths and gaps in our health care response for persons experiencing homelessness, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that homelessness is both a contributor to poor health, as well as a consequence of it. Despite having a universal health care system in Canada, not every citizen benefits in the same way. Read on to learn more about the primary health care needs of people experiencing homelessness in Canada and what can be done to improve health care outcomes for individuals without equitable access.
102
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to Primary Care and Nursing. As you work through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After considering the real-world scenario, we will endeavour to answer each question posed in the learning objectives. Do people experiencing homelessness have equitable access to primary care? What specialized primary care would people who experience homelessness benefit from? Are there special end-of-life considerations for someone experiencing homelessness? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
103
As you learn about the complex relationship between primary health care and homelessness, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider this person’s experience.
Tom
Tom is a 75-year-old retired electrician who is currently living in a local shelter. His wife of 45 years died 3 years ago , and with her death, the pension that was sustaining the household ended. Tom was unable to meet his expenses. As a small business owner for 45 years, he had no pension of his own. He was able to live on the proceeds of the sale of his home for a couple of years; however, his wife had managed their money for their entire marriage and without money management skills Tom’s money ran out. He had been living on the streets until recently. Tom presents at the local Community Health Centre with significant weight loss, lack of appetite, weakness, and memory loss. He reports that he has a persistent cough even though he gave up smoking 2 years ago. He has not seen his own Family Physician, who is in a city 30 km away, in two years. His immediate family members, two sons, live in a different province. His former neighbours have tried to keep in contact with him, however Tom has been reclusive. Staff in the shelter have noted that he has periods of confusion in the evenings and that his sleep is significantly disrupted. The Nurse Practitioner (NP) assessing Tom has no health records to draw upon and he questions Tom’s ability to share an accurate health history.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to the scenario again at the end of the chapter.
Reflection Questions
104
In the chapter on Public Health, we asked you to consider the challenges that go along with experiencing homelessness during a pandemic outbreak. We saw that people were often living in congregate settings, like emergency shelters, without reliable access to healthy food, fresh water, and hygiene facilities. These factors created conditions that led people experiencing homelessness to be particularly vulnerable in these emergency times. For instance, during the COVID-19 outbreak people experiencing homelessness were over 20 times more likely to be admitted to hospital for COVID-19, over 10 times more likely to require intensive care, and over 5 times more likely to die within 21 days of their first positive test result (Richard et al., 2021).
There is a well-recognized truth that vulnerability during a pandemic is often rooted in vulnerability that pre-existed before the pandemic. This tells us that people who experience homelessness were at high risk during COVID-19 because they already had complex underlying issues. Before you begin this section, we encourage you to pause and reflect on the question of whether people experiencing homelessness have equitable access to primary care, and if you believe they do not (as we have not so subtly hinted at) why do you think their access might be inequitable?
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1360#h5p-91
When you think about primary care, such as Family Physicians and Nurse Practitioner led clinics, what might come to mind is our universal health care system. There is often a misconception that because we have “free health care” in Canada, that everyone has the same access to it. However, there is a long history of research that shows people who experience homelessness often have very poor health (Chiu, Redelmeier, Tolomiczenko, Kiss, & Hwang, 2009; Daiski, 2007; Frankish, Hwang, & Quants, 2005; Guirguis-Younger, McNeil, & Hwang, 2014; Hwang, 2001; Jaworsky et al., 2016; Khandor et al., 2011; Kelly & Caputo, 2007).
What we see when we look at these health outcomes is a pattern. If most people who experience homelessness are in poor health, there must be some common factor that explains why. The explanation cannot be found exclusively in biomedical factors, such as genes and predisposition to certain health conditions. These no doubt play a role in poor health, but they do not provide a full account of why there is a connection between people experiencing homelessness and having multiple chronic health conditions. In order to do this – to understand the reasons why we see this relationship emerge – we have to consider the social determinants of health. This concept should be familiar to you from previous chapters, as it is an underlying foundational concept for understanding homelessness. Before we move through the remainder of the section, we invite you to watch this video that expands upon the social determinants of health and situates them within a Canadian context.
The social determinants of health help provide a more nuanced picture of human health, beyond individual level factors. We can see their importance when we think about why people who experience homelessness are often in poor health compared to the housed population. Dr. Stephen Hwang, who has studied the relationship between health and homelessness extensively, explains that there are many barriers to accessing care that exist. Liu and Hwang (2021) have argued that the upstream causes of poor health for people experiencing homelessness include extreme poverty, harsh living environments, trauma, and structural barriers to care, while the downstream causes include infectious diseases, heart disease, substance use disorders, and suicide. You can see a graphic depiction of these barriers in Fig. 1: Interventions to improve health outcomes among homeless people. In the video that follows, Dr. Hwang explains these barriers further.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, Dr. Stephen Hwang argues that by any means that we can define the term equity, people who experience homelessness do not have equitable access to primary health care. He notes that there are several barriers that exist, such as competing obligations and needs, a lack of transportation, not having a phone or computer to communicate, and having previous negative encounters that lead to health care avoidance. Dr. Hwang notes that the health care system is set up to incentivize practitioners to care for people who are well and well-off, who require only brief visits, and who have less complex health needs than those who are more disadvantaged. This video is 3:28 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Do people experiencing homelessness have equitable access to primary care?
There are many obstacles that people who experience homeless face in accessing primary care. Research from the Niagara region of Ontario found that some of the commonly identified barriers include challenges finding a primary care provider, lack of affordability, poor therapeutic relationships, systemic issues, and transportation / accessibility issues (Ramsay, Hossain, Moore, Milo, & Brown, 2019). Stigma and discrimination are particularly prevalent issues that people who experience homelessness face in health care encounters, particularly if they use drugs and/or have mental illness (Paradis-Gagné, Pariseau-Legault, Villemure, & Chauvette, 2020).
Our own research using narrative interviews with 53 people experiencing homelessness or housing vulnerability in a small Ontario town showed that only 28% had a primary care provider locally, an additional 40% had a provider in another town, and 32% had no access to a primary care provider at all (Gilmer & Buccieri, 2020). This research also indicated that participants frequently sought out care in emergency departments because they were unable to access the primary care they needed in the community. When trying to get primary or emergency medical care, the participants largely felt they were discriminated against and treated poorly because they had, or were perceived to have, mental illness, chronic pain, and/or addiction issues (Gilmer & Buccieri, 2020). These findings are supported by Magwood et al., (2020) who have also found that health care practitioners may be reluctant to care for patients with lived experience of homelessness, indicated stigma and bias are barriers that lead to inequitable primary health care access.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1360#h5p-92
We would like to invite you to learn more about our research in this featured reading published in the Journal of Primary Care & Community Health. Here we examine the relationship between primary care access and homelessness in a small town.
Gilmer, C., & Buccieri, K. (2020). Homeless patients associate clinician bias with suboptimal care for mental illness, addictions, and chronic pain. Journal of Primary Care & Community Health, 11.
Stigma and discriminatory treatment are often linked to chronic pain, as people who seek treatment in primary care settings may be viewed as engaging in drug-seeking behaviour. This has the effect of decreasing their access to medical treatments and results in multiple visits or fractured health care, as they try to find a health care provider who can help. For instance, researchers in Calgary examined primary care clinic records and found that patients who were experiencing homelessness visited at a rate 2.02 times higher than those who were housed (Rivera et al., 2018). These findings may indicate that these patients had higher health care needs, and also that their needs were not being fully met when they visited their primary care provider.
In a study of 1,287 people with mental illness involved in a Housing First program in three Canadian cities, researchers found that 43% reported moderate to severe chronic pain that interfered with daily activities (80%), sleep (78%), and social interactions (61%) (Vogel et al., 2017). Chronic pain was associated with increasing age, major depressive disorder, mood disorder with psychotic features, panic disorder, post-traumatic stress disorder, and increased suicidality (Vogel et al., 2017). Among participants who reported experiencing chronic pain, 64% had sought medical treatment, 56% were treated with prescription drugs, and 38% used illicit drugs as a form of pain relief (Vogel et al., 2017). When people are not able to receive health care that meets their needs, they may seek out alternative measures. In the next video, Dr. Abe Oudshoorn identifies and discusses three challenges he has observed with primary care for patients experiencing homelessness.
In this video, Dr. Abe Oudshoorn shares his passion for equitable health care access and argues that the challenges with primary care for people experiencing homelessness are system-wide and multifactorial. First, he notes, people may become disconnected from their primary care provider due to conflict over care or due to their own relocation. Second, they may face discrimination from care providers that can be a barrier to seeking out future health care supports. Finally, when people who experience homelessness lack a foundation of primary care they may receive episodic care, such as at community health centres or emergency shelters, which lacks the continuity needed for ongoing treatments and medication monitoring. Dr. Oudshoorn concludes that what is needed is to reconnect people experiencing homelessness with a stable foundation of primary care. This video is 3:29 in length and has closed captions available in English.
Key Takeaways – Dr. Abe Oudshoorn: Do people experiencing homelessness have equitable access to primary health care?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1360#h5p-93
When we asked the researchers whether people experiencing homelessness have equitable access to primary care, they all said no. There are many barriers to primary care that exist, as we have seen. People may have difficulty finding a primary care provider, staying connected after moving around or losing housing, and may face discrimination when seeking treatment and medication for conditions such as chronic pain, mental illness, and/or addiction. There are also many barriers to primary care that result from institutional biases within our health care system. In the two videos that follow Dr. Rebecca Schiff and Dr. Alex Abramovich speak about racism, homophobia, and transphobia as barriers in our health care system that prevent equitable access for many people experiencing homelessness.
In this video, Dr. Rebecca Schiff argues that people who experience homelessness are one group, like those living in rural and remote communities, who lack equitable access to primary health care. She notes that we must consider intersectionality, such as discrimination in our health care system related to being Indigenous, visibly homeless, and/or a substance user. Dr. Schiff notes that in addition to having poor access to primary care, people who experience homelessness may also have a range of factors that make it more challenging for them to advocate for themselves. This video is 2:18 in length and has closed captions available in English.
Key Takeaways – Dr. Rebecca Schiff: Do people experiencing homelessness have equitable access to primary health care?
In this video, Dr. Alex Abramovich explains that LGBTQ2S+ individuals, particularly those experiencing homelessness, do not have equitable access to primary health care. He notes that many of our health services are not population-specific, nor prepared to appropriately respond to the health care needs of these patients. Within mainstream primary care, LGBTQ2S+ patients may feel unsafe and not know how their physician will respond to them. Dr. Abramovich argues that few specialized clinics exist and those that do often have long waitlists, which is particularly problematic and increases risk of suicidality for trans-identified individuals seeking support for medical transitions. Dr. Abramovich concludes a lot more work needs to be done to improve access to appropriate and timely health care for LGBTQ2S+ persons, including those experiencing homelessness. This video is 3:40 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Do people experiencing homelessness have equitable access to primary health care?
In a review of administrative health data for 2,085 transgender individuals in Ontario, Dr. Abramovich and his team (2020) found that these patients are more likely than cisgender patients to live in lower-income areas, experience chronic health conditions such as asthma, diabetes, chronic obstructive pulmonary disease, and HIV. How do you think experiencing homelessness might make it even more difficult for transgender individuals to get the health care they need? What measures could we take to improve this population’s access to primary health care?
We have considered a number of barriers that people experiencing homelessness face in accessing primary care. In response to these barriers, researchers and care providers have also sought out ways to increase accessibility. For instance, Ramsay et al., (2019) found that health care access can be enhanced for this population through community health care outreach, implementing measures to foster positive relationships, and engaging shelters in coordinating health care. As we have seen, traditional health care settings may not be welcoming spaces for people experiencing homelessness. In the next set of videos, Dr. Tim Aubry and Dr. Kelli Stajduhar discuss how communities are using mobile outreach teams as a way to increase access to primary care.
In this video, Dr. Tim Aubry explains that people who experience homelessness often do not have a family doctor and consequently lack equitable access to primary care. He notes that as a response to this, many cities have developed teams of health care practitioners who offer outreach in shelters, service agencies, and on the street. Dr. Aubry notes that shelters have evolved into health, mental health, and addictions service hubs and while this fills a need, it is also problematic as it goes against the Housing First philosophy of integrating people into the broader community. This video is 3:15 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: Do people experiencing homelessness have equitable access to primary care?
In this video, Dr. Kelli Stajduhar explains that people who experience homelessness may be able to access primary care through practitioners or walk-in clinics, but that these environments often do not feel safe for people who have experienced trauma, violence, discrimination, and who may use substances. Likewise, in the absence of primary care, seeking support in an emergency room may also feel unsafe. Dr. Stajduhar argues that people who experience homelessness are cared for everywhere in our health care system, so it is important all health care practitioners understand key aspects such as harm reduction, trauma and violence informed care, the social determinants of health, and cultural humility and safety. She concludes by discussing the work of mobile primary palliative outreach teams in cities across Canada, who work on providing upstream care to people in a way that is low barrier and meets them where they are at. This video is 5:37 in length and has closed captions available in English.
Key Takeaways – Dr. Kelli Stajduhar: Do people experiencing homelessness have equitable access to primary care?
In this video, Dr. Stajduhar makes the important point that all health care providers need to be aware of how to care for patients experiencing homelessness in a way that is respectful and accounts for the barriers they face. The research supports her position. In a critical ethnography with 12 outreach Nurses who work with people experiencing homelessness, researchers found that there is a need to raise awareness among health care providers about the ethical, clinical, and organization issues of these patients particularly in relation to the ways in which they are stigmatized and excluded from health care settings (Paradis-Gagné, Pariseau-Legault, Villemure, & Chauvette, 2020).
As an alternative to more traditional clinic-based care, mobile outreach allows health practitioners to meet people where they are. In an article that provides a critical history of outreach nursing in Canada, Hardill (2007) notes that street nursing, or nursing outreach to people experiencing visible homelessness, has become an established specialty in Canada, as in America, Great Britain, Europe, and Australia with roots tracing as far as the early 1700s when the Grey Nuns made visits to those who were ill and poor in what is now known as Quebec. In her memoir, “A knapsack full of dreams” respected Toronto Street Nurse Cathy Crowe (2019) writes about the career trajectory that led her to street nursing, and shares frustration over larger structural issues, like the lack of affordable housing, that contribute to poor health outcomes for the people she treats. In this video, Her Nurse Hands, she speaks firsthand about her career as a Street Nurse in Toronto.
Mobile outreach is a critically important approach for reaching people who are experiencing unsheltered homelessness and are disconnected from social services and health care agencies. Sometimes health care is provided directly in shelters or drop-in centres that support people experiencing homelessness. What do you think some of the benefits and drawbacks are of having health care services located in homelessness agencies? Dr. Naomi Thulien and Dr. Tim Aubry speak about this issue in the next two videos.
In this video, Dr. Naomi Thulien argues that the reasons people who experience homelessness do not have equitable access to health care are complex. She notes that finding a primary care physician is difficult for everyone, but that those who experience homelessness also tend to have urgent health care needs that require same day emergency care. She cites health care clinics located within homeless sector agencies as being a source of health care, but also notes that as people move into housing, they often no longer want to access care in these locations. This video is 1:24 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: Do people experiencing homelessness have equitable access to primary health care?
In this video, Dr. Tim Aubry explains that having health care services located in shelters can be problematic in the long run because it sets up a parallel system of health care. Instead, he argues, we should take a Housing First approach that moves away from a treatment-first perspective and focuses on housing people before addressing health, mental health, and/or addictions issues they may be experiencing. This video is 2:32 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: Housing stability as long-term health care
Dr. Thulien and Dr. Aubry both recognize the urgent health care needs of many people who experience homelessness but also caution that having health care directly in shelters may not be what people want after they are housed. In the chapter on Policy, Politics, and Housing in Canada we looked at Housing First, the idea that people are housed before needing to demonstrate they have met ‘housing-readiness’ requirements. Researchers have studied Housing First to see whether it helps people obtain and stay connected to primary health care after being housed. Unfortunately, this does not seem to be the case. Whisler et al., (2021) found that there was no significant improvement in primary care retention for Housing First participants compared to people not receiving the housing intervention. These findings suggest that while housing is a critically important social determinant of health, it is not enough just to get people housed. More targeted interventions are needed to actively help those who want health care to be able to access it without barriers.
Our current primary health care system is not accessible to many people who experience homelessness. We have seen that mobile outreach and shelter-based health care are approaches used to reach people experiencing unsheltered or emergency sheltered homelessness. However, while important strategies, these approaches do not solve the underlying issue that mainstream health care is discriminatory and inaccessible to a large number of people who have complex health problems. Does the solution then lie in creating a separate system, or does it mean we should improve the system we have to make it more equitable? Dr. Bernie Pauly and Dr. Abe Oudshoorn share their views in the next two videos.
In this video Dr. Bernadette [Bernie] Pauly explains that if we want to build a better response to homelessness, we need to develop a system that is accessible and streamlined, where people do not have to go to multiple places, fill out multiple forms, and tell their story multiple times. She notes that many people who experience homelessness do not have a primary care practitioner. While she identifies community health centres as being helpful for promoting equity, she is also clear to note that they are often not integrated into the larger primary care system and are not available in every community. Dr. Pauly cites multiple inequities people experiencing homelessness face when navigating primary care, such as a lack of transportation, competing care responsibilities, hours that are not in line with their availability, and stigmatization. She concludes that while primary care practitioners may recognize the roots causes of poor physical and mental health as being a lack of housing, food, and income, they are not well-equipped to address the social determinants of health. This video is 5:42 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: Do people experiencing homelessness have equitable access to primary care?
In this video, Dr. Abe Oudshoorn argues that it is not advisable to create an alternative system of health services attached to people’s housing status, but rather that we should ensure people experiencing homelessness receive quality care by making improvements to our current health care system. He notes there are several steps we can take to fix our primary care system, including legislation that prevents primary care practices from firing patients, attaching better funding and supports such as integrating social workers into care teams, and coordinating care across teams for patients who relocate. Dr. Oudshoorn concludes that there is a perception that because Canada’s health care system is public people have equal access, but that the health outcomes demonstrate this to be untrue. Poor health outcomes are not individual failures but rather the predictable result of a system that is not designed to be flexible to meet people’s diverse needs. This video is 4:14 in length and has closed captions available in English.
Key Takeaways – Dr. Abe Oudshoorn: The need to enhance Canada’s existing health care system
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1360#h5p-94
When people experience homelessness they often have many competing priorities, such as finding shelter and food, that take precedence over seeking health care. For that reason, it is essential that health care workers understand the challenges these individuals face and advocate for them to get the care they need. For instance, there have been calls from practitioners and people with lived experience for improved training to increase knowledge of patient needs and preferences (Magwood et al., 2020), which can begin during their educational training even before they enter the field (Hossain, Ramsay, Moore, & Milo, 2018).
Family Physicians, for instance, have the opportunity to be powerful vocal advocates for people experiencing homelessness within their local communities, and they can provide direct care while championing policy changes that address the underlying structural causes that lead to poor health (Andermann et al., 2020). Likewise, by virtue of the work they do, Nurses are in a unique position to advocate for patients that others might stigmatize or discriminate against (Crowe & Baker, 2007).
A statement from the Registered Nurses’ Association of Ontario (2004) indicates, “Nurses must be aware of homelessness and basic housing needs in each facet of their practice. This should include all three dimensions of housing which include: house (physical structure), home (social and psychological characteristics) and neighbourhood (physical location and available services). Part of this process will require education and a reflective review of our own beliefs and practices surrounding homelessness. Nurses also have a responsibility to educate the public and advocate on behalf of homeless individuals – for health.” In the next video, Dr. Kelli Stajduhar discusses the responsibility Nurses have to advocate for their patients, even when it feels uncomfortable to do so.
In this video, Dr. Kelli Stajduhar explains that people who experience homelessness are often discriminated against and stereotyped, and Nurses need to push back against situations where their colleagues are being judgemental or making assumptions. She argues that Nurses are positioned in places where they can engage in advocacy and that, while there may be different levels of comfort, instructors can help prepare nursing students by providing them with the capacity and confidence to do so. This video is 2:46 in length and has closed captions available in English.
Key Takeaways – Dr. Kelli Stajduhar: Nursing as a form of advocacy
In this section, we asked you to consider whether people who experience homelessness have equitable access to primary health care. The answer we received from every researcher we asked was a loud and resounding ‘no!’ We noted that people who experience homelessness often have a range of complex chronic health conditions, which is not a coincidence but rather the result of social determinants. The reasons people are often in poor health include a lack of housing, employment, social support, and proper nutrition. These factors are made worse by a lack of accessible primary health care.
We have seen in this section that there are many barriers to care, and that these include institutional racism, homophobia, and transphobia within our health care systems. Mainstream primary care clinics are often inaccessible and discriminatory spaces for people experiencing homelessness, particularly if they have chronic pain, mental illness and/or addictions. As an alternative, mobile outreach teams have been formed in many communities to offer basic health care measures to people on the streets. Some homelessness services, such as emergency shelters, also offer onsite health care which is a valuable, but short-term, solution. We have heard that rather than setting up parallel health care systems, we need to focus on improving our current primary care response so that it is accessible to everyone. One key way to do this is for Family Physicians and Nurses to be champions for their patients’ needs within their own practices and through broader policy reform.
Click the link below to listen to all of the researchers answer the question “Do people experiencing homelessness have equitable access to primary care?” in audio format on our podcast!
105
One of the main takeaway messages from the previous section is that people who experience homelessness generally lack access to primary care, for a range of reasons, despite often having complicated chronic health conditions. Based on what you have learned so far, we would like to challenge you to put yourself in the position of a health care provider who is treating a patient experiencing homelessness. What specialized primary care do you think your patient might benefit from? We encourage you here to consider not only physiological care, but social care as well. What could you do to provide this patient with the best care possible so that their needs are met and so that they feel heard and respected?
Use the space below to record your thoughts on how you might approach a care plan for a patient experiencing homelessness who presented to you in a primary care setting. You may record as few or as many ideas as you wish in thinking about how to provide specialized primary care to a patient experiencing homelessness.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=772#h5p-95
Consider this conundrum: Homelessness creates health problems and then serves as a barrier to receiving adequate and timely health care treatment for them. This is evident from the research. For instance, many people who experience homelessness walk around during the day in ill-fitting shoes without being able to take them off or change their socks. Researchers who used a screening tool to assess foot conditions in a sample of 65 adults experiencing homelessness in British Columbia found that the rates of foot conditions were so high that foot assessments should be implemented as part of standard care for this population, to avoid health complications, hospitalization, limb removal, and disabilities (D’Souza, Mirza, & Karkada, 2021).
People experiencing homelessness have also been found to have high rates of hearing impairment compared to the general Canadian population, which might occur because people are unaware that benefits cover the cost of hearing tests (Noel et al., 2020). Research from Toronto with 132 people experiencing homelessness also showed there were substantial otolaryngology needs, pertaining to abnormal findings on head and neck examinations, such as nasal fracture and/or nasal obstruction (Wu et al., 2020). Shelter-based assessments in Toronto found that among 143 randomly selected individuals, ophthalmological disease burden was high, particularly related to low income and low educational attainment, and that this population is not receiving adequate tailored vision care (Jiang et al., 2020). The majority of vision care problems in Canada can be corrected with prescription glasses, indicating that a high rate of visual impairment among this population points toward barriers in access to care (Asare, Wong, Maurer, & Nishimura, 2019).
Researchers in Toronto looked at the relationship between dental problems and chronic health problems in a sample of 575 adults who were experiencing homelessness, had mental illness, and were part of the At Home / Chez Soi Housing First evaluation in Toronto (Mejia-Lancheros et al., 2020a). They found that among their sample, 43% had dental problems, which were positively associated with also having heart disease, diabetes, chronic bronchitis, stomach or intestinal ulcer, inflammatory bowel disease, migraine, arthritis, kidney / bladder problems, and iron-deficiency anemia (Mejia-Lancheros et al., 2020a). The more chronic health problems a person reported, the more likely they were to have dental problems, indicating that there is a relation between dental health and overall health, and that dental care should be better integrated into social and health care programs for this population (Mejia-Lancheros et al., 2020a). A model pathway to oral health care for people experiencing homelessness needs to incorporate government-sponsored oral health programs, support tailored to homelessness, oral health outreach initiatives, and professional education for care providers (Mago, Brondani, MacEntee, & Frankish, 2018).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=772#h5p-96
The research on health conditions and barriers for people experiencing homelessness is extensive. For instance, people who experience homelessness, particularly if using drugs and/or have severe mental illness, are at disproportionate risk of acquiring Hepatitis C virus (Nikoo et al., 2019), yet a scoping review of the literature indicated there is very limited research on how these individuals feel about testing and treatment (Palayew et al., 2018). Cardiovascular disease affects people experiencing homelessness at rates that exceed housed individuals and is a major cause of death among this population, but managing the condition is challenged by barriers to medication adherence, communication, and timely follow-up (Baggett, Liauw, & Hwang, 2018). In Saskatoon researchers looked at enhancing access to physical therapy services for people who were experiencing poverty and homelessness and found that they faced diverse barriers related to transportation, cost, wait times, and geographic location but that enhancing access by providing physical therapy services in a primary health care community-based setting had positive impacts on the study participants’ overall health, functioning, and wellness (Oosman, Weber, Ogunson, & Bath, 2019).
Living in Canada, the risk of hypothermia is a real concern for people who are experiencing homelessness, particularly if spending extended lengths of time outside. In a Toronto based study, researchers found 79 injuries and 18 deaths with hypothermic events between 2004 and 2015, amongst people experiencing homelessness (Zhang et al., 2019). This study further indicated that the odds of a hypothermic event increased with every 5 degree Celsius decrease in the minimum daily temperature and with every 1 mm increase in precipitation (Zhang et al., 2019). While we often see temporary emergency shelters open when there is an extreme cold advisory, this study actually demonstrated that most cases occurred during periods of low to moderate cold, with 72% occurring when the minimum daily temperatures were above -15 degrees Celsius (Zhang et al., 2019). These findings suggest that special considerations are needed to help prevent hypothermia in cold weather, particularly in the periods where the temperature has dropped below freezing but has not reached a cold enough level to trigger the opening of warming centres.
For people who are securely housed, the weather might pose nothing more than an annoyance. It might be a snowy day that requires clearing the driveway or a rainy day that requires using an umbrella to get to work. When we think about homelessness, the weather takes on another level of urgency. People may freeze to death in the winter and get sunburned or heatstroke in the summer. Opening warming and cooling centres offer only temporary relief. What are some longer-term solutions we could implement to protect people from living and sleeping outside? Can you see the direct connection weather highlights between the need for housing and improving people’s health?
Clearly, there are many varied specialized primary care needs for people experiencing homelessness. We can see from this body of research that homelessness can lead to chronic health conditions, like dental disease, foot problems, head and neck problems, vision problems, and hypothermia among many others. Homelessness then also creates the barriers to treatment, such as by making it difficult to get transportation to appointments, have ongoing communication with primary care providers, take medication at scheduled times, and adhere to complex medical treatment plans. A significant amount of this published research comes from Dr. Stephen Hwang and his associates. We asked him, as a medical Doctor who works with patients experiencing homelessness, about specialized primary care. He explained that the clinical treatment of these conditions does not change with homelessness, but that relational practice does. Listen in as he discusses this in the next video.
In this video, Dr. Stephen Hwang explains that people often ask him whether there is something special about the treatment of health conditions for patients experiencing homelessness. He notes that while there are factors that might complicate treatment or add additional considerations, the basic treatment principles remain the same. Dr. Hwang argues that clinicians need to work with their unhoused patients to identify potential barriers to managing their illness and collaboratively find solutions. He further notes that clinicians should realize it is not necessarily the technical aspects of care that are different, but rather the relationship with the patient that requires the most attention. Dr. Hwang concludes that medical training focuses more on learning the treatments for conditions but should also include aspects of relational care, such as building trust and considering how patients feel in these interactions. This video is 2:29 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Relationship-building in medicine with patients experiencing homelessness
The best-practice approach to providing primary care to patients experiencing homelessness or housing vulnerability differs from mainstream clinical practice. As Dr. Hwang has noted, the treatment of the conditions themselves may be the same but the barriers the patient experiences require a tailored approach. To help health care providers, a team of researchers, practitioners, and people with lived experience have developed a document entitled, “Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience.” We invite you to pause here and read the guideline and then listen to the Canadian Medical Association Journalpodcast, in which some of the team members discuss this important document.
Pottie, K., Kendall, C. E., Aubry, T., Magwood, O., Andermann, A., Salvalaggio, G., Hwang, S. W., Stergiopoulos, V., & Tugwell, P. (2020). Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience. Canadian Medical Association Journal (CMAJ), 192(10), E240–E254.
In the featured reading Pottie et al., (2020) provide clinical guidelines for people who have past or present experiences of homelessness or housing vulnerability. They note that clinical assessment for these patients must take into consideration the person’s gender, age, Indigenous heritage, ethnicity, and history of trauma. They apply a social determinants of health lens, and argue that permanent supportive housing and income assistance are needed for patient wellness. They also indicate in their guidelines that case management interventions, that include mental health and/or addictions supports are recommended as an initial step to support primary care. When asked about implementing the guidelines 86 stakeholders, including 16 with lived experience of homelessness, rated the drafted recommendations in a favourable way (Magood et al., 2020).
The clinical guidelines are an important document for helping us think about how to provide equitable primary care to people experiencing homelessness in a way that is tailored to their needs. For instance, we have seen that traditional health care settings may be exclusionary to people who identify as LGBTQ2S+. Health care providers can provide meaningful care to transgender individuals, who experience high rates of violence, discrimination, and homelessness, if they recognize that addressing homelessness and the social determinants of health requires long-term engagement and interdisciplinary team support (Abramovich, Lam, & Chowdhury, 2020). In the video that follows lead author of this study, Dr. Alex Abramovich, discusses this research.
In this video, Dr. Alex Abramovich explains that trans individuals are medically underserved, and experience poor mental health outcomes and high rates of disease burden compared to cisgender individuals. He notes that trans people often face violence and discrimination, leading to higher rates of suicidality, substance use, depression, and anxiety, with limited support available. Dr. Abramovich argues primary care needs to focus more on providing specialized health clinics for LGBTQ2S+ persons, as it is important to have a doctor who understands your needs and to whom you do not have to explain your identity. Dr. Abramovich concludes that further education and training about LGBTQ2S+ health is needed for people working in health care settings. Rather than relying on patients to provide this information, practitioners should seek out opportunities to learn more within their community and through online resources. This video is 4:51 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Improving access to, and education about, health care for trans patients
Want to learn more about LGBTQ2S+ health care?
Check out these helpful online resources as a starting point.
Primary care for people experiencing homelessness needs to account for the range of challenges and barriers these patients commonly experience. For instance, while workplace injuries may occur for housed individuals, the nature of the work may be different for people experiencing homelessness. In a study of cisgender and transgender women involved in the sex trade, 90% reported at least one lifetime traumatic brain injury and all reported one or more head injuries related to violence in sex work (Baumann et el., 2019). Participants in this study spoke about the stigma and discrimination they felt in health care settings, which served as a barrier that could be improved with enhanced training in anti-oppressive care practices (Baumann et al., 2019).
Traumatic brain injury is a common occurrence for people who experience homelessness, often rooted in their childhood. Song et al., (2018) examined the relationship between childhood trauma and traumatic brain injury amongst a sample of 487 individuals experiencing homelessness in British Columbia. They found 64% had traumatic brain injury and 88% reported childhood trauma including physical abuse (58%), physical neglect (63%), sexual abuse (46%), emotional abuse (62%), and emotional neglect (55%). Their analysis of how these variables are inter-related found that experiences of trauma, physical abuse, or emotional abuse in childhood were associated with having a history of traumatic brain injury (Song et al., 2018). These researchers also found that people who had 4 different types of childhood trauma were significantly more likely to have traumatic brain injury, indicating that negative childhood experiences can have a compounding effect on one’s risk of traumatic brain injury in life.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=772#h5p-97
Traumatic brain injury can result for many reasons. You may have heard the story of Stanley Cup champion Joe Murphy whose brain injury played a role in his experience of homelessness, pain management attempts, and mental illness. As you watch this brief investigative video from W5 entitled, “The rise and fall of a Stanley Cup champion,” we encourage you to think about it from a Primary Care and Nursing perspective. In particular, think back to the start of this section when we asked you to identify a care plan for a patient entering your clinical practice. Imagine now that patient was Joe Murphy.
At the beginning of the video, we encouraged you to think of yourself as Joe Murphy’s Physician or Nurse Practitioner. What medical conditions did you identify that need to be addressed? What social determinants of health emerged to situate his care in a broader context? How would you provide him with the best primary care possible, given his complex set of needs?
Housing First is one effective strategy for helping people with traumatic brain injury become stably housed. A study of 381 participants in the Toronto At Home / Chez Soi study, discussed further in the chapter on Politics, Policy, & Housing in Canada, found that Housing First participants had a significantly lower number of physical violence-related traumatic brain injury events, suggesting Housing First could be a targeted approach to help address this cause of traumatic brain injury (Mejia-Lancheros et al., 2020b).
The research evidence clearly shows that people who experience homelessness often have complicated health conditions that are not adequately addressed by mainstream health care approaches. One study in Montreal examined men’s ability to self-manage chronic health conditions within the context of homelessness and found that while they were generally confident in their abilities, their preferred mode of support was through consistent contact with health care providers and peer-support workers (Merdsoy, Lambert, & Sherman, 2020). The complexity of the health conditions, combined with the challenges of homelessness, makes it imperative for these individuals to have consistent health care. Ideally, this health care should be integrated in a way that meets their needs by offering specialized services that enhance continuity of care without requiring they go to multiple practitioners (Gentil, Grenier, Bamvita, & Fleury, 2020). Dr. Stephen Hwang discusses the importance of health care providers working together to support one another and provide the best patient care experience.
In this video, Dr. Stephen Hwang reflects on the combination of biomedical technical expertise and philosophical orientation towards helping that health care providers need to work in specialty care for populations experiencing homelessness. He notes that having a group of providers who are like-minded is important for practitioners to avoid burnout and have others to discuss challenging clinical situations with. Dr. Hwang concludes that it is important for all primary health care providers to have strong links to specialty care hospitals, as patients who experience homelessness often require hospitalization and/or specialty care. This video is 2:12 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: What specialized primary care would people who experience homelessness benefit from?
Improving patient satisfaction with their health care can involve promoting more tailored primary care programs that are adapted to the needs of patients with lived experience of homelessness (Gentil et al., 2020). Health care providers, like Family Physicians and Nurse Practitioners, can help by identifying which of their patients are experiencing homelessness or housing vulnerability, taking steps to help them connect with case managers, and working collaboratively using trauma-informed and anti-oppressive approaches (Andermann et al., 2020). We conclude this section, on what specialized primary care is needed for people experiencing homelessness, with a reminder from Dr. Naomi Thulien that what these patients need is the same as what all patients need – holistic team-based care in an environment that is beautiful, comfortable, and inclusive.
In this video, Dr. Naomi Thulien argues that we sometimes ask ourselves what people experiencing homelessness need, but we should realize that it is the same as what everyone needs. In primary care, that means a holistic team-based model comprised of Nurses, Social Workers, and Physicians located in a beautiful, comfortable, and accessible setting. Dr. Thulien elaborates that health care appointments should be longer to allow for urgent care matters to be addressed, as well as preventive discussions and measures around the social determinants of health. This video is 2:32 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: What specialized primary health care would people who experience homelessness benefit from?
We began this section by asking you to think about specialized primary care and how you, as a Family Physician or Nurse Practitioner, might apply your knowledge to care for a patient experiencing homelessness. We discussed a broad range of research literature to demonstrate the complexity of primary care needs and heard from Dr. Stephen Hwang that while the treatment plans are the same as for housed patients, it is the relational aspects that are different. We invited you to read and learn about a document outlining guidelines for clinical care of patients who are experiencing homelessness or housing vulnerability. It is important that this work be taken up in a way that is patient-centred, trauma-informed, and inclusive.
Specialized primary care requires that we consider the needs of individuals and tailor the care they receive to those needs. For instance, we saw how transgender individuals often receive care that is not appropriate or informed, which has detrimental effects on their well-being. We considered the role of sex work, violence, and early trauma as factors that account for the high rates of traumatic brain injury among people experiencing homelessness and examined a case study of Stanley Cup champion Joe Murphy. Finally, we saw that the best approach is one in which people receive team-based integrated care, so that their needs are met without having to go to multiple different locations. We ended on the idea that what people experiencing homelessness need from their primary care providers is fundamentally the same as what everyone needs, and that is to feel respected, included, and heard.
Click the link below to listen to all of the researchers answer the question “What specialized primary care would people who experience homelessness benefit from?” in audio format on our podcast!
106
In the final section, we take up a question that is as important as it is difficult. We know that death is part of life. In our society we have ideas about what a “good death” means, which is often that a person dies comfortably at home surrounded by loved ones. Like the pandemic messaging, that says to stay home if you are sick, the idea of dying at home requires that one have a home in which to die. This notion is rather straight-forward but it raises a number of considerations. If a person does not have a home, where do they go to die? What happens to the person’s belongings after they die? Who supports them at end-of-life if they are estranged from their family members?
Before you begin this section we encourage you to pause and consider this idea of a good death and whether it is possible within the context of homelessness. How can a person be supported to die a good death? Are there special end-of-life considerations for someone experiencing homelessness? You may use the space below to write your thoughts and reflections.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=774#h5p-98
This section follows from the previous two sections not only in order, but in logic. If a person has multiple chronic and complex health conditions and does not receive adequate health care to treat them, their risk of dying is considerably higher. We see from the research that people who experience homelessness have four times the rate of cancer (Lawrie, Charow, Giuliani, & Papadakos, 2020) and face higher risks of dying from hypothermia (Zhang et al., 2019), cardiovascular disease (Baggett et al., 2018), or as the result of cirrhosis, drug overdose, murder, or assault (Webster, 2017). In the next video, Dr. Katrina Milaney reflects on how being excluded from mainstream health care creates the conditions of neglect for people experiencing homelessness that carry into end-of-life.
In this video, Dr. Katrina Milaney explains that people who experience homelessness are often excluded from mainstream health care because of discrimination, which can lead them to get caught in a cycle of poor health and exclusionary practices. She notes that this cycle continues at end-of-life, as there are many people dying in shelters without good palliative care. While mobile teams do offer palliative care onsite in some agencies, Dr. Milaney argues we need to address the underlying issue that people experiencing homelessness lack equal access to the same kinds of care and dignity, at any stage of life, as those who are housed. This video is 2:00 in length and has closed captions available in English.
Key Takeaways – Dr. Katrina Milaney: Are there special end-of-life considerations for someone experiencing homelessness?
In a highly cited study, Dr. Stephen Hwang and his team (2009) examined mortality rates for people experiencing homelessness or housing vulnerability compared to those in higher income brackets. They calculated the probability of living to age 75 as an indicator. Take a moment to think now about your own life expectancy. What do you think the chances are that you will live to be 75 years of age? In this study, Hwang et al., (2009) found that for women living in homelessness or precarious housing, the probability of living to age 75 was 60% and for men it was a mere 32%. The risk of dying – and of dying prematurely – is considerably higher when a person is experiencing homelessness than when they are securely housed. Consider this statement as you watch Dr. Naheed Dosani speak about his work providing palliative care to people experiencing homelessness at end-of-life.
As we alluded to in the introductory part of this section, not having housing or a suitable place in which to die, is a primary challenge of supporting people experiencing homelessness to have a good death. Not having housing also removes a person’s ability to choose where they want to die. For instance, a review of how income impacts place of death in Toronto, not specifically related to homelessness, showed the those in the lowest income quintile were more likely to die in a hospital or palliative care unit than at home (Wales, Kalia, Moineddin, & Husain, 2020). While these places can certainly offer excellent end-of-life care, people experiencing homelessness are often lacking choice in whether or not they wish to die somewhere else. This suggests that people with lower incomes may lack the social and financial resources to die in a place of their choosing, such as their own home. In the next video, Dr. Bernie Pauly explains the need for more housing and hospice resources.
In this video Dr. Bernadette [Bernie] Pauly explains that it is often when they are nearing death that people who experience homelessness finally get access to housing. She notes that they often lack access to hospice care and may either get better in housing or die with limited resources. This video is 1:20 in length and has closed captions available in English.
Key Takeaways – Dr. Bernie Pauly: Are there special end-of-life considerations for someone experiencing homelessness?
Access to palliative care is a right that should be available to all persons at end-of-life, but a review of the literature shows that access is largely tied to having a higher socio-economic status (Huynh, Henry, & Dosani, 2015). Since there is no unified national strategy, many programs are inaccessible to people experiencing homelessness or are designed in ways that are prohibitive to meeting their needs (Huynh et al., 2015). Despite the high prevalence of multiple chronic health conditions and early mortality rates, there is limited published research on palliative care for people experiencing homelessness, and associated considerations such as their unique and complex circumstances, patient-related outcomes, caregiver burden, and cost-effectiveness (Sumalinog, Harrington, Dosani, & Hwang, 2017).
One of the barriers for people who are at end-of-life and experiencing structural vulnerability is that health care places tend to be imbued with social relations of power that reinforce structural vulnerability and produce further inequities in access and care (Giesbrecht et al., 2018). For instance, palliative care treatment, such as for people with advanced cancer, may be complicated by complex symptom burden among people who experience homelessness, are Indigenous, have a history of addictions, and have mental health or psychosocial issues (Santos Salas et al., 2019). We need to consider how previous experiences of health care, and power relations within them, influence people’s decision-making in relation to seeking support for serious illnesses like cancer (Moravac, 2018).
Dr. Stajduhar and her team (2019) conducted a critical ethnography with structurally vulnerable people at end-of-life, their support persons, and service providers, and found there were five significant barriers to accessing care that they faced. These included the need to focus on survival like finding food and shelter, the normalization of dying within this population and on the street, the problem of not being identified as being in need of end-of-life care unless actively being treated by a health care provider, having their environments being thought of as unsafe or risky for care providers to go particularly around stigmas attached to substance use, and cracks in the siloed care systems making it difficult to navigate care between health and social service systems (Stajduhar et al., 2019). Here Dr. Stajduhar speaks about her research further.
In this video, Dr. Kelli Stajduhar explains that a palliative approach to care is taking an upstream view for people who have serious and advancing chronic illness. For people experiencing homelessness, attending to the social determinants of health is the first palliative intervention. She notes that the average life expectancy for a person experiencing homelessness is lower than the average housed Canadian, but that these individuals are not always treated as though they are near death because the focus is on basic survival. Dr. Stajduhar notes that the unsafe drug supply and criminalization mean that within many communities dying has become normalized. People who experience homelessness may go to the hospital for serious chronic illness, yet not be identified as needing palliative care interventions. Dr. Stajduhar argues it is important not to make assumptions, but rather to use tools like advanced care planning to document their wishes. Much like the AIDS epidemic, people experiencing homelessness at end-of-life may be closer to non-biological persons than their bio-legal families, but these individuals may not be permitted to participate in their care plans. Dr. Stajduhar concludes that people experiencing homelessness near death may wish to die in a place that is comfortable to them, such as in a tent, and health care workers are needed even if they feel uncomfortable. Part of the work of mobile palliative care teams is about building community capacity and strength to flatten power differentials such as addressing the discrimination and stigma these patients experience, even when near death. This video is 8:55 in length and has closed captions available in English.
Key Takeaways – Dr. Kelli Stajduhar: Are there special end-of-life considerations for people experiencing homelessness?
Dr. Stajduhar explains that in palliative care the question is posed, “Is homelessness a terminal diagnosis?” Based on what you have learned so far, what do you think? Ishomelessness a terminal diagnosis? Does it needto be a terminal diagnosis, or is there something we could do to change this trajectory?
Dr. Stajduhar makes the comparison to people dying during the AIDS epidemic being denied the support of their partners and chosen family because of restrictive societal definitions of who constitutes one’s family. We see similar circumstances as people experiencing homelessness may die, particularly if in hospital, without being permitted to have their street friends and families present. This issue is explored further in the featured reading below, from Dr. Stajduhar and her research team. This article details a study of 25 family caregivers for people at end-of-life, which found that nearly half of the family caregivers were themselves living with constraints of structural vulnerability, such as poverty, substance use, and homelessness, and were part of the person’s street family (Stajduhar, Giesbrecht, Mollison, Dosani, & McNeil, 2020). We invite you to read this ethnographic study below.
Stajduhar, K. I., Giesbrecht, M., Mollison, A., Dosani, N., & McNeil, R. (2020). Caregiving at the margins: An ethnographic exploration of family caregivers experiences providing care for structurally vulnerable populations at the end-of-life. Palliative Medicine, 34(7), 946–953.
A final issue pertaining to end-of-life care that has already been raised, but deserves further consideration, is that of planning for one’s death and what happens afterward. Many people in society create wills as a way to dictate who will receive their property, such as their house, and who will inherit any money they leave behind. Many people will also have written instructions on what they want to happen to them in the event of a medical emergency, such as providing life-sustaining measures or not. When a person who is experiencing homelessness nears death, they often will also have possessions they wish to give to the special people in their lives, and ideas about how they want their final moments to be spent.
Advance care directives are used in palliative and medical settings to help a person document these wishes in the event they are unable to communicate them directly at a later time. Leung et al., (2017) conducted a study in Toronto to see whether advance care directives created in a community setting by people experiencing homelessness would be utilized in subsequent hospitalizations over the period of 1 year and found that hospital workers were significantly likely to use them if they were on record. In the next video Dr. Stephen Hwang, a co-author of this study, explains the value of advance care planning in helping to navigate some of the challenges associated with end-of-life care for people experiencing homelessness.
In this video, Dr. Stephen Hwang discusses the additional challenges of offering palliative care to patients who lack housing. He notes that often these patients have close relationships with others residing or working in shelters and may wish to die in the shelter itself. He explains that these patients may have lost contact with biological family members in their lives and wish to re-establish these connections when they are near death. From a health provider perspective, Dr. Hwang notes, it can be challenging to know who to contact when an unhoused patient arrives at hospital actively near death. He urges practitioners who work with homeless populations to ask the ‘surprise’ question, about whether they would be surprised if the person died within a year. If the answer is no, practitioners should have end-of-life discussions. Dr. Hwang concludes that these conversations should likely occur with most people experiencing homelessness, as their risk of death is considerably higher. This video is 3:07 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Are there special end-of-life considerations for someone experiencing homelessness?
Advance care planning is an important palliative care measure because it offers tangible guidance to care providers while also providing the person who is near death a sense of reassurance that their wishes will be respected. This planning can be done at any stage, even if not immediately near death, to help document and communicate one’s requests. As Dr. Stajduhar explains in the next video, this process provides hope to the individual and their support network within the community.
In this video, Dr. Kelli Stajduhar reflects on her involvement in community-based palliative care work, and the important role it plays for people experiencing homelessness. Notably, she cites advanced care planning as something that occurs in palliative care, where health and social care providers talk with people about what is important to them and what their wishes are. This information is recorded and submitted to the hospital for use in the event the person is admitted while critically ill. Dr. Stajduhar concludes that palliative care approaches offer community members a sense of hope that their wishes will be respected. This video is 3:31 in length and has closed captions available in English.
Key Takeaways – Dr. Kelli Stajduhar: The impact of palliative care in the community
People who experience homelessness and their health care providers negotiate many obstacles in the provision and receipt of palliative care. However, there is tremendous potential and opportunity to improve quality of care at the end–of–life for this vulnerable population (West, Wrobel, Pallotta, & Coatsworth, 2020). Opportunities for helping people achieve a good death are explored further in this brief video entitled, “Dignity, at the end of life, for the homeless.”
Death and dying are difficult topics to consider. As we began this section by stating, we have specific ideas about what a good death looks like in our society, which generally means dying at home, in bed, surrounded by loved ones. Homelessness challenges this notion and requires that we think differently about what it means to support someone who is at end-of-life without the resources and comforts that many housed individuals might take for granted.
We began by referencing the preceding sections that showed people who experience homelessness often have complex and chronic health issues and lack equitable access to the primary care needed to treat them. The rates of mortality are considerably higher amongst people experiencing homelessness, as is dying at an earlier age. You may recall that research shows the chances of living to age 75 are only 60% for women and 32% for men experiencing homelessness (Hwang et al., 2009). These figures are heart-breaking, if not surprising.
We learned that although palliative care is a right there is no unified national strategy, which makes access particularly challenging for people living with structural vulnerabilities like homelessness. The research identified a number of special considerations for people experiencing homelessness at end-of-life. Notably, they may lack access to hospice care, not be permitted to die in a shelter, not have their loved ones with them, and have their possessions discarded against their wishes. Some of these challenges can be prevented through advance care planning, which is a tool used in palliate care to help people document and communicate their wishes. While palliative care is a difficult field, it is critically important to provide hope to people at end-of-life, their loved ones, and the community as a whole.
Click the link below to listen to all of the researchers answer the question “Are there special end-of-life considerations for someone experiencing homelessness?” in audio format on our podcast!
107
Tom
We met Tom at the beginning of the chapter. He has lived on the streets for the bulk of the last 3 years. If you recall the study by Hwang et al. , (2009) the authors indicated that men only have a 32% chance of living to 75 if experiencing homelessness. At 75 years of age, he has surpassed these odds, but he still faces a very uncertain future as his physical and mental health deteriorate. The NP assessing Tom has significant concern that he is experiencing signs of lung cancer. He is also concerned that Tom may have signs of worsening dementia, making his care more complex.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1192#h5p-87
108
We began this chapter on Primary Care and Nursing by inviting you to think about health care as a key consideration related to understanding homelessness in Canada. Although we all have had our own experiences within the health care system, it is important to step back and consider other points of view.
At the start of the chapter, we introduced you to the composite character Tom, who was a 75-year-old widower experiencing homelessness who had a complex set of health issues. The scenario was presented as an entry point into thinking about the complexity of health care access and homelessness. We returned to Tom’s story again at the end to demonstrate how his experience can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada
We then asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked,“Do people experiencing homelessness have equitable access to primary health care?”The answer here was a resounding no. We examined the social determinants of health as an explanation for why people experiencing homelessness are often in poor health. There are a range of barriers they encounter in seeking care including, but not limited to, discrimination within health care settings. We saw that mainstream health care is often inaccessible, so mobile outreach and shelter-based health care clinics are offered as alternatives. While these approaches have their benefits, they do not solve the underlying issue of inequitable primary care access. To change our system, we need dedicated Family Physicians and Nurse Practitioners treating clients with trauma-informed and socially-inclusive care practices, while also advocating for them on a broader scale within society.
Next we asked, “What specialized primary care would people who experience homelessness benefit from?” We began this section by considering a broad range of health conditions that are associated with homelessness, and we learned that while the clinical approach to treatment remains the same whether a patient is experiencing homelessness or is housed, the relational aspects of care are more complex. The need for tailored approaches was demonstrated through the clinical guidelines, consideration of transgender patients, and a case study on traumatic brain injury. Yet, while patient-centered care needs to be tailored to the individual’s needs, it is also critically important to remember that what everyone has in common is the need for health care that is welcoming, respectful, and accessible regardless of their housing status.
Finally, we asked, “Are there special end-of-life considerations for someone experiencing homelessness?” In the last section, we took a difficult look at how ideas about what constitutes a good death are challenged by homelessness. We began by reviewing the common causes of mortality, and how they contribute to premature death. Although palliative care is a fundamental human right, there is no unified national strategy at present, meaning that people living in homelessness or housing vulnerability may not receive the same level of care as those who have more financial resources. Measures such as advance care planning are important steps that can help provide a sense of dignity and hope at end-of-life by reaffirming the value of life and that one’s wishes will be respected after they are gone.
109
Here are some additional resources you may want to check out!
110
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
111
Abramovich, A., de Oliveira, C., Kiran, T., Iwajomo, T., Ross, L. E., & Kurdyak, P. (2020). Assessment of health conditions and health service use among transgender patients in Canada. JAMA Netw Open, 3(8), https://doi.org/10.1001/jamanetworkopen.2020.15036
Abramovich, A., Lam, J. S. H., & Chowdhury, M. (2020). A transgender refugee woman experiencing posttraumatic stress disorder symptoms and homelessness. Canadian Medical Association Journal (CMAJ), 192(1), E9–E11. https://doi.org/10.1503/cmaj.190974
Andermann, A., Bloch, G., Goel, R., Brcic, V., Salvalaggio, G., Twan, S., … Pottie, K. (2020). Caring for patients with lived experience of homelessness. Canadian Family Physician, 66(8), 563–570. PMC7430777
Asare, A. O., Wong, A. M., Maurer, D., & Nishimura, M. (2019). Access to vision services by vulnerable populations in Canada: A scoping review. Journal of Health Care for the Poor and Underserved, 30(1), 6–27. https://doi.org/10.1353/hpu.2019.0003
Baggett, T. P., Liauw, S. S., & Hwang, S. W. (2018). Cardiovascular disease and homelessness. Journal of the American College of Cardiology, 71(22), 2585–2597. https://doi.org/10.1016/j.jacc.2018.02.077
Baumann, R. M., Hamilton-Wright, S., Riley, D. L., Brown, K., Hunt, C., Michalak, A., & Matheson, F. I. (2019). Experiences of violence and head injury among women and transgender women sex workers. Sexuality Research & Social Policy, 16(3), 278–288. https://doi.org/10.1007/s13178-018-0334-0
Chiu, S., Redelmeier, D. A., Tolomiczenko, G., Kiss, A., & Hwang, S. W. (2009). The health of homeless immigrants. Journal of Epidemiology & Community Health, 63(11), 943-948. http://dx.doi.org/10.1136/jech.2009.088468
Crowe, C. (2019). A knapsack full of dreams: memoirs of a street nurse. Victoria, BC: FriesenPress.
Crowe, C., & Baker, N. (2007). Dying for a home: homeless activists speak out. Toronto, ON: Between the Lines.
Daiski, I. (2007). Perspectives of homeless people on their health and health needs priorities. Journal of Advanced Nursing, 58(3), 273-281. https://doi.org/10.1111/j.1365-2648.2007.04234.x
D’Souza, S., M., Mirza, N. A., & Nairy Karkada, S. (2021). Development of a foot care model to determine the risk of foot problems among homeless adults in Canada. Health & Social Care in the Community. https://doi.org/10.1111/hsc.13271
Frankish, C. J., Hwang, S. W., & Quantz, D. (2005). Homelessness and health in Canada: Research lessons and priorities. CJPH, 95, S23-S29. https://doi.org/10.1007/BF03403700
Gentil, L., Grenier, G., Bamvita, J. M., & Fleury, M. (2020). Satisfaction with health and community services among homeless and formerly homeless individuals in Quebec, Canada. Health & Social Care in the Community, 28(1), 22–33. https://doi.org/10.1111/hsc.12834
Giesbrecht, M., Stajduhar, K. I., Mollison, A., Pauly, B., Reimer-Kirkham, S., McNeil, R., … Rose, C. (2018). Hospitals, clinics, and palliative care units: Place-based experiences of formal healthcare settings by people experiencing structural vulnerability at the end-of-life. Health & Place, 53, 43–51. https://doi.org/10.1016/j.healthplace.2018.06.005
Gilmer, C., & Buccieri, K. (2020). Homeless patients associate clinician bias with suboptimal care for mental illness, addictions, and chronic pain. Journal of Primary Care & Community Health, 11. https://doi.org/10.1177/2150132720910289
Guirguis-Younger, M., McNeil, R., & Hwang, S. W. (Eds.). (2014). Homelessness and health in Canada. Ottawa: University of Ottawa Press. Homelessness and Health in Canada (uottawa.ca)
Hardill, K. (2007). From the grey nuns to the streets: A critical history of outreach nursing in Canada. Public Health Nursing, 24(1), 91–97. https://doi.org/10.1111/j.1525-1446.2006.00612.x
Hossain, R., Ramsay, N., Moore, M., & Milo, M. (2018). Health advocacy training through research‐based theatre. Medical Education, 52(11), 1187–1188. https://doi.org/10.1111/medu.13703
Huynh, L., Henry, B., & Dosani, N. (2015). Minding the gap: Access to palliative care and the homeless. BMC Palliative Care, 14, 62. https://doi.org/10.1186/s12904-015-0059-2
Hwang, S. W. (2001). Homelessness and health. CMAJ, 164(2), 229-233. 229.full.pdf (cmaj.ca)
Hwang, S. W., Wilkins, R., Tjepkema, M., O’Campo, P. J., & Dunn, J. R. (2009). Mortality among residents of shelters, rooming houses, and hotels in Canada: 11 year follow-up study. BMJ, 339. doi: https://doi.org/10.1136/bmj.b4036
Jaworsky, D., Gadermann, A., Duhoux, A., Naismith, T. E., Norerna, M., To, M. J., Hwang, S. W., & Palepu, A. (2016). Residential stability reduces unmet health care needs and emergency department utilization among a cohort of homeless and vulnerably housed persons in Canada. Journal of Urban Health, 93, 666-681. https://doi.org/10.1007/s11524-016-0065-6
Jiang, S., Mikhail, M., Slomovic, J., Pereira, A., Lebovic, G., Noel, C., & Lichter, M. (2020). Prevalence and impact of eye disease in an urban homeless and marginally housed population. Canadian Journal of Ophthalmology, 55(1), 76–81. https://doi.org/10.1016/j.jcjo.2019.07.006
Kelly, K., & Caputo, T. (2007). Health and street/homeless youth. Journal of Health Psychology, 12(5), 726-736. https://doi.org/10.1177/1359105307080594
Khandor, E., Mason, K., Chambers, C., Rossiter, K., Cowan, L., & Hwang, S. W. (2011). Access to primary health care among homeless adults in Toronto, Canada: Results from the street health survey. Open Med, 5(2), e94-e103. PMID: 21915240
Lawrie, K., Charow, R., Giuliani, M., & Papadakos, J. (2020). Homelessness, cancer and health literacy: A scoping review. Journal of Health Care for the Poor and Underserved, 31(1), 81–104. https://doi.org/10.1353/hpu.2020.0010
Leung, A. K., To, M. J., Luong, L., Vahabi, Z. S., Gonçalves, V. L., Song, J., & Hwang, S. W. (2017). The effect of advance directive completion on hospital care among chronically homeless persons: A prospective cohort study. Journal of Urban Health, 94(1), 43–53. https://doi.org/10.1007/s11524-016-0105-2
Liu, M., & Hwang, S. W. (2021). Health care for homeless people. Nature Reviews Disease Primers 7, 5. https://doi.org/10.1038/s41572-020-00241-2
Mago, A., Brondani, M. A., MacEntee, M. I., & Frankish, C. J. (2018). A model pathway to oral health care for homeless people. J Can Dent Assoc, 84, i10. https://pubmed.ncbi.nlm.nih.gov/31199725/
Magwood, O., Hanemaayer, A., Saad, A., Salvalaggio, G., Bloch, G., Moledina, A., Pinto, N., Ziha, L., Geurguis, M., Aliferis, A., Kpade, V., Arya, N., Aubry, T., & Pottie, K. (2020). Determinants of implementation of a clinical practice guideline for homeless health. International Journal of Environmental Research and Public Health, 17(21), 7938. https://doi.org/10.3390/ijerph17217938
Mejia-Lancheros, C., Lachaud, J., Nisenbaum, R., Wang, A., Stergiopoulos, V., Hwang, S. W., & O’Campo, P. (2020a). Dental problems and chronic diseases in mentally ill homeless adults: a cross-sectional study. BMC Public Health, 20(1), 419. https://doi.org/10.1186/s12889-020-08499-7
Mejia-Lancheros, C., Lachaud, J., Stergiopoulos, V., Matheson, F. I., Nisenbaum, R., O’Campo, P., & Hwang, S. W. (2020b). Effect of housing first on violence-related traumatic brain injury in adults with experiences of homelessness and mental illness: Findings from the at home/chez soi randomised trial, Toronto site. BMJ Open, 10(12), e038443–e038443. https://doi.org/10.1136/bmjopen-2020-038443
Merdsoy, L., Lambert, S., & Sherman, J. (2020). Perceptions, needs and preferences of chronic disease self‐management support among men experiencing homelessness in Montreal. Health Expectations: An International Journal of Public Participation in Health Care and Health Policy, 23(6), 1420–1430. https://doi.org/10.1111/hex.13106
Moravac, C. C. (2018). Reflections of homeless women and women with mental health challenges on breast and cervical cancer screening decisions: Power, trust, and communication with care providers. Frontiers in Public Health, 6, 30. https://doi.org/10.3389/fpubh.2018.00030
Nikoo, N., Javidanbardan, S., Akm, M., Hakobyan, S., Nikoo, M., Kwan, C., … Krausz, M. (2019). Hepatitis C prevalence and associated risk factors among individuals who are homeless and diagnosed with mental illness: At home / chez soi study, Vancouver, BC. European Journal of Public Health, 29(2), 242–247. https://doi.org/10.1093/eurpub/cky142
Noel, C. W., Mok, F., Wu, V., Eskander, A., Yao, C. M. K. L., Hwang, S. W., … Lee, J. M. (2020). Hearing loss and hearing needs in an adult homeless population: A prospective cross-sectional study. CMAJ Open, 8(1), E199–E204. https://doi.org/10.9778/cmajo.20190220
Oosman, S., Weber, G., Ogunson, M., & Bath, B. (2019). Enhancing access to physical therapy services for people experiencing poverty and homelessness: The lighthouse pilot project. Physiotherapy Canada, 71(2), 176–186. https://doi.org/10.3138/ptc.2017-85.pc
Palayew, A., Kaur, H., Magwood, O., Greenaway, C., Mayhew, A., Hatcher-Roberts, J., & Pottie, K. (2018). P2‐112: Values, preferences, and acceptability of hepatitis C testing and treatment in the homeless and vulnerably housed: A scoping review. Journal of Viral Hepatitis, 25(S2), 163–164. https://doi.org/10.1111/jvh.229_12923
Paradis-Gagné, E., Pariseau-Legault, P., Villemure, M., & Chauvette, S. (2020). A critical ethnography of outreach nursing for people experiencing homelessness. Journal of Community Health Nursing, 37(4), 189–202. https://doi.org/10.1080/07370016.2020.1809858
Pottie, K., Kendall, C. E., Aubry, T., Magwood, O., Andermann, A., Salvalaggio, G., … Hwang, S. W., Stergiopoulos, V., & Tugwell, P. (2020). Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience. Canadian Medical Association Journal (CMAJ), 192(10), E240–E254. https://doi.org/10.1503/cmaj.190777
Ramsay, N., Hossain, R., Moore, M., Milo, M., & Brown, A. (2019). Health care while homeless: Barriers, facilitators, and the lived experiences of homeless individuals accessing health care in a Canadian regional municipality. Qualitative Health Research, 29(13), 1839–1849. https://doi.org/10.1177/1049732319829434
Registered Nurses’ Association of Ontario. (2004). Position statement: Homelessness. RNAO: Ontario. https://rnao.ca/policy/position-statements/homelessness
Richard, L., Booth, R., Rayner, J., Clemens, K. K., Forchuk, C., & Shariff, S. Z. (2021). Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: A retrospective cohort study. CMAJ Open, 9(1), E1–E9. https://doi.org/10.9778/cmajo.20200287
Rivera, L. A., Henschke, M. T., Khoo, E., Ing, S., Bae, S. J., Rice, C. M., … Forseth, M. H. (2018). A modeling study exploring the impact of homelessness on rostered primary care utilization in Calgary, Canada. Canadian Journal of Public Health, 109(4), 451–458. https://doi.org/10.17269/s41997-018-0098-6
Santos Salas, A., Watanabe, S. M., Tarumi, Y., Wildeman, T., Hermosa García, A. M., Adewale, B., & Duggleby, W. (2019). Social disparities and symptom burden in populations with advanced cancer: specialist palliative care providers’ perspectives. Supportive Care in Cancer, 27(12), 4733–4744. https://doi.org/10.1007/s00520-019-04726-z
Song, M. J., Nikoo, M., Choi, F., Schütz, C. G., Jang, K., & Krausz, R. M. (2018). Childhood trauma and lifetime traumatic brain injury among individuals who are homeless. The Journal of Head Trauma Rehabilitation, 33(3), 185–190. https://doi.org/10.1097/HTR.0000000000000310
Stajduhar, K. I., Giesbrecht, M., Mollison, A., Dosani, N., & McNeil, R. (2020). Caregiving at the margins: An ethnographic exploration of family caregivers experiences providing care for structurally vulnerable populations at the end-of-life. Palliative Medicine, 34(7), 946–953. https://doi.org/10.1177/0269216320917875
Stajduhar, K. I., Mollison, A., Giesbrecht, M., McNeil, R., Pauly, B., Reimer-Kirkham, S., … Rounds, K. (2019). “Just too busy living in the moment and surviving”: Barriers to accessing health care for structurally vulnerable populations at end-of-life. BMC Palliative Care, 18(1), 11. https://doi.org/10.1186/s12904-019-0396-7
Sumalinog, R., Harrington, K., Dosani, N., & Hwang, S. W. (2017). Advance care planning, palliative care, and end-of-life care interventions for homeless people: A systematic review. Palliative Medicine, 31(2), 109-119. doi: 10.1177/0269216316649334
Vogel, M., Frank, A., Choi, F., Strehlau, V., Nikoo, N., Nikoo, M., … Schütz, C. G. (2017). Chronic pain among homeless persons with mental illness. Pain Medicine, 18(12), 2280–2288. https://doi.org/10.1093/pm/pnw324
Wales, J., Kalia, S., Moineddin, R., & Husain, A. (2020). The impact of socioeconomic status on place of death among patients receiving home palliative care in Toronto, Canada: A retrospective cohort study. Journal of Palliative Care, 35(3), 167–173. https://doi.org/10.1177/0825859719855020
Webster, P. (2017). Bringing homeless deaths to light. Canadian Medical Association Journal, 189(11), E446–E447. https://doi.org/10.1503/cmaj.1095399
West, K. J., Wrobel, B., Pallotta, S., & Coatsworth, A. (2020). Bearing witness: Exploring the end-of-life needs of homeless persons and barriers to appropriate care. Omega: Journal of Death and Dying, 82(1), 63–91. https://doi.org/10.1177/0030222818801150
Whisler, A., Dosani, N., To, M. J., O’Brien, K., Young, S., & Hwang, S. W. (2021). The effect of a housing first intervention on primary care retention among homeless individuals with mental illness. PloS One, 16(2), e0246859–e0246859. https://doi.org/10.1371/journal.pone.0246859
Wu, V., Noel, C. W., Forner, D., Mok, F., Zirkle, M., Eskander, A., … Lee, J. M. (2020). Otolaryngology needs among an adult homeless population: a prospective study. Journal of Otolaryngology-Head and Neck Surgery, 49(1), 1–47. https://doi.org/10.1186/s40463-020-00445-2
Zhang, P., Wiens, K., Wang, R., Luong, L., Ansara, D., Gower, S., … Hwang, S. W. (2019). Cold weather conditions and risk of hypothermia among people experiencing homelessness: Implications for prevention strategies. International Journal of Environmental Research and Public Health, 16(18), 3259. https://doi.org/10.3390/ijerph16183259
XI
People who experience homelessness often lack access to consistent and reliable primary care. As a result, many turn to emergency services – such as a hospital emergency room (ER) – when health care is needed. It may be that the person uses the ER as a substitute form of gaining access to a health care provider, or it may be that the person waits until a health care issue has become a crisis before they seek care. Either way, hospitals are a site where people experiencing homelessness encounter the health care system. At times it may be brief, such as an ER visit, or it may be extended contact, such as through longer-term hospital admissions.
This raises questions about the roles that hospitals can play in identifying persons experiencing homelessness and in serving as a site of intervention. If it is known that people who experience homelessness are likely, at some point, to access hospital care then we have an opportunity to reimagine the role that hospitals play in addressing and even preventing homelessness in Canada.
112
In this chapter, you are invited to think about how hospitals, and hospital workers, can be considered an extended part of our nation’s homelessness response. While thinking critically about emergency medicine and longer-term hospital admissions, you are encouraged to reflect upon three key questions guiding this chapter’s learning objectives.
As you move through this chapter it is beneficial to keep in mind that hospitals are a key site of contact between people experiencing homelessness and the health care system. It is vital that workers within these settings – whether in the ER or related to longer-term admissions – understand the importance of the roles they play. Read on to learn more about emergency medicine, hospitals, and how they can help patients experiencing homelessness.
113
We begin this chapter by presenting a composite scenario that reflects real-world experiences of homelessness in Canada, as they pertain to Emergency Medicine. As you work through the scenario, you are encouraged to adopt both an empathic perspective, to consider your own response(s) within the scenario, and a critical perspective, to think about how the scenario represents larger issues impacting people in our society.
After considering the real-world scenario, we will endeavour to answer each question posed in the learning objectives. Do people who experience homelessness use emergency medical services at a high rate? What happens after patients who are experiencing homelessness are discharged from hospital? Would improved funding for affordable housing decrease the burden on hospitals? Throughout this chapter, we will examine these three questions, using academic literature, featured articles, lived experience representation, multi-media activities, and virtual guest lectures from some of Canada’s leading homelessness researchers.
At the end of the chapter, we will return to the scenario presented at the beginning and reconsider it in light of what has been learned. Together we will see how a framework of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health is critical for understanding homelessness in Canada. These concepts will re-emerge in each chapter throughout this book to demonstrate the complexity and inter-connected nature of these issues.
114
As you learn about homelessness and the complex ways in which it is experienced, we encourage you to begin with this real life composite scenario. Take a moment here to pause and consider this person’s experience.
Pia
Pia is a 50-year-old female. She has a history of substance misuse, who has been drug free for 2 years. She is currently living in a local shelter as her partner died suddenly from a massive stroke, without an updated will. All of his assets went to his wife, whom he had been estranged from for 15 years, forcing her return to her hometown. Pia presents to the emergency department of the local community hospital with severe abdominal pain. She has a history of GI issues including Irritated Bowel Syndrome (IBS). She has been managing her IBS successfully with diet and the support of her Nurse Practitioner. Since moving home, she has yet to find a primary health care provider. On admission to the emergency department her old records are accessed. The most recent visit was 5 years previous. After reviewing the old records, the first notation made at the top of the new chart is “known drug user.” She is seen by the ER nurse and physician who both ask about drug use. She explains her history to them, including her success with sobriety. She denies any recent drug misuse. She waits in the ER for 16 hours, very uncomfortable. No tests are done. No pain medications are offered. No referral is sent for a surgical consult. She is discharged at 4:00 am still with significant pain. The final entry on the ER record is “discharged home, pain of unknown origin.” Pia was admitted 3 days later for a ruptured appendix, requiring surgical intervention.
With this scenario fresh in your mind, consider these reflection questions. You may wish to record your answers before moving on to the next section. We will return to the scenario again at the end of the chapter.
Reflection Questions
115
In the previous chapter, on Primary Care & Nursing, we examined the inequities that people who experience homelessness face in accessing health care. Research has consistently shown that most people who experience homelessness do not have a primary care provider, such as a Physician or Nurse Practitioner. We also saw in the previous chapter that many people who experience homelessness have chronic health conditions and that these conditions emerge at a premature age. Given this information, we begin this chapter on Emergency Medicineby considering whether people experiencing homelessness may perhaps turn to medical services, such as hospital emergency departments, as a foreseeable outcome. Before you continue through the material, we invite you to consider this question and record your thoughts in the space below. You may write as little or as much as you would like.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=783#h5p-99
By now you likely know that the premise of this book is to ask simple questions that actually have rather complex answers. However, you may be wondering why we asked such a simple question to begin this chapter. Do people experiencing homelessness use emergency medical services at a high rate? This seems like a yes or no answer, so how can we write an entire section about it? Each of the researchers we posed this question to answered with a yes, and then followed it with a “but.” Yes, people who experience homelessness do use emergency medical services at a high rate, but… It is what comes after the “but” that makes this a seemingly simple question with a rather complex answer.
We begin with a video of Dr. Cheryl Forchuk that was recorded while she was onsite at a hospital during the COVID-19 pandemic in the summer of 2021. Dr. Forchuk’s research has shown a connection between homelessness and hospitalization for COVID-19. Notably, participants in her team’s study who had a recent history of homelessness were more likely to be tested for COVID-19 and to have the test return positive (Richard et al., 2021). Further, participants of the study with a recent history of homelessness were found to be 20 times more likely to be admitted to hospital for COVID-19, over 10 times more likely to require intensive care, and over 5 times more likely to die within 21 days of their first positive test result (Richard et al., 2021). In the video below, Dr. Forchuk explains further.
When the videos in this ebook are almost done playing, the message “Stop the video now” will appear in the top left corner. This is a reminder for those who have turned on the Autoplay setting to manually pause the video when the speakers are done to avoid having it autoplay through to the next video. This message will appear in all researcher videos throughout the ebook.
Note: Viewers may still need to use their discretion in stopping other YouTube content such as ads.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk explains that the literature shows people who experience homelessness are more likely to use emergency medical services but that the figures vary by study. She notes that when individuals experiencing homelessness go to the hospital, they have higher rates of admission, longer stays, and increased rates of readmission compared to housed patients. This video is 0:39 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Do people who experience homelessness use emergency medical services at a high rate?
Dr. Forchuk explains that people who experience homelessness do use emergency medical services at a high rate, butthat the estimates vary across studies. Researchers use different methodologies for collecting data about homelessness and emergency department use, such as through surveys, interviews, and focus groups, that can produce different estimates. However, we can also learn a lot about homelessness and people’s access to medical services from administrative health records (Wiens, Rosella, Kurdyak, & Hwang, 2020). For instance, A review of administrative health data from emergency departments in Ontario between 2010 and 2017 identified 39,408 patients who were experiencing homelessness and also showed that the number of emergency department visits increased over the period of study (Strobel et al., 2021). These researchers found that the number of visits were at their highest annually in September and at their lowest each year in January, with hospital visits more highly concentrated in urban centres (Strobel et al., 2021). This study shows how administrative health data can help us learn more about the demographics and characteristics of people experiencing homelessness, by serving as both point-in-time and longitudinal sources of information (Strobel et al., 2021). We invite you to learn more about this study and its findings in this section’s featured reading below.
Strobel, S., Burcul, I., Dai, J. H., Ma, Z., Jamani, S., & Hossain, R. (2021). Characterizing people experiencing homelessness and trends in homelessness using population-level emergency department visit data in Ontario, Canada. Ottawa: Statistics Canada, Health Reports.
Administrative health data, as well as self-reports, are important sources of information for understanding the reasons some people who experience homelessness use emergency medical services at a higher rate. We say “some people” because it must be noted not every person who experiences homeless uses hospitals at a high rate. Rather, what our own research shows is that there is a small percentage who use hospitals on a frequent basis. We conducted surveys, interviews, and hospital record reviews for 52 people experiencing homelessness or housing insecurity in a small semi-rural town in Ontario. This review showed that in the preceding year over half (54%) had visited the hospital. These 28 individuals collectively went to the hospital 76 times, for medical (79%), mental health (17%) and dental (4%) reasons. While 28 of the 52 participants had been to the hospital in the preceding year, 6 were found to be frequent users and another 2 were highly frequent users, accounting for 15 and 28 of the total hospital visits respectively. Collectively these 8 individuals, who accounted for 15% of the sample, produced 75% of the hospital visits for people in this study in 2018 (Gilmer & Buccieri, 2020).
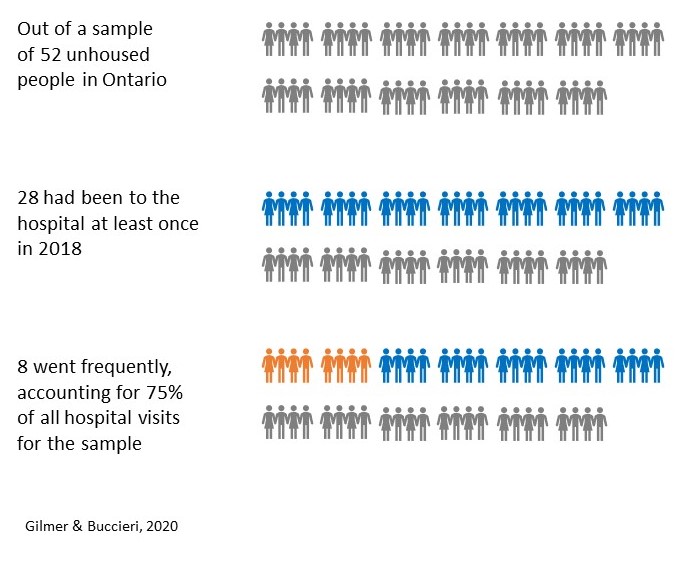
It is clear from this data that not every person who experiences homelessness uses hospital services but that, of those who do, a minority use it frequently. In the next video Dr. Stephen Hwang, St. Michael’s Hospital Chair in Homelessness, Housing and Health, explains in the next video why it is important we consider the reasons that people go to the hospital and not confuse high use with unnecessary use.
In this video, Dr. Stephen Hwang explains that on average people who experience homelessness use the hospital and emergency health services at higher rates, but that it is important not to overgeneralize. He notes there is heterogeneity, as some people are very high users while others are not. Framing the issue more holistically, Dr. Hwang encourages us not to confuse high usage with unnecessary usage, but rather to notice that people experiencing homelessness who seek frequent emergency care often do so because of high rates of illness. He concludes that rather than trying to reduce emergency medical care usage, we should focus instead on improving access to primary care. This video is 3:54 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Do people who experience homelessness use emergency medical services at a high rate?
When people have high rates of chronic illness and low rates of primary care access, it is not surprising they will seek out alternative health care services, such as through a hospital’s emergency department. We said at the beginning of this section that we know as a whole people who experience homelessness use emergency medical services at higher rates, and that it is the “but” that follows we are interested in learning more about. Dr. Hwang tells us the rates are higher, but that we need to recognize people are there for legitimate medical reasons that are not being well-served through mainstream primary care services.
The link between hospital use and primary care issues is well founded in the literature. Our own research, for instance, again shows that amongst the 52 participants only 28% had a primary care provider in the city where they lived, and those who went to the hospital primarily did so for medical issues, pain, mental health support, overdose or drug-related complications, and dental care (Gilmer & Buccieri, 2020). Moderate to severe chronic pain is a common reason why people who experience homelessness seek medical treatment and is more common among people who also have major depressive disorder, post-traumatic stress disorder, and report suicidality among other conditions (Vogel et al., 2017).
It is also common that patients experiencing homelessness seek care at hospitals because they have complex health care issues that require specialized services. Research conducted at The Ottawa Hospital emergency department over a two-year period showed that during this time, 129 surgical referrals were made for 97 adults experiencing homelessness who visited the emergency department (Zuccaro, Champion, Bennett, & Ying, 2018). Of these referred patients, only 36% had a primary care physician and the majority were given surgical referrals due to traumatic injury (64%), with orthopedic surgery being the most commonly consulted service (Zuccaro et al., 2018). Another study of surgical outcomes for ankle fractures conducted in Ontario showed that, although complications are rare, patients who are marginalized are at significantly increased risk of infection and amputation following the procedure (Wolfstadt, Pincus, Kreder, & Wasserstein, 2019). What these studies collectively tell us, is that people who experience homelessness tend to use emergency medical services at a higher rate than those who are housed, but their records indicate they require specialized referrals and have higher risk of post-operative complications. In the video that follows, Dr. Naomi Thulien speaks about the benefit of hospitals offering centralized access to specialized services for these patients with complex medical and social needs.
In this video, Dr. Naomi Thulien argues that people who experience homelessness do use emergency medical services at a higher rate, but it is in part because they offer centralized services. She notes that relationship building is a particularly important part of health care for this population and that this has been challenging during COVID-19. Dr. Thulien concludes that there is no one-size-fits-all approach for health care but that people who experience homelessness benefit from socially inclusive services. This video is 4:06 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Thulien: Do people who experience homelessness use emergency medical services at a high rate?
The notion that there is no-size-fits-all approach for supporting people experiencing homelessness is a common theme that runs through this book. We have seen that some people who experience homelessness use emergency medical services at a high rate, while others do not use it at all.
Can we predict which individuals experiencing homelessness will be high users of emergency medical services based on shared characteristics? Are there factors that you think might lead some people to use emergency departments more than others?
Gabet, Grenier, Cao, and Fleury (2019) set out to answer this question by recruiting 270 individuals from shelters, temporary housing, and permanent housing in Montreal. They interviewed participants at baseline (i.e. entry into the study), and again 12 months later to see whether there were commonalities between those who used emergency departments during that time and those who did not. They found that having a substance use disorder and low perceived physical health were both need-factors that related to higher emergency department use. Interestingly, emergency department use was not associated with the different types of housing (Gabet et al., 2019).
In another study, researchers in Vancouver sought to identify factors associated with hospitalization for people experiencing homelessness or housing vulnerability (Gadermann et al., 2020). They found that hospitalization was predicted by being female and/or transgender, the level of perceived social support, self-reported mental health, and having three or more chronic health conditions, whereas having a higher education was associated with lower rates of hospitalization (Gadermann et al., 2020).
In the study conducted by Gabet et al., (2019) researchers did not find a connection between housing type and hospitalization rates. However, the study conducted by Gadermann et al., (2020) showed that residential moves are associated with higher risk of hospitalization. Why do you think the type of housing may be less important than the number of places a person has lived, as a risk factor for subsequent hospital usage? What might the risk associated with residential instability tell us about having secure housing as a key social determinant of health?
We encourage you to consider these questions as you watch the next video of Dr. Naomi Nichols, who is a Tier II Canada Research Chair in Community-Partnered Social Justice Research at Trent University. She reflects upon youth and how – while we may often say homelessness leads to poor health – we must also recognize the ways constantly having to work to obtain health care can be destabilizing to one’s housing. Here, Dr. Nichols explains further.
In this video, Dr. Naomi Nichols reflects on research her team has conducted in Quebec, on how public sector institutions operate in relation to youth homelessness. She notes that in many ways these institutions are not preventing homelessness, but actively contributing to young people’s housing instability. She argues that the health care system is one example, where young people do relentless and unremitting work seeking access to care, which can have a destabilizing effect on their lives. While we often hear that homelessness leads to poor health, Dr. Nichols argues that it is more complex in that a lack of access to timely and sufficient health care can also be a driver of homelessness. In the absence of this care, young people may turn to emergency rooms, where even despite multiple visits they receive only treatment but not ongoing coordination of care. This video is 3:24 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: The impact of uncoordinated medical services on youth
Researchers leading the “At-Risk Youth Study” in Vancouver also examined hospitalization and homelessness with a focus on the experiences of young people (Chang et al., 2018). They found that of the 1,216 study participants, 31% reported having been hospitalized within 6 months prior to being surveyed and that the reasons were primarily for mental illness, physical trauma, and drug-related issues (Chang et al., 2018). This study again shows that not every person who experiences homelessness uses hospital services at a high rate but that when people do, it is for legitimate medical reasons that often have been left untreated to the point where they have reached a crisis level situation.
We have seen throughout the chapter on Primary Care & Nursing that people who experience homelessness often have chronic health conditions and that they may be faced with premature aging. Those who seek emergency medical services do not do so frivolously, but because they lack equitable access to primary care. That raises an interesting question then – if studies consistently show a large percentage of people experiencing homelessness do not go to the hospital, is it because they do not need medical care? Recall for instance our study which showed that 46% of participants had not been to the hospital in the preceding year (Gilmer & Buccieri, 2020) and the At-Risk Youth Study which showed 69% of young people had not been to the hospital in the preceding 6 months (Chang et al., 2018). Is it the case that these individuals did not require medical care?
While it is possible that some were not in need of emergency care, or had primary care they could access, it is likely that at least some of these individuals needed medical care but avoided going to the hospital. When people who experience homelessness go to the hospital, they often report perceived stigma and discrimination against them. Purkey and MacKenzie (2019) have noted that some people have positive experiences in hospitals, but that many individuals who experience homelessness, particularly if using substances, feel the health care system is designed for middle-class populations and not accountable or flexible enough to meet their needs. Mainstream health care services may not always feel welcoming and inclusive to individuals with specialized needs. In the next video Dr. Alex Abramovich speaks about the use of emergency health care amongst LGBTQ2S+ people and notes that for transgender individuals, in particular, hospital care may be used only when no alternatives exist.
In this video, Dr. Alex Abramovich discusses the complexity of emergency health care use amongst LGBTQ2S+ individuals. He notes that many people within this population have had negative encounters in health care settings and lack access to comfortable, safe, and affirming primary care. Research on LGBTQ2S+ health care can be challenging, as administrative health data generally records sex using binary categories. Dr. Abramovich notes that in research he is leading, the analysis of speciality clinic administrative data identified 2,000 transgender individuals. Although not focused on homelessness, this study did show alarmingly high rates of emergency department use amongst this group, for mental health and suicidality. Dr. Abramovich argues that many people within the LGBTQ2S+ population will avoid health care settings and seek hospital care only when a crisis arises. This video is 3:21 in length and has closed captions available in English.
Key Takeaways – Dr. Alex Abramovich: Do people who experience homelessness use emergency medical services at a high rate?
For populations who require specialized care, such as LGBTQ2S+ persons and/or individuals experiencing homelessness, accessing emergency departments may indicate a lack of primary care options that have resulted in crisis level support needs. Despite the goal of universally accessible patient-centred care, mainstream health care services can be felt as stigmatizing and shaming for patients experiencing homelessness, which may lead them to avoid or abandon seeking treatments they need (Purkey & MacKenzie, 2019).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=783#h5p-100
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=783#h5p-101
People who have concurrent disorders – mental illness and addictions issues – use emergency departments at comparatively higher rates than those without (Zhang et al., 2018) but they may not be well served by mainstream health care services, including primary and emergency sectors. Stigmatization against these and other marginalized patients is an issue across emergency response services, which can negatively affect their quality of care (Alunni-Menichini, Bertrand, Roy, & Brousselle, 2020). Zhang et al., (2018) have suggested that comprehensive programs, such as those that integrate mental health and addiction services with primary care and community-based outreach may better address these individual’s unmet health needs and improve their health outcomes.
Emergency response outreach is an approach that brings hospital personnel and other emergency workers directly into the community to meet individuals with complex needs where they are. The two videos below demonstrate examples of emergency outreach programs, such as through the Ottawa Hospital and Vancouver paramedic bike program. People who experience homelessness have higher rates of emergency department use and are frequent users of public ambulatory health services (Gentil, Grenier, Bamvita, & Fleury, 2020). A study of people who call EMS services, such as ambulance, frequently showed that they are often experiencing structural barriers like poverty and food insecurity at higher rates than the general population average (Agarwal et al., 2019). Bringing emergency response systems to the community may increase their accessibility and also has the potential to increase the time emergency health workers spend with these individuals. Research has shown that Canadian paramedic students report generally positive attitudes about working with people experiencing homelessness, but that their interest and confidence in treating this population decreases between pre- and post- placement in the field (Cochrane et al., 2019). As you watch the videos below, we encourage you to think about how programs such as these have an important role to play in bringing emergency medical services out into the community.
Emergency response is an important part of care for people experiencing homelessness, particularly if a person’s life is at risk (Alunni-Menichini et al., 2020). As we have seen in the previous videos, outreach is one way that emergency services can connect with marginalized patients and offer them specialized supports that they may not otherwise receive. However, while these programs are critically important, they do not negate the need to fix the problems in the mainstream health care system that make it discriminatory and inaccessible for some members of the community. Outreach is good, but we must also work to make hospitals and other health care settings more welcoming and inclusive spaces for treating the specialized needs of people experiencing homelessness.
We began this section by highlighting the simplicity of the question – do people experiencing homelessness use emergency medical services at a high rate? The responses and the research are clear that indeed homelessness often is associated with higher use of emergency medical services. However, the responses do not end there. We have seen throughout, the “but” that follows this answer. Yes, people who experience homelessness use emergency medical services at higher rates, but:
Thus, while we began with a very simple question, we ended up with a rather complicated answer. We have seen throughout this section that when people who experience homelessness do use emergency medical services they often report feeling that the services are not designed for them. They may face discrimination and stigma, particularly if they are seeking care for mental illness, substance use issues, and/or transgender care. Emergency medical outreach services, such as those profiled in Ottawa and Vancouver, offer supports that are more accessible by meeting people where they are in the community. However, as we have stated repeatedly, people who experience homelessness do not have equitable access to health care. We must ensure that all health care systems – whether primary or emergency – are accessible and inviting for all patients who walk through the door.
Click the link below to listen to all of the researchers answer the question “Do people who experience homelessness use emergency medical services at a high rate?” in audio format on our podcast!
116
People who go to the hospital may visit the emergency department, receive treatment, and leave, or they may be admitted for longer term care. Admissions to hospital may be brief, such as for 24 hours, or they may be on-going over several days, weeks, or even months. The duration of the stay is often dependent on the nature of the condition and treatment that is needed. In the previous section we examined the use of emergency medical services among people experiencing homelessness and saw that while some individuals use these ambulatory services and emergency departments at a high rate, it is generally because of complex health issues.
After a period of time spent in the hospital, patients undergo a discharge process. In this section, we set out to learn more about what happens after patients experiencing homelessness are discharged from hospital. Before continuing through the material of this section, we invite you to pause and reflect upon this. Where do people go after leaving the hospital? How well can they manage the follow-up care instructions? What happens if they are unable to maintain their treatment plan on their own? You may use the space below to record your thoughts.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=785#h5p-99
Discharge is a standard part of hospital administration that is guided by a set of protocols. Generally, a dedicated discharge planner, such as a Nurse or Social Worker, will meet with patients as they are preparing to leave the hospital. They will review the treatment plans and ensure the patient has information such as how to care for a wound, change their dressings, take the appropriate prescribed medication, and when to return for follow-up visits. For many patients, being discharged is a welcome process, as it indicates they are able to return home and continue their recovery in a setting that is more familiar. However, when a patient enters the hospital already experiencing homelessness – or loses their housing during their hospital stay – the process of discharge becomes more complicated.
We begin this section by looking at standard discharge practices, with a brief video from Sunnybrook Hospital in Toronto. This video is presented here to highlight how discharge unfolds for patients within the general population, who are housed. As you watch this video, we encourage you to take note of any issues that might arise for a patient if they were experiencing homelessness. Following this video, we present an activity in which we critically examine a standard instructional discharge paragraph, and highlight the areas where homelessness requires additional considerations.
Click the forward arrow to view all 14 slides of the presentation below.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=785#h5p-54
The case study presented above is just one demonstration of how hospital discharge protocols are complicated within the context of homelessness. When we consider the question, “What happens after patients who are experiencing homelessness are discharged from hospital?” we see that there are actually many things that occur. One of these is that we must consider where they go after they are released. When patients are admitted to hospital, they are asked to provide their contact information, including a home address. Sometimes people who are experiencing homelessness will provide a former address, the address of a shelter, or give no fixed address. As most patients are discharged “home,” the first problem that arises is a lack of anywhere to go upon release. Dr. Bill O’Grady explains further in the video that follows.
In this video Dr. William [Bill] O’Grady argues that more specialized education is needed for police and emergency room workers, who regularly interact with people experiencing homelessness. He notes that due to a lack of primary care, when people experiencing homelessness are injured, they often go to the emergency room for treatment. Prior to discharge, Dr. O’Grady says it is important that hospital workers ask these patients where they are going to go. In some cities, he notes, this work is formalized with a social worker located in the hospital specifically to assist these patients find housing. This video is 1:15 in length and has closed captions available in English.
Key Takeaways – Dr. Bill O’Grady: The need for improved hospital discharge practices
In the best-case scenario, hospitals have people on staff who are able to follow the progress of patients experiencing homelessness, from the time they are admitted until they are discharged into secure housing. However, this best-case scenario is not the norm. Researchers in Metro Vancouver, for instance, conducted in-depth interviews with 40 housing and health care providers for older people experiencing homelessness and found they are often discharged to inappropriate locations, such as shelters, because of a lack of better options (Canham et al., 2018). The widespread lack of affordable housing stock across Canada means that people have limited options for where to go after they are released from hospital.
This section’s featured reading, entitled, “Nowhere to go: Exploring the social and economic influences on discharging people experiencing homelessness to appropriate destinations in Toronto, Canada” takes a look at the factors that create discharge pressures in both the health care and homelessness sectors. Researchers conducted semi-structured interviews with 33 key stakeholders, including hospital workers, shelter workers, researchers, policy advisors, and advocates working in homelessness and health care (Jenkinson, Strike, Hwang, & Di Ruggiero, 2021). They found that historical and contemporary socio-economic contexts, such as declining financial resources, have resulted in a culture of efficiency within hospital settings, that prioritize accountability measures and create pressure to discharge patients as soon as they are medically stable (Jenkinson et al., 2021). Conversely, many shelters have adopted exclusion and eligibility policies to block the admission of people exiting hospitals, under the premise that they are not adequately prepared to manage their advanced health care needs (Jenkinson et al., 2021). These conditions create tension, as patients are not permitted to remain in hospital, but have nowhere else to go once released. As you engage with the featured reading below, we encourage you to consider the question of whose responsibility it is (or should be) to help people experiencing homelessness obtain secure housing upon their release.
Jenkinson, J. I. R., Strike, C., Hwang, S. W. & Di Ruggiero, E. (2021). Nowhere to go: Exploring the social and economic influences on discharging people experiencing homelessness to appropriate destinations in Toronto, Canada. Can J Public Health 112, 992–1001.
Before you read this article, we asked you to consider whose responsibility it is (and should be) to secure post-discharge locations. If you have come to this chapter after reading others throughout the book, it will not surprise you our response is that it is the Federal government’s responsibility to ensure there is an adequate stock of safe, secure, and deeply affordable housing for people to access. As patients are discharged from hospital settings, they may experience a sense of disconnection and need for transitional supports (Mutschler, Lichtenstein, Kidd, & Davidson, 2019). We have seen throughout this book that people who experience homelessness are often isolated and lack strong social connections that can support recovery and wellness. Without these supports, patients experiencing homelessness may not only be discharged with nowhere to go, but they may be discharged with no one to help look after them. Dr. Naomi Nichols speaks about this in the video that follows.
In this video, Dr. Naomi Nichols argues that we create public systems that imagine the user is housed, and those who are unhoused face challenges when navigating systems that were not designed with them in mind. As an example, Dr. Nichols cites people who are on a waitlist for mental health services but do not have a phone to be contacted when their place becomes available. She further cites stories from youth of being in hospital following an overdose episode and being discharged in an incapacitated state, early in the morning, to a parking lot, because assumptions were made that a parent would pick them up without verifying their family situation. This video is 2:09 in length and has closed captions available in English.
Key Takeaways – Dr. Naomi Nichols: Discharging youth from the hospital to the parking lot
In the preceding video, Dr. Nichols explained that people face challenges when they have to navigate systems that were not designed with them in mind. We have seen this already, with the standard discharge protocols that assume a person is going to be discharged home, that they have transportation, they are able to ask questions and retain information, and that they have the security of someone to help look after their care. These assumptions are often not appropriate for patients experiencing homelessness. As the previous featured reading showed, the pressures to discharge and the lack of after care options are imbedded in social and economic factors. Dr. Tyler Frederick explains in the next video that people working within these systems are doing their best, but that they face pressures beyond their control.
In this video, Dr. Tyler Frederick reflects on improved service alignment, in which systems like housing and health care would work better together. In past approaches, the hope was people would go to an emergency shelter and be able to receive the supports they need to move on to the next phase of their life. However, Dr. Frederick notes that the reality is often that people are doing the best they can in systems that are not always well aligned. For instance, people working in hospitals may not want to discharge patients into shelters but lack knowledge on the alternatives. This video is 1:49 in length and has closed captions available in English.
Key Takeaways – Dr. Tyler Frederick: Exiting hospitals into shelters
Most patients who enter the hospital are housed. As such, interactions between hospital staff and the homelessness sector are not a regular part of day-to-day operations. It is when a patient who is experiencing homelessness is admitted, and subsequently discharged, that this lack of regular interaction becomes problematic. The health care and homelessness sectors operate separately in many communities, having different budgets, decision-makers, and policies than one another. This can create barriers, such as when a person who is experiencing homelessness is about to be discharged and they have nowhere to go and no one to assist them.
The degree to which health care and homelessness sectors work collaboratively does vary across different geographic areas, with some hospital and shelter staff coordinating services more effectively than others. However, Jenkinson, Strike, Hwang, and Di Ruggiero (2020) have found that there are legal considerations, such as pertaining to health information protection laws, that create barriers to the “circle of care” that exists within a hospital being expanded to include shelter workers outside it. Other studies have supported this finding. For instance, a national survey of 660 stakeholders working in homelessness and health care roles found that the three main challenges for discharging patients experiencing homelessness were related to communication, privacy, and systems pressures (Buccieri et al., 2019). Communication issues resulted as people in both sectors were uncertain whom to contact as Dr. Frederick, a co-investigator in this study, explained in the preceding video. Privacy issues arose as homelessness sector support workers sought to provide or receive information about shared clients but were prohibited from doing so by health information laws. Finally, systems pressures existed within hospitals and shelters which are both often at (or near) full capacity without available beds (Buccieri et al., 2019).
The results of the national survey showed that communities across the country are struggling to support patients experiencing homelessness who are being discharged from hospital (Buccieri et al., 2019). Researchers conducting this study gave participants a series of statements about hospital discharge for patients experiencing homelessness and asked them how much they agreed that the statements applied within their community on a scale of 0 (not at all) to 100 (applies completely). The results, presented below, show quite clear agreement across the country that hospital discharge for people experiencing homelessness is a problem that needs to be better addressed, that improving discharge procedures could reduce chronic homelessness, people are generally discharged to the street and not to supportive housing, that hospitals and homelessness sector agencies do not generally collaborate well, and that these patients are not discharged with plans that are well-adapted to their unique needs (Buccieri et al., 2019).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=785#h5p-55
On a scale of 0 – 100, how much do you agree with the following statements within your own community? | Mean | Median | Mode
| |
1. | Hospital discharge planning for patients experiencing homelessness is an issue that needs to be better addressed in my community. | 92.88 | 100 | 100 |
2. | Improving hospital discharge planning could help reduce chronic homelessness. | 82.98 | 100 | 100 |
3. | People experiencing homelessness are usually discharged from hospitals to the streets or a shelter. | 82.67 | 91 | 100 |
4. | Hospitals and homelessness sector agencies work well together to coordinate care. | 24.33 | 20 | 0 |
5. | People experiencing homelessness are usually discharged from hospitals with treatment plans that are clear and easy to follow. | 17.56 | 10 | 0 |
6. | People experiencing homelessness are usually discharged from hospitals into supportive housing. | 11.09 | 4 | 0 |
When patients are discharged from hospital, prematurely or without the proper medical and social supports in place, the risk of being readmitted grows higher. Indeed, this is what we commonly see when people are discharged while experiencing homelessness. For instance, a review of records for all patients discharged from psychiatric hospitalization in Ontario between April 1st2011 and March 31st2014 indicated that patients who were experiencing homelessness at the time of discharge were more likely to be readmitted within 30 days and to have a subsequent emergency department visit, compared to housed patients (Laliberté, Stergiopoulos, Jacob, & Kurdyak, 2019).
Why do you think people who are experiencing homelessness at the time of discharge have higher rates of readmission and emergency department visits? What could be done to improve these patient’s post-hospitalization outcomes?
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=785#h5p-103
The analogy of a revolving door is perhaps cliché, but also accurate in this situation. There are many reasons that people who experience homelessness return to hospital after discharge. As we have seen, they may not have anywhere to go and end up (best-case scenario) in a shelter or (worst-case scenario) on the street. They may also be discharged on their own, without the support of a person to pick them up or offer them assistance while they are recovering. At the same time, there are structural issues like a lack of communication, privacy issues, and systems pressures that get in the way of coordinated care. All of this creates the conditions for poor health outcomes.
These are all social determinants that give rise to medical complications. You may recall the study by Wolfstadt et al., (2019) that showed marginalized patients may be more likely to have complications following surgery. Consider a situation in which a person is discharged without housing and the local shelter is full or says it cannot accommodate them due to their medical needs. How well do you think that person will be able to follow post-discharge instructions, like changing surgical dressings, while sleeping in a tent under a highway overpass? How will they obtain the medical supplies needed to care for their wound? How hygienic do you think these conditions would be?
Environmental factors are just one reason post-discharge complications arise. People who experience homelessness often do not have adequate follow-up care. In the study about surgical referrals, Zuccaro et al., (2018) found that just under half (49%) of referred patients attended at least one outpatient appointment, and that only 34% were able to complete their full follow-up protocol. Likewise, Alunni-Menichini et al., (2020) have written that the lack of continuity complicates emergency response professionals’ ability to make referrals even more than issues related to coordination. The lack of post-discharge follow-up care results for many reasons. Health care providers may not have contact information needed to inform a patient about an upcoming appointment and if they do, the person may not have transportation to get there. It is also challenging to keep track of appointments when one lacks reminders, such as a wallet card, note on the fridge, or entry into a smartphone calendar. These missed appointments are another reason why medical complications arise, and post-discharge readmissions are more common.
As part of their treatment plans, while admitted and post-discharge, patients may be prescribed medication. Richler, Yousaf, Hwang, and Dewhurst (2019) have found that among vulnerably housed patients admitted to an internal medicine service of a tertiary care, inner-city hospital, the responses to medication were generally positive but that study participants also expressed concern about adverse side effects. While patients are admitted to hospital, they are under the care of a team who ensures they receive the required medication in the correct dose and on the appropriate schedule. However, after they are released, patients are expected to manage their own medication. Again, this is challenging for patients experiencing homelessness. From a practical standpoint, they may not have the money to afford medication, may lack a space to store them (particularly if refrigeration is needed), or they may forget to take them while trying to meet other basic needs like obtaining food (the lack of which can also cause complications with medication). Remembering to take medication may also be more challenging for people who also have mental illness and/or substance use issues.
Researchers who conducted interviews with 129 people experiencing homelessness who were admitted to hospital found that 27% were readmitted again following their discharge (Wang et al., 2021). They wanted to identify the reasons this occurred and found that being prescribed a higher number of medications at the time of discharge was associated with higher odds of being readmitted (Wang et al., 2021). Given the challenges of managing medication while experiencing homelessness, it makes perfect sense that the more medications a person is prescribed, the greater their chances of having complications arise. However, in this same study Wang et al., (2021) looked at factors that reduced the risks of readmission. They found that having an active case manager, having informal support such as friends or family, and sending a copy of the patient’s discharge plan to a primary care physician who had cared for that patient within the preceding year were all associated with lower readmission rates (Wang et al., 2021).
According to Canham et al., (2019), coordinating hospital discharge should begin right from the time of admission, so that a person’s needs can be identified, and planning can begin. In an article that summarizes the findings from their scoping review, these authors write, “Patients would benefit from increased collaboration between healthcare and shelter/housing service providers during this transition because the identified health needs may potentially be met by either sector depending on what the need is and where the patient is within the transition. Hospital and shelter/housing service providers should increasingly mandate shared accountability for the transition of persons who are experiencing homelessness from hospital to increase the likelihood that patients’ needs are identified and supported during this challenging time” (Canham et al., 2019, pg.542).
What a patient needs will vary depending on the individual, making person-centered care critically important. For some people, such as those experiencing homelessness with complex health problems and high service use, on-going case management, harm reduction services, and housing might be the most beneficial post-discharge supports (Fleury, Grenier, Cao, & Meng, 2021). For others time-limited case management may promote continuity of care through low-barrier access, connection to community supports, individualized services, and effective coordination (Lamanna et al., 2018). Further tailored approaches may involve critical time interventions, which have shown statistically significant changes in health care utilization, including inpatient and outpatient services, for people experiencing homelessness in Ontario (Reid et al., 2021).
Increasingly, novel programs have begun to emerge that address discharge planning for people experiencing homelessness by connecting patients with housing supports while they are hospitalized, and then following up with them over a period of time to ensure they receive the wrap-around supports they need. One such example is the Bridge Healing Program in Edmonton that uses hospital emergency departments as a gateway to temporary housing, providing residents of the program with immediate short-term housing before transitioning them into longer-term permanent housing (Wong et al., 2020). This program is characterized as having a strong team, numerous services, connections to permanent housing, and a unique ability to reduce repeat emergency department visits, lengths of stay, and health care costs (Wong et al., 2020).
In Toronto, the Coordinated Access to Care for the Homeless (CATCH) program was implemented to determine the impacts this tailored service might have on frequent emergency department use (Stergiopoulos et al., 2016). The CATCH program is a brief multidisciplinary case management intervention for homeless adults discharged from hospital in Toronto, Canada. Funded in 2010 by the local health authority, CATCH aimed to improve access, continuity of care, and health and service use outcomes for adults experiencing homelessness who are discharged from hospital (Stergiopoulos et al., 2017). In total, 225 CATCH program users were enrolled in the study and completed quantitative survey measures at program entry to assess key health and social outcomes using a pre-post cohort study design. Follow-up assessments took place at 3- and 6-months (Stergiopoulos et al., 2017). In the pre-post analyses, CATCH participants showed statistically significant improvements in mental and physical health status and reductions in mental health symptoms, substance misuse, and the number of hospital admissions (Stergiopoulos et al., 2018).
Dr. Stephen Hwang is a general internist at St. Michael’s Hospital in Toronto, who has also worked on the CATCH program. In the video that follows, he speaks about the challenges of discharging people experiencing homelessness and about his new work with the Navigator Project, that supports patients from admission, through discharge, and 90 days beyond.
In this video, Dr. Stephen Hwang reflects on his work as a General Internist at a hospital and explains that patients who experience homelessness sometimes have unique care challenges that hospital staff may not be accustomed to addressing. For instance, these patients leave against medical advice and are readmitted at higher rates than average. He notes that while well-intentioned, discharge and post-care plans for patients experiencing homelessness may not be well suited for very practical reasons, such as the need to keep track of appointments, have transportation, access medical supplies, engage in follow-up care in a shelter setting, and that patients may also have addictions or substance use issues. Dr. Hwang argues that hospital staff are kept busy with patients in the building and are less aware of what happens after a patient leaves. For this reason, his team has implemented a Navigator approach, in which a case manager meets an unhoused person at admission, develops a relationship, and follows-up for 90 days post-discharge to ensure they are receiving the supports they need. This video is 4:38 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: What happens after patients who are experiencing homelessness are discharged from hospital?
Want to learn more about this project?
Check out the website!
In this video, recorded at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk speaks about her team’s hospital discharge intervention in London, Ontario. She argues that while discharge from hospital can be the start of a person’s homelessness journey, with the right interventions, discharge can be the end. She explains that the London program brings together health, income, and homelessness sector supports to establish connections while the patient is in hospital, prior to their discharge. Dr. Forchuk cites the most recent evidence from the program, which indicates that over three-quarters of the people exited psychiatric hospital programs into housing and after a year 90% were housed, because of their ongoing connections with community support programs. Dr. Forchuk notes that the success rate is lower with medical discharges due to generally shorter lengths of stay, but that in these instances making connections to the homelessness sector can produce longer-term opportunities. This video is 4:51 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: What happens after patients who are experiencing homelessness are discharged from hospital?
Want to learn more about this project?
Check out the CTV News coverage!
We began this chapter by looking at how standard hospital discharge protocols are designed with some key assumptions, about the patient’s access to housing, resources, and social support. However, when a person experiences homelessness their discharge may be complicated by the lack of these factors. We have seen throughout this chapter that people who experience homelessness often have complex health issues and that, while not all individuals use hospital emergency services at a high rate, there are some individuals who do require frequent visits and hospital admissions. People may enter the hospital already experiencing homelessness or they may become homeless through a loss of housing while they are admitted.
When people who are experiencing homelessness are discharged from hospital, they often have nowhere to go. Economic and social influences within hospitals create pressure to focus on efficiency and high turnover, leading to discharge as soon as the patient is medically stable. However, at the same time, shelters face strains from operating at capacity and not being able to care for people who have advanced medical needs. The lack of affordable housing across the country creates the worst-case scenario, in which people are discharged with nowhere to go. The high rates of social exclusion also mean that people who are discharged while experiencing homelessness may not have friends or family to assist them. Individual workers within hospitals and shelters often want to do what is best for these patients, but are limited by structural issues like communication challenges, patient privacy laws, and systems pressures. The results of a national survey showed that these struggles exist in communities across the country.
After discharge, people who experience homelessness are more likely than housed individuals to have medical complications and need to be readmitted. These complications may arise from a range of factors, such as the lack of a secure and hygienic place to tend to one’s wound care, addictions and/or mental health issues that make following a care plan more difficult, challenges with attending post-discharge appointments, and complications from accessing, storing, and taking medication. All of these factors can create barriers for people experiencing homelessness, resulting in higher rates of readmission to hospital.
While there are many issues identified in the research literature, there are also some novel programs that were identified. Notably, Dr. Stephen Hwang and Dr. Cheryl Forchuk spoke about their initiatives in Toronto and London respectively, that start planning for discharge when a patient is admitted and use the time of their hospitalization to connect them with housing and supports. After discharge, patients are then continually supported for a period of time to ensure they remain stably housed and medically well. These programs offer a new way of thinking about discharge processes that are tailored to the unique needs of people experiencing homelessness and offer long-term support beyond the walls of the hospital.
Click the link below to listen to all of the researchers answer the question “What happens after patients who are experiencing homelessness are discharged from hospital?” in audio format on our podcast!
117
In 2018 the Canadian Medical Association Journalpublished a brief commentary piece that was entitled, “Should health care dollars be used to house the homeless?” (Glauser, 2018). Since we ourselves like asking questions, we were intrigued. The article contains quotes and information from Dr. Mitchell Katz detailing a strategy in New York City that redirects public health funding into housing, resulting in lower health care spending because of lower demand. Dr. Stephen Hwang was cited in this article as saying that ending homelessness should be a goal, but that it is not something that we should do because it saves money. We wondered, would improved funding for affordable housing decrease the burden on hospitals? We posed this question to several researchers in the fields of medicine and housing, including Dr. Hwang, to see what they would have to say. Before we share their thoughts and what the research shows, we invite you to read the original article that sparked this discussion and record your own thoughts in the space below. What do you think – should we use health care dollars to house people and reduce the burden on hospitals?
First read the article, then record your thoughts below: Should health care dollars be used to house the homeless? (cmaj.ca)
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=787#h5p-104
Having safe, secure, and affordable housing is a key social determinant of health. For people to be well, they need to have a place where they can go to meet their basic needs, such as resting, eating, and bathing. Having housing is critical for good health. With this in mind, it makes sense that if we were to increase the amount of funding that went into developing affordable housing, more people would be housed and in better physical and mental health. We begin with a brief video of Dr. Cheryl Forchuk explaining the clear connection between housing and health.
In this video, filmed at a hospital during the COVID-19 pandemic, Dr. Cheryl Forchuk agrees that improved funding for housing and poverty would help offset health care costs because people who experience homelessness are vulnerable to a myriad of health issues. This video is 0:33 in length and has closed captions available in English.
Key Takeaways – Dr. Cheryl Forchuk: Would improved funding for affordable housing decrease the burden on hospitals?
Given there is a clear connection between one’s housing status and their health, why then do we not take health care dollars and reinvest them into developing housing? There is a simple and appealing kind of logic behind this way of thinking. Further, the commentary piece we began this section with showed that it can be an effective practice. Indeed, increased funding in housing could decrease hospital burdens but as with all questions in this book, the answer is never that simple. Dr. Abe Oudshoorn discusses the relationship between housing and health care in the next video and explains that the siloed way in which governments are structured creates financial restraints.
In this video, Dr. Abe Oudshoorn argues that there is a well-documented relationship between housing and health such as through simple connections, like housing quality, and through complex connections, like interconnected social determinants of health. He notes that to improve the relationship, investments would be needed in primary care access for this population and increasing the deeply affordable housing stock. However, Dr. Oudshoorn notes that while the economic return on investment is clear, the argument does not get much traction within governments because they are not set up to incentivize one Ministry to create savings for another. This video is 3:26 in length and has closed captions available in English.
Key Takeaways – Dr. Abe Oudshoorn: Would improved funding for affordable housing decrease the burden on hospitals?
In 2010 the United Kingdom introduced Social Impact Bonds as a new way to finance social service and health promotion programs, where investors would provide capital and then be reimbursed if the program met pre-set criteria for what was considered a successful outcome (Katz, Brisbois, Zerger, & Hwang, 2018). Katz et al., (2018) note that there are many areas of concern with this approach, including increased costs to governments, restricted program scope, fragmented policymaking, undermining of public-sector service provision, mischaracterization of the root causes of social problems, and entrenchment of systemically produced vulnerabilities. They further argue that it is essential to consider the long-term, aggregate, and contextualized effects of these social impact bonds (Katz et al., 2018). Different countries have approached the funding of health and social programs in various ways with very mixed results.
How should Canada fund health care and affordable housing development? The way governments are currently structured in Canada means that housing falls under one Ministry and health care falls under another. Dr. Oudshoorn noted that problems arise as Ministries are not incentivized to create cost savings for one another. Should governments implement incentives so that Ministries are rewarded in some way for creating savings in another?
Wiens et al., (2021b) conducted a study on the costs of health care services for adults with a history of homelessness, comparing those with and without mental illness. They found that 16% of the general cohort and 30% of those with mental illness were in the top 5% of health care users in Ontario, based on administrative data. The costs for these frequent health care users were largely attributed to emergency department and inpatient services, and people included in this group were characterized primarily as being female gender, having a regular medical doctor, using acute services in the preceding year, having poor perceived general health, and two or more diagnosed chronic conditions (Wiens et al., 2021b). We have seen throughout this chapter that indeed some people who experience homelessness are frequent users of health care services, with high costs attached.
In additional analysis, Wiens et al., (2021a) examined the relationship between this frequent health service usage and housing status in Ontario based on administrative health records. The findings indicated that as people get housed, their health care usage (and associated costs) initially increase but then decrease, suggesting that housing may reduce health care costs over time (Wiens et al., 2021a). However, another study conducted by Hinds et al. (2018) showed the opposite, that use of health care services initially declined after people went into public housing but then increased after a period of time. These studies show that for some people, being housed increases health care use initially and then reduces over time (Wiens et al., 2021a) and for others being housed decreases health care use initially and then increases over time (Hinds et al., 2018). Clearly, we need to learn more about the factors that lead to increased or decreased usage of health care services, to inform future decision-making. We invite you now to read the article, “Does housing improve health care utilization and costs?” authored by Wiens et al., (2021a) as this section’s featured reading.
Wiens, K., Nisenbaum, R., Sucha, E., Aubry, T., Farrell, S., Palepu, A., Duhoux, A., Gadermann, A., & Hwang, S. W. (2021a). Does housing improve health care utilization and costs? A longitudinal analysis of health administrative data link to a cohort of individuals with a history of homelessness. Medical Care, 59, S110-S116.
It may be that for some people, getting housed creates connections with supports that include access to health care providers. For others, getting housed may reduce their need for health care, as their health status starts to improve. There is much that we still need to learn about the connection between housing and access to health care services. In the chapter on Politics, Policy, & Housing in Canada we introduced Housing First, as a programmatic intervention that has become increasingly popular in Canada. Housing First is an approach that prioritizes getting people housed and then provides wrap-around services based on people’s self-identified needs. Housing First was initially evaluated as an intervention for people who had experienced chronic homelessness and also had a mental illness, through the multi-site “At Home / Chez Soi” study (Goering et al., 2014). One of the primary arguments in favour of Housing First has been that it helps improve people’s well-being and quality-of-life, while also being cost-effective.
In a review of the effectiveness of Housing First for individuals with mental illness, Kerman et al., (2020) used data over a 24-month period from a multi-site randomized controlled trial and found that Housing First was effective in securely housing frequent emergency department users despite their complex health needs. They also found that there were reductions in emergency department use and substance use problems, as well as improvements in mental health symptoms and community functions over the course of the study (Kerman et al., 2020). In the next video, Dr. Kelli Stajduhar discusses housing as a human right that improves people’s well-being, pointing to Housing First as one model that prioritizes people’s health in a non-judgemental way.
In this video, Dr. Kelli Stajduhar argues that housing is a fundamental right and that having affordable housing is necessary for a person to be in good health. She notes that many people who experience homelessness do not want to go to hospital, and will avoid going until necessary because it causes them to relive past traumas and discriminations they have had in institutional settings. Dr. Stajduhar concludes that there are good housing models in the world, such as Housing First, that prioritize health in a non-judgemental way. Living a stable life requires security of housing, which is a lesson we can learn from tent cities. In the absence of affordable housing, people will find ways to create a sense of community but people’s capacity to survive is not a substitute for providing them with affordable housing options. This video is 3:13 in length and has closed captions available in English.
Key Takeaways – Dr. Kelli Stajduhar: Would improved funding for affordable housing decrease the burden on hospitals?
Housing First has been widely adopted because of its core principles, which focus on client-centred practices like choice and harm reduction. However, there has also been interest in the financial implications of Housing First initiatives (Jadidzadeh, Falvo, & Dutton, 2020; Latimer et al., 2017). The question is asked – can we save money by housing people and providing them with supports? Data from the At Home / Chez Soi study indicated that the cost to provide housing and supports was as low as $14,496 annually per person (Latimer et al., 2019). The cost savings that can be achieved by housing people rather than funding emergency supports are certainly appealing from a government or funder perspective, but they do not tell the whole story about investments in Housing First. Dr. Tim Aubry was a lead researcher in the At Home / Chez Soi study. Here he discusses the balancing effect that we also must consider in relation to Housing First, and questions why we even need an economic argument to justify ending homelessness in Canada.
In this video, Dr. Tim Aubry explains that while there are some costs savings associated with programs like Housing First – particularly around reductions in service agency use, hospitalization and emergency medical service use, and correctional system involvement – the cost savings have likely been over-estimated. He argues that a small percentage of individuals use services at high rates but that many more use them at moderate rates or not at all. When services are provided to people through Housing First programs, there is a balancing effect where those who use services at high rates and those who previously did not use services meet in the middle. However, the bigger issue Dr. Aubry notes is that we as Canadians implement many expensive health interventions, such as for cancer and heart disease, without questioning the costs, yet we subject efforts to end homelessness to these kinds of financial analyses. He notes that the question should not be whether we will save money by housing people but rather, why do we have to come up with an economic business case to solve homelessness? This video is 4:37 in length and has closed captions available in English.
Key Takeaways – Dr. Tim Aubry: Would improved funding for affordable housing decrease the burden on hospitals?
Housing First is one intervention that has the potential for improving people’s health and decreasing health care usage, but we cannot assume it is a magic bullet solution. In the next video Political Studies professor Dr. Jonathan Greene reminds us that housing can lead to both increases and decreases in health care usage and that, while Housing First is important, we need to dig deeper to understand the nature of these complex relationships.
In this video, Dr. Jonathan Greene argues that connecting people with stable housing might reduce the costs of emergency medical service use, but that at the same time it could increase the use of on-going primary care. He cautions that we often get focused on finances but what we should be concerned with is finding out what individualized supports people need to remain securely housed. Dr. Greene notes that even in the At Home / Chez Soi study where Housing First was implemented with all the supports, some participants returned to homelessness. Rather than asking ourselves whether supports will save us money, he urges us to focus on investing in finding out which ones will work best. This video is 4:14 in length and has closed captions available in English.
Key Takeaways – Dr. Jonathan Greene: Would improved funding for affordable housing decrease the burden on hospitals?
Throughout this one chapter alone, we have cited 15 articles co-authored by Dr. Stephen Hwang, and this is just a fraction of what he has contributed to our knowledge about health and homelessness. As one of, if not the, leading researcher on the intersections between health care and homeless in the world, we were interested to know what Dr. Hwang would have to say about the question of increasing funding for housing to reduce the burden on hospitals. He raised many interesting points, echoing his statement in the commentary article we began this section with, that while ending homelessness is always the goal, we should do it because it is the right thing to do and not because it saves us money. Listen in as we speak with Dr. Hwang.
In this video, Dr. Stephen Hwang argues that the question of whether spending on housing would decrease health care costs is a contentious issue that needs to be unpacked. He notes that when people ask this question, they are doing so with the recognition that people who experience homelessness may be high users of health care. However, while this is true in some instances, Dr. Hwang encourages us to pause and consider the underlying assumption that says we should do things to save money. He argues that rather than worrying about saving money, we should provide housing because it is the right thing to do. As a parallel example, our society does not ask whether it would save money if we educated fewer people. We educate because it is the right thing to do, and we should also provide housing because it is the right thing to do. Dr. Hwang further makes a distinction between cost-savings and cost-offsets. Some programs, such as Housing First, have cost-offsets associated with decreased use of shelter and psychiatric beds but they are not cost-savings because we still spend money on housing. Dr. Hwang concludes with the observation that very little the health care system does is about saving money. Patients are treated for conditions such as diabetes and high blood pressure without concern over whether money will be saved by doing so. He challenges us to consider why we would expect the housing and homelessness sectors to save the health care system money, when it does not even do so itself. This video is 5:58 in length and has closed captions available in English.
Key Takeaways – Dr. Stephen Hwang: Would improved funding for affordable housing decrease the burden on hospitals?
At the start of this section, we presented a commentary piece published in the Canadian Medical Association Journal with the title, “Should health care dollars be used to house the homeless?” (Glauser, 2018). This article sparked our interest and led us to wonder whether increased investments in affordable housing could help reduce hospital usage. Should health care dollars be re-allocated to housing in order to offset the costs of frequent health care usage? We began this section with the unequivocal assertion that housing is a social determinant of health and that being securely housed is important for physical and mental well-being. However, we also asserted (as we so frequently do) that the answer requires further unpacking.
We saw that the way our government is organized means that there are no incentives for one Ministry to create cost-savings for another. This means that although spending more on housing may decrease people’s use of hospitals, there is no benefit for the housing sector to create this offset. The research shows that people who experience homelessness, particularly if diagnosed with a mental illness, are among the highest users of hospital health care. However, the research was also divided on whether housing created higher or lower health care usage initially and over time.
Housing First is a critically important intervention that operates on the premise that housing should be prioritized, and that people should be given wrap-around supports based on their identified needs. This approach has been widely adopted, in part because of its demonstrated cost-effectiveness. We learned from Dr. Aubry, one of the lead researchers on the At Home / Chez Soi study, that to understand Housing First we must consider the cost balances, rather than cost offsets. Housing First is helpful for many people experiencing homelessness but more than focusing on its costs, we need to focus on fine-tuning its effectiveness. We concluded this section by speaking with Dr. Hwang, who echoed the sentiments of all the researchers and argued that ending homelessness should be done because it is the right thing to do, not because it saves us money.
Click the link below to listen to all of the researchers answer the question “Would improved funding for housing decrease the burden on hospitals?” in audio format on our podcast!
118
Pia
We met Pia at the beginning of the chapter after her unsuccessful visit to the emergency room. Unfortunately, this experience is common for many folks experiencing homelessness, substance use challenges, and mental health challenges. We remind you, for instance, of the patient accounts you viewed previously in this chapter, like the young man who left the hospital after being scolded for bleeding on the floor. Think about the last time you had occasion to be in the emergency department, and the kind of care you received.
We need to ask ourselves:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=1194#h5p-87
119
We began this chapter by noting that people who experience homelessness often lack equitable access to primary health care, which can increase their reliance on emergency medical services. As housing is a key social determinant of health, we wanted to explore the relationship between homelessness, medical services, and hospital usage.
At the start of the chapter, we introduced you to the composite character Mia who visited the emergency department but did not receive the treatment she needed. This scenario was presented as an entry point into thinking about the complexity of homelessness and emergency medicine. We returned to her story again at the end to demonstrate how it can help us understand the foundational concepts of being trauma-informed, person-centred, socially inclusive, and situated within the social determinants of health as critical for understanding homelessness in Canada
We asked you to consider three questions along the way, with the guidance of leading homelessness researchers.
First we asked, “Do people who experience homelessness use emergency medical services at a high rate?” We noted that while this may seem like one of the simpler questions posed throughout this book, it is actually deceptively complex. In posing the question, we found that some (but not all) people who experience homelessness use emergency medical services at a higher rate than housed individuals. However, we also found that they do so because they lack equitable access to primary care and have multiple chronic health conditions. Use of emergency medical services may actually be a last resort for many individuals experiencing homelessness, particularly if transgender, living with mental illness, and/or if they have substance use issues, because of the stigma and discrimination they often face in these settings. As an alternative to hospital care, some emergency medical professionals engage in outreach to meet people in the community. This is no doubt a valuable service, but it does not negate the need to make our health care systems more accessible and equitable for all community members.
Next we asked, “What happens after patients who are experiencing homelessness are discharged from hospital?” This led us to consider what happens to people who are admitted to hospital once they are ready to leave. We found that standard discharge protocols are based on assumptions, such as that the patient has a place to recover, resources at their disposal including transportation, and someone who can care for them. Within the context of patients experiencing homelessness, a lack of housing and supportive relationships can be complicating factors. We learned that there are communication barriers, privacy laws, and systems pressures that make discharge a challenging issue across the country. Further, medical complications mean that many people who are discharged end up being readmitted to hospital within a short period of time. Fortunately, there are some unique programs that are operating to identify patients experiencing homelessness as they are admitted to hospital, and that help connect them with housing and continued supports after they are discharged. With more widespread uptake, these programs could have a real impact in helping people become housed and avoid future hospitalizations.
Finally, we asked, “Would improved funding for affordable housing decrease the burden on hospitals?” This question was prompted by a commentary piece discussing an initiative in New York City to divert public health dollars into housing initiatives. We found that there is a well documented link that shows housing is a key social determinant of health. The question of whether housing should be funded to reduce health care costs, however, was much more contentious. We found that the governmental structure in Canada creates barriers that de-incentivize Ministries from funding areas outside their mandate. We also saw that the research paints a complex picture, in that sometimes when people become housed they initially use less health care, and sometimes they use more. Further study is needed to understand the complexity of this relationship. While housing and health care are related, the exact mechanisms remain unclear. We concluded this section by considering Housing First as a critically important intervention that can have cost benefits but is better understood as having cost balances. In the end, whether housing has an impact on hospital usage, and its associated costs, is less important than focusing on the need to end homelessness because housing is a fundamental human right.
120
Here are some additional resources you may want to check out!
121
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
122
Agarwal, G., Lee, J., McLeod, B., Mahmuda, S., Howard, M., Cockrell, K., & Angeles, R. (2019). Social factors in frequent callers: A description of isolation, poverty and quality of life in those calling emergency medical services frequently. BMC Public Health, 19(1), 684.https://doi.org/10.1186/s12889-019-6964-1
Alunni-Menichini, K., Bertrand, K., Roy, L., & Brousselle, A. (2020). Current emergency response in Montreal: How does it fit in the services offered to homeless people who use substances? The International Journal of Drug Policy, 82, 102758–102758. https://doi.org/10.1016/j.drugpo.2020.102758
Buccieri, K., Oudshoorn, A., Frederick, T., Schiff, R., Abramovich, A., Gaetz, S. & Forchuk, C. (2019), Hospital discharge planning for Canadians experiencing homelessness. Housing, Care and Support, 22(1), 4-14. https://doi.org/10.1108/HCS-07-2018-0015
Canham, S., Davidson, S., Custodio, K., Mauboules, C., Good, C., Wister, A. V., & Bosma, H. (2018). Health needs of older homeless persons who are transitioning from hospital to shelter/housing. Innovation in Aging, 2(suppl_1), 56. https://doi.org/10.1093/geroni/igy023.209
Canham, S. L., Davidson, S., Custodio, K., Mauboules, C., Good, C., Wister, A. V., & Bosma, H. (2019). Health supports needed for homeless persons transitioning from hospitals. Health & Social Care in the Community, 27(3), 531–545. https://doi.org/10.1111/hsc.12599
Chang, D. C., Rieb, L., Nosova, E., Liu, Y., Kerr, T., & DeBeck, K. (2018). Hospitalization among street-involved youth who use illicit drugs in Vancouver, Canada: A longitudinal analysis. Harm Reduction Journal, 15(1), 14–14. https://doi.org/10.1186/s12954-018-0223-0
Cochrane, A., Pithia, P., Laird, E., Mifflin, K., Sonley-Long, V., & Batt, A. M. (2019). Investigating the attitudes of Canadian paramedic students towards homelessness. International Journal of Caring Sciences, 12(3), 1781–1787. https://doi.org/10.1101/19003483
Fleury, M. J., Grenier, G., Cao, Z., & Meng, X. (2021). Typology of currently or formerly homeless individuals based on their use of health and social services. Community Mental Health Journal, 57, 948-959. DOI: 10.1007/s10597-020-00693-6
Forchuk, C., Gyamfi, S., Martin, M. L., Corring, D., Srivastava, R., & Harerimana, B. (2021). Transitional discharge model for community mental health integration: A focused ethnographic study of clients’ perspectives. International Journal of Mental Health Nursing, 30(2), 553-562. https://doi.org/10.1111/inm.12821
Forchuk, C., Martin, M. L., Sherman, D., Corring, D., Srivastava, R., O’Regan, T., Gyamfi, S., & Harerimana, B. (2020). Healthcare professionals’ perceptions of the implementation of the transitional discharge model for community integration of psychiatric clients. International Journal of Mental Health Nursing, 29(3), 498-507. https://doi.org/10.1111/inm.12687
Gabet, M., Grenier, G., Cao, Z., & Fleury, M. J. (2019). Predictors of emergency department use among individuals with current or previous experience of homelessness. International Journal of Environmental Research and Public Health, 16(24), 4965. https://doi.org/10.3390/ijerph16244965
Gadermann, A. M., Karim, M. E., Norena, M., Emerson, S. D., Hubley, A. M., Russell, L. B., Nisenbaum, R., Hwang, S. W., Aubry, T., & Palepu, A. (2020). The association of residential instability and hospitalizations among homeless and vulnerably housed individuals: Results from a prospective cohort study. Journal of Urban Health, 97(2), 239–249. https://doi.org/10.1007/s11524-019-00406-9
Gentil, L., Grenier, G., Bamvita, J. M., & Fleury, M. (2020). Satisfaction with health and community services among homeless and formerly homeless individuals in Quebec, Canada. Health & Social Care in the Community, 28(1), 22–33. https://doi.org/10.1111/hsc.12834
Gilmer, C., & Buccieri, K. (2020). Homeless patients associate clinician bias with suboptimal care for mental illness, addictions, and chronic pain. Journal of Primary Care & Community Health, 11. https://doi.org/10.1177/2150132720910289
Glauser, W. (2018). Should health care dollars be used to house the homeless? Canadian Medical Association Journal (CMAJ), 190(43), E1291–E1292. https://doi.org/10.1503/cmaj.109-5671
Goering, P., Veldhuizen, S., Watson, A., Adair, C., Kopp, B., Latimer, E., Nelson, G., MacNaughton, E., Streiner, D., & Aubry, T. (2014). National at home / chez soi final report. Calgary, AB: Mental Health Commission of Canada. National At Home/Chez Soi Final Report | The Homeless Hub
Hinds, A. M., Bechtel, B., Distasio, J., Roos, L. L., & Lix, L. M. (2018). Changes in healthcare use among individuals who move into public housing: a population-based investigation. BMC Health Services Research, 18(1), 411–411. https://doi.org/10.1186/s12913-018-3109-7
Jadidzadeh, A., Falvo, N., & Dutton, D. J. (2020). Cost savings of Housing First in a non-experimental setting. Canadian Public Policy, 46(1), 23–36. https://doi.org/10.3138/cpp.2019-017
Jenkinson, J. I. R., Strike, C., Hwang, S. W., & Di Ruggiero, E. (2020). Legal, geographic and organizational contexts that shape knowledge sharing in the hospital discharge process for people experiencing homelessness in Toronto, Canada. Health & Social Care in the Community. Early View. https://doi.org/10.1111/hsc.13206
Jenkinson, J. I. R., Strike, C., Hwang, S. W. & Di Ruggiero, E. (2021). Nowhere to go: Exploring the social and economic influences on discharging people experiencing homelessness to appropriate destinations in Toronto, Canada. Canadian Journal of Public Health, 112, 992–1001. https://doi.org/10.17269/s41997-021-00561-0
Katz, A. S., Brisbois, B., Zerger, S., & Hwang, S. W. (2018). Social impact bonds as a funding method for health and social programs: Potential areas of concern. American Journal of Public Health, 108(2), 210–215. https://doi.org/10.2105/AJPH.2017.304157
Kerman, N., Aubry, T., Adair, C. E., Distasio, J, Latimer, E., Somers, J., & Stergiopoulos, V. (2020). Effectiveness of housing first for homeless adults with mental illness who frequently use emergency departments in a multisite randomized controlled trial. Administration and Policy in Mental Health Services Research, 47, 515-525. https://doi.org/10.1007/s10488-020-01008-3
Laliberté, V., Stergiopoulos, V., Jacob, B., & Kurdyak, P. (2019). Homelessness at discharge and its impact on psychiatric readmission and physician follow-up: a population-based cohort study. Epidemiology and Psychiatric Sciences, 29, e21–e21. https://doi.org/10.1017/S2045796019000052
Lamanna, D., Stergiopoulos, V., Durbin, J., O’Campo, P., Poremski, D., & Tepper, J. (2018). Promoting continuity of care for homeless adults with unmet health needs: The role of brief interventions. Health & Social Care in the Community, 26(1), 56–64. https://doi.org/10.1111/hsc.12461
Latimer, E. A., Rabouin, D., Cao, Z., Ly, A., Powell, G., Adair, C. E., … Veldhuizen, S. R. (2019). Cost-effectiveness of Housing First Intervention With Intensive Case Management Compared With Treatment as Usual for Homeless Adults With Mental Illness: Secondary Analysis of a Randomized Clinical Trial. JAMA Network Open, 2(8), e199782–e199782. https://doi.org/10.1001/jamanetworkopen.2019.9782
Latimer, E. A., Rabouin, D., Cao, Z., Ly, A., Powell, G., Aubry, T., Hwang, S. W.,… Goering, P. N. (2017). Costs of services for homeless people with mental illness in 5 Canadian cities: a large prospective follow-up study. CMAJ Open, 5(3), E576–E585. https://doi.org/10.9778/cmajo.20170018
Mutschler, C., Lichtenstein, S., Kidd, S.A. & Davidson, L. (2019). Transition experiences following psychiatric hospitalization: A systematic review of the literature. Community Mental Health Journal, 55, 1255–1274. https://doi.org/10.1007/s10597-019-00413-9
Purkey, E., & MacKenzie, M. (2019). Experience of healthcare among the homeless and vulnerably housed a qualitative study: opportunities for equity-oriented health care. International Journal for Equity in Health, 18(1), 101–101. https://doi.org/10.1186/s12939-019-1004-4
Reid, N., Mason, J., Kurdyak, P., Nisenbaum, R., de Oliveira, C., Hwang, S., & Stergiopoulos, V. (2021). Evaluating the impact of a critical time intervention adaptation on health care utilization among homeless adults with mental health needs in a large urban center. Journal of Psychiatry. https://doi.org/10.1177/0706743721996114
Richard, L., Booth, R., Rayner, J., Clemens, K. K., Forchuk, C., & Shariff, S. Z. (2021). Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: A retrospective cohort study. CMAJ Open, 9(1), E1–E9. https://doi.org/10.9778/cmajo.20200287
Richler, M. J., Yousaf, S., Hwang, S. W., & Dewhurst, N. F. (2019). Descriptive study of homeless patients’ perceptions that affect medication adherence. American Journal of Health-System Pharmacy, 76(17), 1288–1295. https://doi.org/10.1093/ajhp/zxz139
Stergiopoulos, V., Gozdzik, A., Nisenbaum, R., Durbin, J., Hwang, S. W., O’Campo, P., … Wasylenki, D. (2018). Bridging hospital and community care for homeless adults with mental health needs: Outcomes of a brief interdisciplinary intervention. Canadian Journal of Psychiatry, 63(11), 774–784. https://doi.org/10.1177/0706743718772539
Stergiopoulos, V., Gozdzik, A., Nisenbaum, R., Lamanna, D., Hwang, S. W., Tepper, J., & Wasylenki, D. (2017). Integrating hospital and community care for homeless people with unmet mental health needs: Program rationale, study protocol and sample description of a brief multidisciplinary case management intervention. International Journal of Mental Health and Addiction, 15(2), 362–378. https://doi.org/10.1007/s11469-017-9731-5
Stergiopoulos, V., Gozdzik, A., Tan de Bibiana, J., Guimond, T., Hwang, S. W., Wasylenki, D. A., & Leszcz, M. (2016). Brief case management versus usual care for frequent users of emergency departments: The coordinated access to care from hospital emergency departments (CATCH-ED) randomized controlled trial. BMC Health Services Research, 16(1), 432–432. https://doi.org/10.1186/s12913-016-1666-1
Strobel, S., Burcul, I., Dai, J. H., Ma, Z., Jamani, S., & Hossain, R. (2021). Characterizing people experiencing homelessness and trends in homelessness using population-level emergency department visit data in Ontario, Canada. Ottawa: Statistics Canada, Health Reports.
Vogel, M., Frank, A., Choi, F., Strehlau, V., Nikoo, N., Nikoo, M., … Schütz, C. G. (2017). Chronic pain among homeless persons with mental illness. Pain Medicine, 18(12), 2280–2288. https://doi.org/10.1093/pm/pnw324
Wang, A., Pridham, K.F., Nisenbaum, R., Pedersen, C., Brown, R., & Hwang, S. W. (2021). Factors associated with readmission among general internal medicine patients experiencing homelessness. Journal of General Internal Medicine, 36, 1944–1950. https://doi.org/10.1007/s11606-020-06483-w
Wiens, K., Nisenbaum, R., Sucha, E., Aubry, T., Farrell, S., Palepu, A., Duhoux, A., Gadermann, A., & Hwang, S. W. (2021a). Does housing improve health care utilization and costs? A longitudinal analysis of health administrative data link to a cohort of individuals with a history of homelessness. Medical Care, 59, S110-S116. 10.1097/MLR.0000000000001379
Wiens, K., Rosella, L.C., Kurdyak, P., Chen, S., Aubry, T., Stergiopoulos, V., & Hwang, S. W. (2021b). Factors associated with higher healthcare costs in a cohort of homeless adults with a mental illness and a general cohort of adults with a history of homelessness. BMC Health Serv Res, 21, 555. https://doi.org/10.1186/s12913-021-06562-6
Wiens, K., Rosella, L. C., Kurdyak, P., & Hwang, S. W. (2020). Patterns and predictors of high-cost users of the health system: A data linkage protocol to combine a cohort study and randomised controlled trial of adults with a history of homelessness. BMJ Open, 10(12), e039966–e039966. https://doi.org/10.1136/bmjopen-2020-039966
Wolfstadt, J. I., Pincus, D., Kreder, H. J., & Wasserstein, D. (2019). Association between socioeconomic deprivation and surgical complications in adults undergoing ankle fracture fixation: A population-based analysis. Canadian Journal of Surgery, 62(5), 320–327. https://doi.org/10.1503/cjs.012018
Wong, A., Chen, J., Dicipulo, R., Weiss, D., Sleet, D. A., & Francescutti, L. H. (2020). Combatting homelessness in Canada: Applying lessons learned from six tiny villages to the Edmonton bridge healing program. International Journal of Environmental Research and Public Health, 17(17), 6279–. https://doi.org/10.3390/ijerph17176279
Zhang, L., Norena, M., Gadermann, A., Hubley, A., Russell, L., Aubry, T., To, M. J., Farrell, S., Hwang, S. W., & Palepu, A. (2018). Concurrent disorders and health care utilization among homeless and vulnerably housed persons in Canada. Journal of Dual Diagnosis, 14(1), 21–31. https://doi.org/10.1080/15504263.2017.1392055
Zuccaro, L., Champion, C., Bennett, S., & Ying, Y. (2018). Understanding the surgical care needs and use of outpatient surgical care services among homeless patients at the Ottawa Hospital. Canadian Journal of Surgery, 61(6), 424–429. https://doi.org/10.1503/cjs.001317
XII
As we set out to review the literature, conduct researcher interviews, and ultimately produce this book, we gave ourselves a task – to explore seemingly simple questions that have complex answers. With this mission in mind, we have saved the best for last. Here we have come to the point where we reflect on everything we have learned and consider the next steps in moving forward. Homelessness is a difficult topic, and it may feel like there is little we can do about it. As you read the chapters of this book, you may have found yourself struggling with a sense of being overwhelmed. With all of the issues that people who experience homelessness face, what could we as a society possibly do to make this situation better?
Throughout this book we have incorporated quotes from research we previously conducted. One of the questions we asked people in this research was what they would fix about homelessness in their community if they had a magic wand. This seems like a good question for us to pose here as well. Imagine that as you sit reading this Conclusion, having learned all about homelessness in Canada, you are given a magic wand. How would you use it to solve the social problem of homelessness? We began this book with a game, and so we end here with one as well.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=671#h5p-113
As you continue through the Conclusion, we encourage you to keep the magic wand in your pocket. While we may not be able to wave a wand and fix these complex issues so easily, it is a good reminder that we all have more power than we realize.
123
We hope that you have enjoyed learning about homelessness throughout the different chapters and sections of this book, and that it has broadened your understandings and perspectives. In this concluding chapter, we invite you to consider one last question along with us, which guides our final learning objectives.
As you move through this chapter it is beneficial to keep in mind that homelessness is a social issue that impacts our society as a whole. If we conclude that we can end homelessness, and we know how, then we have to ask, “Why don’t we end homelessness?” and “Why haven’t we ended homelessness already?”
124
This chapter is structured slightly differently than those that came before. The researchers who participated in this project were asked a selection of questions that pertained to their particular field of study. You have seen those videos presented throughout the various chapters in this book. When it came to the last question, “Can we end homelessness? How?” we felt it was important each person be able to respond. This concluding chapter is structured around those 26 responses. Although there is considerable agreement among the researchers we spoke to, we present them here in four categories, to highlight the key priorities that emerged, which are important to note.
125
You will likely notice in the video segments that follow, that we often prefaced this question by calling it “the big one.” After the camera stopped recording in one interview, the conversation continued as one researcher raised an interesting query about whether people’s responses might differ depending on the stage of their career. Would people who are newer to the field have more optimism or see the hurdles as insurmountable? Would people who are more established in their career feel compassion fatigue (you remember that from the Social Work chapter, right?), or would they be eager to build on the networks and connections they have developed? After seeing the collection of responses together, we can certainly attest that people at all stages of their career remained passionate about ending homelessness. Whether they felt we were on the right track as a country, is something we will let you explore for yourself.
Before you begin this concluding chapter, we encourage you one last time to consider the question before exploring the range of responses. After all that you have learned, what is your opinion? Can we end homelessness? If so, how? Use the space below to record your thoughts. You may write as little or as much as you wish to answer these questions.
How to complete this activity and save your work: Type your response to the question in the box below. When you are done answering the question navigate to the ‘Export’ page to download and save your response. If you prefer to work in a Word document offline you can skip right to the Export section and download a Word document with this question there.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://ecampusontario.pressbooks.pub/homelessness/?p=680#h5p-105
Homelessness is a complicated issue. However, when we asked the researchers the final question about whether we can end it, and if so how, the answers were surprisingly clear. Although they picked up on different themes or said things in different ways, their responses collectively identified four key priorities that need to be addressed before we can end homelessness in Canada. These priority areas are overlapping and have to be implemented together to be effective. To end homelessness, we must: [1] recognize housing as a human right and create deeply affordable housing to ensure that right is met, [2] implement individualized choice-based supports following the Housing First principles to ensure people’s unique needs are met, [3] hold the government accountable for their social policy choices in the past, present, and future, and [4] prevent homelessness from occurring in the first place by implementing systemic change.
In this chapter, we explore each of these priority areas by focusing on the researchers’ responses. We would like to note that in writing this chapter and presenting the material, we made the choice of which theme to include each researcher in. This does not mean that they only argued for that priority, but rather that we felt they made a strong case for it in their response. As you will see, the researchers all provided thoughtful responses that spanned across many of the priority areas. The choice to assign them to one theme or another was ours. We invite you to join us in exploring each of these priority areas and seeing firsthand the responses we received to the questions: Can we end homelessness and, if so, how?
The idea that housing is a human right is a simple concept, but it had not been officially recognized in Canada until recently with the implementation of the National Housing Strategy (Government of Canada, 2017) and passing of the affiliated National Housing Strategy Act (Government of Canada, 2019). We have seen throughout this book that a lack of housing is a social determinant that is at the root of many challenges, traumas, and hardships associated with homelessness. Implementing the legislation and seeing housing realized as a human right in Canada will require thoughtful consideration; much of this work has already begun (Biss & Raza, 2021; CERA & NRHN, 2021; Porter, 2021; Schwan, Vaccaro, Redi, & Ali, 2021). What we heard from researchers is that we must stop thinking of housing as a commodity that generates wealth, and instead begin to invest in developing deeply affordable housing as a human right.
We have selected four researchers who included this priority in their discussion about ending homelessness in Canada. Here we invite you to watch the responses of Dr. Jonathan Greene, Dr. Naomi Nichols, Dr. Abe Oudshoorn, and Dr. Kaitlin Schwan. You may watch them, in any order you wish, by clicking on the images, which will open the videos in a new window. We encourage you to also review the key takeaways in the box that follows! As you watch the videos, try to keep the other priorities in your mind as well, to see if you can pick up on how they intersect with one another.
 |  |
 |  |
Key Takeaways – Greene, Nichols, Oudshoorn, and Schwan: Can we end homelessness? How?
Dr. Jonathan Greene:
Dr. Naomi Nichols:
Dr. Abe Oudshoorn:
Dr. Kaitlin Schwan:
Creating deeply affordable housing is an essential measure for ending homelessness, but we must also ensure people with complex needs have access to individualized supports grounded in Housing First principles, such as choice, social inclusion, cultural reflexivity, and anti-discriminatory practice. You may recall from the chapter Politics, Policy, and Housing in Canada, that Housing First is an effective approach that prioritizes getting people housed, without readiness requirements, and then offers wrap-around supports based on what clients themselves identify as needing (Aubry, 2020). Housing First was originally designed for adults with mental illness (Chung et al., 2018) but can be adapted, such as for youth (Gaetz, Walter, & Story, 2021), women (Oudshoorn, Forchuk, Hall, Smith-Carrier, & Van Berkum, 2018), Veterans (Forchuk, Richardson, Atyeo, & Serrato, 2021), and Indigenous persons (Distasio, Zell, & Snyder, 2018).
We have selected seven researchers to include within this priority theme because they each discussed the importance of Housing First and/or respecting the unique identities and support needs of individuals. Here we invite you to watch the responses of Dr. Katrina Milaney, Dr. Jeff Karabanow, Dr. Erin Dej, Dr. Alex Abramovich, Dr. Naomi Thulien, Dr. Rebecca Schiff, and Jessica Rumboldt. We would like to remind you that to view them you can simply click on the images which will open a new window. Be sure to read the key takeaways in the box that follows. As you watch, see if you can also identify the other three priorities throughout these videos as well.
 |  |
 |  |
 |  |
 |
Key Takeaways – Milaney, Karabanow, Dej, Abramovich, Thulien, Shiff, and Rumboldt: Can we end homelessness? How?
Dr. Katrina Milaney:
Dr. Jeff Karabanow:
Dr. Erin Dej:
Dr. Alex Abramovich:
Dr. Naomi Thulien:
Dr. Rebecca Schiff:
Jessica Rumboldt:
Over the past several years, there have been positive steps forward in federal policy for housing and homelessness. Notably, we have seen Canada’s National Housing Strategy (Government of Canada, 2017), National Homelessness Strategy (Government of Canada, 2018), and National Housing Strategy Act (Government of Canada, 2019). However, while these are promising initiatives, we cannot forget that the lack of affordable housing and current rates of mass homelessness have resulted from policy decisions made in the 1980s and 1990s. Governments must recognize that the choices they make, through the policies they implement, have a direct impact on homelessness rates in Canada. Governments at all levels [Federal, Provincial / Territorial, and Municipal] need to be held accountable to learn from the past, and from other nations, what measures reduce homelessness, and which do not.
Here we present videos from eight researchers who spoke about the role of the government in needing to have the will to change, learning from past decisions, and looking to other countries for guidance. Here we invite you to watch the responses of Dr. Jeannette Waegemakers Schiff, Dr. Jacqueline Kennelly, Dr. John Ecker, Dr. Nick Kerman, Dr. Nick Falvo, Dr. Stephen Hwang, Dr. David Firang, and Dr. Tim Aubry. Again, we note that you can watch these in any order by clicking on the image and that you should also review the key takeaways in the document that follows. As you watch, be sure to continue thinking about all four priorities that we need to achieve to end homelessness in Canada, as they are all interconnected and will emerge in these videos as well.
 |  |
 |  |
 |  |
 |  |
Key Takeaways – Waegemakers Schiff, Kennelly, Ecker, Kerman, Falvo, Hwang, Firang, and Aubry: Can we end homelessness? How?
Dr. Jeannette Waegemakers Schiff:
Dr. Jacqueline Kennelly:
Dr. John Ecker:
Dr. Nick Kerman:
Dr. Nick Falvo:
Dr. Stephen Hwang:
Dr. David Firang:
Dr. Tim Aubry:
In the Introduction to this book, we posed the question, “What is homelessness?” and learned about the Canadian Definition of Homelessness (Gaetz et al., 2012) which includes people who are precariously housed and those at-risk of losing their housing. These terms reflect individuals who might have some degree of housing, but it is not suitable for long-term habitation, or they are at risk of losing it if they experience a sudden change like a job loss or relationship breakdown. Instead of placing all of our focus on helping people once they are unsheltered or emergency sheltered, we need to look further upstream. There is a growing body of research and advocacy work that demonstrates the importance of making the shift towards prevention (Dej, Gaetz, & Schwan, 2020; Gaetz; 2020; Gaetz & Dej, 2017). Preventing homelessness before it begins is arguably the best way to reduce the number of people experiencing homelessness. To achieve this goal, systems-level changes are needed, particularly related to discharge from public institutions and by implementing eviction-prevention measures to keep people from losing their housing.
The videos below are from seven researchers who all spoke about the importance of prevention as a priority for ending homelessness in Canada. Here we invite you to watch the responses of Dr. Stephen Gaetz, Dr. Tyler Frederick, Dr. Bernie Pauly, Dr. Bill O’Grady, Dr. Cheryl Forchuk, Dr. Sean Kidd, and Dr. Kelli Stajduhar. To watch these videos, simply click on the images. We also remind you to check out the key takeaways for each video in the document that follows. As you watch them, we encourage you to continue thinking about these four priorities for ending homelessness in Canada, and how they intersect with one another.
 |  |
 |  |
 |  |
 |
Key Takeaways – Gaetz, Frederick, Pauly, O’Grady, Forchuk, Kidd, and Stajduhar: Can we end homelessness? How?
Dr. Stephen Gaetz:
Dr. Tyler Frederick:
Dr. Bernie Pauly:
Dr. Bill O’Grady:
Dr. Cheryl Forchuk:
Dr. Sean Kidd:
Dr. Kelli Stajduhar:
Now that you have heard what everyone had to say, what is your opinion? Has your response to this question changed at all from what you wrote down at the beginning of the chapter? Share your thoughts with us by tweeting @Homeless_ebook and using the hashtag #UnderstandingHomelessness.
Click the link below to listen to all of the researchers answer the question “Part 1 – Can we end homelessness, how?” in audio format on our podcast!
Click the link below to listen to all of the researchers answer the question “Part 2 – Can we end homelessness, how?” in audio format on our podcast!
126
We have asked many questions throughout this book and found that, despite their apparent simplicity, the answers to them have been rather complex. In this final concluding chapter, we asked the questions, “Can we end homelessness? How?” We found that although the researchers we spoke to may have highlighted different aspects, there were four key priorities that came through loud and clear. To end homelessness in Canada, we must create deeply affordable housing, as a human right. To end homelessness in Canada, we must implement individualized choice-based supports to meet people’s unique needs. To end homelessness in Canada, we must hold the government accountable for social policy, past, present, and future. To end homelessness in Canada, we must prevent it from occurring through systemic change.
Ending homelessness requires that we all understand that it is not an individual-level problem but rather an issue that is created and sustained by our society. We have heard that homelessness is not natural or inevitable. As we move towards ending it in our country, we must collectively adopt an approach that is trauma-informed, person-centered, socially inclusive, and situated within a social determinants of health framework. Ending homelessness is all of our responsibility because it is an issue that impacts all of our society.
We hope that by reading this book you have developed a keener sense of the complexity of homelessness. While we often hear that housing is the solution, we have to also realize that there are many additional issues and factors to consider. After much deliberation, we decided to call this book, “Understanding Homelessness in Canada: From the Streets to the Classroom.” It is our sincere hope that you take your new understanding of homelessness from the classroom back out into the streets.
127
Here are some additional resources you may want to check out!
128
If you are interested in learning more about homelessness and contributing new knowledge to the field, here are some ideas you may want to consider for an Honour’s or Master’s thesis.
129
Aubry, T. (2020). Analysis of housing first as a practical and policy relevant intervention: The current state of knowledge and future directions for research. European Journal of Homelessness, 14(1), 13-26. https://www.feantsaresearch.org
Biss, M., & Raza, S. (2021). Implementing the right to housing in Canada: Expanding the national housing strategy. Canada: The National Right to Housing Network. https://housingrights.ca/wp-content/uploads/NRHN-OFHA-Expanding-the-NHS-2021.pdf
Centre for Equality Rights in Accommodation and The National Right to Housing Network. (2021). The rights to life, protection of the home & nondiscrimination in Canada: Assessing the housing & homelessness crisis in accordance with Articles 2, 6, 17 & 26 of the ICCPR. Canada: CERA & NRHN. ICCPRSubmission-NRHN-CERA-2021.pdf (housingrights.ca)
Chung, T. E., Gozdzik, A., Palma Lazgare, L. I., To, M. J., Aubry, T., Frankish, J., Hwang, S. W., & Stergiopoulos, V. (2018). Housing First for older homeless adults with mental illness: a subgroup analysis of the At Home/Chez Soi randomized controlled trial. International Journal of Geriatric Psychiatry, 33(1), 85–95. https://doi.org/10.1002/gps.4682
Dej, E., Gaetz, S., & Schwan, K. (2020). Turning off the tap: A typology for homelessness prevention. The Journal of Primary Prevention, 41(5), 397–412. https://doi.org/10.1007/s10935-020-00607-y
Distasio, J., Zell, S., & Snyder, M. (2018). At home in Winnipeg: Localizing housing first as a culturally responsive approach to understanding and addressing urban Indigenous homelessness. Winnipeg: Institute of Urban Studies. At Home in Winnipeg
Forchuk, C., Richardson, J., Atyeo, H., & Serrato, J. (2021). Qualitative findings from a housing first evaluation project for homeless veterans in Canada. Journal of Military, Veteran and Family Health. Advance Access Article. https://doi.org/10.3138/jmvfh-2021-0052
Gaetz, S. (2020). Making the prevention of homelessness a priority: The role of social innovation. The American Journal of Economics and Sociology, 79(2), 353–381. https://doi.org/10.1111/ajes.12328
Gaetz, S., Barr, C., Friesen, A., Harris, B., Hill, C., Kovacs-Burns, K., Pauly, B., Pearce, B., Turner, A., & Marsolais, A. (2012) Canadian definition of homelessness. Toronto: Canadian Observatory on Homelessness Press. COHhomelessdefinition.pdf (homelesshub.ca)
Gaetz, S. & Dej, E. (2017). A new direction: A framework for homelessness prevention. Toronto: Canadian Observatory on Homelessness Press.
Gaetz, S., Walter, H. & Story, C. (2021). THIS is Housing First for youth. Part 1 – program model guide. Toronto, ON: Canadian Observatory on Homelessness Press.
Government of Canada. (2017). A place to call home: Canada’s national housing strategy. Government of Canada, Ottawa. Canada’s National Housing Strategy (placetocallhome.ca)
Government of Canada. (2018). Reaching home: Canada’s homelessness strategy directives. Government of Canada, Ottawa. Reaching Home: Canada’s Homelessness Strategy Directives – Canada.ca
Government of Canada. (2019). National housing strategy act. Government of Canada, Ottawa. National Housing Strategy Act (justice.gc.ca)
Oudshoorn, A., Forchuk, C., Hall, J., Smith-Carrier, T., & Van Berkum, A. (2018). An evaluation of a Housing First program for chronically homeless women. Journal of Social Inclusion, 9(2), 34–. https://doi.org/10.36251/josi.136
Porter, B. (2021). Implementing the right to adequate housing under the national housing strategy act: The international human rights framework. Canada: The National Right to Housing Network. NRHN OFHA Report Cover 2021 (housingrights.ca)
Schwan, K., Vaccaro, M. E., Reid, L., & Ali, N. (2021). Implementation of the right to housing for women, girls, and gender diverse people in Canada. Canada: The National Right to Housing Network. Microsoft Word – EN_CHRC_13.docx (housingrights.ca)
1
The artwork featured here was collected by authors James Davy and Nicole Whitmore who reached out to community members with lived experience of homelessness.
The work of these artists greatly enriched the content of the book.
Featured in Chapter 1.
Homelessness is tormented darkness. There is no real centre. The colours, green, red, and blue represent the elements of earth, fire, and water. The darkness is battling against them. No colours can be established anywhere.
Featured in Chapter 2.
Featured in Chapter 3.
Featured in Chapter 4.
The feeling of having nowhere to go and confusion experienced with homelessness. Colourful matrices surround and are part of the wisps of thought, the hues of the soul, but the inner and outer turmoil is what is featured.
Featured in Chapter 5.
Featured in Chapter 6.
Featured in Chapter 7.
Featured in Chapter 8.
Featured in Chapter 9.
Featured in Chapter 10.
2
Abdel‐Baki, A., Aubin, D., Morisseau‐Guillot, R., Lal, S., Dupont, M., Bauco, P., … Iyer, S. N. (2019). Improving mental health services for homeless youth in downtown Montreal, Canada: Partnership between a local network and ACCESS Esprits ouverts (Open Minds), a national services transformation research initiative. Early Intervention in Psychiatry, 13(S1), 20–28. https://doi.org/10.1111/eip.12814
Abramovich, A. (2016). Preventing, reducing and ending LGBTQ2S youth homelessness: The need for targeted strategies. Social Inclusion, 4 (4).
Abramovich, A. (2017). Understanding how policy and culture create oppressive conditions for LGBTQ2S youth in the shelter system. Journal of Homosexuality, 64(11), 1484–1501. https://doi.org/10.1080/00918369.2016.1244449
Abramovich, A. (2018). Responding to the needs of LGBTQ2S youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Abramovich, A., de Oliveira, C., Kiran, T., Iwajomo, T., Ross, L. E., & Kurdyak, P. (2020). Assessment of health conditions and health service use among transgender patients in Canada. JAMA Netw Open, 3(8), https://doi.org/10.1001/jamanetworkopen.2020.15036
Abramovich, A., Lam, J. S. H., & Chowdhury, M. (2020). A transgender refugee woman experiencing posttraumatic stress disorder symptoms and homelessness. Canadian Medical Association Journal (CMAJ), 192(1), E9–E11. https://doi.org/10.1503/cmaj.190974
Abramovich, A., & Pang, N. (2020) Understanding LGBTQ2S youth homelessness in York Region. Toronto, ON. Report LGBTQ2S Youth in York Region
Abramovich, A., Pang, N., Moss, A., Logie, C. H., Chaiton, M., Kidd, S. A., & Hamilton, H. A. (2021). Investigating the impacts of COVID-19 among LGBTQ2S youth experiencing homelessness. PLOS ONE, 16(9): e0257693. https://doi.org/10.1371/journal.pone.0257693
Abramovich, A., & Shelton, J. (2017a). Conclusion: The way forward. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Abramovich, A., & Shelton, J. (2017b). Introduction: Where are we now?. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Advisory Committee on Homelessness. (2018). Final Report. Canada: Employment and Social Development Canada.
Agarwal, G., Lee, J., McLeod, B., Mahmuda, S., Howard, M., Cockrell, K., & Angeles, R. (2019). Social factors in frequent callers: a description of isolation, poverty and quality of life in those calling emergency medical services frequently. BMC Public Health, 19(1), 684–684. https://doi.org/10.1186/s12889-019-6964-1
Ahajumobi, E. N., & Anderson, P. B. (2020). Homeless Canadians’ perspectives on homelessness in Calgary. Journal of Social, Behavioral and Health Sciences, 14(1). https://doi.org/10.5590/JSBHS.2020.14.1.08
Alberton, A. M., Angell, G. B., Gorey, K. M., & Grenier, S. (2020). Homelessness among Indigenous peoples in Canada: The impacts of child welfare involvement and educational achievement. Children and Youth Services Review, 111, 104846–. https://doi.org/10.1016/j.childyouth.2020.104846
Alschech, J., Taiwo-Hanna, T., & Shier, M. L. (2020). Navigating peer-influences in a large youth homeless shelter in North America. Children and Youth Services Review, 108, 104665–. https://doi.org/10.1016/j.childyouth.2019.104665
Alunni-Menichini, K., Bertrand, K., Roy, L., & Brousselle, A. (2020). Current emergency response in Montreal: How does it fit in the services offered to homeless people who use substances? The International Journal of Drug Policy, 82, 102758–102758. https://doi.org/10.1016/j.drugpo.2020.102758
Andermann, A., Bloch, G., Goel, R., Brcic, V., Salvalaggio, G., Twan, S., … Pottie, K. (2020). Caring for patients with lived experience of homelessness. Canadian Family Physician, 66(8), 563–570. PMC7430777
Andermann, A., Mott, S., Mathew, C. M., Kendall, C., Mendonca, O., Harriott, D., … Pottie, K. (2021). Evidence-informed interventions and best practices for supporting women experiencing or at risk of homelessness: a scoping review with gender and equity analysis. Health Promotion and Chronic Disease Prevention in Canada, 41(1), 1–13. https://doi.org/10.24095/hpcdp.41.1.01
Anderson, N. (1923). The hobo: The Sociology of the homeless man. Chicago: The University of Chicago Press.
Anderson-Baron, J. T., & Collins, D. (2019). “Take whatever you can get”: Practicing Housing First in Alberta. Housing Studies, 34(8), 1286–1306. https://doi.org/10.1080/02673037.2018.1535055
Ansloos, J. P., & Wager, A. C. (2020). Surviving in the cracks: A qualitative study with indigenous youth on homelessness and applied community theatre. International Journal of Qualitative Studies in Education, 33(1), 50–65. https://doi.org/10.1080/09518398.2019.1678785
Asare, A. O., Wong, A. M., Maurer, D., & Nishimura, M. (2019). Access to vision services by vulnerable populations in Canada: A scoping review. Journal of Health Care for the Poor and Underserved, 30(1), 6–27. https://doi.org/10.1353/hpu.2019.0003
Aubry, T. (2020). Analysis of housing first as a practical and policy relevant intervention: The current state of knowledge and future directions for research. European Journal of Homelessness, 14(1), 13-26. https://www.feantsaresearch.org
Aubry, T., Agha, A., Mejia-Lancheros, C., Lachaud, J., Wang, R., Nisenbaum, R., … Hwang, S. W. (2021). Housing trajectories, risk factors, and resources among individuals who are homeless or precariously housed. The Annals of the American Academy of Political and Social Science, 693(1), 102–122. https://doi.org/10.1177/0002716220987203
Baggett, T. P., Liauw, S. S., & Hwang, S. W. (2018). Cardiovascular disease and homelessness. Journal of the American College of Cardiology, 71(22), 2585–2597. https://doi.org/10.1016/j.jacc.2018.02.077
Baker Collins, S., Schormans, A. F., Watt, L., Idems, B., & Wilson, T. (2018). The invisibility of disability for homeless youth. Journal of Social Distress and the Homeless, 27(2), 99–109. https://doi.org/10.1080/10530789.2018.1480892
Baker Collins, S., & Fudge Schormans, A. (2021). Making visible the prevalence of self-identified disability among youth experiencing homelessness. Journal of Social Distress and Homelessness. https://doi.org/10.1080/10530789.2021.1940719
Baker Collins, S., Smith-Carrier, T., Gazso, A., & Smith, C. (2020). Resisting the culture of poverty narrative: Perspectives of social assistance recipients. Journal of Poverty, 24(1), 72–93. https://doi.org/10.1080/10875549.2019.1678551
Ballard, M., Coughlin, J., & Martin, D. (2020). Reconciling with Minoaywin: First Nations Elders’ advice to promote healing from forced displacement. Canadian Journal on Aging, 39(2), 169–177. https://doi.org/10.1017/S0714980819000412
Bani-Fatemi, A., Malta, M., Noble, A., Wang, W., Rajakulendran, T., Kahan, D., & Stergiopoulos, V. (2020). Supporting female survivors of gender-based violence experiencing homelessness: Outcomes of a health promotion psychoeducation group intervention. Frontiers in Psychiatry, 11, 601540–601540. 10.3389/fpsyt.2020.601540
Barbic, S. P., Jones, A. A., Woodward, M., Piercy, M., Mathias, S., Vila-Rodriguez, F., … Honer, W. G. (2018). Clinical and functional characteristics of young adults living in single room occupancy housing: preliminary findings from a 10-year longitudinal study. Canadian Journal of Public Health, 109(2), 204–214. https://doi.org/10.17269/s41997-018-0087-9
Barbic, S. P., Kidd, S. A., Durisko, Z. T., Yachouh, R., Rathitharan, G., & McKenzie, K. (2018). What are the personal recovery needs of community-dwelling individuals with mental illness? Preliminary findings from the Canadian personal recovery outcome measurement (C-PROM) study. Canadian Journal of Community Mental Health, 37(1), 29-47. https://www.cjcmh.com/doi/pdf/10.7870/cjcmh-2018-005
Bardwell, G. (2019). The impact of risk environments on LGBTQ2S adults experiencing homelessness in a midsized Canadian city. Journal of Gay & Lesbian Social Services, 31(1), 53-64. https://doi.org/10.1080/10538720.2019.1548327
Bardwell, G., Boyd, J., Kerr, T., & McNeil, R. (2018). Negotiating space & drug use in emergency shelters with peer witness injection programs within the context of an overdose crisis: A qualitative study. Health & Place, 53, 86–93. https://doi.org/10.1016/j.healthplace.2018.07.011
Bardwell, G., Kerr, T., Boyd, J., & McNeil, R. (2018). Characterizing peer roles in an overdose crisis: Preferences for peer workers in overdose response programs in emergency shelters. Drug and Alcohol Dependence, 190, 6–8. https://doi.org/10.1016/j.drugalcdep.2018.05.023
Barker, B., Kerr, T., Dong, H., Wood, E., & DeBeck, K. (2017). High school incompletion and childhood maltreatment among street‐involved young people in Vancouver, Canada. Health & Social Care in the Community, 25(2), 378–384. https://doi.org/10.1111/hsc.12314
Barker, B., Shoveller, J., Grant, C., Kerr, T., & DeBeck, K. (2020). Long-term benefits of providing transitional services to youth aging-out of the child welfare system: Evidence from a cohort of young people who use drugs in Vancouver, Canada. The International Journal of Drug Policy, 85, 102912–102912. https://doi.org/10.1016/j.drugpo.2020.102912
Baron, S. W., & Forde, D. R. (2020). Childhood trauma, criminogenic social schemas, and violent crime. Deviant Behavior, 41(8), 991–1004. https://doi.org/10.1080/01639625.2019.1596534
Barone, C., Yamamoto, A., Richardson, C. G., Zivanovic, R., Lin, D., & Mathias, S. (2019). Examining patterns of cognitive impairment among homeless and precariously housed urban youth. Journal of Adolescence, 72, 64–69. https://doi.org/10.1016/j.adolescence.2019.02.011
Barrow, S. K. (2018). Scholarship review of queer youth homelessness in Canada and the United States. The American Review of Canadian Studies, 48(4), 415–431. https://doi.org/10.1080/02722011.2018.1531603
Baumann, R. M., Hamilton-Wright, S., Riley, D. L., Brown, K., Hunt, C., Michalak, A., & Matheson, F. I. (2019). Experiences of violence and head injury among women and transgender women sex workers. Sexuality Research & Social Policy, 16(3), 278–288. https://doi.org/10.1007/s13178-018-0334-0
Begun, S. (2019). The association between social capital and pregnancy attitudes among youth experiencing homelessness. Journal of Obstetrics and Gynaecology Canada, 41(5), 710–710. https://doi.org/10.1016/j.jogc.2019.02.159
Benbow, S., Forchuk, C., Berman, H., Gorlick, C., & Ward-Griffin, C. (2019a). Mothering without a home: Internalized impacts of social exclusion. Canadian Journal of Nursing Research, 51(2), 105–115. https://doi.org/10.1177/0844562118818948
Benbow, S., Forchuk, C., Berman, H., Gorlick, C., & Ward-Griffin, C. (2019b). Spaces of exclusion: Safety, stigma, and surveillance of mothers experiencing homelessness. Canadian Journal of Nursing Research, 51(3), 202–213. https://doi.org/10.1177/0844562119859138
Benbow, S., Forchuk, C., Gorlick, C., Berman, H., & Ward-Griffin, C. (2019c). “Until You hit rock bottom there’s no support”: Contradictory sources and systems of support for mothers experiencing homelessness in southwestern Ontario. Canadian Journal of Nursing Research, 51(3), 179–190. https://doi.org/10.1177/0844562119840910
Benoit, C., Jansson, S. M., Smith, M., & Flagg, J. (2018). Prostitution stigma and its effect on the working conditions, personal lives, and health of sex workers. The Journal of Sex Research, 55(4-5), 457–471. https://doi.org/10.1080/00224499.2017.1393652
Benoit, C., Maurice, R., Abel, G., Smith, M., Jansson, M., Healey, P., & Magnuson, D. (2020). “I dodged the stigma bullet”: Canadian sex workers’ situated responses to occupational stigma. Culture, Health & Sexuality, 22(1), 81–95. https://doi.org/10.1080/13691058.2019.1576226
Benmarhnia, T., Alexander, S., Price, K., Smargiassi, A., King, N., & Kaufman, J. S. (2018). The heterogeneity of vulnerability in public health: a heat wave action plan as a case study. Critical Public Health, 28(5), 619–625. https://doi.org/10.1080/09581596.2017.1322176
Benn, A. (2017). The Black queer youth initiative: Challenging racism, stigma & exclusion. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Bezgrebelna, M., McKenzie, K., Wells, S., Ravindran, A., Kral, M., Christensen, J., Stergiopoulos, V., Gaetz, S., & Kidd, S. A. (2021). Climate change, weather, housing precarity, and homelessness: A systematic review of reviews. Int. J. Environ. Res. Public Health, 18, 5812. https://doi.org/10.3390/ijerph18115812
Bingham, B., Moniruzzaman, A., Patterson, M., Distasio, J., Sareen, J., O’Neil, J., & Somers, J. M. (2019a). Indigenous and non-Indigenous people experiencing homelessness and mental illness in two Canadian cities: A retrospective analysis and implications for culturally informed action. BMJ Open, 9(4), e024748–e024748. https://doi.org/10.1136/bmjopen-2018-024748
Bingham, B., Moniruzzaman, A., Patterson, M., Sareen, J., Distasio, J., O’Neil, J., & Somers, J. M. (2019b). Gender differences among Indigenous Canadians experiencing homelessness and mental illness. BMC Psychology, 7(1), 57–57. https://doi.org/10.1186/s40359-019-0331-y
Biss, M., & Raza, S. (2021). Implementing the right to housing in Canada: Expanding the national housing strategy. Canada: The National Right to Housing Network. https://housingrights.ca/wp-content/uploads/NRHN-OFHA-Expanding-the-NHS-2021.pdf
Bodkin, C., Mokashi, V., Beal, K., Wiwcharuk, J., Lennox, R., Guenter, D., … O’Shea, T. (2020). Pandemic planning in homeless shelters: A pilot study of a COVID-19 testing and support program to mitigate the risk of COVID-19 outbreaks in congregate settings. Clinical Infectious Diseases, 72(9), 1639-1641. https://doi.org/10.1093/cid/ciaa743
Bono, K. (2019). The faces of Indigenous homelessness: The perpetual Inuit housing struggle. Master’s Thesis. McGill University.
Bourque, J., VanTil, L., Nadeau, J., LeBlanc, S. R., Ebner-Daigle, J., Gibbons, C., & Darte, K. (2017). Physical health status of homeless veterans in Canada: A cross-sectional study. Journal of Military, Veteran and Family Health, 3(2), 4–11. https://doi.org/10.3138/jmvfh.4251
Bowra, A., & Mashford-Pringle, A. (2021). More than a structure: Exploring the relationship between Indigenous homemaking practices and wholistic wellbeing. Wellbeing, Space and Society, 2. https://doi.org/10.1016/j.wss.2020.100007
Brakenhoff, B., & Slesnick, N. (2018). Substance use and mental health interventions for youth who are homeless: The community reinforcement approach and motivational enhancement therapy. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Brown, S. M., & Bender, K. (2018). Mindfulness approaches for youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Brown, J., Knol, D., Prevost-Derbecker, S., & Andrushko, K. (2007). Housing for Aboriginal oyuth in the inner city of Winnipeg. First Peoples Child & Family Review, 3(2), 56–64. https://doi.org/10.7202/1069464ar
Brown, E. L., Phillippo, K. L., Weston, K., & Rodger, S. (2019). United States and Canada pre-service teacher certification standards for student mental health: A comparative case study. Teaching and Teacher Education, 80, 71–82. https://doi.org/10.1016/j.tate.2018.12.015
Buccieri, K. (2013). Back to the future for Canada’s national anti-drug strategy: Homeless youth and the need for harm reduction. In S. Gaetz, B. O’Grady, K. Buccieri, J. Karabanow, & A. Marsolais (Eds.), Youth homelessness in Canada: Implications for policy and practice (199-215). Toronto, ON: The Canadian Homelessness Research Network. Youth Homelessness in Canada (homelesshub.ca)
Buccieri, K. (2016). H1N1 and homelessness in Toronto: Identifying structural issues in the homelessness sector. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Buccieri, K. (2019). “My brother was his little angel; I was the problem child”: Perceived sibling favoritism in the narratives of youth who become homeless. Journal of Family Issues, 40(11), 1419–1437. https://doi.org/10.1177/0192513X19839748
Buccieri, K. (2020). Pandemic planning: How can my agency prepare for the potential spread of Coronavirus? Toronto, ON: The Homeless Hub.
Buccieri, K., Oudshoorn, A., Frederick, T., Schiff, R., Abramovich, A., Gaetz, S. & Forchuk, C. (2019), Hospital discharge planning for Canadians experiencing homelessness. Housing, Care and Support, 22(1), 4-14. https://doi.org/10.1108/HCS-07-2018-0015
Buccieri, K., Oudshoorn, A., Waegemakers Schiff, J., Pauly, B., Schiff, R., & Gaetz, S. (2020). Quality of life and mental well-being: A gendered analysis of persons experiencing homelessness in Canada. Community Mental Health Journal, 56(8), 1496–1503. 10.1007/s10597-020-00596-6
Buccieri, K. & Schiff, R. (Eds.). (2016). Pandemic preparedness and homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Buck-McFadyen, E. (2021). Competing perspectives on rural homelessness: Findings from a qualitative study in Ontario, Canada. Health & Social Care in the Community. https://doi.org/10.1111/hsc.13633
Burns, V. F., & Sussman, T. (2019). Homeless for the first time in later life: Uncovering more than one pathway. The Gerontologist, 59(2), 251–259. https://doi.org/10.1093/geront/gnx212
Burns, V. F., Sussman, T., & Bourgeois-Guérin, V. (2018). Later-life homelessness as disenfranchised grief. Canadian Journal on Aging, 37(2), 171–184. https://doi.org/10.1017/S0714980818000090
CAMH. (2021). Addiction. Centre for Addiction and Mental Health, Toronto. Addiction | CAMH
Canadian Observatory on Homelessness. (2016). Canadian Definition of Youth Homelessness. Canada: Canadian Observatory on Homelessness.
Canadian Observatory on Homelessness and Blue Door. (2021). The future of men’s supportive housing in York Region: An exploratory study. Ontario: Canadian Observatory on Homelessness and Blue Door. Blue Door Executive Summary
Canham, S. L., Battersby, L., Fang, M. L., Wada, M., Barnes, R., & Sixsmith, A. (2018). Senior services that support Housing First in Metro Vancouver. Journal of Gerontological Social Work, 61(1), 104–125. https://doi.org/10.1080/01634372.2017.1391919
Canham, S., Davidson, S., Custodio, K., Mauboules, C., Good, C., Wister, A. V., & Bosma, H. (2018). Health needs of older homeless persons who are transitioning from hospital to shelter/housing. Innovation in Aging, 2(suppl_1), 56. https://doi.org/10.1093/geroni/igy023.209
Canham, S. L., Davidson, S., Custodio, K., Mauboules, C., Good, C., Wister, A. V., & Bosma, H. (2019). Health supports needed for homeless persons transitioning from hospitals. Health & Social Care in the Community, 27(3), 531–545. https://doi.org/10.1111/hsc.12599
Canham, S. L., Fang, M. L., Battersby, L., & Wada, M. (2019). Understanding the functionality of housing-related support services through mapping methods and dialogue. Evaluation and Program Planning, 72, 33–39. https://doi.org/10.1016/j.evalprogplan.2018.09.008
Canham, S. L., Wister, A., & O’Dea, E. (2019). Strengths, weaknesses, opportunities, and threats to Housing First in Metro Vancouver. Evaluation and Program Planning, 75, 69–77. https://doi.org/10.1016/j.evalprogplan.2019.05.004
Caplan, R., Nelson, G., Distasio, J., Isaak, C., Edel, B., Piat, M., Macnaughton, E., Kirst, M., Patterson, M., Aubry, T., Mulligan, S., & Goering, P. (2020). Indigenous and non‐Indigenous parents separated from their children and experiencing homelessness and mental illness in Canada. Journal of Community Psychology, 48(8), 2753–2772. https://doi.org/10.1002/jcop.22455
Carroll, B. W. (1989). Post-war trends in Canadian housing policy. Urban History Review / Revue d’histoire urbaine, 18(1), 64–74. https://doi.org/10.7202/1017825ar
Centre for Equality Rights in Accommodation and The National Right to Housing Network. (2021). The rights to life, protection of the home & nondiscrimination in Canada: Assessing the housing & homelessness crisis in accordance with Articles 2, 6, 17 & 26 of the ICCPR. Canada: CERA & NRHN. ICCPRSubmission-NRHN-CERA-2021.pdf (housingrights.ca)
Cerswell Kielburger, L., Rockman, P., & Baranek, P. (2018). Preventing burnout among service providers. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Chan, E., & Huys, J. (2017). Addressing the legal needs of LGBTQ2S youth experiencing homelessness. In A. Abramovich, & J. Shelton (eds.), Where Am I Going to Go? Intersectional Approaches to Ending LGBTQ2S Youth Homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Chang, D. C., Rieb, L., Nosova, E., Liu, Y., Kerr, T., & DeBeck, K. (2018). Hospitalization among street-involved youth who use illicit drugs in Vancouver, Canada: A longitudinal analysis. Harm Reduction Journal, 15(1), 14–14. https://doi.org/10.1186/s12954-018-0223-0
Charron, C. B., Hudani, A., Kaur, T., Rose, T., Florence, K., Jama, S., & Pakhalé, S. (2018). Assessing community (peer) researcher’s experiences with conducting spirometry and being engaged in the “Participatory research in Ottawa: Management and point-of-care for tobacco-dependence” (PROMPT) project. Research Involvement and Engagement, 4(1), 43–43. https://doi.org/10.1186/s40900-018-0125-z
Chen, X., Cooper, I., & Rivier, J. (2021). Homelessness prevention and determinants of housing among first-time and recurrent emergency shelter users in Canada. Housing Studies, 1–17. https://doi.org/10.1080/02673037.2020.1865520
Cherner, R. A., Aubry, T., & Ecker, J. (2017). Predictors of the physical and psychological integration of homeless adults with problematic substance use. Journal of Community Psychology, 45(1), 65–80. https://doi.org/10.1002/jcop.21834
Chesnay, C. T., Bellot, C., & Sylvestre, M. E. (2013). Taming disorderly people one ticket at a time: The penalization of homelessness in Ontario and British Columbia. Canadian Journal of Criminology and Criminal Justice, 55(2), 161–185. https://doi.org/10.3138/cjccj.2011-E-46
Chisholm, S., & Hulchanski, D. (2019). Canada’s housing story. In D. Maclennan, H. Pawson, K. Gibb, S. Chisholm, & D. Hulchanski (Eds.). SF 21: Shaping Futures Changing the Housing Story Final Report. University of Glasgow: Policy Scotland. canadas-housing-story-2019-chap-4.pdf (neighbourhoodchange.ca)
Chiu, S., Redelmeier, D. A., Tolomiczenko, G., Kiss, A., & Hwang, S. W. (2009). The health of homeless immigrants. Journal of Epidemiology & Community Health, 63(11), 943-948. http://dx.doi.org/10.1136/jech.2009.088468
Chung, T. E., Gozdzik, A., Palma Lazgare, L. I., To, M. J., Aubry, T., Frankish, J., Hwang, S. W., & Stergiopoulos, V. (2018). Housing First for older homeless adults with mental illness: a subgroup analysis of the At Home/Chez Soi randomized controlled trial. International Journal of Geriatric Psychiatry, 33(1), 85–95. https://doi.org/10.1002/gps.4682
Cochrane, A., Pithia, P., Laird, E., Mifflin, K., Sonley-Long, V., & Batt, A. M. (2019). Investigating the attitudes of Canadian paramedic students towards homelessness. International Journal of Caring Sciences, 12(3), 1781–1787. https://doi.org/10.1101/19003483
Collins, A. B., Boyd, J., Mayer, S., Fowler, A., Kennedy, M. C., Bluthenthal, R. N., … McNeil, R. (2019). Policing space in the overdose crisis: A rapid ethnographic study of the impact of law enforcement practices on the effectiveness of overdose prevention sites. The International Journal of Drug Policy, 73, 199–207. https://doi.org/10.1016/j.drugpo.2019.08.002
Collins, D., & Stout, M. (2021). Does Housing First policy seek to fulfil the right to housing? The case of Alberta, Canada. Housing Studies, 36(3), 336–358. https://doi.org/10.1080/02673037.2019.1707782
Cook, S., & Hole, R. (2020). “Appropriately homeless and needy:” Examining street homeless survival through the lens of Bourdieusian social capital theory. Journal of Human Behavior in the Social Environment, 30(7), 816–834. https://doi.org/10.1080/10911359.2020.1747585
Côté, P. B. (2019). Sexual health services for homeless youth: A qualitative analysis of their experiences. Journal of Social Service Research, 45(3), 429–443. https://doi.org/10.1080/01488376.2018.1480568
Côté, P. B., & Blais, M. (2019). Between resignation, resistance and recognition: A qualitative analysis of LGBTQ+ youth profiles of homelessness agencies utilization. Children and Youth Services Review, 100, 437–443. https://doi.org/10.1016/j.childyouth.2019.03.024
Côté, P. B., & Blais, M. (2021). “The least loved, that’s what I was”: A qualitative analysis of the pathways to homelessness by LGBTQ+ youth. Journal of Gay & Lesbian Social Services, 33(2), 137-156. https://doi.org/10.1080/10538720.2020.1850388
Crabtree, A., Latham, N., Morgan, R., Pauly, B., Bungay, V., & Buxton, J. A. (2018). Perceived harms and harm reduction strategies among people who drink non-beverage alcohol: Community-based qualitative research in Vancouver, Canada. The International Journal of Drug Policy, 59, 85–93. https://doi.org/10.1016/j.drugpo.2018.06.020
Crago, A. L., Bruckert, C., Braschel, M., & Shannon, K. (2021). Sex workers’ access to police assistance in safety emergencies and means of escape from situations of violence and confinement under an “end demand” criminalization model: A five city study in Canada. Social Sciences (Basel), 10(1), 13–. https://doi.org/10.3390/socsci10010013
Crowe, C. (2019). A knapsack full of dreams: memoirs of a street nurse. Victoria, BC: FriesenPress.
Crowe, C., & Baker, N. (2007). Dying for a home: homeless activists speak out. Toronto, ON: Between the Lines.
Cully, L., Wu, Q., & Slesnick, N. (2018). Ecologically based family therapy for adolescents who have left home. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Cunningham, J. (2019). Towards a grounded understanding of the forms of homelessness experienced by Indigenous women in Canada. Recherches amérindiennes au Québec, 49(3), 29. https://doi.org/10.7202/1074538ar
Daiski, I. (2007). Perspectives of homeless people on their health and health needs priorities. Journal of Advanced Nursing, 58(3), 273-281. https://doi.org/10.1111/j.1365-2648.2007.04234.x
da Silva Rebelo, M. J., Fernández, M., & Achotegui, J. (2018). Mistrust, anger, and hostility in refugees, asylum seekers, and immigrants: A systematic review. Canadian Psychology, 59(3), 239–251. https://doi.org/10.1037/cap0000131
Dej, E. (2020). A complex exile: Homelessness and social exclusion in Canada. BC: UBC Press.
Dej, E. & Ecker, J. (2018). “Homelessness & precarious housing in Canada: Where we have been and where we are going.” Public Sector Digest.
Dej, E., Gaetz, S., & Schwan, K. (2020). Turning off the tap: A typology for homelessness prevention. The Journal of Primary Prevention, 41(5), 397–412. https://doi.org/10.1007/s10935-020-00607-y
Dej, E., Sanders, C., & Braimoh, J. (2021). Rewriting the narrative on homelessness in mid-size Canadian cities. Ontario: Centre for Research on Security Practices, Laurier University. Brokering a Counter-Narrative on Homelessness (homelesshub.ca)
De Leeuw, S., Greenwood, M., & Farrales, M. (2021). Indigeneity and wellness: Critically understanding the health of Indigenous peoples and communities. In K. Chamberlain & A. Lyons (Eds.). Routledge International Handbook of Critical Issues in Health and Illness. New York: Routledge International Handbooks.
Distasio, J., Adair, C. E., Hwang, S., Hinds, A., Kopp, B. C., Aubry, T., … Kaufman, A. F. (2021). Exploring the relationship between neighbourhood quality (NQ) and housing stability among formerly homeless individuals with mental illness in housing first. Wellbeing, Space and Society, 2, 100008–. https://doi.org/10.1016/j.wss.2020.100008
Distasio, J., Zell, S., & Snyder, M. (2018). At home in Winnipeg: Localizing housing first as a culturally responsive approach to understanding and addressing urban Indigenous homelessness. Winnipeg: Institute of Urban Studies. At Home in Winnipeg
Doberstein, C. (2020). Role-playing in public engagement for housing for vulnerable populations: An experiment exploring its possibilities and limitations. Land Use Policy, 99, 105032–. https://doi.org/10.1016/j.landusepol.2020.105032
Doberstein, C., & Smith, A. (2019a). Citizen support for spending to reduce homelessness in Canada’s largest urban centres. Housing Studies, 34(7), 1140–1162. https://doi.org/10.1080/02673037.2018.1520820
Doberstein, C., & Smith, A. (2019b). When political values and perceptions of deservingness collide: Evaluating public support for homelessness investments in Canada. International Journal of Social Welfare, 28(3), 282–292. https://doi.org/10.1111/ijsw.12353
Dohoo, C., Stuart, R., Finkelstein, M., Bradley, K., & Gournis, E. (2020). Risk factors associated with group A Streptococcus acquisition in a large, urban homeless shelter outbreak. Canadian Journal of Public Health, 111(1), 117–124. https://doi.org/10.17269/s41997-019-00258-5
Doré-Gauthier, V., Côté, H., Jutras-Aswad, D., Ouellet-Plamondon, C., & Abdel-Baki, A. (2019). How to help homeless youth suffering from first episode psychosis and substance use disorders? The creation of a new intensive outreach intervention team. Psychiatry Research, 273, 603–612. https://doi.org/10.1016/j.psychres.2019.01.076
D’Souza, S., M., Mirza, N. A., & Nairy Karkada, S. (2021). Development of a foot care model to determine the risk of foot problems among homeless adults in Canada. Health & Social Care in the Community. https://doi.org/10.1111/hsc.13271
Dunn, K. (2019). A comparative analysis of Indigenous and non-Indigenous homeless youth in Canada. Master’s Thesis. University of Guelph.
Durbin, A., Kapustianyk, G., Nisenbaum, R., Wang, R., Aratangy, T., Khan, B., & Stergiopoulos, V. (2019). Recovery education for people experiencing housing instability: An evaluation protocol. International Journal of Social Psychiatry, 65(6), 468–478. https://doi.org/10.1177/0020764019858650
Durbin, A., Lunsky, Y., Wang, R., Nisenbaum, R., Hwang, S. W., O’Campo, P., & Stergiopoulos, V. (2018). Borderline intellectual functioning and lifetime duration of homelessness among homeless adults with mental illness. Healthcare Policy, 14(2), 40–46. https://doi.org/10.12927/hcpol.2018.25687
Dutton, D. J., & Jadidzadeh, A. (2019). The incidence of homelessness in Canada is a population-level phenomenon: A comparison of Toronto and Calgary shelter use over time. Canadian Studies in Population, 46(2), 161–171. https://doi.org/10.1007/s42650-019-00013-8
Echenberg, H., & Munn-Rivard, L. (2020). Defining and enumerating homelessness in Canada: Background paper. Ottawa, ON: Library of Parliament.
Ecker, J., & Aubry, T. (2017). A mixed methods analysis of housing and neighbourhood impacts on community integration among vulnerably housed and homeless individuals. Journal of Community Psychology, 45(4), 528–542. https://doi.org/10.1002/jcop.21864
Ecker, J., Aubry, T., & Sylvestre, J. (2019). A review of the literature on LGBTQ adults who experience homelessness. Journal of Homosexuality, 66, 297-323. https://doi.org/10.1080/00918369.2017.1413277
Ecker, J., Aubry, T., & Sylvestre, J. (2020). Pathways into homelessness among LGBTQ2S adults. Journal of Homosexuality, 67(11), 1625–1643. https://doi.org/10.1080/00918369.2019.1600902
Ecker, J., Aubry, T., & Sylvestre, J. (2021). Experiences of LGBTQ adults who have accessed emergency shelters in a large urban city in Canada. Social Work in Public Health. https://doi.org/10.1080/19371918.2021.1976345
Ecker, J., Cherner, R., Rae, J., & Czechowski, K. (2018). Sexual intimacy, mental illness, and homelessness. American Journal of Community Psychology, 61(1-2), 131–140. https://doi.org/10.1002/ajcp.12213
Employment and Social Development Canada. (2018). Toolkit for intensive case management in Canada: A resource for those using a case management program for the housing first model. Canada: Government of Canada.
Evans, J., Collins, D., & Chai, C. (2019). On thin ice: Assembling a resilient service hub. Area (London 1969), 51(3), 451–460. https://doi.org/10.1111/area.12448
Evans, J., & Masuda, J. R. (2020). Mobilizing a fast policy fix: Exploring the translation of 10-year plans to end homelessness in Alberta, Canada. Environment and Planning. C, Politics and Space, 38(3), 503–521. https://doi.org/10.1177/2399654419884581
Falvo, N. (2021). Improving housing stability among Indigenous residents at horizon housing. Calgary: Nick Falvo Consulting. FINAL_Housing-Stability-for-Indigenous-Residents_Report.pdf
Faraji, S. L., Ridgeway, G., & Wu, Y. (2018). Effect of emergency winter homeless shelters on property crime. Journal of Experimental Criminology, 14(2), 129–140. https://doi.org/10.1007/s11292-017-9320-4
Farha, L., & Schwan, K. (2020). A national protocol for homeless encampments in Canada. Canada: UN Special Rapporteur on the Right to Housing. Tent Encampment Protocol (make-the-shift.org)
Fast, D., & Cunningham, D. (2018). “We don’t belong there”: New geographies of homelessness, addiction, and social control in Vancouver’s inner city. City & Society, 30(2), 237–262. https://doi.org/10.1111/ciso.12177
Feir, D. L., & Akee, R. (2018). Estimating institutionalization and homelessness for status First Nations in Canada: A method and implications. International Indigenous Policy Journal, 9(4). https://doi.org/10.18584/iipj.2018.9.4.2
Firang, D. (2019). Exploring housing careers among Ghanaians in Toronto, Canada. Housing Studies, 34(5), 868–891. https://doi.org/10.1080/02673037.2018.1489527
Firang, D. (2020). The impact of COVID-19 pandemic on international students in Canada. International Social Work, 63(6), 820-824. https://doi.org/10.1177/0020872820940030
Firestone, M., Syrette, J., Brant, T., Laing, M., & Teekens, S. (2021). Findings from a process evaluation of an Indigenous holistic housing support and mental health case management program in downtown Toronto. International Journal of Indigenous Health, 16(2), 139-150. https://doi.org/10.32799/ijih.v16i2.33173
Firestone, M., Syrette, J., Jourdain, T., Recollet, V., & Smylie, J. (2019). “I feel safe just coming here because there are other Native brothers and sisters”: Findings from a community-based evaluation of the Niiwin Wendaanimak Four Winds Wellness Program. Canadian Journal of Public Health, 110(4), 404–413. https://doi.org/10.17269/s41997-019-00192-6
Fisher, A., Mago, V., & Latimer, E. (2020). Simulating the evolution of homeless populations in Canada using modified deep q-learning (MDQL) and modified neural fitted q-iteration (MNFQ) algorithms. IEEE Access, 8, 92954–92968. https://doi.org/10.1109/ACCESS.2020.2994519
Fleming, T., Barker, A., Ivsins, A., Vakharia, S., & McNeil, R. (2020). Stimulant safe supply: a potential opportunity to respond to the overdose epidemic. Harm Reduction Journal, 17(1), 6–6. https://doi.org/10.1186/s12954-019-0351-1
Fleming, T., Damon, W., Collins, A. B., Czechaczek, S., Boyd, J., & McNeil, R. (2019). Housing in crisis: A qualitative study of the socio-legal contexts of residential evictions in Vancouver’s Downtown Eastside. The International Journal of Drug Policy, 71, 169–177. https://doi.org/10.1016/j.drugpo.2018.12.012
Fleury, M. J., Grenier, G., Cao, Z., & Meng, X. (2021). Typology of currently or formerly homeless individuals based on their use of health and social services. Community Mental Health Journal, 57, 948-959. DOI: 10.1007/s10597-020-00693-6
Flynn, C., Damant, D., Lapierre, S., Lessard, G., Gagnon, C., Couturier, V., & Couturier, P. (2018). When structural violences create a context that facilitates sexual assault and intimate partner violence against street-involved young women. Women’s Studies International Forum, 68, 94–103. https://doi.org/10.1016/j.wsif.2018.01.004
Forchuk, C., Gyamfi, S., Martin, M. L., Corring, D., Srivastava, R., & Harerimana, B. (2021). Transitional discharge model for community mental health integration: A focused ethnographic study of clients’ perspectives. International Journal of Mental Health Nursing, 30(2), 553-562. https://doi.org/10.1111/inm.12821
Forchuk, C., Martin, M. L., Sherman, D., Corring, D., Srivastava, R., O’Regan, T., Gyamfi, S., & Harerimana, B. (2020). Healthcare professionals’ perceptions of the implementation of the transitional discharge model for community integration of psychiatric clients. International Journal of Mental Health Nursing, 29(3), 498-507. https://doi.org/10.1111/inm.12687
Forchuk, C., Richardson, J., Atyeo, H., & Serrato, J. (2021a). Qualitative findings from a housing first evaluation project for homeless veterans in Canada. Journal of Military, Veteran and Family Health. Advance Access Article. https://doi.org/10.3138/jmvfh-2021-0052
Forchuk, C., Russell, G., Richardson, J., Perreault, C., Hassan, H., Lucyk, B., & Gyamfi, S. (2021b). Family matters in Ontario: Understanding and addressing homelessness among newcomer families in Canada. Canadian Journal of Nursing Research. https://doi.org/10.1177/0844562121998206
Frankish, C. J., Hwang, S. W., & Quantz, D. (2005). Homelessness and health in Canada: Research lessons and priorities. CJPH, 95, S23-S29. https://doi.org/10.1007/BF03403700
Frederick, T. (2019a). ‘A person like me’: identity narratives, dual process theories, and subsistence related decision-making among young people experiencing homelessness, Journal of Youth Studies, 22(8), 1083-1100. DOI: 10.1080/13676261.2018.1563674
Frederick, T. (2019b). Conceptualizing the social and cultural organization of street life among young people experiencing homelessness. Journal of Youth Studies, 22(8), 1133–1149. https://doi.org/10.1080/13676261.2019.1569214
Frederick, T., O’Connor, C., & Koziarski, J. (2018). Police interactions with people perceived to have a mental health problem: A critical review of frames, terminology, and definitions. Victims & Offenders, 13(8), 1037-1054. 10.1080/15564886.2018.1512024
Frederick, T., Vitopoulos, N., Leon, S., & Kidd, S. (2021). Subjective housing stability in the transition away from homelessness. Journal of Community Psychology. Early view. https://doi.org/10.1002/jcop.22702
French, D. (2017). A Provincial response to LGBTQ2S youth homelessness. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Gabet, M., Grenier, G., Cao, Z., & Fleury, M. J. (2019). Predictors of emergency department use among individuals with current or previous experience of homelessness. International Journal of Environmental Research and Public Health, 16(24), 4965. https://doi.org/10.3390/ijerph16244965
Gadermann, A. M., Karim, M. E., Norena, M., Emerson, S. D., Hubley, A. M., Russell, L. B., Nisenbaum, R., Hwang, S. W., Aubry, T., & Palepu, A. (2020). The association of residential instability and hospitalizations among homeless and vulnerably housed individuals: Results from a prospective cohort study. Journal of Urban Health, 97(2), 239–249. https://doi.org/10.1007/s11524-019-00406-9
Gaddis, A., Lake, S., Tupper, K., Nosova, E., Blommaert, K., Wood, E., & DeBeck, K. (2018). Regular MDMA use is associated with decreased risk of drug injection among street-involved youth who use illicit drugs. Drug and Alcohol Dependence, 192, 112–117. https://doi.org/10.1016/j.drugalcdep.2018.07.035
Gaetz, S. (2010). The struggle to end homelessness in Canada: How we created the crisis, and how we can end it. Open Health Services and Policy Journal, 3, 21-26.
Gaetz, S. (2018). Commentary: Harm reduction, managed alcohol programs and doing the right thing. Drug and Alcohol Review, 37(S1), S195–S196. https://doi.org/10.1111/dar.12652
Gaetz, S. (2018). Reflections from Canada: Can research contribute to better responses to youth homelessness? Cityscape, 20(3), 139–146. Cityscape – Volume 20 Number 3 (huduser.gov)
Gaetz, S. (2020). Making the prevention of homelessness a priority: The role of social innovation. The American Journal of Economics and Sociology, 79(2), 353–381. https://doi.org/10.1111/ajes.12328
Gaetz, S., Barr, C., Friesen, A., Harris, B., Hill, C., Kovacs-Burns, K., Pauly, B., Pearce, B., Turner, A., & Marsolais, A. (2012) Canadian definition of homelessness. Toronto: Canadian Observatory on Homelessness Press.
Gaetz, S., & Buccieri, K. (2016). The challenges of pandemic planning in the context of homelessness. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Gaetz, S. & Dej, E. (2017). A new direction: A framework for homelessness prevention. Toronto: Canadian Observatory on Homelessness Press.
Gaetz, S., O’Grady, B., Kidd, S., & Schwan, K. (2016). Without a home: The national youth homelessness survey. Toronto: Canadian Observatory on Homelessness Press
Gaetz, S., Schwan, K., Redman, M., French, D., & Dej, E. (2018). The roadmap for the prevention of youth homelessness – executive summary. A. Buchnea (Ed.). Toronto, ON: Canadian Observatory on Homelessness Press.
Gaetz, S., Walter, H. and Story, C. (2021). THIS is Housing First for youth. Part 1 – program model guide. Toronto, ON: Canadian Observatory on Homelessness Press.
Gaetz, S., Ward, A., & Kimura, L. (2019). Youth homelessness and housing stability: What outcomes should we be looking for? Healthcare Management Forum, 32(2), 73–77. https://doi.org/10.1177/0840470418817333
Gattis, M., & Larson, A. (2017). Discrimination & mental health outcomes of Black youth experiencing homelessness. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Gauvin, G., Labelle, R., Daigle, M., Breton, J. J., & Houle, J. (2019). Coping, social support, and suicide attempts among homeless adolescents. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 40(6), 390–399. https://doi.org/10.1027/0227-5910/a000579
Gazso, A., Baker Collins, S., Smith-Carrier, T., & Smith, C. (2019). The generationing of social assistance receipt and “welfare dependency” in Ontario, Canada. Social Problems. https://doi.org/10.1093/socpro/spz032
Gentil, L., Grenier, G., Bamvita, J. M., Dorvil, H., & Fleury, M. J. (2019). Profiles of quality of life in a homeless population. Frontiers in Psychiatry, 10, 10. https://doi.org/10.3389/fpsyt.2019.00010
Gentil, L., Grenier, G., Bamvita, J. M., & Fleury, M. (2020). Satisfaction with health and community services among homeless and formerly homeless individuals in Quebec, Canada. Health & Social Care in the Community, 28(1), 22–33. https://doi.org/10.1111/hsc.12834
Gentil, L., Grenier, G., & Fleury, M. J. (2021). Determinants of suicidal ideation and suicide attempt among former and currently homeless individuals. Social Psychiatry and Psychiatric Epidemiology, 56(5), 747–757. https://doi.org/10.1007/s00127-020-01952-3
Gicas, K. M., Cheng, A., Panenka, W. J., Kim, D. D., Yau, J. C., Procyshyn, R. M., … Barr, A. M. (2021). Differential effects of cannabis exposure during early versus later adolescence on the expression of psychosis in homeless and precariously housed adults. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 106, 110084–110084. https://doi.org/10.1016/j.pnpbp.2020.110084
Giesbrecht, M., Stajduhar, K. I., Mollison, A., Pauly, B., Reimer-Kirkham, S., McNeil, R., … Rose, C. (2018). Hospitals, clinics, and palliative care units: Place-based experiences of formal healthcare settings by people experiencing structural vulnerability at the end-of-life. Health & Place, 53, 43–51. https://doi.org/10.1016/j.healthplace.2018.06.005
Gilmer, C., & Buccieri, K. (2020). Homeless patients associate clinician bias with suboptimal care for mental illness, addictions, and chronic pain. Journal of Primary Care & Community Health, 11. https://doi.org/10.1177/2150132720910289
Glauser, W. (2018). Should health care dollars be used to house the homeless? Canadian Medical Association Journal (CMAJ), 190(43), E1291–E1292. https://doi.org/10.1503/cmaj.109-5671
Global Social Service Workforce Alliance Case Management Interest Group. (2018). Core concepts and principles of effective case management: Approaches for the social service workforce. 1st Edition. Global Social Service Workforce Alliance. Core concepts and principles of effective case management
Goering, P., Veldhuizen, S., Watson, A., Adair, C., Kopp, B., Latimer, E., Nelson, G., MacNaughton, E., Streiner, D., & Aubry, T. (2014). National at home / chez soi final report. Calgary, AB: Mental Health Commission of Canada. National At Home/Chez Soi Final Report | The Homeless Hub
Goldman-Hasbun, J., Nosova, E., DeBeck, K., Dahlby, L., & Kerr, T. (2019). Food insufficiency is associated with depression among street-involved youth in a Canadian setting. Public Health Nutrition, 22(1), 115–121. https://doi.org/10.1017/S1368980018002574
Goldman‐Hasbun, J., Nosova, E., Kerr, T., Wood, E., & DeBeck, K. (2019). Homelessness and incarceration associated with relapse into stimulant and opioid use among youth who are street‐involved in Vancouver, Canada. Drug and Alcohol Review, 38(4), 428–434. https://doi.org/10.1111/dar.12921
Government of British Columbia. (n.d.). B.C.’s mental health reform, assertive community treatment best practices. BC, Government of British Columbia, Ministry of Health and Ministry Responsible for Seniors. Assertive Community Treatment Guidelines for BC (gov.bc.ca)
Government of Canada. (2016). The new Canadian drugs and substances strategy. Canada. The New Canadian Drugs and Substances Strategy – Canada.ca
Government of Canada. (2017). A place to call home: Canada’s national housing strategy. Government of Canada, Ottawa. Canada’s National Housing Strategy (placetocallhome.ca)
Government of Canada. (2018). Reaching home: Canada’s homelessness strategy directives. Government of Canada, Ottawa. Reaching Home: Canada’s Homelessness Strategy Directives – Canada.ca
Government of Canada. (2019). National housing strategy act. Government of Canada, Ottawa. National Housing Strategy Act (justice.gc.ca)
Government of Canada. (2021a). Cannabis legalization and regulation. Canada. Cannabis Legalization and Regulation (justice.gc.ca)
Government of Canada. (2021b). Controlled drugs and substances act. Canada. Controlled Drugs and Substances Act (justice.gc.ca)
Government of Canada. (2021c). Good Samaritan drug overdose act. Canada. Good Samaritan Drug Overdose Act (justice.gc.ca)
Greene, J. (2014). Urban restructuring, homelessness, and collective action in Toronto, 1980–2003. Urban History Review, 43(1), 21–37. https://doi.org/10.7202/1030805ar
Greenwood, M. & Lindsay N. M. A. (2019). A commentary on land, health and Indigenous knowledge(s). Global Health Promotion, 26(3), 82-86. https://doi.org/10.1177/1757975919831262
Greer, A., Buxton, J. A., Pauly, B., & Bungay, V. (2021). Organizational support for frontline harm reduction and systems navigation work among workers with living and lived experience: qualitative findings from British Columbia, Canada. Harm Reduction Journal, 18(1), 60. https://doi.org/10.1186/s12954-021-00507-2
Guirguis-Younger, M., McNeil, R., & Hwang, S. W. (Eds.). (2014). Homelessness and health in Canada. Ottawa: University of Ottawa Press. Homelessness and Health in Canada (uottawa.ca)
Hainstock, M., & Masuda, J. R. (2019). “We have a roof over our head, but we have to eat too:” Exploring shifting foodscapes from homelessness into Housing First in Kingston, Ontario. Health & Place, 59, 102197–102197. https://doi.org/10.1016/j.healthplace.2019.102197
Hardill, K. (2007). From the grey nuns to the streets: A critical history of outreach nursing in Canada. Public Health Nursing, 24(1), 91–97. https://doi.org/10.1111/j.1525-1446.2006.00612.x
Harris, M., Gadermann, A., Norena, M., To, M., Hubley, A. M., Aubry, T., Hwang, S. W., & Palepu, A. (2019). Residential moves and its association with substance use, healthcare needs, and acute care use among homeless and vulnerably housed persons in Canada. International Journal of Public Health, 64(3), 399–409. https://doi.org/10.1007/s00038-018-1167-6
Hasford, J., Amponsah, P., & Hylton, T. (2018). (2018). Anti-racist praxis with street-involved African Canadian youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Hasford, J., Nelson, G., Worton, S. K., Macnaughton, E., MacLeod, T., Piat, M., Tsemberis, S., Stergiopoulos, V., Distasio, J., Aubry, T., & Goering, P. (2019). Knowledge translation and implementation of housing first in Canada: A qualitative assessment of capacity building needs for an evidence-based program. Evaluation and Program Planning, 75, 1–9. https://doi.org/10.1016/j.evalprogplan.2019.03.001
Henry, R. (2015). My life story, my youth. In Inclusion Working Group, Canadian Observatory on Homelessness (Eds.). Toronto, ON: Homeless Hub. Chapter 6: My Life Story My Youth.pdf
Hinds, A. M., Bechtel, B., Distasio, J., Roos, L. L., & Lix, L. M. (2018). Changes in healthcare use among individuals who move into public housing: a population-based investigation. BMC Health Services Research, 18(1), 411–411. https://doi.org/10.1186/s12913-018-3109-7
Hopper, E. K., Olivet, J., & Bassuk, E. L. (2018). Trauma-informed care for street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Hossain, R., Ramsay, N., Moore, M., & Milo, M. (2018). Health advocacy training through research‐based theatre. Medical Education, 52(11), 1187–1188. https://doi.org/10.1111/medu.13703
Huey, L., & Ferguson, L. (2020). “Did not return in time for curfew”: A descriptive analysis of homeless missing persons cases. International Criminal Justice Review, 105756772091864–. https://doi.org/10.1177/1057567720918640
Humphries, J., & Canham, S. L. (2021). Conceptualizing the shelter and housing needs and solutions of homeless older adults. Housing Studies, 36(2), 157–179. https://doi.org/10.1080/02673037.2019.1687854
Huynh, L., Henry, B., & Dosani, N. (2015). Minding the gap: Access to palliative care and the homeless. BMC Palliative Care, 14, 62. https://doi.org/10.1186/s12904-015-0059-2
Hwang, S. W. (2001). Homelessness and health. CMAJ, 164(2), 229-233. 229.full.pdf (cmaj.ca)
Hwang, S. W., Wilkins, R., Tjepkema, M., O’Campo, P. J., & Dunn, J. R. (2009). Mortality among residents of shelters, rooming houses, and hotels in Canada: 11 year follow-up study. BMJ, 339. doi: https://doi.org/10.1136/bmj.b4036
Ion, A., Greene, J., Masching, R., Poitras, M., Brownlee, P., St. Denys, R., … Anaquod, J. (2018). Stable homes, strong families: reimagining housing policies and programs for Indigenous peoples living with and affected by HIV and AIDS in Canada. Housing and Society, 45(2), 118–138. https://doi.org/10.1080/08882746.2018.1496696
Isaak, C. A., Reynolds, K., Sareen, J., & Distasio, J. (2019). The entrepreneurship of survival among urban adults experiencing homelessness and mental illness. Journal of Community Psychology, 47(6), 1548–1562. https://doi.org/10.1002/jcop.22204
Ivsins, A., Pauly, B., Brown, M., Evans, J., Gray, E., Schiff, R., … Stockwell, T. (2019). On the outside looking in: Finding a place for managed alcohol programs in the harm reduction movement. The International Journal of Drug Policy, 67, 58–62. https://doi.org/10.1016/j.drugpo.2019.02.004
Jadidzadeh, A., & Falvo, N. (2019). Patterns of exits from housing in a homelessness system of care: the case of Calgary, Alberta. Housing Studies, 34(1), 66–91. https://doi.org/10.1080/02673037.2018.1432755
Jadidzadeh, A., Falvo, N., & Dutton, D. J. (2020). Cost savings of Housing First in a non-experimental setting. Canadian Public Policy, 46(1), 23–36. https://doi.org/10.3138/cpp.2019-017
Jadidzadeh, A., & Kneebone, R. (2018). Patterns and intensity of use of homeless shelters in Toronto. Canadian Public Policy, 44(4), 342–355. https://doi.org/10.3138/cpp.2018-013
Jaworsky, D., Gadermann, A., Duhoux, A., Naismith, T. E., Norerna, M., To, M. J., Hwang, S. W., & Palepu, A. (2016). Residential stability reduces unmet health care needs and emergency department utilization among a cohort of homeless and vulnerably housed persons in Canada. Journal of Urban Health, 93, 666-681. https://doi.org/10.1007/s11524-016-0065-6
Jenkinson, J. I. R., Strike, C., Hwang, S. W., & Di Ruggiero, E. (2020). Legal, geographic and organizational contexts that shape knowledge sharing in the hospital discharge process for people experiencing homelessness in Toronto, Canada. Health & Social Care in the Community. Early View. https://doi.org/10.1111/hsc.13206
Jenkinson, J. I. R., Strike, C., Hwang, S. W. & Di Ruggiero, E. (2021). Nowhere to go: Exploring the social and economic influences on discharging people experiencing homelessness to appropriate destinations in Toronto, Canada. Canadian Journal of Public Health, 112, 992–1001. https://doi.org/10.17269/s41997-021-00561-0
Jiang, S., Mikhail, M., Slomovic, J., Pereira, A., Lebovic, G., Noel, C., & Lichter, M. (2020). Prevalence and impact of eye disease in an urban homeless and marginally housed population. Canadian Journal of Ophthalmology, 55(1), 76–81. https://doi.org/10.1016/j.jcjo.2019.07.006
Johnstone, M., Lee, E., & Connelly, J. (2017). Understanding the meta-discourse driving homeless policies and programs in Toronto, Canada: The neoliberal management of social service delivery. International Social Work, 60(6), 1443–1456. https://doi.org/10.1177/0020872817706406
Joly, L. E., & Connolly, J. (2019). It can be beautiful or destructive: Street-involved youth’s perceptions of their romantic relationships and resilience. Journal of Adolescence, 70, 43–52. https://doi.org/10.1016/j.adolescence.2018.11.006
Jones, P. W., Thornton, A. E., Jones, A. A., Knerich, V. M., Lang, D. J., Woodward, M. L., … Gicas, K. M. (2020). Amygdala nuclei volumes are selectively associated with social network size in homeless and precariously housed persons. Frontiers in Behavioral Neuroscience, 14, 97–97. https://doi.org/10.3389/fnbeh.2020.00097
Jones, T., & Ellis, J. (2017). It’s a kiki…. In A. Abramovich, & J. Shelton (eds.), Where Am I Going to Go? Intersectional Approaches to Ending LGBTQ2S Youth Homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
3
Kahan, D., Lamanna, D., Rajakulendran, T., Noble, A., & Stergiopoulos, V. (2020). Implementing a trauma‐informed intervention for homeless female survivors of gender‐based violence: Lessons learned in a large Canadian urban centre. Health & Social Care in the Community, 28(3), 823–832. https://doi.org/10.1111/hsc.12913
Kaltsidis, G., Grenier, G., Cao, Z., & Fleury, M. J. (2020). Change in housing status among homeless and formerly homeless individuals in Quebec, Canada: A profile study. International Journal of Environmental Research and Public Health, 17(17), 6254. https://doi.org/10.3390/ijerph17176254
Karabanow, J., Hughes, J., Kidd, S., & Frederick, T. (2018). Homeless youth and the search for stability. Wilfrid Laurier University Press. Project MUSE
Karamouzian, M., Cheng, T., Nosova, E., Sedgemore, K., Shoveller, J., Kerr, T., & Debeck, K. (2019). Perceived devaluation among a cohort of street-involved youth in Vancouver, Canada. Substance Use & Misuse, 54(2), 324–330. https://doi.org/10.1080/10826084.2018.1523193
Karamouzian, M., Dohoo, C., Forsting, S., McNeil, R., Kerr, T., & Lysyshyn, M. (2018). Evaluation of a fentanyl drug checking service for clients of a supervised injection facility, Vancouver, Canada. Harm Reduction Journal, 15(1), 46–46. https://doi.org/10.1186/s12954-018-0252-8
Katz, A. S., Brisbois, B., Zerger, S., & Hwang, S. W. (2018). Social impact bonds as a funding method for health and social programs: Potential areas of concern. American Journal of Public Health, 108(2), 210–215. https://doi.org/10.2105/AJPH.2017.304157
Kaufman, D. F. (2020a). Canadian homeless mobilities: Tracing the inter-regional movements of at home / chez soi participants. The Canadian Geographer, 65(3), 292-305. https://doi.org/10.1111/cag.12658
Kaufman, D. (2020b). Expulsion: A type of forced mobility experienced by homeless people in Canada. Urban Geography, 1–23. https://doi.org/10.1080/02723638.2020.1853919
Kelly, K., & Caputo, T. (2007). Health and street/homeless youth. Journal of Health Psychology, 12(5), 726-736. https://doi.org/10.1177/1359105307080594
Kennedy, M. C., Boyd, J., Mayer, S., Collins, A., Kerr, T., & McNeil, R. (2019). Peer worker involvement in low-threshold supervised consumption facilities in the context of an overdose epidemic in Vancouver, Canada. Social Science & Medicine (1982), 225, 60–68. https://doi.org/10.1016/j.socscimed.2019.02.014
Kennedy, M. C., Klassen, D. C., Dong, H., Milloy, M.-J. S., Hayashi, K., & Kerr, T. H. (2019). Supervised injection facility utilization patterns: A prospective cohort study in Vancouver, Canada. American Journal of Preventive Medicine, 57(3), 330–337. https://doi.org/10.1016/j.amepre.2019.04.024
Kennedy, M. C., Scheim, A., Rachlis, B., Mitra, S., Bardwell, G., Rourke, S., & Kerr, T. (2018). Willingness to use drug checking within future supervised injection services among people who inject drugs in a mid-sized Canadian city. Drug and Alcohol Dependence, 185, 248–252. https://doi.org/10.1016/j.drugalcdep.2017.12.026
Kennelly, J. (2020). Urban masculinity, contested spaces, and classed subcultures: young homeless men navigating downtown Ottawa, Canada. Gender, Place and Culture: A Journal of Feminist Geography, 27(2), 281–300. https://doi.org/10.1080/0966369X.2019.1650724
Kerman, N., Aubry, T., Adair, C. E., Distasio, J, Latimer, E., Somers, J., & Stergiopoulos, V. (2020). Effectiveness of housing first for homeless adults with mental illness who frequently use emergency departments in a multisite randomized controlled trial. Administration and Policy in Mental Health Services Research, 47, 515-525. https://doi.org/10.1007/s10488-020-01008-3
Kerman, N., Ecker, J., Gaetz, S., Tiderington, E., & Kidd, S. A. (2021). Mental health and wellness of service providers working with people experiencing homelessness in Canada: A national survey from the second wave of the COVID-19 Pandemic. The Canadian Journal of Psychiatry, 1-9. https://doi.org/10.1177/07067437211018782
Kerman, N., Gran-Ruaz, S., & Lem, M. (2019). Pet ownership and homelessness: a scoping review. Journal of Social Distress and the Homeless, 28(2), 106–114. https://doi.org/10.1080/10530789.2019.1650325
Kerman, N., & Kidd, S. A. (2020). The healthcare triple aim in the recovery era. Administration and Policy in Mental Health and Mental Health Services Research, 47, 492-496. https://doi.org/10.1007/s10488-019-00997-0
Kerman, N., Lem, M., Witte, M., Kim, C., & Rhoades, H. (2020). A multilevel intervention framework for supporting people experiencing homelessness with pets. Animals (Basel), 10(10), 1869. https://doi.org/10.3390/ani10101869
Kerman, N., & Sylvestre, J. (2020). Surviving versus living life: Capabilities and service use among adults with mental health problems and histories of homelessness. Health & Social Care in the Community, 28(2), 414–422. https://doi.org/10.1111/hsc.12873
Kerman, N., Sylvestre, J., Aubry, T., & Distasio, J. (2018). The effects of housing stability on service use among homeless adults with mental illness in a randomized controlled trial of housing first. BMC Health Services Research, 18(1), 190–190. https://doi.org/10.1186/s12913-018-3028-7
Kerman, N., Sylvestre, J., Aubry, T., & Schütz, C. G. (2019). Predictors of mental health recovery in homeless adults with mental illness. Community Mental Health Journal, 55(4), 631–640. https://doi.org/10.1007/s10597-018-0356-3
Kerr, T., Mitra, S., Kennedy, M. C., & McNeil, R. (2017). Supervised injection facilities in Canada: past, present, and future. Harm reduction journal, 14(1), 28. https://doi.org/10.1186/s12954-017-0154-1
Khandor, E., Mason, K., Chambers, C., Rossiter, K., Cowan, L., & Hwang, S. W. (2011). Access to primary health care among homeless adults in Toronto, Canada: Results from the street health survey. Open Med, 5(2), e94-e103. PMID: 21915240
Kidd, S. A., Gaetz, S., & O’Grady, B. (2017). The 2015 national Canadian homeless youth survey: Mental health and addiction findings. The Canadian Journal of Psychiatry, 62(7), 493-500. https://doi.org/10.1177/0706743717702076
Kidd, S. A., Gaetz, S., O’Grady, B., Schwan, K., Zhao, H., Lopes, K., & Wang, W. (2021). The second national Canadian homeless youth survey: Mental health and addiction findings. The Canadian Journal of Psychiatry, 66(10), 897-905. https://doi.org/10.1177%2F0706743721990310
Kidd, S. A., Greco, S. & McKenzie, K. (2021). Global climate implications for homelessness: A scoping review. J Urban Health, 98, 385–393. https://doi.org/10.1007/s11524-020-00483-1
Kidd, S., Thistle, J., Beaulieu, T., O’Grady, B., & Gaetz, S. (2019). A national study of Indigenous youth homelessness in Canada. Public Health (London), 176, 163–171. https://doi.org/10.1016/j.puhe.2018.06.012
Kidd, S. A., Vitopoulos, N., Frederick, T., Daley, M., Peters, K., Clarc, K., … McKenzie, K. (2019). Peer support in the homeless youth context: Requirements, design, and outcomes. Child & Adolescent Social Work Journal, 36(6), 641–654. https://doi.org/10.1007/s10560-019-00610-1
Kidd, S. A., Vitopoulos, N., Frederick, T., Leon, S., Karabanow, J., & McKenzie, K. (2019). More than four walls and a roof needed: A complex tertiary prevention approach for recently homeless youth. American Journal of Orthopsychiatry, 89(2), 248–257. https://doi.org/10.1037/ort0000335
Kidd, S. A., Vitopoulos, N., Frederick, T., Leon, S., Wang, W., Mushquash, C., & McKenzie, K. (2020). Trialing the feasibility of a critical time intervention for youth transitioning out of homelessness. American Journal of Orthopsychiatry, 90(5), 535–545. https://doi.org/10.1037/ort0000454
Kiran, T., Craig-Neil, A., Das, P., Lockwood, J., Wang, R., Nathanielsz, N., … Hwang, S. W. (2021). Factors associated with SARS-CoV-2 positivity in 20 homeless shelters in Toronto, Canada, from April to July 2020: a repeated cross-sectional study. CMAJ Open, 9(1), E302–E308. https://doi.org/10.9778/cmajo.20200253
Kirst, M., Friesdorf, R., Ta, M., Amiri, A., Hwang, S. W., Stergiopoulos, V., & O’Campo, P. (2020). Patterns and effects of social integration on housing stability, mental health and substance use outcomes among participants in a randomized controlled Housing First trial. Social Science & Medicine (1982), 265, 113481–113481. https://doi.org/10.1016/j.socscimed.2020.113481
Kitson, C., & O’Byrne, P. (2020). The experience of violence against women who use injection drugs: An exploratory qualitative study. Canadian Journal of Nursing Research, 340-352. https://doi.org/10.1177/0844562120979577
Klimas, J., Nosova, E., Socías, E., Nolan, S., Brar, R., Hayashi, K., … Wood, E. (2018). Factors associated with discontinuation of methadone maintenance therapy (MMT) among persons who use alcohol in Vancouver, Canada. Drug and Alcohol Dependence, 186, 182–186. https://doi.org/10.1016/j.drugalcdep.2018.01.027
Koch, J., Scherer, J., & Holt, N. (2018). Slap shot! Sport, masculinities, and homelessness in the downtown core of a divided western Canadian inner city. Journal of Sport and Social Issues, 42(4), 270–294. https://doi.org/10.1177/0193723518773280
Kolahdooz, F., Nader, F., Yi, K. J., & Sharma, S. (2015). Understanding the social determinants of health among Indigenous Canadians: Priorities for health promotion policies and actions. Global Health Action, 8(1), 27968–27968. https://doi.org/10.3402/gha.v8.27968
Kouyoumdjian, F. G., Wang R., Mejia-Lancheros, C., Owusu-Bempah, A., Nisenbaum, R., O’Campo, P., Stergiopoulos, V., & Hwang, S. W. (2019). Interactions between police and persons who experience homelessness and mental illness in Toronto, Canada: Findings from a prospective study. The Canadian Journal of Psychiatry, 64(10),718-725. 10.1177/0706743719861386
Kozloff, N., Bergmans, Y., Snider, C., Langley, J., & Stergiopoulos, V. (2018). Crisis response with street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Krüsi, A., Kerr, T., Taylor, C., Rhodes, T., & Shannon, K. (2016). “They won’t change it back in their heads that we’re trash’: The intersection of sex work‐related stigma and evolving policing strategies. Sociology of Health & Illness, 38(7), 1137–1150. https://doi.org/10.1111/1467-9566.12436
Lake, S., Kerr, T., Nosova, E., Milloy, M. J., Wood, E., & DeBeck, K. (2018). Patterns of non-injection drug use associated with injection cessation among street-involved youth in Vancouver, Canada. Journal of Urban Health, 95(2), 267–277. https://doi.org/10.1007/s11524-017-0225-3
Laliberté, V., Stergiopoulos, V., Jacob, B., & Kurdyak, P. (2019). Homelessness at discharge and its impact on psychiatric readmission and physician follow-up: a population-based cohort study. Epidemiology and Psychiatric Sciences, 29, e21–e21. https://doi.org/10.1017/S2045796019000052
Lamanna, D., Stergiopoulos, V., Durbin, J., O’Campo, P., Poremski, D., & Tepper, J. (2018). Promoting continuity of care for homeless adults with unmet health needs: The role of brief interventions. Health & Social Care in the Community, 26(1), 56–64. https://doi.org/10.1111/hsc.12461
Latimer, E. A., Rabouin, D., Cao, Z., Ly, A., Powell, G., Adair, C. E., … Veldhuizen, S. R. (2019). Cost-effectiveness of Housing First Intervention With Intensive Case Management Compared With Treatment as Usual for Homeless Adults With Mental Illness: Secondary Analysis of a Randomized Clinical Trial. JAMA Network Open, 2(8), e199782–e199782. https://doi.org/10.1001/jamanetworkopen.2019.9782
Latimer, E. A., Rabouin, D., Cao, Z., Ly, A., Powell, G., Aubry, T., Hwang, S. W.,… Goering, P. N. (2017). Costs of services for homeless people with mental illness in 5 Canadian cities: a large prospective follow-up study. CMAJ Open, 5(3), E576–E585. https://doi.org/10.9778/cmajo.20170018
Lawrie, K., Charow, R., Giuliani, M., & Papadakos, J. (2020). Homelessness, cancer and health literacy: A scoping review. Journal of Health Care for the Poor and Underserved, 31(1), 81–104. https://doi.org/10.1353/hpu.2020.0010
Leger, P., Hamilton, A., Bahji, A., & Martell, D. on behalf of the CSAM Policy Committee. (2021). Policy brief: CSAM in support of the decriminalization of drug use and possession for personal use. The Canadian Journal of Addiction, 12(1), 13-15. Policy Brief: CSAM in Support of the Decriminalization of Dr… : Canadian Journal of Addiction (lww.com)
Lem, M. (2019). Serving homeless populations through a one health approach. Canadian Veterinary Journal, 60(10), 1119–1120. https://europepmc.org/article/PMC/PMC6741821
Lemieux, A. J., Leclair, M. C., Roy, L., Nicholls, T. L., & Crocker, A. G. (2020). A typology of lifetime criminal justice involvement among homeless individuals with mental illness: Identifying needs to better target intervention. Criminal Justice and Behavior, 47(7), 790–807. https://doi.org/10.1177/0093854819900305
Leung, A. K., To, M. J., Luong, L., Vahabi, Z. S., Gonçalves, V. L., Song, J., & Hwang, S. W. (2017). The effect of advance directive completion on hospital care among chronically homeless persons: A prospective cohort study. Journal of Urban Health, 94(1), 43–53. https://doi.org/10.1007/s11524-016-0105-2
Lévesque, I. S., & Abdel-Baki, A. (2020). Homeless youth with first-episode psychosis: A 2-year outcome study. Schizophrenia Research, 216, 460–469. https://doi.org/10.1016/j.schres.2019.10.031
Liu, M., & Hwang, S. W. (2021). Health care for homeless people. Nature Reviews Disease Primers 7, 5. https://doi.org/10.1038/s41572-020-00241-2
Liu, M., Mejia-Lancheros, C., Lachaud, J., Latimer, E., Aubry, T., Somers, J., … Hwang, S. W. (2021). Overall and gender-specific associations between dimensions of adverse childhood experiences and mental health outcomes among homeless adults. Canadian Journal of Psychiatry, 706743721989158–706743721989158. https://doi.org/10.1177/0706743721989158
Lo, A., Kerr, T., Hayashi, K., Milloy, M. J., Nosova, E., Liu, Y., & Fairbairn, N. (2018). Factors associated with methadone maintenance therapy discontinuation among people who inject drugs. Journal of Substance Abuse Treatment, 94, 41–46. https://doi.org/10.1016/j.jsat.2018.08.009
Luongo, N. M. (2018). Disappearing in plain sight: An exploratory study of co-occurring eating and substance abuse dis/orders among homeless youth in Vancouver, Canada. Women’s Studies International Forum, 67, 38–44. https://doi.org/10.1016/j.wsif.2018.01.003
MacDonald, S. A., & Gaulin, D. (2020). The invisibility of rural homelessness in a Canadian context. Journal of Social Distress and Homelessness, 29(2), 169-183. 10.1080/10530789.2019.1688540
Macnaughton, E., Nelson, G., Worton, S. K., Tsemberis, S., Stergiopoulos, V., Aubry, T., … Goering, P. (2018). Navigating complex implementation contexts: Overcoming barriers and achieving outcomes in a national initiative to scale out Housing First in Canada. American Journal of Community Psychology, 62(1-2), 135–149. https://doi.org/10.1002/ajcp.12268
Magee, C., Norena, M., Hubley, A. M., Palepu, A., Hwang, S. W., Nisenbaum, R., … Gadermann, A. (2019). Longitudinal associations between perceived quality of living spaces and health-related quality of life among homeless and vulnerably housed individuals living in three Canadian cities. International Journal of Environmental Research and Public Health, 16(23), 4808. https://doi.org/10.3390/ijerph16234808
Magnan‐Tremblay, L., Lanctôt, N., & Couvrette, A. (2020). The hopelessness effect: Counsellors’ perceptions of their female clients involved in sex work in Canada. Health & Social Care in the Community, 28(5), 1430–1437. https://doi.org/10.1111/hsc.12993
Mago, A., Brondani, M. A., MacEntee, M. I., & Frankish, C. J. (2018). A model pathway to oral health care for homeless people. J Can Dent Assoc, 84, i10. https://pubmed.ncbi.nlm.nih.gov/31199725/
Magwood, O., Hanemaayer, A., Saad, A., Salvalaggio, G., Bloch, G., Moledina, A., Pinto, N., Ziha, L., Geurguis, M., Aliferis, A., Kpade, V., Arya, N., Aubry, T., & Pottie, K. (2020). Determinants of implementation of a clinical practice guideline for homeless health. International Journal of Environmental Research and Public Health, 17(21), 7938. https://doi.org/10.3390/ijerph17217938
Maina, G., Crizzle, A., Maposa, S., & Fournier, B. (2019). Sociodemographic profiles and clinical outcomes for clients on methadone maintenance treatment in a western Canadian clinic: Implications for practice. Journal of Forensic Nursing, 15(4), 231. DOI:10.1097/JFN.0000000000000246
Malenfant, J. A., Nichols, N., & Schwan, K. (2019). Chasing funding “to eat our own tail”: The invisible emotional work of making social change. Canadian Journal of Nonprofit and Social Economy Research, 10(2). https://doi.org/10.29173/cjnser.2019v10n2a307Malla, A., Iyer, S., Shah, J., Joober, R., Boksa, P., Lal, S., … Vallianatos, H. (2019). Canadian response to need for transformation of youth mental health services: ACCESS Open Minds (Esprits ouverts). Early Intervention in Psychiatry, 13(3), 697–706. https://doi.org/10.1111/eip.12772
Mamdani, Z., McKenzie, S., Pauly, B., Cameron, F., Conway-Brown, J., Edwards, D., Howell, A., Scott, T., Seguin, R., Woodrow, P., & Buxton, J. A. (2021). “Running myself ragged”: stressors faced by peer workers in overdose response settings. Harm Reduction Journal, 18(1), 18. https://doi.org/10.1186/s12954-020-00449-1
Maremmani, A. G., Bacciardi, S., Gehring, N. D., Cambioli, L., Schütz, C., Jang, K., & Krausz, M. (2017). Substance use among homeless individuals with schizophrenia and bipolar disorder. The Journal of Nervous and Mental Disease, 205(3), 173–177. https://doi.org/10.1097/NMD.0000000000000462
Maremmani, A. G. I., Bacciardi, S., Somers, J. M., Nikoo, M., Schütz, C., Jang, K. L., & Krausz, M. (2018). Substance dependence among bipolar, unipolar depression and psychotic homeless: A Canadian national study. Frontiers in Psychiatry, 9, 701–701. https://doi.org/10.3389/fpsyt.2018.00701
Marsella, O., Forchuk, C., & Oudshoorn, A. (2020). Exploring harm reduction among Canadian veterans experiencing homelessness. Journal of Military, Veteran and Family Health, 6(2), 17–25. https://doi.org/10.3138/jmvfh-2019-0042
Marshall, C. A., Boland, L., Westover, L. A., Marcellus, B., Weil, S., & Wickett, S. (2020). Effectiveness of interventions targeting community integration among individuals with lived experiences of homelessness: A systematic review. Health & Social Care in the Community, 28(6), 1843–1862. https://doi.org/10.1111/hsc.13030
Marshall, C. A., Keogh-Lim, D., Koop, M., Barbic, S., & Gewurtz, R. (2020a). Meaningful activity and boredom in the transition from homelessness: Two narratives. Canadian Journal of Occupational Therapy (1939), 87(4), 253–264. https://doi.org/10.1177/0008417420941782
Marshall, C. A., Roy, L., Becker, A., Nguyen, M., Barbic, S., Tjörnstrand, C., … Wickett, S. (2020b). Boredom and homelessness: A scoping review. Journal of Occupational Science, 27(1), 107–124. https://doi.org/10.1080/14427591.2019.1595095
McCay, E., & Aiello, A. (2018). Dialectical behaviour therapy to enhance emotional regulation and resilience among street-involved youth. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
McCready, L. T. (2017). Black queer youth, unstable housing and homelessness: Understanding the impact of family conflict, school and community-based violence on racialized LGBTQ2S youth. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
McNeil, R., Fleming, T., Collins, A. B., Czechaczek, S., Mayer, S., & Boyd, J. (2021). Navigating post-eviction drug use amidst a changing drug supply: A spatially-oriented qualitative study of overlapping housing and overdose crises in Vancouver, Canada. Drug and Alcohol Dependence, 222. https://doi.org/10.1016/j.drugalcdep.2021.108666
McParland, K., Rousseau-Thomas, J., & Waegemakers Schiff, J. (2019). A critical review of research and policy in youth-focussed Housing First. Canadian Review of Social Policy (1987), 79, 50–.
Mejia-Lancheros, C., Lachaud, J., Nisenbaum, R., Wang, A., Stergiopoulos, V., Hwang, S. W., & O’Campo, P. (2020a). Dental problems and chronic diseases in mentally ill homeless adults: a cross-sectional study. BMC Public Health, 20(1), 419. https://doi.org/10.1186/s12889-020-08499-7
Mejia-Lancheros, C., Lachaud, J., O’Campo, P., Wiens, K., Nisenbaum, R., Wang, R., Hwang, S. W., & Stergiopoulos, V. (2020) Trajectories and mental health-related predictors of perceived discrimination and stigma among homeless adults with mental illness. PLoS ONE, 15(2), e0229385. https://doi.org/10.1371/journal.pone.0229385
Mejia-Lancheros, C., Lachaud, J., Stergiopoulos, V., Matheson, F. I., Nisenbaum, R., O’Campo, P., & Hwang, S. W. (2020). Effect of Housing First on violence-related traumatic brain injury in adults with experiences of homelessness and mental illness: findings from the At Home/Chez Soi randomised trial, Toronto site. BMJ Open, 10(12), e038443–e038443. https://doi.org/10.1136/bmjopen-2020-038443
Mejia-Lancheros, C., Lachaud, J., Woodhall-Melnik, J., O’Campo, P., Hwang, S. W., & Stergiopoulos, V. (2021). Longitudinal interrelationships of mental health discrimination and stigma with housing and well-being outcomes in adults with mental illness and recent experience of homelessness. Social Science & Medicine (1982), 268, 113463–113463. https://doi.org/10.1016/j.socscimed.2020.113463
Merdsoy, L., Lambert, S., & Sherman, J. (2020). Perceptions, needs and preferences of chronic disease self‐management support among men experiencing homelessness in Montreal. Health Expectations: An International Journal of Public Participation in Health Care and Health Policy, 23(6), 1420–1430. https://doi.org/10.1111/hex.13106
Meyer, J. P., Isaacs, K., El-Shahawy, O., Burlew, A. K., & Wechsberg, W. (2019). Research on women with substance use disorders: Reviewing progress and developing a research and implementation roadmap. Drug and Alcohol Dependence, 197, 158–163. https://doi.org/10.1016/j.drugalcdep.2019.01.017
Milaney, K., Kamran, H., & Williams, N. (2020). A portrait of late life homelessness in Calgary, Alberta. Canadian Journal on Aging, 39(1), 42–51. https://doi.org/10.1017/S0714980819000229
Milaney, K., Lockerbie, S. L., Fang, X. Y., & Ramage, K. (2019). The role of structural violence in family homelessness. Canadian Journal of Public Health, 110(5), 554–562. https://doi.org/10.17269/s41997-019-00219-y
Milaney, K., Williams, N., Lockerbie, S. L., Dutton, D. J., & Hyshka, E. (2020). Recognizing and responding to women experiencing homelessness with gendered and trauma-informed care. BMC Public Health, 20(1), 397–397. https://doi.org/10.1186/s12889-020-8353-1
Miller, K., Bissoondial, K., & Morgan. (2017). YMCA Sprott House: Creating a better space for LGBTQ2S youth in Toronto. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Mills, C. W. (1967). The sociological imagination. London: Oxford University Press.
Montgomery, P., Mossey, S., & McCauley, K. (2019). Priorities for supportive housing services: Perspectives of people with mental illness in northeastern Ontario. Canadian Journal of Nursing Research, 51(4), 264–273. https://doi.org/10.1177/0844562119835730
Moravac, C. C. (2018). Reflections of homeless women and women with mental health challenges on breast and cervical cancer screening decisions: Power, trust, and communication with care providers. Frontiers in Public Health, 6, 30. https://doi.org/10.3389/fpubh.2018.00030
Morisseau-Guillot, R., Aubin, D., Deschênes, J.-M., Gioia, M., Malla, A., Bauco, P., … Abdel-Baki, A. (2020). A promising route towards improvement of homeless young people’s access to mental health services: The creation and evolution of an outreach service network in Montréal. Community Mental Health Journal, 56(2), 258–270. https://doi.org/10.1007/s10597-019-00456-y
Murnan, A., Zhang, J., & Slesnick, N. (2018). Ecologically based treatment for mothers experiencing homelessness who have children in their care. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Mutschler, C., Lichtenstein, S., Kidd, S.A. & Davidson, L. (2019). Transition experiences following psychiatric hospitalization: A systematic review of the literature. Community Mental Health Journal, 55, 1255–1274. https://doi.org/10.1007/s10597-019-00413-9
Nasmith, T. E., Gadermann, A., Jaworsky, D., Norena, M., To, M. J., Hwang, S. W., & Palepu, A. (2020). Clinically significant substance use and residential stability among homeless or vulnerably housed persons in Canada: a longitudinal cohort study. Journal of Public Health, 43(3), 532-540. https://doi.org/10.1093/pubmed/fdaa018
National Action Plan. (2021). 2021 missing and murdered Indigenous women, girls, and 2SLGBTQQIA+ people national action plan: Ending violence against Indigenous women, girls, and 2SLGBTQQIA+ people. Canada.
Nelson, G., Aubry, T., Tsemberis, S., & Macnaughton, E. (2020). Psychology and public policy: The story of a Canadian Housing First project for homeless people with mental illness. Canadian Psychology = Psychologie Canadienne, 61(3), 257–268. https://doi.org/10.1037/cap0000206
Nelson, G., Caplan, R., MacLeod, T., Macnaughton, E., Cherner, R., Aubry, T., … Goering, P. (2017). What happens after the demonstration phase? The sustainability of Canada’s At Home/Chez Soi Housing First programs for homeless persons with mental illness. American Journal of Community Psychology, 59(1-2), 144–157. https://doi.org/10.1002/ajcp.12119
Nichols, N. (2018). The social organization of access to justice for youth in “unsafe” urban neighbourhoods. Social & Legal Studies, 27(1), 79–96. https://doi.org/10.1177/0964663917703179
Nichols, N. (2019). Youth, school, and community: Participatory institutional ethnographies. Toronto: University of Toronto Press. https://doi.org/10.3138/9781487517724
Nichols, N., & Braimoh, J. (2018). Community safety, housing precariousness and processes of exclusion: An institutional ethnography from the standpoints of youth in an “unsafe” urban neighbourhood. Critical Sociology, 44(1), 157–172. https://doi.org/10.1177/0896920516658941
Nichols, N., Schwan, K., Gaetz, S., & Redman, M. (2021). Enabling evidence-led collaborative systems-change efforts: An adaption of the collective impact approach. Community Development Journal. https://doi.org/10.1093/cdj/bsab011
Nichols, N., Schwan, K., Gaetz, S., Redman, M., French, D., Kidd, S., O’Grady, B. (2017). Child welfare and youth homelessness in Canada: A proposal for action. Toronto: Canadian Observatory on Homelessness Press.
Nikoo, N., Javidanbardan, S., Akm, M., Hakobyan, S., Nikoo, M., Kwan, C., … Krausz, M. (2019). Hepatitis C prevalence and associated risk factors among individuals who are homeless and diagnosed with mental illness: At home / chez soi study, Vancouver, BC. European Journal of Public Health, 29(2), 242–247. https://doi.org/10.1093/eurpub/cky142
Noel, C. W., Mok, F., Wu, V., Eskander, A., Yao, C. M. K. L., Hwang, S. W., … Lee, J. M. (2020). Hearing loss and hearing needs in an adult homeless population: A prospective cross-sectional study. CMAJ Open, 8(1), E199–E204. https://doi.org/10.9778/cmajo.20190220
O’Grady, B., Gaetz, S., & Buccieri, K. (2011). Can I see your ID? The policing of youth homelessness in Toronto. Toronto: JFCY & Homeless Hub. CanISeeYourID_nov9.pdf (homelesshub.ca)
O’Grady, B., Gaetz, S., & Buccieri, K. (2013). Tickets… and more tickets: A case study of the Enforcement of the Ontario Safe Streets Act. Canadian Public Policy, 39(4), 541-558. https://www.muse.jhu.edu/article/534407
Olson, N., & Pauly, B. (2021). Homeless encampments: Connecting public health and human rights. Canadian Journal of Public Health, 112, 988-991. https://doi.org/10.17269/s41997-021-00581-w
Oosman, S., Weber, G., Ogunson, M., & Bath, B. (2019). Enhancing access to physical therapy services for people experiencing poverty and homelessness: The lighthouse pilot project. Physiotherapy Canada, 71(2), 176–186. https://doi.org/10.3138/ptc.2017-85.pc
Orchard, T., Murie, A., Elash, H. L., Bunch, M., Middleton, C., Sadakhom, D., … Benoit, C. (2019). “People like us”: Spatialised notions of health, stigma, power and subjectivity among women in street sex work. Culture, Health & Sexuality, 21(4), 478–494. https://doi.org/10.1080/13691058.2018.1490455
O’Reilly-Fleming, T. (1993). Down and out in Canada: Homeless Canadians. Toronto: Canadian Scholar’s Press.
O’Shea, T., Mbuagbaw, L., Mokashi, V., Bulir, D., Gilchrist, J., Smieja, N., … Smieja, M. (2020). Comparison of four COVID-19 screening strategies to facilitate early case identification within the homeless shelter population: A structured summary of a study protocol for a randomised controlled trial. Trials, 21(1), 941–941. https://doi.org/10.1186/s13063-020-04890-2
Oudshoorn, A., Benbow, S., Esses, V., Baker, L., Annor, B., Coplan, I., Shantz, J., & Ezukuse, V. (2020). Homelessness prevention for refugees: Results from an analysis of pathways to shelter. European Journal of Homelessness; 14(2), 189-205. EJH_14-2_WEB.pdf (feantsaresearch.org)
Oudshoorn, A., Dej, E., Parsons, C., & Gaetz, S. (2020). Evolving an evidence‐based model for homelessness prevention. Health & Social Care in the Community, 28(5), 1754–1763. https://doi.org/10.1111/hsc.13000
Oudshoorn, A., Forchuk, C., Hall, J., Smith-Carrier, T., & Van Berkum, A. (2018). An evaluation of a Housing First program for chronically homeless women. Journal of Social Inclusion, 9(2), 34–. https://doi.org/10.36251/josi.136
Oudshoorn, A., May, K., Van Berkum, A., Schwan, K., Nelson, A., Eiboff, F., K., Begun, S., Nichols, N., & Parsons, C. (2021). Exploring the presence of gender-based approaches to women’s homelessness in Canadian communities. Gender Based Approaches Report
O’Grady, B., Kidd, S., & Gaetz, S. (2020). Youth homelessness and self identity: a view from Canada. Journal of Youth Studies, 23(4), 499–510. https://doi.org/10.1080/13676261.2019.1621997
Pakhale, S., Kaur, T., Charron, C., Florence, K., Rose, T., Jama, S., … Tyndall, M. (2018). Management and point-of-care for tobacco dependence (PROMPT): A feasibility mixed methods community-based participatory action research project in Ottawa, Canada. BMJ Open, 8(1), e018416–e018416. https://doi.org/10.1136/bmjopen-2017-018416
Palayew, A., Kaur, H., Magwood, O., Greenaway, C., Mayhew, A., Hatcher-Roberts, J., & Pottie, K. (2018). P2‐112: Values, preferences, and acceptability of hepatitis C testing and treatment in the homeless and vulnerably housed: A scoping review. Journal of Viral Hepatitis, 25(S2), 163–164. https://doi.org/10.1111/jvh.229_12923
Paradis, E. (2016). Outsiders within: Claiming discursive space at national homelessness conferences in Canada. Social Inclusion, 4(4), 97–107. https://doi.org/10.17645/si.v4i4.670
Paradis, E., Wilson, R. M., & Logan, J. (2014). Nowhere else to go: Inadequate housing & risk of homelessness among families in Toronto’s aging rental buildings. Toronto, Ontario: Cities Centre, University of Toronto.
Paradis-Gagné, E., Pariseau-Legault, P., Villemure, M., & Chauvette, S. (2020). A critical ethnography of outreach nursing for people experiencing homelessness. Journal of Community Health Nursing, 37(4), 189–202. https://doi.org/10.1080/07370016.2020.1809858
Parkes, T., Matheson, C., Carver, H., Budd, J., Liddell, D., Wallace, J., … Foster, R. (2019). Supporting harm reduction through peer support (SHARPS): Testing the feasibility and acceptability of a peer-delivered, relational intervention for people with problem substance use who are homeless, to improve health outcomes, quality of life and social functioning and reduce: study protocol. Pilot and Feasibility Studies, 5(1), 64–64. https://doi.org/10.1186/s40814-019-0447-0
Parpouchi, M., Moniruzzaman, A., Rezansoff, S. N., Russolillo, A., & Somers, J. M. (2018). The effect of housing first on adherence to methadone maintenance treatment. The International Journal of Drug Policy, 56, 73–80. https://doi.org/10.1016/j.drugpo.2018.03.012
Parpouchi, M., Moniruzzaman, A., & Somers, J. M. (2021). The association between experiencing homelessness in childhood or youth and adult housing stability in housing first. BMC Psychiatry, 21(1), 138–138. https://doi.org/10.1186/s12888-021-03142-0
Patrick, C. (2014). Aboriginal homelessness in Canada: A literature review. Toronto: The Canadian Observatory on Homelessness.
Paul, S., Corneau, S., Boozary, T., & Stergiopoulos, V. (2018). Coping and resilience among ethnoracial individuals experiencing homelessness and mental illness. International Journal of Social Psychiatry, 64(2), 189–197. https://doi.org/10.1177/0020764017748986
Pauly, B., Brown, M., Chow, C., Wettlaufer, A., East Side Illicit Drinkers Group for Education, … & Sutherland, C. (2021). “If I knew I could get that every hour instead of alcohol, I would take the cannabis”: Need and feasibility of cannabis substitution implementation in Canadian managed alcohol programs. Harm Reduction Journal, 18, 65. https://doi.org/10.1186/s12954-021-00512-5
Pauly, B., Brown, M., Evans, J., Gray, E., Schiff, R., Ivsins, A., Krysowaty, B., Vallance, K., & Stockwell, T. (2019). “There is a Place”: Impacts of managed alcohol programs for people experiencing severe alcohol dependence and homelessness. Harm Reduction Journal, 16(1), 70–70. https://doi.org/10.1186/s12954-019-0332-4
Pauly, B., Mamdani, Z., Mesley, L., McKenzie, S., Cameron, F., Edwards, D., Howell, A., Knott, M., Scott, T., Seguin, R., Greer, A. M., & Buxton, J. A. (2021). “It’s an emotional roller coaster… But sometimes it’s fucking awesome”: Meaning and motivation of work for peers in overdose response environments in British Columbia. The International Journal on Drug Policy, 88, 103015. https://doi.org/10.1016/j.drugpo.2020.103015
Pauly, B., Perkin, K., & Cross, G. (2016). The case of Victoria, BC. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Pauly, B., Vallance, K., Wettlaufer, A., Chow, C., Brown, R., Evans, J., … Stockwell, T. (2018). Community managed alcohol programs in Canada: Overview of key dimensions and implementation. Drug and Alcohol Review, 37(S1), S132–S139. https://doi.org/10.1111/dar.12681
Perri, M., Dosani, N., & Hwang, S. W. (2020). COVID-19 and people experiencing homelessness: challenges and mitigation strategies. Canadian Medical Association Journal (CMAJ), 192(26), E716–E719. https://doi.org/10.1503/cmaj.200834
Pettey, D., & Aubry, T. (2018). Tobacco use and smoking behaviors of individuals with a serious mental illness. Psychiatric Rehabilitation Journal, 41(4), 356–360. https://doi.org/10.1037/prj0000302
Pijl, E. M., & Belanger, Y. D. (2020). Lost in transition: Entering the liminal space of rural homelessness in a small prairie town. Journal of Social Distress and Homeless, 1–9. https://doi.org/10.1080/10530789.2020.1763575
Polillo, A., Sylvestre, J., Kerman, N., Lee, C. M., Aubry, T., & Czechowski, K. (2018). The experiences of adolescents and young adults residing with their families in emergency shelters in Canada. Journal of Children & Poverty, 24(2), 89–107. https://doi.org/10.1080/10796126.2018.1470438
Ponka, D., Agbata, E., Kendall, C., Stergiopoulos, V., Mendonca, O., Magwood, O… & Pottie, K. (2020). The effectiveness of case management interventions for the homeless, vulnerably housed and persons with lived experience: A systematic review. PLoS ONE, 15(4): e0230896. https://doi.org/10.1371/journal.pone.0230896
Porter, B. (2021). Implementing the right to adequate housing under the national housing strategy act: The international human rights framework. Canada: The National Right to Housing Network. NRHN OFHA Report Cover 2021 (housingrights.ca)
Pottie, K., Kendall, C. E., Aubry, T., Magwood, O., Andermann, A., Salvalaggio, G., … Hwang, S. W., Stergiopoulos, V., & Tugwell, P. (2020). Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience. Canadian Medical Association Journal (CMAJ), 192(10), E240–E254. https://doi.org/10.1503/cmaj.190777
Purkey, E., & MacKenzie, M. (2019). Experience of healthcare among the homeless and vulnerably housed a qualitative study: opportunities for equity-oriented health care. International Journal for Equity in Health, 18(1), 101–101. https://doi.org/10.1186/s12939-019-1004-4
Quirouette, M., Frederick, T., Hughes, J., Karabanow, J., & Kidd, S. (2016). “Conflict with the law”: Regulation & homeless youth trajectories toward stability. Canadian Journal of Law and Society, 31(3), 383–404. https://doi.org/10.1017/cls.2016.26
Ramsay, N., Hossain, R., Moore, M., Milo, M., & Brown, A. (2019). Health care while homeless: Barriers, facilitators, and the lived experiences of homeless individuals accessing health care in a Canadian regional municipality. Qualitative Health Research, 29(13), 1839–1849. https://doi.org/10.1177/1049732319829434
Ranasinghe, P. & Valverde, M. (2006). Governing homelessness through land-use: A sociolegal study of the Toronto shelter zoning by-law. Canadian Journal of Sociology, 31(3), 325-349. https://www.jstor.org/stable/20058713
Raphael, D. (2016). Social determinants of health: A Canadian perspective, 2nd Edition. Toronto: Canadian Scholar’s Press.
Ratnam, C., Fitzpatrick, A., & Thang, H. (2018). Engaging with newcomer youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Reddon, H., DeBeck, K., Socias, M. E., Dong, H., Wood, E., Montaner, J., … Milloy, M. (2018). Cannabis use is associated with lower rates of initiation of injection drug use among street‐involved youth: A longitudinal analysis. Drug and Alcohol Review, 37(3), 421–428. https://doi.org/10.1111/dar.12667
Redden, M., Gahagan, J., Kia, H., Humble, Á. M., Stinchcombe, A., Manning, E., … Thomas, R. (2021). Housing as a determinant of health for older LGBT Canadians: Focus group findings from a national housing study. Housing and Society, 1–25. https://doi.org/10.1080/08882746.2021.1905996
Redvers, N., Nadeau, M., & Prince, D. (2020). Urban land-based healing: A northern intervention strategy. International Journal of Indigenous Health, 16(2), 322–337. https://doi.org/10.32799/ijih.v16i2.33177
Registered Nurses’ Association of Ontario. (2004). Position statement: Homelessness. RNAO: Ontario. https://rnao.ca/policy/position-statements/homelessness
Reid, N., Khan, B., Soklaridis, S., Kozloff, N., Brown, R., & Stergiopoulos, V. (2020). Mechanisms of change and participant outcomes in a recovery education centre for individuals transitioning from homelessness: A qualitative evaluation. BMC Public Health, 20(1), 497–497. https://doi.org/10.1186/s12889-020-08614-8
Reid, N., Kron, A., Lamanna, D., Wen, S., Durbin, A., Rajakulendran, T., … Stergiopoulos, V. (2021). Building bridges to housing for homeless adults with intellectual and developmental disabilities: Outcomes of a cross‐sector intervention. Journal of Applied Research in Intellectual Disabilities, 34(1), 16–27. https://doi.org/10.1111/jar.12779
Reid, N., Kron, A., Rajakulendran, T., Kahan, D., Noble, A., & Stergiopoulos, V. (2020). Promoting wellness and recovery of young women experiencing gender-based violence and homelessness: The role of trauma-informed health promotion interventions. Violence Against Women, 27(9). https://doi.org/10.1177/1077801220923748
Reid, N., Mason, J., Kurdyak, P., Nisenbaum, R., de Oliveira, C., Hwang, S., & Stergiopoulos, V. (2021). Evaluating the impact of a critical time intervention adaptation on health care utilization among homeless adults with mental health needs in a large urban center. Journal of Psychiatry. https://doi.org/10.1177/0706743721996114
Richard, L., Booth, R., Rayner, J., Clemens, K. K., Forchuk, C., & Shariff, S. Z. (2021). Testing, infection and complication rates of COVID-19 among people with a recent history of homelessness in Ontario, Canada: A retrospective cohort study. CMAJ Open, 9(1), E1–E9. https://doi.org/10.9778/cmajo.20200287
Richard, L., Hwang, S. W., Forchuk, C., Nisenbaum, R., Clemens, K., Wiens, K., … Shariff, S. Z. (2019). Validation study of health administrative data algorithms to identify individuals experiencing homelessness and estimate population prevalence of homelessness in Ontario, Canada. BMJ Open, 9(10), e030221–e030221. https://doi.org/10.1136/bmjopen-2019-030221
Richler, M. J., Yousaf, S., Hwang, S. W., & Dewhurst, N. F. (2019). Descriptive study of homeless patients’ perceptions that affect medication adherence. American Journal of Health-System Pharmacy, 76(17), 1288–1295. https://doi.org/10.1093/ajhp/zxz139
Rivera, L. A., Henschke, M. T., Khoo, E., Ing, S., Bae, S. J., Rice, C. M., … Forseth, M. H. (2018). A modeling study exploring the impact of homelessness on rostered primary care utilization in Calgary, Canada. Canadian Journal of Public Health, 109(4), 451–458. https://doi.org/10.17269/s41997-018-0098-6
Rodger, S., Bird, R., Hibbert, K., Johnson, A. M., Specht, J., & Wathen, C. N. (2020). Initial teacher education and trauma and violence informed care in the classroom: Preliminary results from an online teacher education course. Psychology in the Schools, 57(12), 1798–1814. https://doi.org/10.1002/pits.22373
Rogers, T., & Shafer, R. (2018). Addressing homelessness in our schools and language arts classrooms. Language Arts, 96(2), 102–112. National Council of Teachers of English (ncte.org)
Rotondi, M. A., O’Campo, P., O’Brien, K., Firestone, M., Wolfe, S. H., Bourgeois, C., & Smylie, J. K. (2017). Our health counts Toronto: Using respondent-driven sampling to unmask census undercounts of an urban indigenous population in Toronto, Canada. BMJ Open, 7(12), e018936–e018936. https://doi.org/10.1136/bmjopen-2017-018936
Roy, L., Crocker, A., Hurtubise, R., Latimer, E., Côté, M., Billette, I., & Boissy, F. (2020). Reducing criminal justice involvement of individuals experiencing homelessness and mental illness: Perspectives of frontline practitioners. Canadian Journal of Criminology and Criminal Justice, 62(2), 1–21. https://doi.org/10.3138/cjccj.2019-0056
Roy, S., Svoboda, T., Issacs, B., Budin, R., Sidhu, A., Biss, R. K., … Connelly, J. (2020). Examining the cognitive and mental health related disability rates among the homeless: Policy implications of changing the definition of disability in Ontario. Canadian Psychology = Psychologie Canadienne, 61(2), 118–126. https://doi.org/10.1037/cap0000211
Saewyc, E., Mounsey, B., Tourand, J., Brunanski, D., Kirk, D., McNeil-Seymour, J., Shaughnessy, K., Tsuruda, S., & Clark, N. (2017). Homeless & street-involved Indigenous LGBTQ2S youth in British Columbia: Intersectionality, challenges, resilience & cues for action. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Saewyc, E. M., Shankar, S., Pearce, L. A., & Smith, A. (2021). Challenging the stereotypes: unexpected features of sexual exploitation among homeless and street-involved boys in western Canada. International Journal of Environmental Research and Public Health, 18(11), 5898–. https://doi.org/10.3390/ijerph18115898
Sandu, R. D., Anyan, F., & Stergiopoulos, V. (2021). Housing first, connection second: the impact of professional helping relationships on the trajectories of housing stability for people facing severe and multiple disadvantage. BMC Public Health, 21(1), 249–249. https://doi.org/10.1186/s12889-021-10281-2
Santos Salas, A., Watanabe, S. M., Tarumi, Y., Wildeman, T., Hermosa García, A. M., Adewale, B., & Duggleby, W. (2019). Social disparities and symptom burden in populations with advanced cancer: specialist palliative care providers’ perspectives. Supportive Care in Cancer, 27(12), 4733–4744. https://doi.org/10.1007/s00520-019-04726-z
Scheim, A. I., Bauer, G. R., & Shokoohi, M. (2017). Drug use among transgender people in Ontario, Canada: Disparities and associations with social exclusion. Addictive Behaviors, 72, 151–158. https://doi.org/10.1016/j.addbeh.2017.03.022
Schiff, R. (2016a). Conclusion. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Schiff, R. (2016b). Regina, Saskatchewan: The case of small, isolated urban centres. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Schiff, R., Buccieri, K., Waegemakers Schiff, J, Kauppi, C., & Riva, M. (2020). COVID-19 and pandemic planning in the context of rural and remote homelessness. Canadian Journal of Public Health, 111(6), 967–970. https://doi.org/10.17269/s41997-020-00415-1
Schiff, R., & Møller, H. (Eds.). (2021). Health and health care in northern Canada. Toronto: University of Toronto Press.
Schütz, C., Choi, F., Jae Song, M., Wesarg, C., Li, K., & Krausz, M. (2019). Living with dual diagnosis and homelessness: Marginalized within a marginalized group. Journal of Dual Diagnosis, 15(2), 88–94. https://doi.org/10.1080/15504263.2019.1579948
Schwan, K., Dej, E. & Versteegh, A. (2020). Girls, homelessness, and COVID-19: The urgent need for research and action. Girlhood Studies, 13(3), 151-168. https://doi.org/10.3167/ghs.2020.130311
Schwan, K., Kidd, S., Gaetz, S., O’Grady, B., & Redman, M. (2017). Mental health care for homeless youth: A proposal for federal, provincial, and territorial leadership, coordination, and targeted investment. Toronto: Canadian Observatory on Homelessness Press. Canadian Observatory On Homelessness Policy Brief (homelesshub.ca)
Schwan, K., Vaccaro, M. E., Reid, L., & Ali, N. (2021). Implementation of the right to housing for women, girls, and gender diverse people in Canada. Canada: The National Right to Housing Network. Microsoft Word – EN_CHRC_13.docx (housingrights.ca)
Schwan, K., Vaccaro, M., Reid, L., Ali, N., & Baig, K. (2021b). The pan-Canadian women’s housing & homelessness survey. Toronto, ON: Canadian Observatory on Homelessness. Pan-Canadian-Womens-Housing-Homelessness-Survey
Selfridge, M., Greer, A., Card, K. G., Macdonald, S., & Pauly, B. (2020). “It’s like super structural” – Overdose experiences of youth who use drugs and police in three non-metropolitan cities across British Columbia. The International Journal of Drug Policy, 76, 102623–102623. https://doi.org/10.1016/j.drugpo.2019.102623
Shaikh, A., & Rawal, H. (2019). Interconnections among homelessness, family separation, and mental health: Implications for multi-sectoral social services. Journal of Social Service Research, 45(4), 543–557. https://doi.org/10.1080/01488376.2018.1481174
Shankar, S., Gogosis, E., Palepu, A., Gadermann, A. M., & Hwang, S. W. (2019). “I haven’t given up and I’m not gonna”: A phenomenographic exploration of resilience among individuals experiencing homelessness. Qualitative Health Research, 29(13), 1850–1861. https://doi.org/10.1177/1049732318798353
Sibley, M. A. (2020). Attachments to victimhood: Anti-trafficking narratives and the criminalization of the sex trade. Social & Legal Studies, 29(5), 699–717. https://doi.org/10.1177/0964663919897970
Simpson, A., Furlong, A., & Jetha, N. (2018). At-a-glance: Bringing equity into the fold: A review of interventions to improve mental health. Health Promotion and Chronic Disease Prevention in Canada, 38(10), 380–384. https://doi.org/10.24095/hpcdp.38.10.04
Skolnik, T. (2018). How and why homeless people are regulated differently. Queen’s Law Journal, 43(1), 297. https://ssrn.com/abstract=3219919
Smith, E., Milaney, K., Henderson, R. I., & Crowshoe, L. (2021). Adverse childhood experiences and health among indigenous persons experiencing homelessness. BMC Public Health, 21(1), 85–85. https://doi.org/10.1186/s12889-020-10091-y
Sohn, J. & Gaetz, S. (2020). Upstream Canada: An early intervention strategy to prevent youth homelessness & school disengagement. Toronto: Canadian Observatory on Homelessness Press.
Song, M. J., Nikoo, M., Choi, F., Schütz, C. G., Jang, K., & Krausz, R. M. (2018). Childhood trauma and lifetime traumatic brain injury among individuals who are homeless. The Journal of Head Trauma Rehabilitation, 33(3), 185–190. https://doi.org/10.1097/HTR.0000000000000310
Stajduhar, K. I., Giesbrecht, M., Mollison, A., Dosani, N., & McNeil, R. (2020). Caregiving at the margins: An ethnographic exploration of family caregivers experiences providing care for structurally vulnerable populations at the end-of-life. Palliative Medicine, 34(7), 946–953. https://doi.org/10.1177/0269216320917875
Stajduhar, K. I., Mollison, A., Giesbrecht, M., McNeil, R., Pauly, B., Reimer-Kirkham, S., … Rounds, K. (2019). “Just too busy living in the moment and surviving”: Barriers to accessing health care for structurally vulnerable populations at end-of-life. BMC Palliative Care, 18(1), 11. https://doi.org/10.1186/s12904-019-0396-7
St. Arnault, D., & Merali, N. (2019a). Pathways for refugees’ descent into homelessness in Edmonton, Alberta: The urgent need for policy and procedural change. Journal of International Migration and Integration, 20(4), 1161–1179. https://doi.org/10.1007/s12134-019-00652-5
St. Arnault, D., & Merali, N. (2019b). Refugee pathways out of homelessness in urban Alberta, Canada: implications for social justice-oriented counselling. Counselling Psychology Quarterly, 32(2), 227–245. https://doi.org/10.1080/09515070.2018.1437540
Statistics Canada. (2020). 2016 census Aboriginal community portraits. Canada: Statistics Canada.
Stergiopoulos, V., Gozdzik, A., Nisenbaum, R., Durbin, J., Hwang, S. W., O’Campo, P., … Wasylenki, D. (2018). Bridging hospital and community care for homeless adults with mental health needs: Outcomes of a brief interdisciplinary intervention. Canadian Journal of Psychiatry, 63(11), 774–784. https://doi.org/10.1177/0706743718772539
Stergiopoulos, V., Gozdzik, A., Nisenbaum, R., Lamanna, D., Hwang, S. W., Tepper, J., & Wasylenki, D. (2017). Integrating hospital and community care for homeless people with unmet mental health needs: Program rationale, study protocol and sample description of a brief multidisciplinary case management intervention. International Journal of Mental Health and Addiction, 15(2), 362–378. https://doi.org/10.1007/s11469-017-9731-5
Stergiopoulos, V., Gozdzik, A., Tan de Bibiana, J., Guimond, T., Hwang, S. W., Wasylenki, D. A., & Leszcz, M. (2016). Brief case management versus usual care for frequent users of emergency departments: The coordinated access to care from hospital emergency departments (CATCH-ED) randomized controlled trial. BMC Health Services Research, 16(1), 432–432. https://doi.org/10.1186/s12913-016-1666-1
Stergiopoulos, V., Naidu, A., Schuler, A., Bekele, T., Nisenbaum, R., Jbilou, J., … Rourke, S. B. (2019). Housing stability and neurocognitive functioning in homeless adults with mental illness: A subgroup analysis of the At Home/Chez Soi study. Frontiers in Psychiatry, 10, 865–865. https://doi.org/10.3389/fpsyt.2019.00865
Stewart, S. (2018). Supporting Indigenous youth experiencing homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Stewart, S. (2019). Family counselling as decolonization: Exploring an Indigenous social-constructivist approach in clinical practice. First Peoples Child & Family Review, 14(1), 43-56. https://fpcfr.journals.publicknowledgeproject.org/index.php/FPCFR/article/view/371
Strobel, S., Burcul, I., Dai, J. H., Ma, Z., Jamani, S., & Hossain, R. (2021). Characterizing people experiencing homelessness and trends in homelessness using population-level emergency department visit data in Ontario, Canada. Ottawa: Statistics Canada, Health Reports.
Sumalinog, R., Harrington, K., Dosani, N., & Hwang, S. W. (2017). Advance care planning, palliative care, and end-of-life care interventions for homeless people: A systematic review. Palliative Medicine, 31(2), 109-119. doi: 10.1177/0269216316649334
Sylvestre, J., Kerman, N., Polillo, A., Lee, C. M., & Aubry, T. (2017). A profile of families in the emergency family homeless shelter system in Ottawa, Ontario, Canada. Canadian Journal of Urban Research, 26(1), 40–51. Canadian Journal of Urban Research
Sylvestre, J., Kerman, N., Polillo, A., Lee, C. M., Aubry, T., & Czechowski, K. (2018). A Qualitative study of the pathways into and impacts of family homelessness. Journal of Family Issues, 39(8), 2265–2285. https://doi.org/10.1177/0192513X17746709
Sylvestre, J., Klodawsky, F., Gogosis, E., Ecker, J., Polillo, A., Czechowski, K., … Hwang, S. (2018). Perceptions of housing and shelter among people with histories of unstable housing in three cities in Canada: A qualitative study. American Journal of Community Psychology, 61(3-4), 445–458. https://doi.org/10.1002/ajcp.12243
Thistle, J. (2017.) Indigenous definition of homelessness in Canada. Toronto: Canadian Observatory on Homelessness Press.
Thistle, J. (2019). From the ashes. My story of being Métis, homeless and finding my way. Simon Schuster: Toronto, Canada
Thistle, J., & Smylie, J. (2020). Pekiwewin (coming home): Advancing good relations with Indigenous people experiencing homelessness. Canadian Medical Association Journal (CMAJ), 192(10), E257–E259. https://doi.org/10.1503/cmaj.200199
Thulien, N. S., Gastaldo, D., Hwang, S. W., & McCay, E. (2018). The elusive goal of social integration: A critical examination of the socio-economic and psychosocial consequences experienced by homeless young people who obtain housing. Canadian Journal of Public Health, 109(1), 89–98. https://doi.org/10.17269/s41997-018-0029-6
Thulien, N. S., Gastaldo, D., McCay, E., & Hwang, S. W. (2019). “I want to be able to show everyone that it is possible to go from being nothing in the world to being something”: Identity as a determinant of social integration. Children and Youth Services Review, 96, 118–126. https://doi.org/10.1016/j.childyouth.2018.11.005
Thulien, N. S., Kozloff, N., McCay, E., Nisenbaum, R., Wang, A., & Hwang, S. W. (2019). Evaluating the effects of a rent subsidy and mentoring intervention for youth transitioning out of homelessness: Protocol for a mixed methods, community-based pilot randomized controlled trial. JMIR Research Protocols, 8(12), e15557–e15557. https://doi.org/10.2196/15557
Thulien, N. S., Wang, A., Mathewson, C., Wang, R., & Hwang, S. W. (2021). Tackling exclusion: A pilot mixed method quasi-experimental identity capital intervention for young people exiting homelessness. PLOS ONE. https://doi.org/10.1371/journal.pone.0256288
Timler, K., Varcoe, C., & Brown, H. (2019). Growing beyond nutrition: How a prison garden program highlights the potential of shifting from food security to food sovereignty for Indigenous peoples. International Journal of Indigenous Health, 14(2), 95–114. https://doi.org/10.32799/ijih.v14i2.31938
To, M. J., Palepu, A., Matheson, F. I., Ecker, J., Farrell, S., Hwang, S. W., & Werb, D. (2016). The effect of incarceration on housing stability among homeless and vulnerably housed individuals in three Canadian cities: A prospective cohort study. Canadian Journal of Public Health, 107(6), e550–e555. https://doi.org/10.17269/CJPH.107.5607
Trent University Homelessness Research Collective. (2019). “A good day is waking up inside.” Conversations about homelessness, housing vulnerability, and health care across the City of Kawartha Lakes and Haliburton County. ON: Trent University HRC.
Turner, A., Albanese, T., & Pakeman, K. (2017). Discerning “functional and absolute zero:” Defining and measuring an end to homelessness in Canada. The School of Public Policy Publications (SPPP), 10(2), 1–43. https://doi.org/10.11575/sppp.v10i0.42616
Urbanoski, K., Veldhuizen, S., Krausz, M., Schutz, C., Somers, J. M., Kirst, M., … Goering, P. (2018). Effects of comorbid substance use disorders on outcomes in a Housing First intervention for homeless people with mental illness. Addiction (Abingdon, England), 113(1), 137–145. https://doi.org/10.1111/add.13928
Van Berkum, A., & Oudshoorn, A. (2019). “Where to now?” Understanding the landscape of health and social services for homeless women in London, Ontario, Canada. Journal of Social Inclusion, 10(1), 41. https://doi.org/10.36251/josi.158
Van den Hoonaard, W. (2018). The vulnerability of vulnerability: Why social science researchers should abandon the doctrine of vulnerability. In the Sage Handbook of Qualitative Research Ethics (pp. 305-321). SAFE Publications Ltd, https://dx-doi-org.proxy1.lib.trentu.ca/10.4135/9781526435446.n21
van Ingen, C., Sharpe, E., & Lashua, B. (2018). Neighborhood stigma and the sporting lives of young people in public housing. International Review for the Sociology of Sport, 53(2), 197–212. https://doi.org/10.1177/1012690216641146
Victor, J., Shouting, M., DeGroot, C., Vonkeman, L., Brave Rock, M., & Hunt, R. (2019). I’taamohkanoohsin (everyone comes together): (Re)connecting Indigenous people experiencing homelessness and substance misuse to Blackfoot ways of knowing. International Journal of Indigenous Health, 14(1), 42–59. https://doi.org/10.32799/ijih.v14i1.31939
Vitopoulos, N., Cerswell Kielburger, L., Frederick, T., & Kidd, S. (2018). Developing a trauma-informed mental health group intervention for youth transitioning out of homelessness. In S. Kidd, N. Slesnick, T. Frederick, J. Karabanow, & S. Gaetz (eds.), Mental health & addiction interventions for youth experiencing homelessness: Practical strategies for front-line providers. Toronto, ON: Canadian Observatory on Homelessness.
Vitopoulos, N. A., Frederick, T. J., Leon, S., Daley, M., McDonald, C., Morales, S., … Kidd, S. A. (2018). Development of a complex tertiary prevention intervention for the transition out of youth homelessness. Children and Youth Services Review, 94, 579–588. https://doi.org/10.1016/j.childyouth.2018.08.038
Vogel, M., Frank, A., Choi, F., Strehlau, V., Nikoo, N., Nikoo, M., … Schütz, C. G. (2017). Chronic pain among homeless persons with mental illness. Pain Medicine, 18(12), 2280–2288. https://doi.org/10.1093/pm/pnw324
Vogel, M., Nikoo, M., Nikoo, N., Schütz, C. G., Walter, M., Somers, J., & Krausz, M. (2019). Association of substance use patterns with psychiatric disorders in homeless persons with psychiatric disorders in Vancouver. Int J Ment Health Addiction 17, 1200–1213. https://doi.org/10.1007/s11469-018-0040-4
Voisard, B., Whitley, R., Latimer, E., Looper, K., & Laliberté, V. (2021). Insights from homeless men about PRISM, an innovative shelter-based mental health service. PloS One, 16(4), e0250341–e0250341. https://doi.org/10.1371/journal.pone.0250341
Von Riesen, K. (2020). Providing meaningful spiritual care to Indigenous populations experiencing homelessness. Master’s Thesis. University of Manitoba.
Waegemakers Schiff, J. (2015). Working with homeless and vulnerable people: Basic skills and practices. UK: Oxford University Press.
Waegemakers Schiff, J., & Lane, A. (2016). The Calgary response. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Waegemakers Schiff, J., & Lane, A. M. (2019). PTSD symptoms, vicarious traumatization, and burnout in front line workers in the homeless sector. Community Mental Health Journal, 55(3), 454–462. https://doi.org/10.1007/s10597-018-00364-7
Waegemakers Schiff, J., Pauly, B., & Schiff, R. (2016). Health needs and analysis of pandemic planning in four Canadian cities. In K. Buccieri, & R. Schiff (eds.), Pandemic Preparedness and Homelessness: Lessons from H1N1 in Canada. Toronto, ON: Canadian Observatory on Homelessness.
Waegemakers Schiff, J., & Rook, J. (2012). Housing first: Where is the evidence? Toronto: Homeless Hub.
Waite, S., Ecker, J., & Ross, L. E. (2019). A systematic review and thematic synthesis of Canada’s LGBTQ2S+ employment, labour market and earnings literature. PloS One, 14(10), e0223372–e0223372. https://doi.org/10.1371/journal.pone.0223372
Wales, J., Kalia, S., Moineddin, R., & Husain, A. (2020). The impact of socioeconomic status on place of death among patients receiving home palliative care in Toronto, Canada: A retrospective cohort study. Journal of Palliative Care, 35(3), 167–173. https://doi.org/10.1177/0825859719855020
Wallace, B., Pauly, B., Perkin, K., & Cross, G. (2019). Where’s the housing? Housing and income outcomes of a transitional program to end homelessness. Journal of Poverty, 23(2), 161–178. https://doi.org/10.1080/10875549.2018.1549185
Wang, J. Z., Mott, S., Magwood, O., Mathew, C., Mclellan, A., Kpade, V., … Andermann, A. (2019). The impact of interventions for youth experiencing homelessness on housing, mental health, substance use, and family cohesion: a systematic review. BMC Public Health, 19(1), 1528–1528. https://doi.org/10.1186/s12889-019-7856-0
Wang, A., Pridham, K.F., Nisenbaum, R., Pedersen, C., Brown, R., & Hwang, S. W. (2021). Factors associated with readmission among general internal medicine patients experiencing homelessness. Journal of General Internal Medicine, 36, 1944–1950. https://doi.org/10.1007/s11606-020-06483-w
Wardhaugh, J. (1999). The unaccommodated woman: Home, homelessness and identity. The Sociological Review, 47(1): 91-109. https://doi.org/10.1111/1467-954X.00164
Webster, P. (2017). Bringing homeless deaths to light. Canadian Medical Association Journal, 189(11), E446–E447. https://doi.org/10.1503/cmaj.1095399
West, K. J., Wrobel, B., Pallotta, S., & Coatsworth, A. (2020). Bearing witness: Exploring the end-of-life needs of homeless persons and barriers to appropriate care. Omega: Journal of Death and Dying, 82(1), 63–91. https://doi.org/10.1177/0030222818801150
Wheeler, C., Price, C., & Ellasante, I. (2017). Pathways into and out of homelessness for LGBTQ2S youth. In A. Abramovich, & J. Shelton (eds.), Where am I going to go? Intersectional approaches to ending LGBTQ2S youth homelessness in Canada & the U.S. Toronto, ON: Canadian Observatory on Homelessness.
Whisler, A., Dosani, N., To, M. J., O’Brien, K., Young, S., & Hwang, S. W. (2021). The effect of a housing first intervention on primary care retention among homeless individuals with mental illness. PloS One, 16(2), e0246859–e0246859. https://doi.org/10.1371/journal.pone.0246859
Wiens, K., Nisenbaum, R., Sucha, E., Aubry, T., Farrell, S., Palepu, A., Duhoux, A., Gadermann, A., & Hwang, S. W. (2021). Does housing improve health care utilization and costs? A longitudinal analysis of health administrative data link to a cohort of individuals with a history of homelessness. Medical Care, 59, S110-S116. 10.1097/MLR.0000000000001379
Wiens, K., Rosella, L.C., Kurdyak, P., Chen, S., Aubry, T., Stergiopoulos, V., & Hwang, S. W. (2021). Factors associated with higher healthcare costs in a cohort of homeless adults with a mental illness and a general cohort of adults with a history of homelessness. BMC Health Serv Res, 21, 555. https://doi.org/10.1186/s12913-021-06562-
Wiens, K., Rosella, L. C., Kurdyak, P., & Hwang, S. W. (2020). Patterns and predictors of high-cost users of the health system: A data linkage protocol to combine a cohort study and randomised controlled trial of adults with a history of homelessness. BMJ Open, 10(12), e039966–e039966. https://doi.org/10.1136/bmjopen-2020-039966
Wolfstadt, J. I., Pincus, D., Kreder, H. J., & Wasserstein, D. (2019). Association between socioeconomic deprivation and surgical complications in adults undergoing ankle fracture fixation: A population-based analysis. Canadian Journal of Surgery, 62(5), 320–327. https://doi.org/10.1503/cjs.012018
Wong, A., Chen, J., Dicipulo, R., Weiss, D., Sleet, D. A., & Francescutti, L. H. (2020). Combatting homelessness in Canada: Applying lessons learned from six tiny villages to the Edmonton bridge healing program. International Journal of Environmental Research and Public Health, 17(17), 6279–. https://doi.org/10.3390/ijerph17176279
Woolley, E. (2015). Why wasn’t homelessness a social problem until the 1980s? Homeless Hub. https://www.homelesshub.ca/blog/why-wasnt-homelessness-social-problem-until-1980s
Wu, H., & Karabanow, J. (2020). COVID-19 and beyond: Social work interventions for supporting homeless populations. International Social Work, 63(6), 790–794. https://doi.org/10.1177/0020872820949625
Wu, V., Noel, C. W., Forner, D., Mok, F., Zirkle, M., Eskander, A., … Lee, J. M. (2020). Otolaryngology needs among an adult homeless population: a prospective study. Journal of Otolaryngology-Head and Neck Surgery, 49(1), 1–47. https://doi.org/10.1186/s40463-020-00445-2
Yakubovich, A. R., & Maki, K. (2021). Preventing gender-based homelessness in Canada during the COVID-19 pandemic and beyond: The need to account for violence against women. Violence Against Women, 1-13. DOI: 10.1177/10778012211034202
Yazdani, K., Nikoo, M., Sayre, E. C., Choi, F., Jang, K., & Krausz, R. M. (2020). The impact of employment on recovery among individuals who are homeless with severe mental illness in the Vancouver at home / chez soi trial. Social Psychiatry and Psychiatric Epidemiology, 55(12), 1619–1627. https://doi.org/10.1007/s00127-020-01887-9
Young, S., & Fairbairn, N. (2018). Expanding supervised injection facilities across Canada: lessons from the Vancouver experience. Canadian Journal of Public Health, 109(2), 227–230. https://doi.org/10.17269/s41997-018-0089-7
Young, M. G., & Manion, K. (2017). Harm reduction through housing first: an assessment of the Emergency Warming Centre in Inuvik, Canada. Harm Reduction Journal, 14(1), 8–8. https://doi.org/10.1186/s12954-016-0128-8
Zhang, L., Norena, M., Gadermann, A., Hubley, A., Russell, L., Aubry, T., To, M. J., Farrell, S., Hwang, S. W., & Palepu, A. (2018). Concurrent disorders and health care utilization among homeless and vulnerably housed persons in Canada. Journal of Dual Diagnosis, 14(1), 21–31. https://doi.org/10.1080/15504263.2017.1392055
Zhang, P., & Kteily-Hawa, R. (2018). Poetry, prose, and personhood: The art of storytelling with the homeless. Canadian Journal for the Study of Adult Education, 30(2), 69-79. https://cjsae.library.dal.ca/index.php/cjsae/article/view/5438
Zhang, P., Wiens, K., Wang, R., Luong, L., Ansara, D., Gower, S., … Hwang, S. W. (2019). Cold weather conditions and risk of hypothermia among people experiencing homelessness: Implications for prevention strategies. International Journal of Environmental Research and Public Health, 16(18), 3259. https://doi.org/10.3390/ijerph16183259
Zuccaro, L., Champion, C., Bennett, S., & Ying, Y. (2018). Understanding the surgical care needs and use of outpatient surgical care services among homeless patients at the Ottawa Hospital. Canadian Journal of Surgery, 61(6), 424–429. https://doi.org/10.1503/cjs.001317
4
 | Are you a student who read this book? Tell us what you think!
|
 | Are you an instructor who adopted this book? Tell us what you think!
|
 | Did you come across our book online? We would love to hear from you!
|
You can also reach out to us directly at understandinghomelessness.ebook@gmail.com.
Thank you for your time!