Welcome to Therapeutic Communication for Health Care Administrators Digital Text Open Educational Resources (OER). These resources are intended for learners preparing for positions in front-line health care settings. Recognizing the diverse titles for these types of roles, we intend that the title Health Care Administrator is an umbrella term that includes all types of front-line Health Care Administrators. This OER is intended to be used with the companion resources, Therapeutic Communications for Health Care Administrators Game Simulations to be released in Spring 2022.
Health Care Administrators are often the first point of contact for clients and their families and often are the liaison between the health care providers, and the client; thus, therapeutic communication is an essential competency. An environmental scan was sent to industry partners and colleagues in the Ontario higher education system in Spring 2020. Based on those results, it was identified that many existing resources do not address the communication skills of the health care administrator role. The digital text and companion game simulations address the gaps while also providing essential digital resources that can be used in remote, hybrid, or face-to-face delivery formats.
This digital text OER has been developed with Universal Design for Learning (UDL) elements in mind. The authors have purposefully used inclusive language such as they and them for singular pronouns in place of gendered pronouns. The cultural chapter components have been reviewed by members of the cultural communities addressed in the chapter while also recognizing that one or two reviewers do not represent entire cultures. We welcome your review and feedback and encourage you to reach out to the authors with any concerns, suggestions for modifications, and ideas for enhancements.
Kimberlee is a faculty member in the Business School at Conestoga College ITAL, in Kitchener Ontario and can be reached at kcarter@conestogac.on.ca. Currently on secondment, as an Open Educational Resources (OER) projects consultant is pursuing a passion for equitable education through the creation of OER for learners. Kimberlee has spent 17 years working with learners to develop competencies to work on the front lines of health care administration and prior to becoming an educator, spent most of her career working in a variety of health care administration roles in hospitals in Ontario and British Columbia. Kimberlee will be forever grateful for the opportunity to collaborate with colleagues Marie and Connie who are learner-first focussed and share the perspective that the development of ongoing therapeutic communication skills is important for learners and by extension for communities.
Marie Rutherford, Dip., Nursing, LD, BGS.
Marie Rutherford is a faculty member in the School of Business at Georgian College CAAT, in Barrie Ontario and can be reached at marie.rutherford@georgiancollege.ca. Her area of focus for the past 22 years is Office Administration Health Services. Years prior to commencing her teaching career, Marie completed a diploma nursing program. After receiving her licensing, Marie spent a number of years as a nurse in a variety of health care settings before transitioning to administrative health care roles. Marie has continued her education through additional advanced degree studies. Marie is passionate about education and the opportunities provided by open educational resources (OER). This cross-collaboration has provided the opportunity to share her years of experience in diverse health care settings along with her motivation to support learners in impactful and meaningful ways.
Connie Stevens, RN.,BScN, MA. PhD (c)
Connie Stevens is a faculty member in the Pilon School of Business at Sheridan College, in Mississauga, Ontario and can be reached at connie.stevens1@sheridancollege.ca. Connie is the program coordinator for Office Administration and a professor in the Office Administration- Health services program. Connie is a Registered Nurse with vast experience in Sexual Health, Sexual Assault, Domestic Violence, Forensic nursing, Communicable diseases, cardiology, neonatology, and immunization. The personal and professional cross-collaboration with Conestoga and Georgian has provided the opportunity for growth and development and the ultimate contribution to future learners. Connie enjoys sharing her experiences and is an endless storyteller (all true!).
Funding Acknowledgements
2
This project is made possible with funding by the Government of Ontario and through eCampusOntario’s support of the Virtual Learning Strategy. To learn more about the Virtual Learning Strategy visit: https://vls.ecampusontario.ca.
Acknowledgements
3
Gratitude and Thanks
We wish to express our gratitude and thanks to the following list of people who supported and participated in this project.
Leadership Teams
With thanks and gratitude, to our respective leadership teams for their support and encouragement in this endeavour.
Conestoga College ITAL:
Barbara Kelly PhD, Vice-President of Academic/Student Affairs/Human Resources and Research
Gary Hallam M.Sc., Vice President, International & Executive Dean School of Business, School of Hospitality & Culinary Art
Michelle Grimes PhD, Dean School of Business
Jeff Fila PhD, Director of Special Projects
Lil Premsukh, MA(LIC), CDP Chair, School of Business
Pavla Kazda MBA PMP, Dean School of Business, Automotive Business
Sara Budd M.Ed, Associate Dean School of Business, Automotive Business
Sheridan College ITAL:
Anne-Liisa Longmore EdD, Dean Pilon School of Business
Brian Chama PhD, Associate Dean Pilon School of Business
Peer Reviewers
We wish to thank our Ontario colleagues for providing a peer review as we were completing this resource.
Jennifer Ethier MSc., Professor Office Administration – Health Services program, Georgian College CAAT
Wendy Fisher Dipl., CMS, Professor and Coordinator, Office Administration – Health Services program, Mohawk College CAAT
Kellie Hayward BA., MEd, Professor, Office Administration- Health Services program, Sheridan College ITAL
Dina Mikhael, MD, MSc., Professor, Office Administration- Health Services program, Sheridan College ITAL
Claire Palvetzian, M.Ed., B.A. Kin, Professor Health Office Administration and Medical Office Practices programs. Conestoga College ITAL
Support Teams
Holly Ashbourne, Hon. BA, MLIS Conestoga College ITAL, liaison to accessibility and library supports, for providing a final review, and countless support with Pressbooks technology through workshops, diving into Pressbooks to have a look, and answer numerous questions.
Erjona Ferizi, OER Projects Assistant, who on her co-op from the Bachelor of Public Relations program at Conestoga College ITAL provided ongoing administrative support, coordinated events, and completed extensive first-line copy edits, accessibility checks, labelling multiple images and participation in content creation and learner review feedback.
Stephanie Lewis, OER Assistant, Health Office Administration Program, Conestoga College ITAL through the fall semester of 2021, co-constructed alongside us content and interactive learning objects. Additional thanks for examining the content and providing feedback from the learner’s perspective. Thank you for paying it forward for future learners.
Camila Redondo Morant, OER Assistant, Health Office Administration Program, Conestoga College ITAL through the fall and winter semesters of 2021/2022, co-constructed alongside us content and interactive learning objects. Additional thanks for examining the content and providing feedback from the learner’s perspective. Thank you for paying it forward for future learners.
James Yochem, Hon. BA, MLIS Copyright Coordinator, Conestoga College ITAL for answering numerous copyright and copy edit questions.
Antonina Gousseva, BA, Dipl. LIT, Conestoga College ITAL for ensuring this resource met all accessibility requirements.
Juliet Conlon, MLS, Conestoga College ITAL for support in searching out existing OER.
Jen Booth, BA, MISt OER Librarian Georgian College CAAT for supporting students through ancillary resource creation.
Elan Paulson, PhD, Teaching and Learning Consultant Conestoga College ITAL for providing consultations on design for learning.
Learners
Learner Volunteers for Ancillary Development
Kahan Durgesh Choksi, Georgian College, Office Administration – Health Services, Georgian College CAAT
Jennifer Wilson, Office Administration – Health Services, Georgian College CAAT
Learner Content Contributors via Contest Submissions
Nicole Skinner, Office Administration – Health Services, Georgian College CAAT
Tara Friedmann, Health Office Administration program, Conestoga College ITAL
Hawagor Ilyas Unia, Health Office Administration program, Conestoga College ITAL
Volunteer Actors for Videos, Voices, and Images
Jess Bailey
Krystal Carter
Meher Kaur Chhabra
Royston Dalmeida
Erjona Ferizi
Guillermo Herrera-Valencia
Jocelyn Kiryluk
Stephanie Lewis
Tina Maputol
Camila Redondo Morant
Fabio Munoz
Blessing Okeoghene Omobo
Mariam Raza
Kevin Swayze
Stephen Njenga
Devesh Rajarshi
Media
We wish to thank our media partners for their contributions.
David Ward Media and crew for video services
Krystal Carter Communications for photography services
Disclaimer
We have done our best to acknowledge all participants involved and with correct job titles and credentials. In the event, we have made an error please reach out to any one of the authors to have this corrected.
Media 1.1 Anxiety Scene [Video]. CC-BY-NC-SA 2021. Conestoga College.
Learning Objectives
Recognize the importance of professional communication to meeting the goals of health care settings.
Apply the transmission model and interactive model of communication to the process of communication in health care settings.
Explore the importance of types, channels, active listening, and courteous communication for professional communication in health care settings.
Summarize what a Health Care Administrator (HCA) can do to demonstrate professional communication.
Introduction
Health care administrators (HCAs) are often the first point of contact for clients in many health care settings. This may take the form of verbal communication such as speaking to a client who is looking for a new family physician and has called the office to find out if the physician is accepting new patients. HCAs are often the first person a client interacts with when arriving for their in-person health appointments. Sometimes, when clients arrive to check-in, the health care administrator (HCA) is on the phone and may use non-verbal communication to convey a warm hello by making eye contact, a friendly wave, and a smile. If a client appointment is to take place on the telephone or through virtual conferencing software, it is the HCA who will make the arrangements for the client to talk with the health care provider (HCP). HCAs are frequently required to communicate with clients, clients’ family members, and other members of the health care team through written communication like email. With this in mind let’s consider the role that customer service skills play in communicating professionally to ensure that the clients’ health care needs are met.
Assessing What You Already Know
Most people have had at least one, if not several communication interactions with health care administrators. Consider the last time you went to the dentist, family doctor, or even took your pet to the Veterinarians. As you reflect upon the following questions and statements, consider what you might already perceive about professional communication based on your past experiences.
Professional Communication in Health Care Settings
Health care clients expect competence when seeking health care services because decisions about health care choices impact their quality of life. Consider that a health care administrator (HCA) may have the education and training required to competently perform their employment tasks, but if they do not present and communicate in the way a client expects, it may be difficult for the client to trust that the HCA is competent. This is why a set of standards regarding how to dress, behave, and communicate is set by the HCP and are the professional expectations to be followed by the staff working for the HCP. Clients will only share their health concerns when they believe that their HCP is competent and trustworthy. When clients share all of their health concerns, then health care providers have a better chance of meeting the goals to provide services that meet their client’s health care needs.
You may have heard the expression the customeris always right, this expression sets the tone that customer satisfaction is the focus of the business. When customers are satisfied with the service, they will likely purchase the business goods and/or services again, and refer their friends. Health care settings provide health and wellness services as their business. Since many health care appointments are paid for using Provincial health insurance plans or third-party insurance plans, there is often a disconnect to people viewing health care settings as businesses. This is likely because there does not appear to be a transaction of goods for money directly with the client.
In Canada, the health care and social assistance sector is the second-largest industrial sector employer (Government of Canada, 2015). Health care businesses provide valuable services that improve quality of life by caring for Canadians and by providing employment. Health care businesses are customer-centred with the added complexities of clients with health concerns who are not feeling well, clients with differing views about treatment and care options, intersecting situational factors, and clients accompanied by worried family members. Subsequently, leading to the extension of services to multiple people. Keeping the focus of communication on the client’s needs is important for effective professional communication. Effective professional communication leads to good customer service. Good customer service in the health sector works towards the goals of meeting the client’s health care needs.
Since health care administrators are often the first point of contact for clients they make the first impression of the service that the client can expect. Health care settings are busy and it is easy to get focused on tasks and forget the importance of actively participating in the communication process with other people. Actively communicating with all people is important to professional communication and good customer service. Good customer service is perceived by clients when they leave the health care setting satisfied that their health care needs have been met by competent and caring professionals.
Models of Communication for the Communication Process
At the core of communication is a process that involves a sender responsible for encoding a message in a way that can be decoded by the receiver of that message (Grimes et al., 2018). Consideration of communicating should be given to the context in which the communication will take place. Let’s review the following two models of communication and apply them to the context of health care settings.
A transmission model of communication is a linear, one-way process in which the focus is on the sender and the message to be communicated to the receiver. The assumption is the receiver receives the message but there is no attempt to clarify understanding of the message or to continue the conversation actively with the receiver (Grimes et al., 2018).
A health care setting example of the transmission model is a client watching a pre-recorded video explaining how to complete the forms in an intake package before their first appointment.
Ideally, in this situation, an interaction model of communication will take place between the client and the HCA once the client checked in for their first appointment and before the client sees the health care provider. If the intake form is complete, then the health care provider has all of the information needed to proceed with the encounter . The client will perceive an efficient office due to the good customer service that they received.
An interaction modelof communication is a process in which participants alternate roles of sender and receiver by incorporating feedback to communicate in an interactive way. For example, in the Osgood-Schramm model of communication one person encodes a message that is received and interpreted, then the receiver encodes a message to respond and sends that feedback back to the first person, who then interprets and may choose to respond by asking a question to continue the conversation (Smith, 2018). An interaction model of communication is then considered to be a cyclical process.
Figure 1.1 The Osgood-Schramm model of communication Source: Smith, 2018. [Image description].
Applying the Interaction Model to a HCA Communication with a Client
The HCA begins the conversation as the sender and the client is the receiver. The client receives the message to provide health card and confirm contact information, the client answers and then asks the question about how long the wait will be. The client’s response lets the HCA know the message has been received, but now the client has switched roles and asked a question, thus becoming the sender.
The first time the question is asked the HCA is discourteous in their response but the client receives the message that the HCA does not know how long the wait will be. However, the response “nope” sends the message that the HCA does not care that the client will be inconvenienced.
The client tries again and this time to send the message that by not knowing how long the wait will be that their anxiety is getting worse. The HCA responds with indifference and the client is told to take a seat. Thus, exacerbating the client’s anxiety which does not meet the client’s health care needs.
Imagine that instead of ending the conversation abruptly, the HCA had instead received and interpreted what the client said, acknowledged the client was feeling anxious, observed body language and what the client was saying, and provided a clear answer. This would have provided clarity to the client for what was expected next and likely reduced the client’s anxiety.
What do you think will happen next during this client’s encounter?
Will the client have their health care needs met?
Is this good customer service?
Considerations for Professional Communication
Communication Types
You will encounter many types of communication in health care settings and they are generally described as:
Written communication, a message using written words, text, symbols, and images.
Verbal/oral communication, a message expressed through spoken words using pitch, pace, and volume to convey a message.
Nonverbal communication, a message observed by watching another person’s body language such as facial expressions, eye contact, gestures, and movements (Garmaise-Yee et al., 2020)
It is important for both sender and receiver to be aware of the congruency between both verbal and nonverbal communication and seek clarification through feedback when there is incongruency perceived. In addition, it is important for both sender and receiver to consider their own bias when encoding and decoding what is being communicated. Preconceived ideas, whether we are aware of them or not, impact our ability to communicate effectively with other people.
Communication Channels
Channels of communication are the conduits for the message to move between the sender and the receiver (Grimes et al., 2018). Channels of communication in health care settings generally include:
telephone
posted mail
email
fax
social media
virtual conferencing software
face-to-face communication.
It is important for a sender to consider the type of communication, audience, and intended message when choosing a channel to send their encoded message. Choosing a channel that is incongruent with the type of communication, message, or audience may lead to miscommunication and block communication between sender and receiver. Once communication is blocked, the client may interpret receiving poor customer service or worse, not having their health care needs met.
For example, it would be incongruent to send confirmation of an urgent specialist appointment to a client using postal mail. Postal mail will take much longer to reach the client than an emailed message or telephone call. Some clients may not have email and require a telephone call. If you have not considered the intended audience’s needs (in this case, the client), they may end up missing their appointment. In the case of postal mail, there may be no opportunity for the client to ask questions or clarify the required preparation for the appointment; this poor customer service may lead to poor health care outcomes for the client. The client may have their appointment delayed because they did not receive the information in a timely manner or may come to the appointment unprepared. Subsequently, requiring the appointment to be rescheduled. One caveat to this is you must have expressed consent to email a message or leave a message on voice-mail.
Active Listening
Actively listening and allowing time for interpretation should be stressed no matter which communication type or communication channel is chosen. It is important to listen without distractions, listen for understanding by watching for congruency between spoken words and nonverbals, and seek clarification through feedback when there is any indication of a misunderstanding. This can be challenging in a busy setting, where there are multiple distractors such as telephone, multiple clients, multiple health care providers, and many urgent tasks. Active listening techniques can be learned and practiced and is a skill set valued in health care settings.
Courteous Communication
Courteous communication is essential to the communication process, professional communication, and good customer service. It is important to remember that clients and their families are often stressed when seeking health care services. This may mean that their communication may be discourteous. An HCA demonstrating professional communication will not take this personally and will remain courteous when communicating with others. Courteous communication starts with respecting others, actively listening, acknowledging, and responding with the appropriate amount of friendliness. In uncomfortable communication situations, people often compensate for their uncomfortableness by being overly cheerful and friendly. This can be interpreted as disingenuous and block professional communication.
Reflection
Consider a time when you were trying to tell someone something important, and they were looking down at their phone.
Consider a time when you experienced another person overcompensating by being too friendly.
How did this make you feel?
Discuss with a friend a time when you have had discourteous communication similar to the interaction that this chapter started with. Can you identify where in the interaction model of communication the breakdown happened?
Was it in the encoding of the message, decoding of the message, or in the feedback portion?
Demonstrating Professional Communication
You may be asking how can I demonstrate professional communication as the first point of contact in a health care setting? A health care administrator can display professional communication by:
Considering your role in the communication process and apply the interaction model of communication through active listening and providing feedback when necessary.
Greeting clients in a courteous manner and identifying yourself.
In-person, by wearing employee identification, greeting clients with a warm hello, and introducing yourself.
On the phone, by saying hello, the name of the Doctor’s office or department, then state your name and position.
Keep your tone of voice pleasant, and speech evenly paced, pitch and volume appropriate to what is being communicated. Enunciate clearly, and check that nonverbal body language is congruent with what is being spoken.
Review written work for grammatical errors, spelling errors, and tone before sending.
Considerations
Consider a time when you have entered an office, store, or searched out other types of service.
What made you feel welcome?
What made you feel unwelcome?
Is there anything you learned from those experiences that you will apply to the role of the Health Care Administrator?
Recognized the importance of professional communication to meeting the goals of health care settings
Applied the transmission model and interactive model of communication to examples of communication in health care settings
Explored the importance of communication types, channels, active listening, and courteous communication for professional communication in health care settings
Summarized what a Health Care Administrator (HCA) can do to demonstrate Professional Communication
Key Terms
Active listening: To listen without distraction to what is being spoken. Confirm congruency between verbal and nonverbal communication.
Bias: An inclination towards a certain point of view without consideration for other points of view.
Business Goods: Tangible items manufactured by businesses (Wade, 2020).
Caveat: Caution, warning, qualification, or forewarning.
Client: A term used in health care in place of the customer.
Competence: Possession of sufficient knowledge and/or skill level in a specific discipline.
Conduits: A way to transmit or distribute something.
Congruent: Verbal and nonverbal communication are matched.
Context: Interrelated conditions in which something occurs or exists.
Courteous: Pleasant and kind communication with respect for others.
Decoded/Decoding: Interpreting the message for themselves and turning that communication into thoughts.
Disingenuous: Face or insincere.
Encoding: Determines how a message will be received by the intended receiver/audience and develops the message, and makes adjustments accordingly.
Encounter: A client visit or appointment with a provider.
Expressed Consent: The client has signed a formal consent giving permission.
HCA: Health Care Administrators.
Incongruency: Verbal and nonverbal communication does not match.
Interaction Model of Communication: A process in which participants alternate roles or sender and receiver by incorporating feedback to communicate in an interactive way.
Message: Content to be delivered and interpreted.
Nonverbal Communication: Body language such as wave, eye contact, and mouthing words. Nonverbal communication is observed by watching another person’s body language, such as facial expressions, eye contact, gestures, and movements.
Quality of Life: General level of human happiness based on factors like life expectancy, educational standards, health, sanitation, and leisure time.
Receiver: The person responsible for decoding the message.
Sender: The person responsible for developing and sending the message.
Services: Intangible offerings by business that can’t be touched, stored or held (Wade, 2020).
Tone: Pitch of voice that expresses a mood or emotion.
Third Party Insurance Plans: Insurance plans which are covered by private companies such as Manulife, Sunlife, and Equitable Insurance companies. People have this type of coverage through extended health care plans offered by employers or purchased by the client.
Transmission Model of Communication: A linear, one-way process in which the focus is on the sender and the message to be communicated to the receiver.
Verbal/Oral Communication: A type of communication where the message is expressed through spoken words using pitch, pace, and volume to convey a message.
Written Communication: A type of communication where the message is communicated with written words, text, symbols, and images.
Figure 1.1: An image demonstrating that communication is a cyclical process. The person on the left encodes the message to be sent to the person on the right. The person on the right receives the message, interprets and then encodes a feedback response to be sent back to the person on the left. [Return to Figure]
Figure 1.2: The person’s nonverbals demonstrate pain. Hands cover eyes, and forehead is furrowed. The message can be read that this person is crying or sad. [Return to Figure]
Assessing What You Already Know Activity (Text-based)
Question 1
What displays of professionalism will a client expect to see when they encounter a health care administrator for the first time? Check all that apply.
The client will expect to see that the office is clean, tidy, and that the health care administrator is easy to identify, and processes their check in promptly.
Clients expect to wait for health care appointments and understand that the staff are stressed and grumpy.
The client will expect to be greeted by a friendly health care administrator upon check in.
Solution: Options 1 and 3 are correct. The client will expect to find a friendly team and a tidy office.
Question 2
Are health care offices considered businesses in Canada? Why or why not?
Yes, because health care are services provided to Canadians and health care providers are compensated.
No, because health care is free in Canada.
Solution: Option 1 is correct. Health care is not free in Canada it is paid through taxes. Complete the chapter reading to learn more.
Question 3
In the opening scenario do you think the health care administrator is focused on what the client needs? Why or Why not?
No, because they ignore how the client is feeling and are focused on the task of checking the client in for their appointment
Yes, if the client does not get checked in then they may miss their appointment and never see the doctor.
Solution: Option 1 is correct. Although updating the client information is important, health care administrators should identify client’s feelings and needs.
Question 4
Check all the modes of communication that a health care administrator might use.
Email or using Canada Post to mail documents.Social Media such as Facebook, Twitter, and Instagram.
Virtual conferencing and online software applications (apps) such as ZOOM, MS Stream, MS Teams.
Telephone or cellphone.
Solution: All the options are correct. Health care administrators use several ways of communication with clients.
Question 5
If the health care administrator is speaking to a client on the telephone which type of communication is being used? Check all that apply.
Non-verbal communication.
Written communication.
Verbal communication
Solution: Option 3 is correct. On the telephone you are using your voice and this is considered verbal communication. You are not using written or non-verbal communication. However, in some offices virtual conferencing software is used and if camera’s are turned on some nonverbal communication can be seen. [Return to Activity]
Check your Understanding (Text-based Activity)
Question 1
A client watches an instructional video on how to take their blood pressure and record the measurement on to a form. The client is expected to come to their next appointment with the form completed. This is an example of which type of communication model?
An interactive communication model.
A transmission communication model.
Solution: Option 2 is correct. This is a transmission model of communication because communication is linear with no option to clarify the instructions learned from the video.
Question 2
Complete the sentence using the options above. The sender conveys a message that needs to be:
Decoded by the receiver.
Guessed by somebody.
Decoded by the sender.
Solution: Option 1 is correct. Communication is a process that involves a sender responsible for encoding a message in a way that can be decoded by the receiver of that message.
Question 3
What do clients expect from a health care administrator? Choose all that apply.
That the health care administrator will be able to diagnose what is causing the client’s symptoms.
That the health care administrator knows how to do their job well.
That the health care administrator will actively communicate with them in a pleasant and respectful way.
Solution: Options 2 and 3 are correct, clients trust in a job well done and expects kind communication. Diagnosing a client’s medical issues is beyond a HCA scope of practice.
Question 4
Which of the following is the best way to greet a client who has just entered the office?
Ignore the client, after all, you are busy.
With a warm hello and/or a wave.
Look up, give a smile, and go back to what you were doing.
Solution: Option 2 is correct. Client expects a warm greeting and your attention.
Review scope of practice for health office administrators when communicating therapeutically.
Explore the importance of self-awareness in developing empathy for effective therapeutic communication.
Apply common behavioural and cognitive development theories to an example of changing perspectives.
Introduction
Health Care Administrators (HCAs) are often the first person that the client speaks to when booking their appointment, upon checking in for their encounter, and they are often the last person the client speaks to at the conclusion of the encounter. HCAs are the person family members speak to for updates on loved ones receiving health care. For these reasons, we propose that it is essential that HCAs continuously improve their therapeutic communication skills. Therapeutic communication is complex and requires a lifetime commitment of reflection, practice, making mistakes, and learning from those mistakes. This chapter focuses on defining therapeutic communication, the Health Care Administrator’s (HCA) scope of practice for communicating therapeutically, and self-awareness for developing effective therapeutic communication.
Assessing What You Already Know
Consider that people seeking health care are often feeling vulnerable. The way a Health Care Administrator communicates with them may impact their ability to access the health care they need. As you reflect upon the following questions and statements, consider the awareness you already have about communicating therapeutically with others.
Therapeutic, by its very definition, relates to curative treatments and that benefit both the mind and the body (Merriam Webster). Effective therapeutic communication requires people to be compassionate. This may seem to be innate in people but that is not always true. In health care settings, effective therapeutic communication is used to care for people so that their health care needs can be met. We propose that effective therapeutic communication skills can be learned through continuous self-reflection, empathy development, and practice.
Scope of Practice
Most health care providers are regulated under the Regulated Health Professions Act (RHPA) and the Medicine Act, 1991 (Ontario Government). Health care administrators (HCAs) are not regulated professionals and, therefore, follow the policy and procedures set by the regulated health care provider (HCP) for which they work. HCAs may be assigned tasks that involve controlled acts under the HCP supervision. It is important that HCAs are aware of their scope of practice, and if there is doubt regarding the performance of a task, or expression of behaviours, then the HCA should check with their immediate supervisor, or HCP for which they work. You may be wondering how this applies to communicating therapeutically?
Reflection
The following are just two examples to consider when deciding if something is within the scope of practice of a Health Care Administrator:
The use of therapeutic communication in providing a client with psychological therapy treatment would fall outside of HCA’s scope of practice and should be left to the health care provider.
Actively listening to a client, and acknowledging the stress a client is experiencing while they express the impact that caring for their father (who suffers from Alzheimer’s disease) is on their daily life, may fall within the scope of the HCA. The caveat is that the observations made are shared with the health care provider for further assessment.
Discuss with a classmate a potential situation in which you need to determine if it is outside or within the scope of practice of the HCA.
How will you make this determination?
What do you need to consider?
If you are not sure if it is within or outside of the HCA’s scope of practice who will you ask?
Empathy
Empathy is helpful when therapeutically communicating with others because you feel what they are experiencing with the person, and that shared feeling leads to connection and trust with the client. Empathy is an awareness of how someone is experiencing or feeling an emotional event because you have felt the same or similar emotion. Wiseman (2007), suggests that an empathetic episode occurs when the perspective of how someone is feeling is communicated to the person (who is having an emotional event) and then it is confirmed to be true by that person.
For example, a client shares with the HCA that they are extremely sad after the death of their beloved cat Smudgie. The HCA remembers the sadness she felt when her rabbit Hopper died and expresses to the client, “this is a difficult time as pets are like family.” The client then responds, “yes, I was closer to Smudgie than I am to some of my family”. The HCA responds with a caring glance and thanks the client for sharing.
Empathy: The Human Connection to Patient Care
Please note that the following video contains people in various healthcare situations that some viewers may find upsetting or triggering.
As you watch the following video, reflect upon moments when you have been in similar situations.
Can you feel the emotion that the people in the video are feeling?
If yes, then the emotion that you are experiencing is empathy.
Sympathy is not considered helpful when therapeutically connecting with another person because the sympathetic person feels sorry for the other person and can only imagine how they might be feeling. Often, when sympathizing with someone, people try to solve the person’s problem to assist them in moving outside of their emotional state. This may invalidate the person’s feelings making them feel judged, or as if they do not have a reason to be upset (Brown B., 2018). A person who feels judged or invalidated will shut down communication and it is likely that their needs will not be met.
For example, a client shares with the HCA that they are sad that they will have to quit their job to look after their mother who is in the early stages of dementia. The HCA feels terrible that the client’s mother is suffering from dementia and that the client must now lose income to look after their mother. The HCA responds by suggesting that the client looks into some inexpensive adult daycare centres. The client does not respond and leaves the encounter feeling confused because she interprets the HCA’s response to mean that the HCA doesn’t think that the client can look after their own mother. The HCA doesn’t understand how difficult it will be to have strangers care for their mother.
Empathy versus Sympathy
As you watch the following video reflect upon your use of similar phrases when expressing sympathy
Thinking about what you have learned about the difference between empathy and sympathy, what might you do differently in the future?
Wiseman (2007) proposes that empathy can not happen if people are not self-aware. To be self-aware one must examine their behaviours and the perspective from which they view the world, and also from reflecting upon communication interactions with other people. Then they must consider that the people that they communicate with will have different perspectives than they do. If we think back to the Osgood-Schram Model of Communication discussed previously, how often have you gone back and forth in the feedback phase and discovered that the receiver had not grasped the message you had sent? Have you ever reflected upon a conversation days later with someone and been surprised to learn that their interpretation of the conversation was completely different from yours?
Let’s consider where varying perspectives come from.
Interpretation and Perspectives
Interpretation and Perspectives
What do you see in the following image?
What do your classmates, friends, or family see in the following image?
Is it the same or different?
Image 2.1 Illusion image in which a person may interpret as a duck or as a rabbit or both. [Image Description]
If you read the description below the image, you may have been conditioned to look for a rabbit or a duck. Perhaps, you have experienced similar diagrams in your past; so, you may have known to look deeper into the diagram for further clues to what you should be looking for. Similarly, how one perceives communication with other people includes interpreting clues from the way the other person looks, talks, and behaves and comparing that to what they have been conditioned to expect by previous experiences. This conditioning is part of the development of your perspective.
You may be wondering how you came to develop the perspectives that you have and if you can change your perspectives. The first step in becoming self-aware is to reflect upon why you believe what you do? You can do this through examination of your attitudes, beliefs, and values. eCampus Ontario (2018) proposes that one learns attitudes, beliefs, and values over time and that they are central to the ongoing development of self. Effective therapeutic communication can then be developed by acknowledging and accepting that other people have different perspectives than you do. This does not make their experiences less valid than yours, just different.
Classical Conditioning
Prior experiences play a role in developing attitudes, beliefs, and values by conditioning our responses to situations we have experienced before. You may have heard this referred to as the lens from which we view the world. Consider that Ivan Pavlov, a Russian physiologist, discovered that dogs could be conditioned to salivate even when food was not present and that this discovery led to a field of behavioural study known as classical conditioning (Fields, T., 2020). Classical conditioning is a learning process in which coupling stimuli produces a response (Fields, T., 2020). In Pavlov’s studies, he paired his dog’s responses of salivation with food to the presence of the researcher bringing the food, noises, or lights (Fields, T., 2020). Once conditioned, the dogs salivated when the researcher entered the room, to specific noises, or lights even if there was no food present (Fields, T., 2020).
Let’s consider areas common to many people where classical conditioning may take place. These are just a few examples, consider what else you might add.
Culture, ethnicity, religion and/or spirituality
Life experiences such as interactions with culture, ethnicity, religion or spirituality are the ways in which people have been conditioned to interpret the world. These experiences work as base knowledge in which to make comparisons of a new experience to what is already known. Communication between people is blocked when one thinks that their way is the only correct way and attempts to impose their views on others.
Income and social status that includes education, economic, and environmental factors
Consider that income and social status are number one on the list of the social determinants of health (Pan-Canadian Health Inequalities Reporting Initiative, 2020). Meaning social determinants that affect the health outcomes for people. Income and social status can be related to the amount of or type of educational experiences a person has had. For example, people who have had opportunities to pursue higher education may have the option to pursue a career in which they receive a lot of satisfaction. A person who could not afford to pursue post-secondary education may have limited options for the type of career they may wish to pursue. Economics determines the type of environment that people live in, the types of nutritional food they eat, the educational supports both at school and at home, and access to social and recreational activities (Pan-Canadian Health Inequalities Reporting Initiative, 2020).
You might be wondering how do these examples relate to self-awareness when communicating in health care settings?
Consider that a child who has grown up in poverty, whose adults had to work multiple jobs to put food on the table, may not have had regular medical appointments and only went to the doctor’s when extremely ill.In this situation, they may not seek out health care for what they perceive as minor symptoms. They may be conditioned to go to work or go to school and tough it out, meaning go while sick because the cost of losing pay to go to a doctor’s appointment or look after an unwell child is not an option. Alternatively, a child growing up in affluence may perceive that everyone goes to the doctor’s when they are running a fever or have a twisted ankle from soccer practice since they have been conditioned to perceive this as a way that everyone lives.
Self-awareness of how you have been conditioned to perceive when to seek health care may impact how you perceivea client’s decision to book an appointment. If you were conditioned to believe to go to the doctors regularly, then you may find yourself judging a client for not bringing their ill child in sooner, and your non-verbal communication may project that belief, whether you intend to or not.
Reflect
Take a moment to share with a friend something you grew up believing or experiencing that you thought everyone believed or experienced.
Is this the same belief or experience that your friend had?
If yes, has your friend been raised in similar circumstances in which life experiences are similar?
If not, then what has your friend experienced that is different?
Do you think that your previous experience has conditioned you to perceive future experiences in the same way?
Has this impacted what you value?
Cognitive Development in Changing Perceptions
Jean Piaget’s Cognitive Development Theory proposes that as people mature, they take what they know and compare it to something new, then develop a new way of thinking about it and that this follows a sequence starting from the time people are born (DeWolfe, T.E., 2019). Cognitive Development Theory can therefore be considered in answering the question, can you adapt or change your perceptions?
Consider in the Concrete Operations Stage, the person can comprehend other people’s viewpoints and in the Formal Operations Stage, abstract ideas and concepts like justice can be understood, even if not directly experienced (DeWolfe, T.E., 2019). We propose that if people are aware that they might have been conditioned to believe what they do then when they come across someone with a different perspective if they are in the concrete operations stage, they accept that people have different perspectives and if they are in the formal operations stage, they can reason out the two ideas and determine if they will change their thinking.
Application to an Example
Jordan was raised in a home where people mistrust medical personnel and they are skeptical to have vaccinations. This skepticism came from a poor experience a parent had when receiving a vaccination many years ago. That interaction now impacts Jordan’s parent’s life and those around them. However, if Jordan studies anatomy and physiology they may come to understand how vaccinations work and that not everyone believes what Jordan’s parents do.
Jordan will consider where the skepticism to vaccinations came from, compare it to what they are learning about vaccinations, and may come to the conclusion that vaccinations are important to overall health and well-being. In this situation, Jordan has reasoned out what they were conditioned to believe by comparing it to the new information that they have learned. No matter which decision Jordan makes whether to have vaccinations or not, they will have made an informed decision.
Reviewed scope of practice for health office administrators when communicating therapeutically.
Explored the importance of self-awareness in developing empathy for effective therapeutic communication.
Applied common behavioural and cognitive development theories to an example of changing perspectives.
Key Terms
Attitudes: Immediate disposition towards a concept or object.
Beliefs: Ideas based on your previous experiences and convictions often serve as a frame of reference for viewing the world.
Caveat: A caution, warning, qualification, or forewarning.
Classical Conditioning: Classical conditioning is a learning process in which coupling stimuli produce a response (Fields, T., 2020).
Cognitive Development Theory: Jean Piaget’s Cognitive Development Theory proposed that people develop their thinking by comparing new experiences to what they already know. This theory proposed that cognitive development follows a sequence.
Concrete Operations Stage: This is a stage in Jean Piaget’s theory where a child can comprehend other people’s viewpoints (DeWolfe, T.E., 2019).
Controlled Acts: May only be performed by authorized regulated health professionals (CPSO, 2021).
Empathy: Awareness of how someone is experiencing or feeling an emotional event because you have felt the same or similar emotion.
Formal Operations Stage: This is a stage in Jean Piaget’s theory where abstract ideas and concepts like justice can be understood even if not directly experienced (DeWolfe, T.E., 2019)
Innate: inherent or born with.
Invalidate: To view the person’s issues as if there is no merit or foundation.
Judged: A formed negative opinion.
Scope of Practice: Work within the limits of what you have been educated or trained to do.
Self Awareness: Examination of a person’s own behaviours and perspective of themselves.
Social Determinants of Health: Social determinants like income and social status that affect the health outcomes for people.
Stimuli: An agent that produces a response
Sympathy: To feel sorry for someone else.
Therapeutic Communication: Relates to treatments that are curative and benefit mind and body (Merriam Webster, n.d).
Values: Core concepts and ideas that you categorize as good or bad, right or wrong, or what might be worth making a sacrifice for.
References
Brown, B. (2018). Dare to lead : brave work, tough conversations, whole hearts. Random House.
Figure 2.1: Illusion image in which a person may interpret as a rabbit or as a duck. [Return to Figure]
Assessing What You Already Know (Text-based Activity)
Question 1
Consider the following examples and choose the statement that best reflects how you would respond to this situation.
Statement one: Juan, your friend has just found out that they did not pass their AP midterm exam. Juan is visibly upset and tells you that if they have to take this course again they will not graduate with his peers. You respond therapeutically by:
Telling Juan that you had that same AP teacher and that this is going to be a challenging semester for them and you wish them good luck.
Telling Juan that this is a challenging situation and asking Juan what you could do that would be helpful.
Telling Juan about a time that you failed a midterm and how it motivated you to study harder and you ended up with 80% as your final grade.
Solution: The correct response is option two. This is an example of therapeutic communication you have acknowledged Juan’s feelings and asked how you could help.
Statement two: A client completing registration for an upcoming surgery mentions to you (the health care administrator) that they are extremely worried about the upcoming surgery so much that they have not been sleeping. You respond therapeutically by saying:
That is a fairly common before surgery but you don’t need to worry the surgeon is very good.
Yes, waiting for surgery can be worrisome. I will make a not for the surgeon to prescribe something to help you sleep.
Yes, waiting for surgery can be worrisome. When you speak to the surgeon mention that you are having trouble sleeping.
Solution: The correct response is: Option 3. You have validated the way the client is feeling and you have stayed within your scope of practice by asking the client to speak to the surgeon about this concern. Return to the Activity
Media 3.1 ASL Scene [Video]. CC-BY-NC-SA 2021. Conestoga College.
Learning Objectives
Explore the types of health care teams and their role in the delivery of health services.
Describe therapeutic communications tools utilized by health teams to support patient outcomes.
Build collaborative communication strategies to function as a member of health care teams.
Analyze the role of self-awareness in team-based communication.
Introduction
A health care team is a group of professionals contributing to the care and treatment of a patient. The team typically consists of professionals from interdisciplinary areas such as physicians, nurses, and technologists. Communication among members of a health care team is essential for quality patient care and effective team performance. Building cooperative and respectful team relationships assist in a patient’s perception of the care they are receiving. Critical patient information needs to be shared with members of health care teams to ensure a collaborative approach. Conversely, lack of communication creates opportunities for errors to occur, quality of care diminished, and can place patient safety at risk.
Assessing What You Already Know
As you complete this activity reflect on what you already know about teams and team dynamics.
Many components are involved in working effectively in a health care team. Communication channels bring the team together to enable patient-centred care. Therapeutic communication is an important tool that helps put the patient at ease and builds trust in the health care team. When managing patient care each member of the team will have their own interpretation of the information presented and how the information is actioned can be dependent on each member’s uniqueness, expertise, and level of involvement within the team.
Interpersonal communication is the exchange of information between two or more people involving verbal and nonverbal methods. Developed interpersonal communication skills are vital to ensure collaboration with team members to support the best interest of patients. In most health care settings, teams are formed to support patient care and outcomes. A variety of teams are found in health care settings. They can be described as interprofessional care, collaborative care, shared care, or team care.
Common Types of Health Care Teams
Primary care is the fundamental level of health services and contacts a patient has with the health care system. Primary health care teams are composed of health care providers who provide comprehensive health care within the community. As an example, a primary team could consist of a group of family physicians, nurse practitioners, practise managers, pharmacists, and health care administrators (HCAs) working to support the team. Primary care teams work to meet public and patient expectations, optimize health outcomes, and work to support and sustain the health care delivery systems.
Secondary care is concentrated health services. Secondary health care teams are composed of specialized health care providers who provide expert and specific care to patients who are often referred to them by a primary health care provider or team. Secondary health care teams are often found in a hospital setting. As an example, a patient is referred to a hospital outpatient clinic for care or inpatient emergency care. The team composition can include specialized physicians such as a cardiologist, technicians, nurses, dieticians, and HCAs.
Tertiary care is advanced and highly specialized health services. Tertiary health care teams are found in health care settings focusing on advanced treatments and extended procedures such as cancer treatment or neurosurgery. Patients are referred to tertiary health care teams by either the primary or secondary health team. Tertiary team composition typically, includes medical specialists, nurses, technicians, and HCAs.
Team Communication
Think of a time when you worked as part of a group or team. Consider the following reflective questions:
What worked well from a communication perspective?
How did team members cooperate with each other?
What did not work well and why?
How would you improve areas where communication did not work?
Collaboration and Open Communication
Collaboration described in the context of the health care team involves professionals undertaking interdependent roles working together, investing in shared strategies, problem-solving, and decision making to design care plans supporting patient outcomes. Inherently, effective teams who coordinate care successfully establish methods of communication, inclusive of data management systems, team meetings, and responses to rapidly evolving public health needs.
Collaboration is a collective action focused on achieving a common goal “in a spirit of harmony and trust” (Franklin, Bernhardt, Lopez, Long-Middleton, & Davis, 2015).
Interventions to support collaborative team dynamics include:
remove the reliance on continuing the way things have always been done, try new approaches
encourage change, look for opportunities to find solutions, and improve processes
support transparency in all interactions
recognize and celebrate collaboration within the team
Judgement and Decision Making
Many thinking strategies are needed in a health care setting to ensure quality patient outcomes and accountability. Health care team members typically utilize and apply knowledge based on their scope of practice and role. Clinical reasoning is a process undertaken by health care professionals to understand a patient’s problem, analyze information, and implement interventions. Health care decision making is also a process inclusive of definable steps in a sequential order.
Figure 3.1. Individuals and teams often have several choices for decision-making as represented by these three doors. Source: “Three Doors” by Jeremy Brooks is licensed under CC BY-NC 2.0 [Image Description]
Self-Awareness and Identity
Most humans form self-identities through their communication with others, and much of that interaction occurs in a group context. A group may be defined as three or more individuals who affiliate, interact, or cooperate in a familial, social, or work context (Grimes M. et al., 2018).
One should aim to acquire an understanding and develop a sense of when it is important to be the leader, the collaborator, and indeed, at times, the follower. Ultimately one moves back and forth between these roles over the course of a relationship, including the relationship with the client and relationships within interprofessional collaborative teams (Wagner. J. 2018).
Self-Awareness Exercises
Developing self-awareness provides the opportunity to adjust the thoughts and personal interpretations, as you change your interpretations emotions change. Try researching practices surrounding the following:
Mindful meditation-being acutely aware of what you are feeling in a moment
Observing others
Journal thoughts and ideas
Personal visualizing
Self-reflection
Reflective questions:
How do these practices relate to the development of therapeutic communications skills within the health care team context?
Could you add an additional practice you are aware of not listed here? Why did you choose this practice?
Technology and the Impact on Health Care Team Communication
Technology has enhanced the accessibility of team communication in health care settings with the ability to communicate through the variety of devices and channels available. Connected health care spaces enables more agile treatment plans to develop within the team. Health care innovation allows the sharing and analyzing of patient data with team members to support decision-making capabilities. Technology can strengthen therapeutic communication team relationships when used in a consistent manner to update team members and share information practices.
Navigating Challenging Conversations and Workplace Conflict
An integral part of being a member of the health care team involves navigating challenging or difficult conversations. These conversations may arise based on a number of contributing factors such as stress, fatigue, time of day, a patient who is in pain, angry, or appears aggressive. We should attempt to approach these situations in a non-judgemental manner and avoid labelling someone as hostile or unpleasant. Practicing therapeutic communication techniques can help to de-escalate encounters.
Conflict may typically be thought of as being negative, and it understandably can produce feelings of anxiety for many people. However, conflict is not always negative. In fact, conflict can be positive and productive, leading to creative approaches, reinforced working relationships, and more efficient outcomes. Positive conflict is a conflict where there are positive outcomes—that is, the focus remains on the issues and all parties respectfully and professionally search for outcomes that are agreeable to everyone involved (Ashman M. 2018).
Consider this Scenario
Zahara works as an occupational therapist on a health care team in a regional hospital. Zahara is recognized as having a positive attitude among team members and clients feel supported in their face-to-face encounters.
Unfortunately, Zahara does not like the documentation side of the role and often does not complete chart notes quickly after seeing patients. Team members find this challenging when reviewing the chart and this delay can impact care decisions.
What is the conflict in this scenario?
Do Zahara’s actions show a lack of consideration for the health care team?
How might this impact client care?
Will this impact Zahara’s career?
How can this situation be addressed effectively using therapeutic communication strategies?
Diversity and the Health Care Team
Diversity in care teams involves members from multiple races, ages, genders, ethnicities, and orientations who present with various backgrounds and experiences. Health care teams composed of diverse members often have a wide range of decision-making and critical thinking abilities as they relate to health care decisions leading to more positive outcomes. Unconscious bias can impact decisions as a result of this some teams do not embrace diversity. Developing an awareness of unconscious bias allows for strategies to prevent and address it.
Check Your Understanding
After completing the chapter content, complete this activity to assess your understanding of concepts presented.
Reviewed the complexity of health care delivery systems makes the ability to work effectively as a member of the health care team an essential attribute.
Explored different types of health care teams.
Considered strategies for effective and productive communication channels.
Key Terms
Accountability: The act of being responsible for an action.
Affiliate: Association such as a member/ To contribute to group working conditions (Merriam Webster, n.d).
Agile: Ability to move quickly and easily (Merriam Webster, n.d).
Bias: An inclination towards a certain point of view without consideration for other points of view.
Collaborative: To work together to achieve a common goal.
Components: To contribute to a larger whole in your scope of practice.
Composition: The make-up of the team who is involved.
Comprehensive: Having vast knowledge on a topic or to cover completely.
Conversely: Opposite way of looking at something.
Implementation: To enact or start something such as a rule.
Innovation: New idea, method, or product (Merriam Webster, n.d).
Interdependent: Dependent on each other.
Interdisciplinary: More than one branch of knowledge.
Interprofessional: More than one branch of knowledge.
Neurosurgery: Surgery of the nervous system.
Primary: Main care provider.
Reasoning: To apply reasoning techniques to situations of distress.
Reliance: A thing or person someone might rely on for assistance.
Secondary: Coming after main care.
Sequential: Following a logical order.
Tertiary: Third order or level.
Transparency: Open and direct approach (Merriam Webster, n.d).
Utilized: A device that can be used for practical assistance or someone a client can ask questions of.
Franklin, C. M., Bernhardt, J. M., Lopez, R. P., Long-Middleton, E. R., & Davis, S. (2015). Interprofessional teamwork and collaboration between community health workers and healthcare teams: An integrative review. Health Services Research and Managerial Epidemiology. doi:10.1177/2333392815573312
Figure 3.1: Individuals and teams often have several choices for decision-making as represented by these three doors. [Return To Figure]
Assessing What You Already Know (Text-based Activity)
Question 1
Recall the video shown at the start of the chapter showing a discussion between two health care team members, HCAs. From the options below, select the statement which describes your initial impression of the situation:
One team member is not communicating effectively to assist a patient with their needs.
This is simply a miscommunication and does not affect patient needs.
Both team members are not communicating effectively to assist a patient with their need
Solution. The correct response is option three. Communication breakdown usually involves a series of missed opportunities and a failure to collaborate together. Read the chapter to explore health care teams and communication.
Question 2
As you complete this activity reflect on what you already know about teams and team dynamics.
Poor team work practices can lead to the following consequences. Select all that apply:
Solve problems
Incomplete communication
Higher risk of errors
Failing to utilize expertise
Solution. The correct response is Options two, three and four.
Option two. Incomplete communication. In many situations incomplete communication could affect patient care and incomplete hand-over or transfer of information can and will occur. Read the chapter to explore health care teams and communication
Option three. higher risk of errors. This could be a serious consequence when communication breaks down, it places patient safety at risk. Explore this chapter to discover communication strategies of productive health care teams
Option four. failing to utilize expertise. The failure of productive team practices can result in some teams members not contributing fully to positive patient outcomes. Read the chapter to explore health care teams and communication. Return to Activity
Check your Understanding (Text-based Activity)
Question 1
Select the term which applies to this statement: When working with others on a health care team you accept responsibility for your actions.
Accountability
Credit
Praise
Solution. The correct response is Option one. Accountability. All team members are accountable for their actions in a health care setting to support patient care and assist with positive care outcomes.
Question 2
When working with others it is effective to avoid decisions that favour one point of view over another based on a close minded approach. Select the term which describes this action.
Tolerance
Preference
Bias
The correct response is Option three. Bias based decisions create challenges for teams to be productive and often discounts therapeutic communication based approaches.
Question 3
Interprofessional care includes, select all that apply,
Clear verbal communications
Two-way communications between professionals
Respectful communication
Solution: The correct response is Options one, two and three. Interprofessional care is integral to a client’s overall care. It includes respectful, clear two way communication between all professionals. Return to Activity
Recognize the role of interprofessional communication in health care settings.
Describe the elements and goals of interprofessional communication.
Explore behavioural practices influencing interprofessional care teams.
Apply strategies for managing conflict within the context of interprofessional teams.
Introduction
Interprofessional communication occurs when health professionals communicate with each other, with patients, their families, and with the community in general. Multidisciplinary or interdisciplinary are terms used to describe the makeup of health care teams. Individuals from different health care disciplines approach a patient or care of a patient from their own perspective. The primary goal of these teams is to integrate expertise from separate disciplines into a single consultation to support patient care and outcomes. This encompassing care is often referred to using the short form IPC meaning interprofessional care.
Assessing What You Already Know
Consider your pre-existing knowledge surrounding interprofessional teams as you complete this activity
Role of Interprofessional Communication in Health Care
As the nature of health care continues to evolve the more interwoven health care professionals are in coordinating care following an interprofessional-focused approach. In the past health care management was often physician or disease-focused. Recently, this foundation has since migrated to a robust team of health professionals working together for patient care and disease prevention. This seemingly harmonious approach will not occur without reflective practice, mindful effort, and understanding the importance of communication. Learning to function effectively within the interprofessional dynamic begins through the establishment of mutual respect and trust.
Establishing Trust-Interprofessional Practices
As a self-check consider the following definition as well as the reflective questions within the context of communication.
Trust (noun): Belief in the reliability, truth, ability or strength of someone or something, as in “good relationships are built on trust.”—Oxford English Dictionary
Questions for reflection:
Does my personal competence and follow through establish trust with others?
What experiences can I offer to support cooperation while working with others?
How do I manage stressful communication-based situations with others?
Elements of Interprofessional Communication
Six interdependent competency domains have been identified to achieve the goal of interprofessional collaboration (Canadian Interprofessional Health Collaborative CIHC, 2010, as cited Garmaise-Yee et al., 2020) ). These are defined as the “knowledge, skills, attitudes, and values that shape the judgements essential for interprofessional practice” (Canadian Interprofessional Health Collaborative, 2010; as cited in Garmaise-Yee et al., 2020) and include:
Interprofessional communication
Patient/client/family/community-centred care
Role clarification
Team functioning
Interprofessional conflict resolution
Collaborative leadership
The first two competencies, interprofessional communication and patient/client/family/community-centred care have a strong influencing role in all healthcare situations, so as shown in figure 4.1, they encircle the other four competencies. The next section explores the 6 competencies further.
Figure 4.1 Source: National Interprofessional Competency Framework. The six goals of interprofessional collaboration. [Image Description]
The first two competencies, interprofessional communication and patient/client/family/community-centred care have a strong influencing role in all healthcare situations, so as shown in figure 4.1, they encircle the other four competencies. According to the Centre for Interprofessional Education, Toronto Academic Health Science Centre (2017) the six competencies identified are explained further as outlined in the next section.
Interprofessional Communication Competency
Explored in the Professional Communication chapter elements of effective communication apply relative to interprofessional communication.
Behavioural examples to strengthen interprofessional communication include the following:
communicate clearly using terminology understood by the collaborative team, patients, and family
ensure complete information is provided as directed
be responsive to changing needs and circumstances
provide information in a timely manner, avoid withholding sensitive information
use recognized and accepted communication channels (checklists and templates are helpful)
review updated information when it is available
demonstrate respect with all members of the interprofessional team
model and create an environment of mutual trust, respect for privacy and confidentiality, while maintaining patient dignity
Patient/Client/Family/Community-Centred Care Competency
Patient-centred care encircles the foundational belief clients/patients and their families are partners in the design and development of care plans, all functioning as members of one team. Input is gathered collaboratively from team members to support engagement through each stage and process of care plan implementation.
Behavioural examples of patient-centred care involve:
actively seeking clarification from patients, their families, and the interprofessional team when involved with the planning, coordination, and implementation of patient care plans
support and encourage access to community resources and involvement
promote access to preventive care measures by applying therapeutic communication strategies and information sharing
Role Clarification Competency
This involves developing an understanding of your role and the role of all collaborative professionals on the team. The ability to apply this knowledge correctly achieves care goals for patients and supports the health of the community within the bigger picture. This understanding helps to identify gaps in care, addresses duplication of resources, and enhances the implementation of care plans. The HCA can model a variety of behaviours to support this.
Behavioural examples of role clarification include:
demonstrate an understanding of your own role as well as the roles of each member of the team
consider the roles of members while respecting the diversity of the team members as they relate to patient care and team dynamics
utilize professional development opportunities to expand knowledge of interprofessional educational practices
practice self-awareness in view of one’s own limitations and the need for consultation with other members of the healthcare team based on roles and professional scope
Team Functioning Competency
When interprofessional health care teams form it is common practice to establish ground rules of how the team will work together.
Behavioural examples of team functioning include:
Recognize and share with the interprofessional team individual and systemic power discrepancies and gaps expressed by patients and their families.
Participate in the development of team values and goals.
Support team psychological safety to establish a sense of confidence that the team will not embarrass, reject or punish someone for speaking up.
Advocate against and avoid harmful behaviour to a team i.e. gossip, destructive comments rumours that impact team morale and development.
Interprofessional Conflict Competency
Conflict is a natural event occurring when groups or teams are working together. Joan Wagner provided this insight from the publication Leadership and Influencing Change in Nursing, for centuries, people accepted adversarial disputes and harsh conflict as a by-product of human nature. This acceptance caused people to analyze only how conflict could be resolved, that is, how they could make it go away (Wagner, 2018).
Conflicts and disagreements are inevitable with interpersonal communication. Several factors that influence conflict can include, role boundary concerns, accountability and the scope of practice of those involved in the communication stream. Recognizing and managing conflict effectively supports therapeutic communication goals.
Types of Conflict
Categorizing and understanding the types of conflict arising assists with framing resolutions. Here are four types of common conflict occurring within interprofessional teams (Wagner. J. 2018).
Data/Information. These encompass elements inclusive of, lack of information, interpretation of information, incomplete information, and differing assessment procedures.
Values. Conflicts related to day-to-day values and self-definition.
Relationship. These conflicts stem from stereotypes, misperceptions, and poor communication efforts.
Structural. Conflicts relate to how a situation occurs, who is involved in the decision-making, and unequal power and authority (Wagner. J. 2018).
Behaviour examples of interprofessional conflict resolution and management include:
Constructively address potential areas for conflict arising.
Seek out solutions to support the resolution or to prevent conflicts.
Support mutually agreed solutions in an appreciative manner
Keep an open mind with differing views.
Avoid blaming, and judging for optimal patient outcomes.
Communicate with empathy
Listen without interrupting
Be available for communication opportunities
Demonstrate support
Use a client-centred approach to frame discussions.
Use an evidence-informed approach to make decisions.
Be open to hearing varying disciplinary perspectives.
Engage in self-reflection.
Engage in respectful discussions.
Reflect on the perspectives of all team members.
Share your perspective and rationale (Garmaise-Yee et al., 2020)
Figure 4.2 shows a graphical representation of conflict resolutions strategies
Figure 4.2 Managing Conflict Strategies. Source: Introduction to Communication in Nursing. Garmaise-Yee. J. et al (2020) [Image Description]
Collaborative Leadership
Collaborative leadership transpires when interprofessionals work together with patients, families, to provide as well as assess the care and the services provided. Each professional understands their role and accountability all with the goal of promoting healthy outcomes.
Behavioural examples of collaborative leadership include:
Encourage participation in the coordination of planning care to achieve care goals.
Designate accountability, recognize and address role overlap.
Respectfully acknowledge appropriate expertise when needed in order to help guide patient/client needs.
Advocate for patients, clients, and their families to facilitate the integration of care.
Collaborating with Interprofessional Teams to Support Patient Outcomes
Collaboration is especially significant in the healthcare environment to meet the increasingly complex demands of patients with multiple comorbidities. Collaboration pools resources to facilitate improvements in cost, availability, and quality of care (Tsakitzidis et al, 2016).
Scenario
Social media can be used to create virtual communities in health care environments. Many individuals also engage in social media outside of their professional practice. Typically, you do not have members of your organization on your personal social media platforms. Today, a friend of yours mentioned she saw a personal post by a member of your team which stated: “I have never met a more difficult group of HCA’s in our organization”
Reflecting on this. Consider these questions:
What would you do?
How can this be effectively handled? Should it be handled?
Check Your Understanding
Apply your knowledge from the chapter as you complete this review activity
Explored the elements involved in interprofessional communication.
Reviewed the six domains of interprofessional competency framework as applied within the health care environment.
Highlighted the behaviours to support conflict resolution when arises within the team and focused on areas of collaborative opportunities to improve care outcomes richly available through interprofessional teams.
Key Terms
Accountability: Accepting responsibility for one’s actions.
Adversarial: Involves two opposing sides.
Advocate: A person who will support and ask questions for those in a position that is unable to.
Appreciative: Showing gratitude.
Competency: Having acquired sufficient knowledge for their scope of practice.
Comorbidities: Two or more diseases present in a patient.
Constructively: In a way for a beneficial purpose.
Disciplines: Subject area or field of study.
Discrepancies: A variance or disagreement.
Domain: The area in which one’s scope of practice resides.
Encompassing: Everyone in the circle of care has complete knowledge of the situation at hand.
Harmonious: Everyone involved in reaching an agreement.
Interprofessional Communication: Communication taking place between health care professionals with clients/patients, families, and the community in general.
Interwoven: To mix or blend knowledge in relation to a person’s circle of care.
Migration (migrated): Moving from one location to another.
Misperceptions: Inaccurate or false information (Merriam Webster, n.d).
Multidisciplinary: Combining or involving more than one professional area of practice (Merriam Webster, n.d).
Preventive: Able to be avoided.
Rationale: Explanation of controlling principles, such as practice, belief, opinion, or phenomena (Merriam Webster, n.d).
Self-aware (self-awareness): A person being aware of their own individuality or personality.
Sensitive: Aware of the feelings and attitudes of those around you.
Systemic: Integral to a predominant economic, political practice, or social.
Tsakitzidis, G., Timmermans, O., Callewaert, N., Verhoeven, V., Lopez-Hartmann, M., Truijen, S., Meulemans, H., & Van Royen, P. (2016) Outcome indicators on interprofessional collaboration interventions for elderly. International Journal of Integrated Care, 16(2): 5. doi: 10.5334/ijic.2017
Figure 4.1: An image showing the six domains and goals of interprofessional communication in a circle detailing the connection of all six domains. [Return To Figure]
Figure 4.2: An image demonstrating strategies for managing conflict for interprofessional health care teams. [Return To Figure]
Assessing What You Already Know (Text-based Activity)
Question 1
Recall the recorded scenario at the start of the chapter with a new member joining a health centre and assess the communication by selecting one of the following statements:
The exchange was appropriate and the HCA was friendly and supportive for the new team member.
It did not start off ideal, however, the HCA was able to bring the conversation back to assist the new member.
Nothing was resolved in this scenario.
Solution: Option 2 is correct. Both the players in this scenario did not immediately introduce themselves and this led to an initial misunderstanding of why the new team member was here.
Question 2
Consider this statement: Sharing relevant information and expertise is an important part of effective interprofessional health care teams, but it is not the only element which enable health care teams to work well. Select from the statement below, what may also help.
Team members aim to be responsive to hearing the perspectives of other team members.
Collaborative decisions can be made independently to reflect the specialized information.
Team member must be willing to not be influenced by the information shared by other team members.
Solution: Option 1 is correct. Interprofessional teams bring a variety of insights and perspectives to support and address patient needs in a collaborative format. Continue exploring this chapter to learn more about interprofessional communication.
Question 3
Listen the following statement and choose true or false. Communication is not always the best process through with team roles are expressed and team goals are achieved.
True.
False.
Solution: The statement is false. There are a variety of important behavioral roles performed by different members of interprofessional health care teams. Communication is the process through with team roles are expressed and team goals are achieved. Return to Activity
Check your Understanding (Text-based Activity)
Question 1
Interprofessional teams will experience conflict. Conflict can encompass which of the following, select all which apply:
Clear expectations.
Lack of or incomplete information.
Lack of shared team values.
Communication disruptions due to misconceptions or stereotyping.
Solution: Options 2, 3 and 4 are correct. Clear expectations will avoid conflict not create it. When expectations are clearly defined it supports movement forward within the team.
Question 2
In a clinic or hospital setting you want a professional team that will advocate.
True.
False.
Solution: The statement is true. A professional team should support and advocate all of the members. Return to Activity
The Helping Interview: A Common Therapeutic Communication Tool
Explore the health care administrators role in the helping interview.
Evaluate effective and ineffective communication techniques.
Identify blocks to effective therapeutic communication.
Introduction
When people are asked if they have been on an interview, most people think they are being asked if they have been on a job interview. There are many types of interviews that go beyond employment interviews. For example, a talk-show host interviewing a famous guest or informational interviews that are sometimes referred to as coffee chats. All interviews have similar components such as a conversation between two or more people, questions that gather information, and a common interest between the people involved. Since health care involves helping people, almost everyone who works in health care is in a helping role. The helping interview refers to an interview with a person seeking help and the people providing that help. In this chapter, we will consider the client encounter and explore the components within the phases of the helping interview, the role of the health care administrator, and evaluate effective and ineffective therapeutic communication techniques and behaviours.
Assessing What You Already Know
As you reflect upon the following questions and statements consider what you already perceive about interviews.
When studying the helping interview framework it is helpful to break it into phases and evaluate the components that make up each phase. Once you have identified the components of the helping interview, you can begin to reflect upon how you can build upon the skills you already have, and develop the skills you are missing. It should be noted that there may be multiple cycles of the phases with differing helpers during a client encounter. Let’s begin by breaking the helping interview framework into the following three phases:
Build Trust
Identify the Need
Resolution and Next Steps
Build Trust
Clients seek health care most often when they are ill or feeling unwell. Most clients trust that the health care provider (HCP) is competent due to their credentials and education. In order for clients to be honest about uncomfortable or embarrassing symptoms, the client must believe that the HCP will listen without judgement and treat the symptoms competently. The College of Nurses of Ontario (2006) list trust as one of the five components of the nurse-client relationship and state that trust is critical because clients seek care when they are vulnerable. The College of Physicians and Surgeons of Ontario (2007, page 7) states that “trustworthiness is the cornerstone of the practice of medicine”. Helpers can not help patients without trust between helper and client (CPSO, 2007). Fine & Glasser (1996) suggest that trust is a fundamental element in all helping professions. Since HCAs are part of the health care team, an extension to the HCP, and most often the first person the client or their family interacts with during an encounter, trust then begins with the HCA.
Building Trust Upon Booking Appointments
Clients arrange health care appointments on the phone, through email, or through intake forms. If the client is having a serious health issue they will typically call, or you will follow up with a request to call. It should be noted that client incoming calls are triaged and the client is directed according to the urgency of their symptoms. For example, if the client is calling about chest pain or excessive bleeding, you would keep them on the phone and call an ambulance on their behalf. If the symptoms are urgent such as a broken bone you direct them to the nearest emergency room. If their symptoms warrant an urgent booking then you schedule accordingly. It is at this time that you begin the trust-building phase of the encounter.
Consider the Following Scenario
A client phones to make an appointment for his 3-year-old child who suffers from frequent ear infections.
HCA: Hello Dr. Vunderful’s office, Please hold Client: Hello, Hello…. oh, they put me on hold
Five minutes later HCA: Sorry to keep you waiting. How may I help you? Client: Hi this is Regie Singh, that was a very long wait. I am calling about my son Jagmeet. I think he has another ear infection. HCA: Hi Regie, Oh, I am sorry to hear that. It is very busy as you can tell from your wait. I can get Jagmeet in the day after tomorrow at 2 p.m. Client: I don’t think he can wait that long. He is very warm and cranky. Can we come today? HCA: Sighs heavily. Umm, not really, it is busy. Did you take his temperature? What is it? Client: No, I don’t have a thermometer but he is super warm. I already had to take the day off work today are you sure you can’t get Jagmeet in today? HCA: Well I am going to use an emergency spot. Come at 4 p.m. I hope he really is as sick as you claim. Client: Thank you? (unsure questioning tone to his voice)
In the scenario above do you think that Regie trusts that Jagmeet will be taken care of? The HCA has not demonstrated compassion to Regie who has stayed home from work to take care of Jagmeet, the HCA has not displayed competence by asking more questions about Jagmeet’s state, and the HCA is disrespectful by suggesting that Regie is lying about how sick Jagmeet is. In this situation, it is likely that Regie does not trust that the HCA (and by extension the health care provider) cares about Jagmeet. This has set the tone for the encounter and trust has not been established.
Considerations to build trust on the telephone:
Say hello and state the name of the clinic
If you need the client to hold wait until they confirm that they will hold
Express compassion and empathy as you listen to the client’s concerns
Take the time to listen to the client’s concerns including those that extend beyond the reason for the visit
Triage and book the appointment with consideration to the client’s needs
If in doubt about the urgency while triaging, speak to the health care provider (HCP) and let the client know you are confirming with the HCP
If you are not able to meet the client’s requests for booking then provide alternative options to the client
Building Trust at Check In
Once a client and their family have arrived at the office for their encounter they will check in with the Health Care Administrator (HCA). HCAs display competency with a warm greeting, acknowledging the client, identifying themselves, and providing an efficient check in process. A professional office has individual seating, is clean, and is set up for confidentiality. In our opening scenario, the HCA was efficient, displayed competence by following confidentiality, and then did what they could to make the client and their partner feel comfortable and trust was established. Contrarily, imagine for a moment that Regie arrives with Jagmeet to the office already feeling as if their appointment is an imposition, now they enter a chaotic office, a long line to check in, Regie can hear confidential conversations with other clients, there are not enough seats, and the office garbage pails are overflowing. Do you think that Regie will trust that Jagmeet will receive proper health care?
Considerations to Build Trust at Check In:
Keep the office waiting room clean, tidy, and check for adequate seating
Greet the client warmly, with a smile, and ask for their health card
Confirm demographic information using an appropriate voice level to maintain confidentiality
Let the client know how long the wait will be and ask them to have a seat in the waiting room
Look at the client to demonstrate that you are actively listening to the client and acknowledge that you have had heard what the client has said to you
Identify the Help Required
In order to identify the help that the client and their family are seeking, health care administrators (HCA) can utilize a number of effective therapeutic communication techniques, and avoid ineffective communication and behaviours. You may be wondering if this is in the scope of practice of the HCA. In many health care offices, the HCA is responsible for the initial intake of the client. For example, filling in the subjective and objective components of the client encounter in a SOAP note (CPSO, 2021). In circumstances where intake is not a requirement of the HCA role, observations can be made and reported to the health care provider (HCP).
Power
HCA should be aware of the unequal balance of power between the client, family members, and the HCA. The College of Nurses of Ontario (2006) suggests that unequal power exists because health care providers have access to information and knowledge that the client and their family do not. It is important to keep this in mind when communicating with a client, avoid misuse of this power, remain respectful to the client, and to be aware of the client’s vulnerability.
Effective Questioning and Behaviours
During the intake process, the HCA may require specific details about the client and the reason they are seeking health care. A closed question often works best in this circumstance. For example, How do you spell your last name? Is it your left arm or your right arm that you fell on? By contrast open-ended questions invite the client to expand upon the answer and provide further information. For example, What brings you in today? Clients may answer open-ended questions in a way that implies not all the information has been given. For example, they may answer the question What brings you in today with I have not been feeling myself. In this situation, you may need to use a probing question to encourage the client to share more. For example, you may respond with how would you describe not feeling like yourself? Which the client may respond with I have been exhausted and having trouble sleeping, I go to bed at 8 p.m. but I am up again at midnight. At this point, you have engaged the client in the Interaction Model of Communication discussed previously and are likely to gain a better understanding of the client’s health care needs.
Active Listening
Active listening is a critical behaviour in the helping interview because it communicates that the message has been listened to and understood. Open RN (n.d.) proposes that active listening communicates that we are verifying that we understand what the other person is saying to us. Consider in the Osgood-Schramm Model of Communication the role of the receiver, in receiving the message, and then providing that feedback to the sender. The HCA can demonstrate active listening by looking at the client, nodding when appropriate, and providing verbal cues that the client is being listened to. Active listening can be demonstrated by the HCA by looking at the client, nodding when appropriate, and providing verbal cues that the client is being listened to.
Touch
Figure 5.1 Health Care Administrator comforting client with therapeutic touch.
In health care, touch is used as a form of communication and is expressed as a light touch on a hand, arm, or shoulder. Open RN (n.d.) proposes that the communication of touch is used to express concern, compassion or comfort. Touch is used with an acute awareness of the client’s cues of acceptance, to this type of communication. If the client recoils or tells you not to touch them, then do not touch them.
The table below represents effective therapeutic communication techniques and behaviours that can be used during the helping interview. These techniques will assist to identify the health care need that the client is seeking.
Use of nonverbal and verbal cues to encourage clients/client’s families to continue talking.
Acknowledging that you are listening by nodding your head, saying yes, and offering general leads.
General Leads
Questions used to propel or guide the conversation forward.
What happened next?
Silence
Deliberately silent to give people involved in the conversation time to reflect and process what could be said next.
No speaking
Touch
Sometimes there are no words and a light touch to the top of the hand, arm, shoulder, or back conveys a caring message. Caveat, you must look for cues that the other person will accept being touched. If they recoil do not touch them.
A light touch to the top of a hand, arm, shoulder, or back.
Making Observations
Observing a client’s demeanour or behaviour can help to open up a conversation and for the client to tell you more.
You appear to be in pain
Acknowledging
Acknowledging what a client has said to be their experience builds trust.
I agree having to wait for results can be frustrating and scary
Paraphrasing
Repeating what the client has said for confirmation. This must be used sparingly as not to come across as patronizing.
Client: I twisted my left ankle at soccer and it sent shooting pains to my hip.
HCA: Your left ankle and your left hip are in a lot of pain because you twisted while at soccer.
Client: Yes
Open-ended Questions
A questioning technique that requires expansion or further clarification.
What brings you in today?
Closed Questions
Closed questions can be answered simply and do not require further reflection or clarification.
Is it your left arm or your right arm that you fell on?
Ineffective Therapeutic Communication Techniques and Behaviours
It is important to be aware of ineffective communication and behaviours that block communication, and leave the client and their family without the help that they need. The table below represents ineffective communication techniques and behaviours to be avoided.
Requires the client or client’s family to explain. Invalidates the client or client’s family experience and may cause them to become defensive.
Client: I quit smoking for 6 months I didn’t feel any better. I don’t think quitting smoking will help this time either. HCA: Why don’t you think quitting smoking will be different this time?
Arguing
Arguing with a client implies that they are lying, misinformed or uneducated. This can exacerbate an emotional response or cause the client to shut down.
Client: The insurance company said you can bill them directly. HCA: I can’t bill the insurance company you will have to pay and put in a claim for yourself. Client: I emailed them and I have printed off their response. HCA: It does not matter what you have printed I can not bill them directly
Asking Personal questions
It is inappropriate to ask questions that are not relevant to the situation.
HCA: Marital Status, please. Client: Not married. HCA: Why aren’t you married
Giving Personal opinions
Giving a personal opinion takes away the client’s decision-making.
HCA: Would you like a listing of personal home care supports for your father?Client: No thank you, I will take care of him. HCA: Well if it was my father I would have someone come in to help us.
Changing the Subject
Changing the subject during a communication demonstrates a lack of empathy and will demonstrate that you don’t wish to know what the client or their family is telling you.
Client: Do you know how much longer the wait will be? I just started a new job and can’t be late. HCA: That is a really pretty lipstick colour you are wearing. What colour is it? Client: Um, Pink shell from the local drug store. I guess I will just sit back down.
Generalizations
Generalizations minimize the client’s or their family’s experience(s) and take the focus away from the immediate concern.
Client Family Member: My dad can’t seem to remember his phone number or answer common questions coherently. I am concerned that his new medication is causing confusion. HCA: Oh, well as parents age they do get confused.
False Reassurance
Discourages further expressions of feelings
Client: I am really worried about this upcoming procedure. HCA: Don’t worry Dr. Smalt can do this procedure in his sleep.
Sympathy
Sympathy takes the focus away from the client and attempts to move them out of their emotional state.
Client: I can’t believe that my partner died so suddenly. HCA: I am so sorry that your partner died. I can’t imagine what I would do if my partner died like that. Client: Yes that would be difficult for you.
Resolution and Next Steps
The last part of the helping interview is finding a resolution to the identified health care need(s). While it is not always possible that a health care need can be resolved in one encounter, there are next steps that can be conveyed to the client. Diagnosis, prognosis, and next steps are conveyed to the client by the health care provider (HCP). After the encounter, the client will go to the health care administrator (HCA) to book the next steps such as future health care appointments, tests, receive instructions, and make payments. Thus the HCA is the last person the client and their family see and complete the helping interview. The HCA ensures that the client and their family are aware of any test preparation, appointment bookings, directions, additional costs such as parking, follow-up appointments, and insurance receipts. Utilizing effective communication techniques, avoiding ineffective communication techniques and behaviours, will ensure the client and their family leave with their health care needs met.
Assessing What You Already Know (Text-based Activity)
Question 1
The last time you made an appointment to see your family Doctor, who was responsible for gathering information about your symptoms? Check all that apply.
Nurse.
Doctor.
Health Care Administrator.
Solution: All the options are correct. The health care administrator asks you why you want to see the doctor and in some offices, the health care administrator is responsible for initial intake to learn more about intake and SOAP notes continue reading the chapter. The nurse may be responsible for gathering your symptom information and completing initial assessments. The doctor is responsible for assessing your symptoms during the examination.
Question 2
Reflect upon the last time you attended a job interview. What made the interview a positive experience or a negative experience. Choose all that apply. There are really no right or wrong answers as your experience is valid.
It was a positive experience because the interviewer made me feel welcomed, comfortable, and I knew what to expect. Continue the chapter reading to learn about building trust and what is similar to the helping interview.
It was a negative experience because the interviewer was abrupt, I felt out of place, and didn’t know what to expect. Continue the chapter reading to learn about building trust and what is similar to the helping interview.
What other type of experience did you have.
Solution:There are really no right or wrong answers as your experience is valid. Continue the chapter reading to learn about building trust and what is similar to the helping interview. Return to Activity
Check your Understanding (Text-based Activity)
Question 1
Making observations is an effective therapeutic communication technique because it can help open up a conversation with the client.
True
False.
Solution: The statement is true.
Question 2
Asking Why questions is an effective therapeutic communication technique because it helps the client or client’s family explain more.
True
False
Solution: The statement is false. Asking Why questions may the customer feel questioned.
Question 3
Giving personal opinions is an ineffective therapeutic communication technique because it takes away the client’s decision making.
True.
False.
Solution: The statement is true.
Question 4
Changing the subject is an effective therapeutic communication technique because it helps the client reduce stress and anxiety.
True.
False.
Solution: The statement is false. Changing the subject demonstrates a lack of empathy and will demonstrate that you don’t wish to know what the client or their family is telling you.
Question 5
Sometimes, a light touch to the top of a hand, arm or shoulder conveys a caring message.
True.
False.
Solution: The statement is true.
Question 6
Asking closed questions is always better than an open question in health care settings.
True.
False.
Solution: The statement is false. Both open and closed questions are useful in health care settings.
Question 7.
Which of the following statements is correct:
The helping interview has a particular characteristic: one person seeks help, and the other provides help.
A Health Office Administrator doesn’t need to learn about helping interviews. That is the physician’s role.
The helping interview is the same as a job interview.
Solution: Option 1 is correct. A helping interview is different from a job interview, in which one person seeks help, and the other provides help. Health office administrators should learn about this, because communication is an essential part of the role. Return to Activity
Explore the health communication between various cultures.
Develop a level of understanding of various cultures.
Develop the awareness of health care communications and interactions between health care administrators and diverse client populations.
Enhance self-awareness when communicating with diverse populations.
Introduction
The following chapter will explore cultural communication styles with diverse cultures, including Anglo-Saxon-Western, Black-African, Chinese, Filipino, Indigenous, LGBTQ2S+, and South Asian. These cultures were selected based on Ontario demographics and are alphabetical to avoid any hierarchy of importance. Finally, trauma-informed communication will be discussed. The HCA should be aware that cultures can change over time when persons are exposed to new knowledge, beliefs and norms, so the cultural norms discussed in this chapter may change over time. It is not possible to cover all the various and wonderful cultures that make up our world. We invite you to explore, investigate, and add to the cultures discussed in this chapter.
Assessing What You Already Know
Thanks to global access to travel and the high potential for requiring health care while in other countries. A Health Care Administrator should consider their day-to-day interactions with others from differing cultures or communities. Cultural competencies will decrease misunderstanding in health and studies support the need for cultural competence to increase a person’s successful health outcome.
Many diverse aspects of multicultural communications can include usage, use of words and phrases that may be interpreted differently and non-verbal communication such as facial expressions, gestures, seating arrangements, personal distance, and sense of time may vary. When interacting with patients, their families and other health care professionals, it is important to consider the following guidelines.
As a professional HCA learn some generalizations about other cultures but does not use those beliefs to stereotype the individual one is communicating with, ask questions to confirm and learn. Individuals are multi-faceted human beings. Do not assume that there is one right way (yours!) to communicate. Self-awareness and self-reflection will assist one with multi-cultural skill development. It is important to be aware of one’s gestures, body language or postures that indicate receptivity in one culture might indicate aggressiveness in another.
The HCA should listen actively and empathetically by putting themself in the other person’s shoes. At times, it is best to acknowledge potential historical events that have occurred and remain open to learning more about them. Truthful acknowledgement of oppression and the mistreatment that has taken place on the basis of cultural differences is crucial for successful communications.
HCA’s should be aware of power imbalances such as those between health care workers and clients, between those of client’s families and health care workers, and the various levels of health care disciplines.
Remember that cultural norms may not apply to the behaviour of any particular individual. Persons are influenced by one’s ethnic background, family, education, personality and life experience; much more than cultural norms (Tuazon, 2021). To develop an understanding of cultural communications, consider the following list as it explores cultural communication techniques that include language, gestures and positionality when interacting with clients from differing cultures.
One way to enhance diverse understanding is to provide patients with easy-to-understand instructions, including directions to appointments. It is essential to provide enough time for patients to express and share their concerns and listen carefully to patients when they are speaking. Patients should always be included in decision-making and care plan development. Patients should be encouraged to access their Personal Health records to illicit an awareness and demonstrate the acceptance of being a part of their health care plan.
If required, offer assistance to clients when filling out forms or performing tasks they may not have done before, such as scheduling appointments, making a referral, going to the lab for bloodwork or x-rays. Always communicate with patients through their preferred communication method (phone, mail, secure messaging) (Shepherd et al., 2019).
Anglo-Saxon Western Cultural Communications
An Anglo-Saxon person speaks English. A Westerner is a person who comes from a country in the western part of the world, particularly North America. The Western medicine system includes medical and healthcare professionals such as doctors, nurses, therapists, and pharmacists who manage and treat disease using conventional, evidence-based practices such as drugs, surgery, lifestyle changes or treatment protocols.
The assumptions in Western health care systems include a patient-centred approach where the individual needs have priority over their needs and decision making. The literal meanings of medical words are essential and should be explained; for example, the term palliative. Many health uncertainties in life can be managed with the correct diagnosis, medication treatment, or medical interventions.
Persons from western cultures tend to have an explicit and direct communication style. Therefore, the clients become a part of their health care plans and often will communicate the need to be involved. It is an expectation in western culture to make informed decisions, and thus the client may ask for clarification from any health care professional. Westerners are accustomed to seeking second medical opinions, which should not be conveyed as an insult to the professional as clients are involved with their health care plans and decision-making.
Clients from western cultures generally follow medical advice, particularly if they understand it. Clients will ask many healthcare professionals questions to obtain answers, as they have a right to know and transparency is key to their decision-making. The client learns by detailed inquiry extensive or questioning of the physical examination or laboratory results. Clients coming into a health care facility may appear anxious. As institutional rules restrict their privacy and actions, communicating with the client may appear to be a challenge when you deal with the person in the sick role who believes they are powerless due to institutional limitations such as meal times and visitors.
Typically elderly clients should be addressed with their prefix Mr., Ms., Mrs., Dr., Miss., and surname. However, clients may prefer to be addressed by their first name. It is essential to ask the client how they prefer to be addressed.
Black- African Cultural Communications
Language barriers may limit the HCA’s ability to communicate efficiently when communicating with Black immigrant populations. Between African and Caribbean immigrants, the populations speak over 2,100 languages and dialects (Komen, 2020). As a language translator is preferred practice, it is essential to get a professional who speaks the language and the dialect.
Many Black immigrants come from cultures with power distance, meaning some members have higher status than others. People of perceived lower status do not direct eye contact to people of higher status (Neuliep, 2014). Before looking a client directly in the eye, step back and perceive how the person interacts with you and act accordingly.
Non-Verbal Communication with Black Immigrants
The following recommendations may not apply to all black immigrants. It is essential to know what culture the client accepts or feels connected to, to provide culturally sensitive and culturally competent care as many practices will be individualized (Shepherd et al., 2019). Such as, in Black Muslim cultures, men and women may not wish to shake hands with the opposite sex. Be mindful of the cultural gender roles.
However, in some African cultures, the HCA should avoid pointing with their index finger, as this gesture may be considered offensive. The HCA should use an open hand with their palm facing down when offering direction to the client room or diagnostic centres.
In some African cultures, the left hand is considered unclean; therefore, the HCA should pass paperwork or pamphlets to the client using the right hand.
Some Black immigrant cultures like to be in closer proximity when speaking. Although the HCA should speak quietly for privacy reasons, they should avoid whispering. In some African cultures, whispering can be viewed as gossiping.
Chinese Cultural Communications
Being late for an appointment is considered an insult in Chinese business culture so make sure you are on time. This can be challenging in busy clinics. As well, when scheduling client appointments, be sensitive to Chinese holidays such as the Chinese New Year, which changes yearly, as many other institutions may be closed.
In Chinese culture, there is a strong emphasis on familial hierarchy. For example, following Chinese business protocol, people are expected to enter the meeting room in hierarchical order. This may apply to families coming for a clinic visit. As an initial greeting traditional Chinese person may nod or bow slightly. Handshakes are also common greeting practice; however, wait for your client to initiate the gesture. Handshaking is done with a rather gentle grip because a very firm handshake suggests aggression (Shepherd et al., 2019). People from China will often pause after something has been said to show respect and contemplate a good response.
When speaking, people from China do not use many gestures or demonstrative expressions and will become annoyed with someone who does. Emotion is often repressed, and humility is a virtue. When you need to point, use your whole hand. Avoid using any excessively demonstrative behaviour or gesture. Do not raise your voice too loud or snap your fingers, wink, or whistle when speaking. Maintaining good eye contact is appropriate. People from China are taught to avert their eyes to avoid intimidation. It is unacceptable to blow your nose in a handkerchief or tissue and then put it in your pocket or handbag. This is considered unsanitary. Gentlemen — do not cross your legs with your foot resting on your knee. It is considered disrespectful, and you may inadvertently point the sole of your shoe at someone – an absolute insult!
Indigenous Cultural Communications
All persons are to be treated as individuals within their cultures. Some people may self-select to follow some practices and add others, particularly with language and communication styles. Indigenous populations are unique as well. Those living in remote communities may have low proficiency in the English language, with English being the second or third language spoken within their community. The following information will provide a provide overview for communicating with the population.
Health care administrators need to have or develop an understanding of the historical context of Aboriginal people as there may be cross-cultural misunderstandings or a lack of recognition of Aboriginal beliefs and “ways of doing things”. Remember, there are complex centralized health systems or restrictions and potential logistical challenges in accessing health services.
Cultural Perceptions of Health and Wellness
First Nations Health Authority’s health model represents a fluid and holistic concept of health and wellness. The model centres on the individual human being. There is a focus and importance of a healthy and balanced life’s mental, emotional, spiritual, and physical facets. The Indigenous values supporting wellness include respect, wisdom, responsibility and relationships (First Nations Health Authority, 2021). It is essential that the HCA has a cultural awareness of the Indigenous health care approaches.
Traditionally, indigenous peoples learn things through prayer, visions, dreams or divination—extensive or brief divination, prayers or supplication, by entering into a trance state (Ball & Bernhardt, 2008). The practices emphasize communication with spirit beings and direct requests for healing. This communication occurs through prayer, song and ceremony. Additionally, one looks for areas of disharmony and imbalance within the external community, within the community of one’s mind, and in the relationship with our bodies, the earth, the plant people, the animal people and all of creation. Healing is through achieving balance and harmony in our many relationships. The approach to each person is different because each person is unique and has their own set of imbalances. By contrast, biomedicine generally looks for the one treatment that will benefit the highest number of people with a particular disease.
Develop an Awareness of Aboriginal English Language Patterns
In Canada, Aboriginal English speakers may omit a subject pronoun. Pronouns include I, you, she, he, it, we, they. The use of double negatives is every day in many dialects of Aboriginal English. How comments are stated can hold meaning. Such as reading intonation, the ups and downs of the voice pause between speakers, the use of gestures and facial expressions contribute to the meaning of the words used.
Based on historical experiences, understand that Indigenous peoples may not immediately trust the health care administrator (HCA) or the health care system. Native American patients are reluctant to tell health care providers about a hallucination or dream experience due to the risk of labelling the client negatively or the concern that the dream could indicate psychosis (Fadden, 2016). In order for this reluctance to be overcome trust must be established with the client. One way that health care workers can build trust with clients from indigenous communities is by following through on the agreements or decisions.
Health Care Administrator Communication Approaches
First and foremost, the use of Indigenous translators, patient navigators, or Indigenous health workers should always be considered to enhance Indigenous peoples’ understanding of health or assist in seeking healthcare services (Ball et al., 2006). The HCA must learn about the Indigenous communities in the area of residence and work. Health care is a sensitive matter to the indigenous and should not be asked about directly. Also, always seek permission and explain to the client why one needs to touch them, such as taking their blood pressure. Establishing rapport and mutual respect first may allow the client to feel more comfortable in the health care setting.
When calling a client, use formal addresses with older people and Elders and ask them how they wish to be acknowledged. During the interaction, recognize that extended silence during conversations is considered the ‘norm’ and is valued in some Indigenous cultures. The meaning of the silence may vary. It can be used as a show of respect, contemplation, disagreement, a time of reflection, or considering what has been said. Listen and wait your turn to speak without speaking over the client. Verbal and physical interactions should be mirrored to the pace of the individual. Consider the choice of vocabulary, delivery rate, clarity and logical ordering of ideas during a verbal interaction; building trust is the goal of assisting the client. Consider the following in your approaches. If a client appears to be struggling with reading or writing, sensitively offer assistance. Do not ask clients whether or not they can read or write, as this may can shame and embarrassment. Do not speak loudly or in a patronizing manner; offer professional assistance.
The HCA should not assume that an accent indicates a lack of education or sophistication. However, if an interpreter is available, this may assist with cultural sensitivities and learning for the health care professional. During conversations, be careful with the use of humour, as it can be misunderstood or misinterpreted.
Speakers of English may use eye contact to convey or assess sincerity and attentiveness, and if a client does not look the professional in the eye, the assumption may be that they are being untruthful, deceptive or uncooperative. Too much eye contact is awkward, and in the worst case, rude and possibly confrontational. As well, it may not be customary in some communities to maintain eye contact with authority figures.
The HCA should never hesitate to seek the translator’s expertise or the indigenous support available within your institution.
LGBTQ2S+ Cultural Communications
In LGBTQ2S+ populations, there are some specific communication skills, awareness and language to be utilized by the Health Care Administrator. Interactions with the LGBTQ2S+ persons are no different than the procedures we follow with any patient, other than language and a developed understanding of their cultures. As with many cultures, language, beliefs and approaches are fluid and can change over time and, most importantly, differ between individuals (Rowe, 2020). The equality issues and acceptance of transgender and nonbinary people can be demonstrated by the correct use of terms and language.
The proper use of gender identity terms, including pronouns, can signal courtesy and acceptance. “Pronouns are basically how we identify ourselves apart from our name. It’s how someone refers to you in conversation,” says Mary Emily O’Hara, a communications officer at the American Gay and Lesbian Alliance Against Defamation (GLAAD) “and when you’re speaking to people, it’s a really simple way to affirm their identity” (Walmsley, 2021). Everyone uses pronouns when referring to themselves. The primary way of understanding and knowing the correct pronoun is to ask the client. When introducing yourself say, “My name is George, I am the Health Administrator, I use he/him pronouns, What about you?” Utilizing the correct pronoun reaffirms to the client that they are accepted and worthy. Using correct pronouns to demonstrate respect is also essential because of the extensive history of discrimination and barriers that LGBTQ2S+ persons have been subjected to over time, particularly when seeking health care (Table, et al., 2021).
The HCA should use the terms that the client uses to describe themselves and their partners. For example, if the client calls themself “gay,” do not use the term “homosexual.” If a woman refers to her “wife,” then say “your wife” when referring to her. The HCA’s primary focus has to be on making all patients comfortable. When taking a medical history, do not use words that assume people have an opposite-sex partner or spouse, ask “Are you in a relationship?”. Gender-neutral and non-biased language assists in open and honest dialogue.
The use of accepted language and terms can change. Some of the terms currently used are different from those used in the past to describe similar ideas, identities, and experiences. Moreover, some terms are acceptable to use by specific populations yet not accepted by some people to use as labels (Nett, 2021). The HCA is to recognize and respect all people as individuals.
Vanessa Goes to the Doctor
The video is an excellent demonstration of correct and incorrect communications with a person from the trans community. Remember if you make a mistake when dealing with a client, politely apologize and learn from your error. The HCA’s role is one of continuous learning and improvement of client service.
The guidelines for communication from chapter two apply to all individuals. As language is an essential element for Health Care Administrators, the use of a glossary is helpful to demonstrate further respectful, informed, and accurate interactions. The following further reading will list the current accepted terms and definitions as used by GLAAD, Center for Transgender Equality, the Trans Journalists Association, NLGJA: The Association of LGBTQ Journalists, Human Rights Campaign, InterAct and the American Psychological Association, and Egale Canada Human Rights Trust.
Cultural Interactions with Persons from the Philippines
The Philippines represents a variety of cultures. It is located in the heart of South-East Asia, though the culture is heavily influenced by non-Asians from Spain, Mexico, and the United States. The Catholic Church is very influential in the Philippines culture.
Communication Style
The Philippine style of communication is indirect and takes into consideration the perception of the recipient. In order to save face and remain courteous, Filipinos rarely give a direct answer of ‘no’ and will avoid disagreement, rejection and confrontational behaviour, especially when a superior is involved. The word ‘yes’ is often used to disguise more negative responses and avoid causing embarrassment or offence. ‘Yes’ may mean ‘maybe’ or ‘I’ll think about it’ or even an outright ‘no’. A healthcare professional will have to be more alert to the subtle cues hidden in conversation, such as nonverbal communication, to help decipher meaning. This ambiguity in response means that it can take longer to get a firm negative answer.
Language
Because of the years of U.S. military presence in the Philippines, most westernized gestures and communication styles are recognized and understood. As well, English is the language of most interactions in the Philippines.
Gender
Women are accepted in business circles. However, they should avoid acting domineeringly with male colleagues. Women managers are expected to be highly competent and assert their authority in a professional, restrained manner. Although there are social inequalities in the Philippines, Filipinos believe that everyone must be treated with respect, and they behave with modesty and graciousness, especially in their dealings with the poor or less fortunate.
Greetings
In the Philippines, showing respect for one’s elders is a tradition that has been preserved for generations. The ‘honouring-gesture’ called pagmamano involves a younger person asking for an elder’s hand and gently touching their own forehead with it while bowing. The practice is common whenever someone visits relatives or meets their godparents (Engson, 2021).
It is common for most people in the Philippines to shake hands as a way of greeting. This can occur between men and women, but there are some boundaries. Even though most parts of the Philippines find it acceptable to shake hands between men and women, the touching of women is a very sensitive issue. In some areas, men and women do not shake hands because it involves touching. In every part of the Philippines, any touching of women in public is deemed inappropriate. Filipinos are widely regarded as needing a little more personal space than people from western culture.
Approach
Most Filipino people expect pretty constant eye contact, and it is a sign of self-confidence. Also, when introducing yourself, it is proper to use academic and professional titles. In addition to formal titles, it is customary to introduce yourself to the eldest or most important person first (Shepherd et al., 2019).
‘Small talk’ is an integral part of establishing relationships with Filipinos. Be aware that embarrassing someone, or reprimanding them in front of others, can cause them to “lose face”, trust or loss reputation, and this has very negative consequences in this culture. Maintaining cordial relationships is essential in the Philippines. Keep your comments as positive as possible (Engson, 2021).
Nonverbal Cultural Communication
Hold your hand out, palm downward, and make a scratching motion with the fingers to beckon someone. Beckoning someone with the palm up and wagging one finger can be interpreted as an insult. Pointing at someone or something can be perceived as an insulting gesture. Filipinos typically point at objects using an open hand. They may use a glance with a slight nod or purse their lips to signify which way to provide directions. Consider some of the following when communicating with people from the Filipino culture. When counting indicating ‘two’ with the fingers is done by holding up the ring and little finger, not the forefinger and middle finger. The thumb is not used to count numbers in the Philippines (Engson, 2021).
As far as body language, do not put your hands on your hips when conversing, and this gesture can be misinterpreted as a challenge to another person. However, nodding and raising eyebrows with a smile is one way of how Filipinos greet each other casually and quickly, acknowledging that you saw that person. A friendly tap sometimes follows this gesture on the shoulder if they are within reach.
People from the Philippines may be pointing their lips at someone or something. Instead of lifting their finger or arm, Filipinos commonly use their lips to point to an object or another person, and this gesture is called nguso (Tuazon, 2021).
Positioning ones’ arms extended while lowering the head is commonly done when passing in front of two people talking to each other or crossing a room when someone is watching a TV. Followed by an “excuse me,” this gesture is seen as a sign of courtesy and respect.
If Filipinos do not understand a question, they open their mouths. Raised eyebrows signify recognition and agreement. Laughter may convey pleasure or embarrassment; it is commonly used to relieve tension. Raising one’s voice is unacceptable in the Filipino culture. It is crucial for the HCA professional to maintain a low, controlled tone of voice at all times (Tuazon, 2021).
When you are about to pass in between two people talking, you do not need to say ‘excuse me’ or ‘pardon me.’ Doing so will only interrupt their conversation. Lower your head and extend your arm downwards before going in between them. Without saying anything, this gesture instantly indicates politeness and respect for the two people conversing.
Verbal Communication
Filipino people are known for being very comforting. They do not regularly discuss politics or religion. It is acceptable to make light of social, political and economic issues, but it is not acceptable for foreigners to discuss politics with the Filipino people. Raising one’s voice is unacceptable in the Filipino culture. It is crucial to maintain a low, controlled tone of voice at all times (Tuazon, 2021)
South Asian, India Communications Interactions
India is home to over a billion people, with tremendous cultural diversity between languages, geographic regions, religious traditions and social structures. The following health communications are not intended to represent every Indian person. However, there are common themes and principles. Most Indians tend to have a strong sense of pride in their culture. Persons from India are from South Asia; therefore, the terms Indians or South Asians will be used interchangeably in this text.
When interacting with clients from India, it is essential to understand and have an awareness of India’s historical and current cultural and social influences. Although this is changing, the caste system remains one of the most critical influences in Indian society. The caste system encompasses a complex ordering of social groups based on ritual purity, creating a social and religious hierarchy that may continue to thrive among Indians abroad. A person’s caste identity is inherent in their surnames (most times, but not always). Technically there is human equality under the law; however, inequality still exists between the castes and is an accepted reality of Indian life (South Asian Caste System, 2021).
How does the caste system impact health communications or interactions? Persons of a higher caste may expect to be serviced before someone of a lower caste. A person in a higher caste may appear more demanding; however, it is essential to communicate with all clients with trust, respect and equity. As well clients should be reminded that they are triaged based on health needs and urgency.
Many persons’ from India’s health care beliefs are rooted in spirituality and preventative practices, particularly in yoga practice. Some clients may perceive disease and illness as a punishment from god due to actions in one’s past life, and those good or bad personal circumstances are deserved.
Gender will also influence who a health care professional addresses first (Shepherd et al., 2019). Typically, a male family member will be in charge of the health care of other family members; therefore, the male person may be participating in the health care decisions, and their presence should be addressed alongside the client.
Gender may also play a role in regards to the health care professional. Due to the modest nature of the female body, women clients may prefer or expect a female health care practitioner. When scheduling appointments, it is recommended to advise the client of the gender of the health care professional providing their assessment or examinations.
When registering an infant, the administrative professions should be aware that the naming of newborns often occurs after hospital discharge. The baby is taken to their religious institution, where the leader will provide a letter to guide the family in naming the newborn. Hence, babies may be labelled as ‘baby boy’ or ‘baby girl’ until this ceremony.
Verbal Communication with South Asian Populations
The communication style of Indian South Asians tends to be polite and indirect. Whereas direct communication is used with relationships with a high level of trust or crucial situations, such as during health care crises. Direct refusals, such as stating ‘no’, may be considered to be too harsh. Therefore, Indians may give evasive refusals and provide indirect disagreement. Indians tend to use the phrases ‘maybe’ or ‘I will do my best as a way to express ‘no’. Sometimes clients will remain silent versus providing a verbalized ‘no’. Pay attention to what is not being said, as the absence of agreement may be an expression of disagreement (Kaur, 2021).
The term ‘yes’ has various connotations that differ from the word’s usage in Western cultures. South Asians may say ‘yes’ to indicate that they are listening to the health care professional in contrast to their disagreement or refusal through their body language (discussed below). Cultural politeness and modesty can sometimes mean that some Indians automatically answer ‘yes’ to direct questions that require a yes or no answer. One way to address any ambiguity is to check for clarification several times using open-ended questions. For example, rather than asking, “Is the appointment time suitable?” it is better to ask, “Which day and time works for you?”.
Non-Verbal Communications with South Asian Populations
Consider the following norms in South Asian cultures. To beckon a client to come forward, hold one’s hand out, palm downward, and make a scooping motion with the fingers. Beckoning someone with the palm up or wagging one finger is perceived as an insult. Pointing with your finger is considered accusatory or rude. Indians may prefer to point with their chin.
South Asians prefer minimal eye contact or may avert their eyes, particularly from the opposite gender. Women may avoid eye contact altogether. Direct eye contact is generally appropriate as long as one diverts their gaze every so often.
South Asians may tilt their head to the side or shake them to both sides to indicate agreement and understanding. This head movement is comparable to the Western gesture indicating “I do not know” with a tilting one’s head to the side or a shrug of the shoulders. Out of politeness, Indians will often nod to acknowledge what is said out; however, this does not always mean they understand or agree. Touching anyone on the top of the head is deemed to be insensitive and offensive, as the head is considered the holiest part of one’s body (Kaur, 2021).
Considerations
It is an essential part of the health care administrator’s (HCA) role to interact efficiently with persons from all cultures. To do this HCA can explore local cultures to develop a broader understanding of how culture influences health and health care. HCA should work towards understanding and demonstrating cultural competency to enhance the working relationships with clients and the interdisciplinary health care team. Cultural competency requires regular exploration, practice, reflection, and is a lifelong commitment to self-development.
Explored the health communication between various cultures.
Developed a level of understanding of various cultures.
Developed the awareness of health care communications and interactions between health care administrators and diverse client populations.
Enhanced self-awareness when communicating with diverse populations.
Key Terms
Ambiguity: Something that does not have a clear meaning. (Merriam-Webster, n.d)
Avert: Avoid. (Merriam-Webster, n.d)
Conventional: Something that is usual. (Merriam-Webster, n.d)
Dialect: A language distinguished by vocabulary, grammar, and pronunciation using other regional types and creating a single language. (Merriam-Webster, n.d)
Domineeringly: Overbearing control over other individual. (Merriam-Webster, n.d)
Elder: An identified and respected member of an Aboriginal community. Elders have ley information about their community and are often sought for guidance and support. Often they may be called ‘aunty’ or ‘uncle’ as a sign of respect, even if they are not related.
Equality: The quality of having the same rights. (Merriam-Webster, n.d)
Gestures: A movement of the body that emphasizes an idea. (Merriam-Webster, n.d)
Gossip: Rumour about others. (Merriam-Webster, n.d)
Graciousness: Kindness and politeness. (Merriam-Webster, n.d)
Hierarchy: A system in which people are placed by levels with different importance. (Merriam-Webster, n.d)
Holiest: Something that has a divine quality. (Merriam-Webster, n.d)
Mirrored: Adjective of something that gives an accurate representation. (Merriam-Webster, n.d)
Positionality: The position that your race, gender, sexuality, and ability position your identity in society (Merriam Webster, n.d).
Powerless: Lacking the capacity to act. (Merriam-Webster, n.d)
Proficiency: Advancement in any knowledge. (Merriam-Webster, n.d)
Pride: A feeling that you deserve to be respected (Merriam-Webster, n.d)
Rapport: A relationship that is harmonious. (Merriam-Webster, n.d)
Reluctance: State of feeling aversion. (Merriam-Webster, n.d)
Restrained: Not excessive. (Merriam-Webster, n.d)
Subtle: Something that is hard to notice. (Merriam-Webster, n.d)
Supplication: Humility
Transparency: Obvious or easy to understand. (Merriam-Webster, n.d)
Trauma: A very difficult experience that causes mental or emotional problems, usually for a long time. (Merriam-Webster, n.d)
Whispering: Soft speech to avoid being overheard. (Merriam-Webster, n.d)
Wisdom: The knowledge that is gained by experiences in life. (Merriam-Webster, n.d)
Worthy: Having value. (Merriam-Webster, n.d)
References
Ball, J. and Bernhardt, B. M. (2008). First Nations English dialects in Canada: Implications for speech-language pathology. Clinical Linguistics & Phonetics, 22(8): 570–588. https://doi.org/10.1080/02699200802221620
Ball, J., Bernhardt, B., and Deby, J. (2006). First Nations English dialects: Exploratory project proceedings. Unpublished monograph, First Nations English Dialect Project.
Engson, J., (2021). Communicating with persons from Philippines. Personal Communication, October 21, 2021.
Neuliep, J.W. (2014). Intercultural communication: A contextual approach (6th ed.). Los Angeles: SAGE Publications.
Rowe, K. (2020). Improving provider confidence and partnership with LGBT patients through inclusivity and education. Doctor of Nursing Practice Projects, 5. https://scholarworks.seattleu.edu/dnp-projects/5
Table, B., Tronstad, L. D., & Kearns, K. (2021). ‘Anything is helpful’: Examining tensions and barriers towards a more LGBT-inclusive healthcare organization in the United States. Journal of Applied CommunicationResearch: 1-20. https://dx.doi.org/10.1080/00909882.2021.1991582
Tuazon, N. (2021). People of Filipino Heritage. In L.D. Purnell & E.A. Fenkl (Eds.), Textbook for Transcultural Health Care: A Population Approach (pp. 365-394). Springer Nature.
Communicate clearly as part of a team while providing exemplary customer service to clients with differing limitations or needs.
Explore strategies to support communication channels with clients of differing abilities.
Develop an understanding of addressing persons with communication limitations such as verbal, visual, or hearing impairment.
Demonstrate empathy and understanding of differing needs.
Introduction
This chapter will provide how to communicate with clients who have differing limitations or needs effectively. As you can see from Devante’s story, many people can develop changes in their abilities through trauma, disease, age or can be born with the differing ability. While this chapter will explore general communication principles with persons with diverse needs, it will cover verbal, vision, and hearing impairments; this is not to suggest these are the only limitations requiring clear communication exchanges or interactions.
Governing Principles for Communicating with Clients with Limitations
An impairment may be new or temporary, such as an injury, surgery or drug impairment. When the impairment is new, try different methods to address the clients’ needs. For example, if the person requires assistance in communication, treat them as you would any other person requiring assistance. The first principle is to ask the client how to best communicate with them. Then listen to their response. The client is the expert on their needs and what works for them. Do not insist that your way is the correct way; they have lived with their limitations daily (Harrington, 2020).
If a person asks for assistance, clarify how to help and what to do. For example, do they want you to take their arm? Ensure that you speak clearly and wait for responses and cues as to how they wish to proceed. Do not touch anything without asking first. For example, service animals or wheelchairs. A person’s assistive device (e.g. wheelchair, cane, walker) is considered a part of their personal space. Acknowledge the presence of an interpreter, attendant, or companion, but remember to address the person with a disability directly.
Communications with Clients with Verbal Impairments
There are a variety of reasons that a client may be non-verbal so one should never assume the reason. Whether their verbal impairment is permanent or temporary, exploring alternate modes to communicate effectively with the client is essential. Once again, ask the client how to proceed. For example, they may be verbally impaired, but their hearing may be intact and they can provide you with an answer it just might be in a different format than you are expecting.
If the client is presenting to the health care setting alone, do not assume they speak another language or cannot hear. Use hand motions or actions to attempt to decipher the clients’ needs. Nodding and pointing may assist with the initial assessment. The use of signage in different languages may assist with determining if the client is not verbalizing due to a language barrier. However, if a support person accompanies the client, speak and face the client and if the support person intervenes, acknowledge their presence; however, continue to speak and face the client.
The verbal impairment may be new or temporary, such as a facial injury, dental surgery, drug impairment or trauma. When the impairment is new, try different methods to address the clients’ needs (Harrington, 2020). These communication modes may include writing if the client understands and can read English. Consider pointing to, or having the client point to pictures or maps to engage in the Interaction Model of Communication. If the client has had the verbal impairment longer term, they may have a preferred way of managing communication; please ask them how to best communicate with you.
Communications with Clients with Visual Impairments
Visual impairments reduce one’s ability to see clearly. Very few people are completely blind. The majority have some vision. Some have tunnel vision and can only see straight ahead. Others have no central vision but can see around the edges. People with cataracts often have an unclear vision and see things through a ‘foggy window’.
How to Recognizing a Visual Impairment
A person with a visual impairment may wear dark glasses, use a white cane, have a guide dog, be accompanied by someone who will act as a guide. They may exhibit squinting, read at close range, or they move to get close to people. They may also be asking someone to read a sign or document out loud.
How to Enhance Communication with Clients with Visual Impairments
You may ask if the person would like assistance and ask how you can help them and listen for their instructions. As the person has problems with visualization, address the person by name and identify yourself and your role. Speak directly to the person in a normal tone of voice. When the HCA provides verbal directions, be precise and clear.
It is important to inform the person if and when you are leaving the area, as they can not see if you have left the room. The HCA could explain to the client how they could be contacted, i.e. call bell, the position of the phone and extension. The HCA should verbally tell the person when you are giving them materials or returning their health or hospital card or any other documents across a counter or table.
When in a health care setting, orient the patient to their surroundings, such as the furniture, closets, call bell, washroom, curtains, the shape of the room, roommate. It is an excellent time to assess the area to identify any potential hazards (furniture, equipment) in the person’s travel path (Harrington, 2020).
Communication with Clients with Hearing Impairments
There are several different types of hearing loss, including hard-of-hearing, deafened, and oral deaf (unable to speak or hear). The awareness and knowledge of the hearing loss type are essential in communication, particularly ensuring messages are received, acknowledged, and understood.
How to Enhance Communications with Clients with Hearing Impairments
People who are hearing impaired may require assistive devices or utilize an American Sign Language (ASL) interpreter when communicating. Most people who are hard-of-hearing can understand some speech with or without hearing aids. The client may choose to write their messages. They often also read lips to assist with communication (Naseribooriabadi, 2017).
Although clients may have a preferred manner to communicate the HCA can try some of the following suggestions for clear communication. Attract the person’s attention before speaking. The best way is a gentle touch on the shoulder or gently waving your hand. And look at and speak directly to the person. Make sure you are in a well-lit area where your patient can see your face. Avoid standing in front of a window as this will create a shadow on the face.
The HCA should be aware to keep hands and other objects away from their face so the person can see you and your lips. If wearing a mask and if possible for you to remove it, please do so before giving instructions. Alternatively, utilize masks with a clear, transparent window.
When able, use illustrations, drawings or critical words/phrases to explain information. Often, lip reading is easier when you know the subject.
The HCA should always use professional, qualified sign language interpreters; again, American Sign Language is the most common.
Technological devices such as cochlear implants or external hearing aids assist the client with sound. If the person uses a hearing aid, try to speak in an area with few competing sounds. Keep the person’s hearing aids handy when removing them. If you remove a person’s hearing aids, make sure they are placed in a secure location. A personal hearing aid or cochlear implant battery should be the last thing removed or turned off before surgery (or other procedure) and the first thing made available in recovery.
When trying to call into a client’s room, do not use the intercom. Make a personal visit to the client’s room. Alternatively, if communicating via video meeting, use captioning on video screens for health teaching tools (Kumar, 2017).
Communicated clearly as part of a team while providing exemplary customer service to clients with differing limitations or needs.
Explored strategies to support communication channels with clients of differing abilities.
Developed an understanding of addressing persons with communication limitations such as verbal, visual, or hearing impairment.
Demonstrated empathy and understanding of differing needs
Key Terms
Barrier: Something that could be mental or physical that prevents you from progressing.
Cochlear implants: Electronic prostheses are used to aid in hearing. Has an external microphone and one or more electrodes placed into the cochlea. (Merriam-Webster, n.d.)
Decipher: Interpret or decode a message sent to the receiver. (Merriam-Webste, n.d.)
Device: Equipment that serves a specific function. (Merriam-Webster, n.d.)
Expert: Someone who has obtained mastery or experience through education or life experience.
Gentle touch: Used to console a person, placing one hand softly onto another’s shoulder.
Hazards: Are potential risks of danger. (Merriam-Webster, n.d.)
Impairment: Regression or loss of mobility. (Merriam-Webster, n.d.)
Interaction Model of Communication: Process in which participants alternate roles of sender and receiver and incorporate feedback.
Limitations: Due to varying impeding factors one person may not be able to do the same things as someone else.
Methods: Process or steps taken to achieve an objective. (Merriam-Webster, n.d.)
Squinting: Straining one’s eyes in order to try and see something clearly.
Temporary: For short periods of time. (Merriam-Webster, n.d.)
References
Canadian Radio-television and Telecommunications Commission. (2021, September 15). Video relay service(VRS). Government of Canada. https://crtc.gc.ca/eng/phone/acces/rela.htm
Harrington, C. N., Koon, L. M., & Rogers, W. A. (2020). Design of health information and communication technologies for older adults. In A. Sethumadhavan & F. Sasangohar (Eds.), Design for Health: Applications for Human Factors (pp. 341-363). Academic Press. https://doi.org/10.1016/C2018-0-00043-2
Kumar, N. (2017, May). Sign language recognition for hearing impaired people based on hands symbols classification. In 2017 International Conference on Computing, Communication and Automation (ICCCA) (pp. 244-249). IEEE. https://doi.org/10.1109/CCAA.2017.8229808
Naseribooriabadi, T., Sadoughi, F., & Sheikhtaheri, A. (2017). Barriers and facilitators of health literacy among D/deaf individuals: A review article. Iranian Journal of Public Health, 46(11): 1465-1474. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5696685/
When a person requires assistance in communication, the first principle is:
Ask the client how to best communicate with them.
Assume all hearing impaired persons use American Sign Language.
All persons requiring assistance will give you a memo for communications.
Solution. The correct response is option one. When a person requires assistance in communication the first principle is to ask the client how to best communicate with them. The client knows what techniques assist with their ability to understand others. The health care professional will adapt their communication to mee the needs of the client. Return to Activity
Describe the key elements of utilizing Language Interpreter Services.
Explore the diverse range of communication modalities language interpreters provide.
Communicate clearly as part of a team while providing exemplary customer service to persons who speak another language.
Develop an awareness of when, why and how to utilize language interpreters.
Introduction
In any health care setting, the clients will reflect the community where you work. The world is becoming more diverse due to the ability to travel, explore and settle. Thus clients may speak other languages. Many countries have accessibility policies, laws or standards for providing excellent customer service. As an employee, it is essential to abide and be in compliance with the company’s practice (Schenker et al., 2011).
This chapter will explain the why who, what, where and how to use a language interpreter service.
Assessing What You Already Know
A professional language interpreter is a gold standard when communicating with a person who speaks another language than the provider. The use of the interpreter has resulted in improved health outcomes.
As per chapter seven, there are many different mannerisms, expectations and health beliefs given the diversity of the clients. English is often not the clients’ first language. When clients are stressed, as with a health crisis, they may revert to their first language. Not only is the language more accessible for them to have two-way communications, but it may also provide comfort to speak with someone who speaks their language (Brandl et al., 2020).
Who Should Utilize an Interpreter Service?
During an initial interaction, it is important to determine the client’s level of verbal interaction. The use of signage in different languages may assist with determining if the client is not verbalizing due to a language barrier or an impairment. At this time, nodding and pointing may assist with communication during the initial assessment.
When it is determined that the client speaks another language, contact a professional interpreter. Confidentiality is a principal foundation of any health care interaction. Thus, friends or family members should not interpret the private and personal health information between a provider and client. Customer Service best practices assert utilizing a professional interpreter service to obtain and share accurate health information. If you are allowed to use a Professional Interpreter and choose not to, you might be held liable for resulting damages in a court of law.
What is The Interpreter’s Professional Role?
For this text, the two languages would include English and another language. An interpreter is tested for understanding and dictation in both languages by their agency. They must abide by a strict code of Ethics and adhere to confidentiality policies and privacy laws. Their role is to remain impartial and unbiased and stay true to the actual message, as close as the languages will allow. Most Language interpreter Services have their employees pass a criminal reference check to ensure character and reliability. Many organizations hire language interpreter services for all employees to utilize. It is essential to know how to access the service.
How to Use an Interpreter Service While on the Telephone
Many initial health care interactions begin on the telephone. When a client calls the office, and they do not speak your language, for this text, the language is English, the client or someone else may tell you the language and dialect they speak. No confidential health care information has been exchanged, therefore speaking with a friend or family member to arrange an interpreter adheres to privacy laws. If the client requests to schedule an appointment, then there is time to schedule an interpreter. However, if the client requests to discuss their situation over the telephone, the following actions can be followed. First, explain to the client that you are getting an interpreter and ask them to hold (Kester et al., 2021).
As the Health Care administrator, you will already be aware of the Language Interpreter Services offered by your institution.
The first step to accessing services is to Contact the service and request a professional who is fluent in the clients’ language. This may take a few minutes. Record the Interpreters name and ID number for the client’s chart. Explain to the interpreter that the client is on the telephone and requesting service and then add the interpreter to the client call, introduce the interpreter and their role. The HCA will need to allow time for the client to hear, process and respond to the interpreter. The interpreter may seek clarification of some medical terms and remember you will take turns speaking. Finally, at the end of the call, clarify the conversation and thank the interpreter.
Remember, English may not be the client’s first language. However, they may understand English yet may not feel comfortable speaking English. Again, further rationale to utilize the interpreters’ skills.
How to Use an Interpreter Service In-person
If the client has scheduled an appointment for health care services, it will allow the administrator more time to book the interpreter. There may not be time to prepare in settings such as the emergency department or a drop-in clinic. If there is insufficient time to book the interpreter, the interpreter can provide their services over a speakerphone in a private area, where others cannot hear the exchange (Kester et al., 2021).
In-person use of the interpreter service
Contact the service and request a professional who is fluent in the clients’ language. This may take a few minutes. Record the Interpreters name and ID number for the client’s chart.
Explain to the client that a professional language interpreter will be at the appointment in person or be on a phone call to interpret.
Provide the interpreter with the date and time of the client’s appointment
At the appointment, introduce the interpreter and their role.
Whether the interaction is with the administrator or another health care professional, allow/schedule time for the client to hear, process and respond to the interpreter.
The interpreter may seek clarification of some medical terms.
You will take turns speaking.
At the end of the appointment, clarify the conversation and thank the interpreter.
Remember, English may not be the client’s first language. However, they may understand English yet may not feel comfortable speaking English. Again, further rationale to utilize the interpreters’ skills.
Table 8.1 Use of Language Interpreter Do’s and Do Nots
Do
Do Not
Incorporate the first person i.e. How are you? Versus “ask them how they are?”
Assume the interpreter understands all medical terminology
Limit facial expressions
Use gestures
Remain facing the client
Do not look at the interpreter
Pace your speech appropriately
Refrain from using figures of speech and cultural references
Schedule extra time for the interaction
Eliminate vague expressions and words with double meanings
Ask one question at a time
Do not fidget or get distracted: focus on the client (see chapter two for body language)
Enunciate words and speak slowly and audibly
Encourage requests for clarification
Respect the role of the interpreter
Remain present for all communication
Considerations
When utilizing a professional language interpreter, the HCA should create a level of comfort for the client. This can be done by using a professional language interpreter to ensure confidential and accurate translation to the client. Professional Interpreters are bound by ethics and confidentiality laws. HCA should know the process to schedule an interpreter for a client visit. HCA should always direct the communication to the client and not the interpretor.
Described the key elements of utilizing Language Interpreter Services.
Explored the diverse range of communication modalities language interpreters provide.
Communicated clearly as part of a team while providing exemplary customer service to persons who speak another language.
Developed an awareness of when, why and how to utilize language interpreters.
Key Terms
Accessibility: The quality of being easy to obtain or use, easily understood, or appreciated.
Adheres: To maintain loyalty (Merriam Webster, n.d).
Audibly: Can be heard.
Character: Features that describe an individual.
Clarification: To understand an idea.
Confidentiality: The state of keeping or being kept secret or private.
Dialect: A regional variety of language distinguished by vocabulary, grammar, and pronunciation from other regional types and constituting a single language (Merriam Webster, n.d).
Dictation: To understand words that are being used.
Enunciate: To pronounce words clearly so they are understandable.
Ethics: A set of rules.
Fluent: The act of mastering an idea and being comfortable with it.
Impairment: Diminishment or loss of a function (Merriam Webster, n.d).
Impartial: The act of not being biased and treating everyone and everything equally.
Insufficient: Not being enough.
Interpreter: A person who interprets, especially one who translates speech orally (Merriam-Webster, n.d).
Mannerisms: A specific style that an individual should act and speak.
Privacy: The state of being free from public attention.
Rationale: Explanation of controlling principles, such as practice, belief, opinion, or phenomena (Merriam Webster, n.d).
Reliability: The act of dependency you have on an individual.
Unbiased: Not being fair.
Utilize: To use/ take advantage of.
Verbal interaction: The words individuals use to get a message across.
References
Brandl, E. J., Schreiter, S., & Schouler-Ocak, M. (2020). Are trained medical interpreters worth the cost? A review of the current literature on cost and cost-effectiveness. Journal of Immigrant and Minority Health, 22(1), 175-181. https://doi.org/10.1007/s10903-019-00915-4
Kester, E., Palafox,P., Langdon, P., & Cheng, L., (2021). Cultural and Language Considerations for Working with Interpreters. Collaborating with interpreters and translators. Eau Claire, WI: Thinking Publications.
Schenker, Y., Pérez-Stable, E. J., Nickleach, D., & Karliner, L. S. (2011). Patterns of interpreter use for hospitalized patients with limited English proficiency.Journal of General Internal Medicine, 26(7), 712-717. https://doi.org/10.1007/s11606-010-1619-z
Assessing What You Already Know (Text-based Activity)
Question 1
Have you ever tried to communicate with someone who speaks a different language than you do? To explain yourself, did you: (select all that apply)
Use symbols
Speak louder
Get frustrated
Draw a picture
Use hand signs
Solution. While initially, when communicating with a person who speaks another language you may feel frustrated and speak louder to the client, this is not the best option. To communicate effectively, the health care administrator could utilize other tools such as symbols, pictures and use of hand signals.
Question 2
Sometimes people who may not speak the dominant language well feel most comfortable bringing a family member to interpret for them. Sometimes this may even be a child. What might be the reason that a family member and especially children may not be a good interpreter. (Select all that apply)
The family member especially children may find the health care news upsetting and may not translate word-for-word what is being said
Privacy violations may happen if we are not completely sure we have the client’s expressed consent for disclosure of private health information
The family member may not understand the medical terms and therefore not explain correctly.
Solution. The correct response is option one, two and three. The Health care administrator cannot verify if the information is correct when a family member interprets. As well, this is a PHIPA violation. Return to Activity
Check your Understanding (Text-based Activity)
Question 1
The language interpreter will
Be able to understand and speak the client’s language and dialect.
Is bound by confidentiality clauses/agreements
May ask for clarification
Solution. The correct response is option one, two and three. The language interpreter must be able to understand and speak the client’s language and dialect. They are bound by strict confidentiality agreements and follow PHIPA. At times the conversation may last longer as the interpreter may ask for clarification. Return to Activity
Describe the encompassing elements of loss and grief.
Explore the stages and models of grief applying the Kübler-Ross Grief Cycle.
Recognize how personal beliefs, culture, spirituality, and experiences, affect responses to sensitive communication.
Review options for end-of-life care recognizing the personal decision making involved.
Introduction
According to the Canadian Mental Health Association (CMHA), grief is both a feeling and a process that people typically go through after a death or other significant loss (2021). Loss in its simplest description means losing something or someone and from this loss feelings of grief emerge. Loss and grief are entities experienced in the health care environment. Health care professionals often prepare patients/clients and their families for this sometimes inevitable experience. A serious injury, chronic illness, an unexpected alteration in body, or death are experiences that can trigger an array of emotional responses categorized as loss and grief. Anticipatory grief is a reaction to an upcoming, impending, or expected loss event. Experiencing grief can be an important part of the process and can help a person sort out emotions in preparation for the loss. In these sensitive moments what is said or not said has a significant impact. Importantly the perception of loss is real and unique to each person. Grief is in the internal emotional processing of the loss an individual experiences.
A compassionate approach is needed and HCAs can provide comfort both in words and in action. It can be challenging to comfort someone who is experiencing grief as it may remind us we are not able to remove or stop the pain. As empathetic practitioners, we often want to make it better and take the pain away. This chapter is designed to provide a thoughtful examination of loss and grief to support therapeutic communication processes.
Assessing What You Already Know
This activity to designed to explore what you may know about this chapter topic
As mentioned in the introduction to the chapter grief can trigger several emotional reactions. Developing an awareness of these emotional responses strengthens the ability to support patients/clients, and their families. Some examples of emotional reactions are explored further in the next paragraphs.
Sadness is an emotional reaction commonly associated with grief. The profound hopelessness, despair, and loneliness can make the individual feel emotionally unstable. They may cry frequently as an emotional display.
Shock as an emotional reaction sees an individual expressing feelings of disbelief . At this point, the individual may feel numb and are experiencing trouble accepting the loss has occurred or is occurring.
Guilt is an emotional response that often leaves the individual feeling guilty for something they did or didn’t do. Even if the loss is out of their control, they may still feel they could have done anything to help prevent it.
Fear can be an emotional response to grief and individuals may feel anxious, uncertain about the future, and generally express feelings of worry. The fear is generally rooted in moving on to accept life as it now is, not as it was.
Media Review: 5 Things About Grief No One Really Tells You
Please be aware, this video contains information that some may find emotionally intense to view.
As you watch the following video consider the five elements explored surrounding grief and respond to the reflective questions.
Reflective Questions:
How does the content explored in the video relate to therapeutic communication when communicating with a client experiencing grief?
Is there anything you would add to the concepts presented in the video? Why does this additional component belong here?
Our understanding of grief is a constantly evolving process and over time several grief models have emerged. According to Clewell (2004), Sigmund Freud proposed over 100 years ago a theory of grief which proposed that “mourning comes to a decisive end when the subject severs its emotional attachment to the lost one and reinvests the free energy in a new object.”
A more recent model of grief is known as the adaptive grief model. This model was proposed by Kenneth Doka and Terry Martin in the book Grieving Beyond Gender. Adaptive grief reflects that grief is a complex process and is unique to the individual. It involves accepting that life will never look or feel the same. The theory also recognizes response to grief has many variables such as an individual’s personality and cultural background.
Stages of Grief
Elisabeth Kübler-Ross was a psychiatrist who conducted significant investigative studies relating to near-death grief and from this groundbreaking research key stages of grief were identified in her book On Death and Dying (1993). The five stages identified include denial, anger, bargaining, depression and acceptance. These stages are a part of the framework that facilitates learning to live with loss and they are also sometimes referred to as the Kübler-Ross Grief Cycle. Initially, this cycle referred to death only and has since been expanded to encompass all types of grief and loss. David Kessler a death and grieving expert identified the sixth stage of grief referred to as finding meaning. Kessler explored this stage in the book titled Finding Meaning, The Sixth Stage of Grief (2019).
Let’s explore the grief stages further outlined by Kübler-Ross. Each stage is listed in order based on the grief cycle however, it is important to consider not every individual goes through all stages, nor do they transition in the order provided in this chapter. Grief and loss are experienced uniquely for everybody.
Denial
Denial is often presented as the first stage of grief lasting weeks or months. Think of a time when you received extremely upsetting news involving a loss. Often the immediate denial reaction triggers feelings of being in a state of shock or numbness with little to no emotional reaction. The temptation to think a mistake or error has been made accompanies the denial phase. The state of shock denial helps with the survival need surrounding the event, it is the creation of an alternate reality as a coping strategy.
Anger
In this stage, the individual begins to transition back to reality. Individuals may begin to blame others or question, why me? Anger can be the most difficult for caregivers to witness. Individuals experiencing the anger stage may lash out at everyone alike because they are angry about their situation. Often, nothing done is done right for them. They have negative things to say about other aspects of their life as well (Lowey, 2015).
Bargaining
In this stage, an individual may experience a sense of false hope. If they make a promise to do better it may fix the situation and take away the grief and loss. The person attempts to create a deal in a hopeless effort to repair the event. It is a stage that is rarely visible to onlookers as it happens internally within the person affected. In this stage, individuals realize that they are past denial and they have been angry about it, with neither of the two causing any change in the outcome (Lowey, S. 2015).
Depression
Depression is the fourth stage and is a natural part of grief where feelings of sadness occur. The ability to function with normal day-to-day routines may be impacted. Some individuals may experience a prolonged period of sadness and will require additional considerations and supports.
Acceptance
The final stage is acceptance. This stage does not mean that the person is happy about the situation, but rather that they have come to accept it and have found a sense of peace with it. The first four stages involved mostly negative emotions which have taken a toll on those involved. In the case of a terminally ill patient, the time has progressed and patients can begin to move past the negative emotions and focus on the time they have left. During this stage, their hope for a cure is replaced by a hope that their final days will be peaceful and their death will be what they want it to be (Lowey, 2015).
Responding to Grief
Scenario: Employed as Health Care Administrator an individual has arrived at the health care facility and they are experiencing the recent loss of their life partner and they make the following statements. As you read through these, consider possible therapeutic responses:
I don’t think I will ever get over the loss of my partner, what do you think I should do?
How can I live with this loss?
When will I feel better?
Communicating with Individuals Experiencing Grief and Loss
As mentioned at the start of this chapter, it can be overwhelming to communicate with someone who is grieving and experiencing a loss. In the role of an HCA, we will be exposed to many forms of loss and grief. Loss and grief can be intensely emotional. Being aware of communication techniques to support patients/clients and their families during these circumstances are critical for establishing and maintaining a therapeutic relationship.
Behaviour strategies to support the therapeutic communication process can include:
Acknowledge the situation. Recognizing what the individual is going through at this moment is extremely painful. This provides space for the individual to grieve fully. Making a statement such as “It’s really tough right now for you” demonstrates a recognition of the emotional pain.
Express authentic concern. Focus on the individual experiencing this loss. Making a statement such as “I’m sorry you’re suffering” demonstrates an empathetic acknowledgment.
Provide space for the grieved to talk. Asking if the grieved would like to talk or share how they feel about their loss is helpful.
Recognize common situations that result in difficult communication, such as a patient receiving bad news about their health condition. It’s human nature to want to avoid stressful situations. Supporting someone who is grieving may be a stressful situation.
Ambiguous Loss
This is a type of loss experienced where there is no clear or direct understanding of the loss. Examples of this kind of loss include infertility, unexpected termination of a pregnancy, a family member in cognitive decline. Ambiguous loss can be either physical or psychological. This differs in comparison to traditional loss largely in the way the individual’s loss is perceived and supported by those around them. With ambiguous loss, it tends not to be legitimized by society therefore, the typical supports provided may not exist. An HCA can demonstrate support when therapeutically communicating with client and family members recognizing loss may not be an obvious event and something that transpires over time.
Tips for Supporting Ambiguous Loss
Review this list.
Identifying and recognizing this event is a loss.
Provide information regarding support groups.
Recognize what still exists in life.
Support ways to find new hope for now and the future.
Beliefs, Culture, Spirituality, and Experiences
In times of grief and loss, individual beliefs can provide support and comfort. The manner in which people mourn is affected by religious practices, beliefs, and cultural traditions. People who are grieving are sometimes described as bereaved. Personal philosophies may affect reactions and responses to grief and loss. For example, in some cultures, people believe a deceased family member’s spirit influences the remaining family members. Individuals gain comfort in the belief that their loved one is watching over them. Generally, beliefs provide a mechanism to help people make sense of the loss experienced.
In most cultures, death is associated with rituals which are designed to honour the individual lost and help the family members cope with their loss. For instance how a body is handled after death matters as does burial or cremation beliefs. Another example is the privatization of grief, in some cultures, grief is expressed quietly while in others grief is expressed loudly and publicly. As HCA’s we should recognize various beliefs and respond with care and without judgement. Remember there is no right or wrong way to grieve.
Some cultural examples to consider surrounding death and dying include:
African death ritual of turning all pictures to face the wall and covering all mirrors, windows, and reflective surfaces so the dead can’t view themselves.
Death customs in China see the removal of mirrors and hanging cloth on the doorway of their homes. Not following proper rituals means death and misfortune for the grieving family.
Some South American practices include drinking a mixture of ashes and bananas to keep the spirit of the deceased alive.
In Russia, prior to a funeral family members stop clocks and cover mirrors to avoid more death in the family.
The combination of social and cultural influences impacts the grieving cycle. The social influences of grief include: withdrawal from activity typically enjoyed to avoid judgement by others, isolation from society, arising conflict related to grieving differently than others in their social circle leading to unrealistic expectations and unresolved grief.
Cultural Considerations
Read the following options concern beliefs surrounding death. Which option best describes your belief? How do you think your belief is impacted by your cultural identity?
Death is passing on to a new life – it is a spiritual journey.
Death is an end, not the start of an afterlife.
Death separates the dead from the living.
Death is a momentary event.
I do not identify with any of the statements and I have a different opinion.
I am undecided where my beliefs reside.
End-of-Life Care Options and Decisions
End-of-life care is the term used to describe the support and medical care given during the time surrounding death. End-of-life care and planning are critically important to the next decades of health care in Canada. Between 2005 and 2036 in Canada, the number of seniors 65 years and older is projected to increase by up to 25% and the number of deaths by 65%. The majority of patients are currently admitted to hospital and many to intensive care units at the end of life; however, up to 70% of elderly patients say they would prefer a less aggressive treatment plan focusing on providing comfort rather than a technologically supported, institutionalized death (Fowler, 2013). According to Health Canada Services at Canada.ca, these options include palliative care, do not resuscitate (DNR) orders, refusal or withdrawal of treatment, refusal of food and water, sedation to ensure comfort, and medical assistance in dying. Decisions at end of life are uniquely individual and personal.
Palliative Care
This is specialized care offered to those experiencing a serious illness. This type of care focus is primarily on relieving symptoms and the encompassing stressors caused by the condition. Often the goal is to provide and support quality of life for the patient and their family members. The supports can include, emotional, nutritional, medical interventions such as pain medications, and additional comfort measures. Palliative care can be provided in a hospital setting, as residential care in a long-term care facility, and daycare/homecare. As an HCA you may work in a palliative care setting and therapeutic communication skills are essential elements of supporting quality of life for clients and their families.
Advance Care Planning (ACP)
This is a formal process supporting adults of varying stages of life identifying and sharing their values and decisions regarding future medical care. An example of this is a document commonly referred to as a living will, included within the living will is usually advance care directives. A directive in this context could outline how medical care will be utilized if the individual does not have the capacity to make a decision during a critical health event. Other examples of advance care planning include a do not resuscitate (DNR) order, substitution decision-maker assigned often to a loved one by the client to make health and other related decisions if they become unable to do so.
Assisted Dying
This is a practice where a person suffering a terminal illness or incurable condition is assisted in concluding their life. In Canada, it is often referred to as MAiD (medical assistance in dying). Clients who make these end-of-life decisions need support and understanding as do their family members. It is often a highly emotional time for all persons involved and therapeutic communication techniques are extremely important to ensure clear, timely communication is conveyed to the client and family surrounding this event.
Explored the components of loss and grief within the context of health care.
Recognized everyone experiences grief and loss in their life.
Focused on grief and the internal processing of loss.
Explored how developing an awareness of loss and grief better equips the HCA to approach situations involving these sensitive interactions with care and empathy.
Key Terms
Alternate: Taking the place of the current.
Anticipatory grief: Is a reaction to an upcoming, impending, or expected loss event.
Bargaining: Negotiating, agreement, or contract. (Merriam-Webster, n.d)
Bereaved: Someone who is afflicted by the death of a loved one. (Merriam-Webster, n.d)
Cognitive: Thinking, reasoning, knowing, remembering, and problem-solving abilities.
Compassionate: Showing concern for others.
Despair: Complete loss of hope.
Disbelief: Inability to accept something is real or true.
Grief: Is both a feeling and a process that people typically go through after a death or other significant loss.
Legitimized: Viewed as valid.
Mourn: To feel or show deep sorrow or regret.
Philosophies: A system of thought.
Rituals: Ceremony consisting of several ordered steps.
Shock: State of being severely disturbed. (Merriam-Webster, n.d)
Spirit: The non-physical part of a person their emotions and character; the soul.
Trigger: Something that causes the appearance of something else. (Merriam-Webster, n.d)
Clewell, T. (2004, March 1). Mourning beyond melancholia: Freud’s psychoanalysis of loss. Journal of the American Psychoanalytic Association, 52(1): 43-67. https://doi.org/10.1177%2F00030651040520010601
Fowler, R., & Hammer, M. (2013, June 1). End-of-life care in Canada.Clinical and Investigate Medicine, 36(3): E127-32. doi: 10.25011/cim.v36i3.19723
Kübler-Ross, E. (1969, revised 1993). On death and dying. Collier Books/Macmillan Publishing.
Assessing What You Already Know (Text-based Activity)
Question 1
Recall the recording at the start of this chapter. Based on what you heard and the members involved in this recording, do you think Dr. Oleg has disappointing health news for the client, Kelly?
True
False
The correct response is True. It can be very challenging to deliver disappointing news.
Question 2
Consider a friend reached out to you today. This friend told you they were in an car accident last week and are presently in the hospital recovering. This friend shared since the accident their ability to walk appears to be compromised. The primary care physician is unsure what deficits will remain for mobility. The friend expressed feelings a sadness and worry about what will come next in their recovery process. If you were to apply a description to what your friend is experiencing which of the following words apply, select all that apply:
Confusion
Lack of motivation
Loss
Grief
The correct response is option three. This is an example of a physical loss where your friend is experiencing the possible alteration of body and ability. This will have a number of considerations for their future.
Question 2
Is grief a normal reaction to a loss?
True
False
The correct response is true, grief can be a normal reaction to any type of loss.
Question 3
Is anger an unusual response to grief?
True
False
The correct response is false. Anger is a normal part of grieving. it is not unusual for people to experience a range of emotions as part of the healing process. Return to Activity
Assess the implication of stressors on anxiety disorders and mood disorders using common theoretical models.
Explore symptoms and behavioural manifestations of common anxiety disorders and mood disorders.
Review effective therapeutic communication techniques when communicating with a client suffering from anxiety disorders and mood disorders
Consider the scope of practice of the health care administrator in supporting clients in various levels of mental well-being.
Introduction
The Canadian Mental Health Association (CMHA), National (2019) proposes that 1 in 5 people experience an issue with their mental well-being in a given year, and mental health symptoms worsen if supports are difficult to access. The ability to recognize behaviours associated with mental health challenges assists in communicating effectively with those who are suffering from them. Studying and learning about common mental health illnesses, reduces fear, increases compassion, and allows for greater empathy when communicating with people suffering from issues with mental well-being. The health care administrator (HCA) who utilizes effective therapeutic communication techniques when communicating with clients experiencing a mental health issue, will assist the client and their family in accessing the supports that they need.
Assessing What You Already Know.
As you reflect upon the questions and statements consider what you already perceive about mental well-being.
All people will experience stress during their lifetime, and people’s perception to stressors differs. A small amount of eustress is considered helpful because it is short in duration and it works to sharpen senses and focus (Jenkins et al., 2021). Think about the few minutes before you begin a test, that feeling of butterflies in your stomach, then once the test begins you settle in and focus. While a certain level of eustress can be helpful, it can not be sustained for long periods of time, and once stress becomes overwhelming it is then considered distress. If levels of distress do not dissipate then it begins to impact a person’s well being both physical and mental (Jenkins et al., 2021).
Hans Seyle’s General Adaptation Syndrome
Hans Seyle’s General Adaptation Syndrome (GAS) model offers a three-stage explanation for how the body responds to stress and how repeated stressors can lead to a number of disorders and diseases. The first phase is the alarm phase when the fight-or-flight response in the body begins. In this phase the hypothalamus release hormones including Adrenaline and Cortisol into the bloodstream (Herkimer County Community College & Pelz. B., n.d.). Cortisol and Adrenaline provide that boost of energy that allows the body to fight or flee. If the stressor remains, then the person moves into the second phase, the resistance phase, where the initial jolt is gone but the body remains on alert with increased glucose levels, cortisol levels, and high blood pressure (Stangor. C., & Walinga. J., 2014). Long sustained levels of Cortisol will weaken the immune system and if chronic, may lead to disorders and disease (Stangor. C., & Walinga. J., 2014). The final phase is the exhaustion phase, the body is no longer able to adapt, the ability to resist combined with the constant levels of Cortisol takes it tole on the body resulting in damage to the body (Herkimer County Community College & Pelz. B., n.d.).
Consider this Situation
Consider for a moment that Jamal has just been told by Dr. Livingstone that he has cancer. Jamal doesn’t hear anything Dr. Livingstone is telling them after the word cancer. Luckily Jermaine has come with Jamal and can take down the information. It is likely that Jamal’s body is preparing to flee.
Jamal later accepts the diagnosis and begins their treatment. Over the course of two years, there are periods of exacerbation and remission. Each time, Jamal adapts and stays resistant but over the course of treatment these types of stressors along with the disease they are fighting, take their toll not only on Jamal’s physical health but on their mental well-being.
Jamal has been in remission for more than five years and is considered cured. Jamal’s anxiety about cancer coming back and chronic depression make it impossible for Jamal to hold down steady employment. Jermaine is tired all of the time and suffers from chronic headaches, and worries that Jamal will never be able to contribute to the family household and feels guilty for resenting Jamal. Fox (2019) suggests that cancer survivors may suffer from anxiety & depression, and their families from caregiver burnout. The good news is there are supports available to assist.
Physical Signs & Behavioural Manifestations of Stress
Signs that a person under stress may exhibit include:
Physical
Dry mouth, heavy breathing, dilated pupils, sweaty palms, rapid heart rate, and trembling. Consider these are physical manifestations of the body’s flight or fight responses to the stressor (Stangor. C., & Walinga. J., 2014).
Cognitive
Difficulty concentrating or making decisions.
Behavioural
Misuse of drugs & alcohol, excessive eating, or smoking (Herkimer County Community College & Pelz. B., n.d.).
Anger is a manifestation of stress and can range from being slightly annoyed for having to wait in line, to feelings of rage over a real or perceived injustice (Canadian Mental Health Association National, 2019).
Clients and their families seek health care when they are feeling unwell, dealing with life’s stressors and uncertainties. As a Health Care Administrator (HCA) you will see signs and behaviours that may seem on the surface as excessive or unreasonable responses to the situation.
Consider this Situation
Karla, arrived an hour early for their appointment, is pacing back and forth in the waiting room and comes to the check-in window numerous times to find out how long the wait will be. Each time that Karla comes to the window they are increasingly agitated to the point that you sense they are getting angry.
You might be thinking the client came an hour early so this is an unreasonable response.
Consider that the behaviour is related to the stressor:
Karla is here to obtain recent test results.
Perhaps their agitation is related to the stressor of wondering what the test results will reveal and not that they have to wait.
Awareness that stressors may be behind those behaviours, will assist you to empathize with the client and to show them compassion.
Anxiety Disorders & Mood Disorders
Anxiety differs from stress, with anxiety the excessive worry is persistent even when the stressors are removed (American Psychological Association, 2020). Mood disorders and anxiety disorders impact the daily lives of approximately 11.6% of Canadians 18 years or older (Government of Canada, 2015). 27% of people with mood or anxiety disorders, report that their daily life has been highly impacted by their disorder, and 95% of those reported seeing a health care provider for assistance (Government of Canada, 2015). Psychological disorders often occur together, this comorbidity means that the most severe disorders are concentrated in about 6% of the population (Stangor. C., & Walinga. J., 2014). It is likely that you will have clients and their families coming to the office suffering from an anxiety or mood disorder at some point in your career and learning about those disorders, and awareness about the signs, symptoms, behavioural manifestations will increase your empathy and ability to connect clients to supports.
Anxiety Disorders
General Anxiety Disorder (GAD)
General Anxiety Disorder (GAD) is a psychological disorder in which significant distress and dysfunction are caused by worrying excessively (six months or more), about common situations even though the person recognizes there is nothing to worry about (Government of Canada, 2009). Physical symptoms of GAD may include irritability, insomnia, lack of concentration, trembling, and achy muscles, in which symptoms can range from mild anxiety to panic disorder (Stangor. C., & Walinga. J., 2014).
Levels of Anxiety
There are generally thought to be four levels of anxiety with signs and symptoms varying based on the level. Townsend (2014) proposes that low levels of anxiety provide motivation, but that anxiety can become problematic when symptoms are severe enough to interfere with a person’s daily life. Responding therapeutically to people in the various levels of anxiety will reduce their level of anxiety and provide an opportunity to meet their health care needs. A Health Care Administrator (HCA) will need to consider their scope of practice in responding to various situations involving people with anxiety. It may be necessary to report incidents to the Health Care Provider (HCP) or request the help of the HCP when situations exceed the HCA’s scope of practice.
Mild Anxiety
Mild Anxiety is a common experience of everyday life, and much like eustress is considered helpful since it heightens awareness and perceptions. A client experiencing mild anxiety may present as fidgety, irritable, bite their nails, swing their foot, and ask many questions as ways to relieve anxiety (Townsend. M., 2014).
Effective therapeutic responses to someone experiencing mild anxiety is answering questions, being direct, and offering reassurance through both verbal and nonverbal communication.
Moderate Anxiety
Moderate Anxiety symptoms may present as decreased perception, single focus, dry mouth, rapid breathing, fast speech, and even anger as the body’s sympathetic system responds to the real or perceived threat. A person experiencing moderate anxiety may require more direction and assistance with solving problems (Townsend. M., 2014).
An effective therapeutic response to someone experiencing moderate anxiety is to use techniques such as observation and validation. For example, observe that the person is anxious and say something like, “you seem anxious about your appointment”, wait for the person’s response, and then validate their response.
Answer questions that the person asks you, speak in a calm and reassuring manner, begin to exaggerate your breath as you speak to them, in this way the person will begin to mimic your breath and as you begin to slow down breathing, so will they. Subsequently, their pace of speech will slow down too.
Severe Anxiety
Severe Anxiety symptoms may present as a lack of concentration, and the person may only be able to follow one instruction at a time (Townsend. M., 2014). Physical symptoms increase such as headaches, heart palpitations, and insomnia (Townsend. M., 2014).
In this circumstance an effective therapeutic response includes, giving one verbal instruction at a time, writing out any follow-up instructions, and giving written instructions to a client’s family member if they are available, and you have the client’s consent.
Panic Attack
A panic attack is characterized by an unexpected sudden surge of fear with physical symptoms that are similar to a heart attack; such as dizziness, heart palpitations, shortness of breath, trembling, choking, and nausea (Bridley. A. & Daffin Jr. L.W., 2018) (Stangor. C., & Walinga. J., 2014). A person who is experiencing a panic attack may want to leave the situation.
An effective therapeutic response to a person experiencing a panic attack is to allow them space to get up and move or lay down if they are experiencing dizziness. If they insist on leaving, ask if there is someone you can call, encourage a short walk around the block, and ask them to return. It would be best for a HCA to call the HCP for assistance with the client or the client’s family members in this situation.
Panic Disorder
Bridley.A., & Daffin JR. L.W. (2018) propose that panic disorder is a series of unexpected panic attacks and that people suffering from panic disorder manifest behavioural changes like fear of leaving their house because they do not know what caused the panic attack or when it might happen again. People suffering from panic disorder become anxious and may focus on cues to what might set off another attack, and as a result may avoid situations in which attacks have occurred, like driving, elevators, or specific spaces (Stangor. C., & Walinga. J., 2014).
Phobias
A phobia is a fear of something specific such as an object, activity, or situation, and can range from a sense of unease, mild anxiety, or panic attack (Bridley. A., & Daffin JR. L.W., 2018). Most often the person will avoid what they fear, even if that avoidance is extreme. Depending on the severity of a person’s phobia , they can function without anyone noticing but for those whose phobias lead to panic disorder it can become debilitating and impact their daily life. Stangor. C., & Walinga. J. (2014) proposes that agoraphobia is one of the most severe phobias, in which suffers fear to leave their homes and interact with others. See the list below of some common phobias.
Table 10.1 Modified List of Common Phobias from Introductory to Psychology-1st Canadian Edition. From Stangor & Walinga, 2014.
Name
Description
Acrophobia
Fear of heights
Agoraphobia
Fear of situations that are difficult to escape from
Arachnophobia
Fear of spiders
Astraphobia
Fear of thunder and lightning
Claustrophobia
Fear of closed-in-spaces
Cynophobia
Fear of dogs
Mysophobia
Fear of germs or dirt
Ophidiophobia
Fear of snakes
Pteromerhanophobia
Fear of flying
Social phobia
Fear of social situations
Trypanophobia
Fear of injections
Zoophobia
Fear of small animals
Obsessive Compulsive Disorder (OCD)
Obsessive-compulsive disorder (OCD) is a psychological disorder in which a person engages in obsessions or compulsions as they attempt to calm frightening and distressing thoughts (Bridley. A., & Daffin JR. L.W., 2018). Unnecessary behaviours become ritualistic due to the calm they bring even when the person suffering from OCD recognizes the behaviours are not healthy (Stangor. C., & Walinga. J., 2014).
Posttraumatic Stress Disorder (PTSD)
Figure 10.1 A soldier who is battling PTSD
People that witness, experience, or learn about someone close to them experiencing a traumatic event are at risk of suffering from posttraumatic stress disorder (PTSD) (Veteran’s Affairs Canada, 2019). Approximately 9.2 % of Canadians will experience PTSD in their lifetime with a higher incidence reported in women (Veteran’s Affairs Canada, 2019). Types of traumatic events include, but are not limited to, combat, sexual abuse, violent crimes, major accidents, and natural disasters (Government of Canada, 2021).
High levels of anxiety with flashbacks to the initial trauma are reported in people suffering from PTSD, and subsequently, people with PTSD wish to avoid reminders of that trauma (Stangor & Walinga, 2014). Manifestations of PTSD are similar to other types of anxiety disorders such as panic attacks, pain, headaches, digestive problems, as well as depression, alcohol misuse, and substance misuse (Veterans Affairs’ Canada, 2019). Since flashbacks can be intense with outbursts, this may lead to embarrassment and shame for the trauma survivor, causing them to withdraw, further exacerbating their symptoms because they have isolated themselves from others (Veteran’s Affairs Canada, 2019).
Since PTSD is the manifestation of a traumatic event, applying a trauma-informed approach (TIA) to communicate therapeutically with clients suffering from PTSD is important. As you will learn in the Trauma-Informed Communication chapter, a TIA is critical to building trust with the client, while promoting lifelong health and wellbeing for people who have suffered a trauma. For a Health Care Administrator (HCA) this starts with empathy and awareness that a person displaying behaviours that appear extreme or that you may find frightening, like an outburst related to a flashback, may be suffering from PTSD. It is important to remain empathetic and provide the person with as much privacy and discretion that is safe for you to do so. Consider the scope of practice of HCA, and with discretion, ask for assistance from the Health Care Provider (HCP).
Mood Disorders
Most people experience times of feeling low due to varying situational factors. For example, complex interpersonal relationships, loss, and even external factors such as low daylight hours during long Canadian winters. Consider Mrs. Weber (in the opening scenario) may be suffering from a mood disorder due to the situation of her partner moving into a long-term care home and the loss of what their relationship once was. Mood disorders negatively impact the way people think, socialize, perceive interactions, and can manifest into negative moods, sadness, and depression (Stangor. C., & Walinga J., 2014). Diagnosing depression is far beyond the scope of the health care administrator (HCA) but awareness about the signs, symptoms and behavioural manifestations will increase your empathy and ability to connect clients to support.
Depression
Figure 10.2 Woman looking depressed. Photo credit OER Conestoga College.
Levels of depression vary between people based on many factors such as situational factors, biological factors, and hereditary factors or a combination of factors.Dysthymia is considered a mild form of depression but long-lasting at a minimum of two years. Major depressive disorder, also referred to as clinical depression is considered a more severe form of depression since negative feelings of sadness, despair and loss of interest limit the person’s day-to-day activities (Stangor. C., & Walinga J., 2014).
Stangor. C., & Walinga. J. (2014) proposes that people suffering from depression have overwhelming negative moods and this may be demonstrated by the following symptoms:
Changes in appetite
Difficulty concentrating
Fatigue
Feeling hopeless, helpless and pessimistic
Misuse of alcohol or drugs
Irritability
Loss of interest in things that were once pleasurable
Loss of interest in personal appearance
Persistent aches and pains
Sleep disorders
Suicidal thoughts
Types of Depression Diagnoses
The following is a list of common types of depression diagnoses that are not covered in this chapter. You are encouraged to explore them on your own. Are there any others that you would add to this list?
Postpartum Depression
Seasonal Affective Disorder (SAD)
Situational Depression
Persistent Depressive Disorder
Atypical Depression
Treatment-Resistant Depression
Bipolar Disorder
Bipolar disorder differs from depression in that there are periods of depression, periods of stable mood, periods of mania, or mixed episodes that display both depression, and mania, at the same time (CAMH Bipolar Clinic Staff, 2013). During periods of mania, behaviour can range from exaggerated self-esteem, increased talking, racing thoughts, poor judgement, increased irritability, lack of concentration to hallucinations and suicidal thoughts (CAMH Bipolar Clinic Staff, 2013). Stangor. C., & Walinga. J. (2014) proposes that if bipolar disorder is left untreated symptoms exacerbate leading to harm to self or others.
Schizophrenia
Demonstration of Behavioural Manifestations in a Client with Schizophrenia
Attribution to Simulated Patient with Schizophrenia video from the ARISE Therapeutic Communication for Schizophrenia Serious Game created by Chippewa Valley Technical College and licensed under CC-BY- 4.0.
In Canada, one out of ten Canadians over the age of ten were living with diagnosed schizophrenia according to data gathered in 2016-2017 (Government of Canada, 2020). Stangor. C., & Walinga. J. (2014) proposes that schizophrenia is one of the most debilitating psychological disorders because symptoms impact daily life so severely. While symptoms vary in people with a Schizophrenia diagnosis the American Psychiatric Association divides them into three categories as seen in the chart below (Stangor. C., & Walinga, J., 2014).
Table 10.2 Positive, Negative, and Cognitive Symptoms of Schizophrenia. From Stangor & Walinga, 2014.
Positive Symptoms
(not seen in the general population)
Negative Symptoms
(seen in the general population)
Cognitive Symptoms
(changes due to Schizophrenia)
Hallucinations
Social withdrawal
Poor executive control
Delusions (of grandeur or persecution)
Flat affect and lack of pleasure in everyday life
Trouble focusing
Derailment
Apathy and loss of motivation
Working memory problems
Grossly disorganized behaviour
Distorted sense of time
Poor problem-solving abilities
Inappropriate affect
Lack of goal-orientated activity
Movement disorders
Limited speech
Poor hygiene and grooming
Mental Illness, Substance Misuse, Addiction, and Homelessness
Due to behavioural manifestations of mental illness, people suffering from mental illness find it challenging to maintain regular employment and stable income. This may lead to housing insecurity, homelessness, and poor health care outcomes. The Canadian Mental Health Association (CMHA) Ontario (2021), estimates that 25 – 50 percent of homeless individuals suffer from a mental health illness. Without supports, people experiencing homelessness combined with the behavioural manifestation of mental illness may also suffer from substance misuse or addiction (CMHA Ontario, 2021). According to a 2018 report, approximately 25% of people who responded to the survey indicated that addiction or substance use was the reason that they were homeless (Baker. N., Cooper. I., Hunter. P., Quayum. S., Rivier. J., 2018).
Employment opportunities exist for Health Care Administrators with organizations that support people suffering from mental illness, addiction, and homelessness. Investigation into the reasons that people suffering from mental illness behave the way they do, will assist you in understanding the supports needed, reduce your fear of behaviours, and increase your confidence to competently and compassionately assist clients suffering from mental illness, substance misuse, addiction, and homelessness.
Assessed the implication of stressors on anxiety disorders and mood disorders using common theoretical models.
Explored symptoms and behavioural manifestations of common anxiety disorders and mood disorders.
Reviewed effective therapeutic communication techniques when communicating with clients suffering from anxiety disorders and mood disorders.
Considered the scope of practice of the health care administrator in supporting clients in various levels of mental well-being.
Key Terms
Addiction: A solid need to habitually use or do something. (Merriam-Webster, n.d)
Agoraphobia: Anxiety about being in places or situations where escape might not be possible (Stangor & Walinga, 2014).
Anxiety: Excessive worry, nervousness, or fear even when the stressors are removed.
Anxiety disorders: Psychological disturbances that include irrational fears of what most would perceive as everyday situations and objects (Stangor. C, & Walinga. J., 2014).
Alarm phase: First phase in Hans Seyle’s General Adaptation Syndrome. The fight-or flight response is activated (Pelz & Herkimer County Community College, n.d.).
Behaviours: The way a person act (Merriam-Webster, n.d).
Comorbidity: Suffering from two or more disorders at the same time.
Compulsions: Repetitive behaviours.
Distress: When the level of stress is no longer helpful and becomes overwhelming and debilitating (Pelz & Herkimer County Community College, n.d.).
Dysthymia: Mild form of depression.
Exacerbation: Increase in severity.
Exhaustion phase: The third and final phase of Hans Seyle’s General Adaptation Syndrome model. The body is no longer able to adapt and sustained levels of Cortisol takes it tole on the body (Pelz & Herkimer County Community College, n.d.)
Eustress: Stress for a short duration considered good stress eu/stress.
Fidgety: Inclined to easily upset (Merriam-Webster, n.d).
Flight-or-fight response: The activation of both sympathetic nervous system and the endocrine system in response to a real or perceived threat. Blood flow goes to essential organs allowing the body to either fight the threat or flee from the threat (Pelz & Herkimer County Community College, n.d.).
General Adaptation Syndrome (GAS): Hans Selye created this term to refer to the three phases in which the mind and body change in response to long-term stress.
Homelessness: Not having a place to live (Merriam-Webster, n.d).
Major depressive disorder: Clinical depression is a severe form of depression as it limits the person’s day-to-day activities.
Misuse: incorrect use of something (Merriam-Webster, n.d)
Mood disorders: Lowering of a person’s mood.
Obsessions: Repetitive thoughts.
Outburst: stern expression of a feeling (Merriam-Webster, n.d).
Panic Attack: An unexpected sudden surge of fear with physical symptoms.
Panic disorders: A series of unexpected panic attacks that becomes debilitating.
Phobia: Fear of something specific such as an object, activity, or situation.
Posttraumatic Stress Disorder (PTSD): A psychological condition occurring when a person experienced a highly stressing situation (Merriam-Webster, n.d).
Remission: A period of time when there is relief from symptoms.
Resistance phase: The second phase of Hans Seyle’s General Adaptation Syndrome model. The body remains on alert but the initial jolt is gone (Pelz & Herkimer County Community College, n.d.)
Stress: Researchers vary on their definition of stress but it is generally thought to be the response to a stimulus (stressor) or response to a perception of a stressor (Pelz & Herkimer County Community College, n.d.).
Stressor: Being something an individual determines is overwhelming or a potential threat to their wellbeing (Pelz & Herkimer County Community College, n.d.).
Sympathetic system: the part of the nervous system that prepares the body to react to situations of stress or alarm (Merriam-Webster, n.d).
Townsend, M. (2014). Psychiatric mental health nursing : Concepts of care in evidence-based practice [ProQuest Ebook Central].Philadelphia, Pennsylvania : F. A. Davis Companyhttps://ebookcentral-proquest-com.conestoga.idm.oclc.org
Develop the understanding of a trauma-informed approach to communication.
Develop a trauma-informed approach in the health care settings.
Develop an awareness of the client’s reactions or behaviours that may be related to past trauma.
Create safe and less traumatic environments for clients who may have experienced trauma.
Introduction: What is a Trauma-Informed Approach?
Many people experience trauma in their lives, many of whom do not seek timely health care. Thus it is essential for all communications with health care professions, to begin with, a foundation of understanding that all persons have experienced trauma at some time in their lives. The approach is called trauma-informed communications. Trauma refers to any experience that may cause intense physical and psychological stress reactions. It can refer to “an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or threatening and that has lasting adverse effects on the individual’s functioning and physical, social, emotional, or spiritual well-being” (Substance Abuse and Mental Health Services Administration (SAMHSA), 2019). To establish effective communication, healthcare professionals need to know the six principles of trauma-informed care: safety, trustworthiness and transparency; peer support; collaboration and mutuality; empowerment, voice and choice; and cultural issues (National Center on Domestic Violence, Trauma & Mental Health, 2019).
Children and young people who have experienced trauma have little space for learning. Their constant state of tension and arousal can leave them unable to concentrate, pay attention, retain and recall new information. Their behaviour is often challenging in the health care environment when the goal is to assist the client. Trauma can also affect a client’s decisions or the ability to trust others, including health care professionals. As a result, it becomes increasingly challenging for the trauma survivors when communicating with others as they tend to protect themselves from reliving the traumatic experience. The traumatized client may feel like danger lurks around the corner constantly.
Acute trauma from a singular incident, such as a natural disaster, accident, or acts of violence.
Chronic trauma is repeated and prolonged, resulting from situations such as domestic violence or abuse.
Complex trauma is varied, and multiple traumatic events, often of an interpersonal nature, such as abuse or profound neglect, often occur with caregivers.
Historical trauma may include multigenerational and experienced by a specific cultural, racial or ethnic group, often related to significant events that oppressed a group of people, such as slavery, the Holocaust, forced migration or violent colonization (City of San Diego, n.d.).
One may experience one, some or all these traumatic stresses during their lifetime. Multiple studies show that severe or ongoing exposure to highly stressful or threatening events can significantly impact a client’s ability to function in a socially acceptable manner (Haskell & Randell, 2019; King, 2021; National Child Traumatic Stress Network (NCTSN), 2017). Therefore the health care administrator must be informed in the practice of trauma-informed communication. The American Substance Abuse and Mental Health Service Administration (SAMSHA) defines “a program, organization, or system that is trauma-informed as one that: 1) Realizes the widespread impact of trauma and understands potential paths for recovery; 2) Recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system; 3) Responds by fully integrating knowledge about trauma into policies, procedures, and practices; and 4) Seeks to resist re-traumatization actively” (2019).
Example: Adverse Childhood Experiences (ACEs)
Adverse childhood events (ACEs) will impact a person’s health status (Robert Wood Johnson Foundation, 2013). Trauma Warning: loud voices and glass breaking. Be Aware: In this video, the term ‘fag’ is used as British slang for cigarettes.
Why is Utilizing a Trauma-Informed Approach Essential for the Health Care Administrator?
As a professional Health Care Administration, one will work in various settings and encounter very diverse populations. A trauma-informed approach (TIA) addresses vital information about the client’s well-being that considers adverse life experiences and their potential influence on their health care decision-making. A trauma-informed approach is critical to promoting lifelong health and well-being for anyone who has had adverse childhood and adult experiences.
All staff should have initial training on a trauma-informed approach and how to apply trauma-informed principles in every client interaction. The awareness and application of the trauma-informed approach increase trust and reliability in all interactions with clients (OASH, 2021; National Child Trauma Stress Network (NCTSN), 2020). Not all clients will appear as they have experienced past trauma, however, if the HCA develops an awareness of their professional approach it can prevent retraumatizing the client. Retraumatization can occur when a client must explain their story over and over with multiple health care providers or service workers (SAMHSA’s Trauma and Justice Strategic Initiative, 2014).
The HCA helps to avoid re-traumatizing the client can include the HCA reviewing the client’s chart for referral or consultation reports before asking the client questions. Often times the HCA has the information, however, the client must repeat their story. The HCA can use their verbal assessment skills to assess if a client is uncomfortable in a setting and move them to another area. Any sensory can trigger a client to re-experience an event. Consider smells, sights, sounds or touches that may be interpreted as good or bad can take action to change the health care environments. At times the client may cringe when exposed to a particular noise, using the HCA assessment skills of the situation can allow the HCA to be proactive in preventing retraumatizing a client. It may be best to assume that all clients have a past and some may have been trauma-induced.
The goal of the helping interview is to achieve and maintain a trusting relationship with the client.
HCA and other professionals model positive, non-shaming communication to support healing for those in need and promote health and well-being for everyone. The HCA should listen patiently without interruption, pleasantly provide information and answers, and ensure all participants have opportunities to speak and be heard.
HCA’s can provide non-judgmental, warm, empathic, and genuine interactions at all times, including ongoing training to connect with their clientele while maintaining healthy professional boundaries (National Child Trauma Stress Network (NCTSN), 2020).
Building safety, transparency and trustworthiness, peer support, collaboration and mutuality, empowerment, voice and choice, and cultural issues are vital principles for a trauma-informed approach (National Child Trauma Stress Network (NCTSN), 2020). The HCA should recognize that responses to trauma can include dismissing feelings, avoiding things that are reminders of previous traumatic experiences, and increased sensitivity to these reminders, people, and the environment. It may be an opportunity for the HCA to provide information for the clients about trauma and its effects. When possible, offer flexibility and choices as to how a survivor can interact with our programs and staff.
It is essential to take a survivor’s trauma responses seriously (e.g., they may be jumpy or anxious, have a hard time sleeping, or they may need to avoid a neighbourhood that has too many reminders of past experiences). This can be demonstrated by communicating respectfully using appropriate terms and language to build healthy, trusting and professional relationships and be an active listener (OASH, 2021).
Best Practices for Trauma-Informed Communication
Communicate respectfully. The tone of voice can significantly impact how people receive and react to messages.
Be respectful of others’ life experiences. Recognize that someone’s mental health issues, substance abuse or physical health concerns may be rooted in “what has happened to them” and not because “something is wrong with them.”
Build healthy relationships. When interacting with others, treat people with dignity and respect.
Be an active listener.
Focus on behaviours and not the person.
Use appropriate body language.
Creating a Safe environment for all Clients to Communicate Without Fear of Judgement
An emotional safety setting may seem challenging to achieve because it is hard to measure. One definition of emotional safety includes “a feeling that your innermost thoughts, feelings and experience are, and will be, honoured as one honour themselves. You need not prove nor impress; you simply are. When a client feels safe, they feel open, even, at ease, and fluid with the spontaneity of a healthy child.”
The HCA should understand emotional safety. Emotional safety means that one feels accepted; it is the sense that one is safe from emotional attack or harm. Most trauma survivors have probably felt emotionally unsafe or had their sense of “being all right” taken away by others. Many survivors share that the ongoing and unrelenting attacks on their sense of well-being are more painful than a beating (King, 2009). Clients should always feel they are welcome in your health care setting (Washington Coalition of Sexual Assault Programs, 2012).
The health care exposure may help clients manage feelings. Trauma may affect a person’s ability to achieve an emotional balance. Many survivors may experience diverse feelings and worries that make it difficult to make decisions, follow plans, and tend to responsibilities for their health care needs. Thus, HCA can provide clients with a greater sense of control, such as booking appointment times conducive to the client’s schedule. The HCA can activate and engage the client in thinking and planning to gain or lead to a better sense of control. This can also mean providing or offering a caring and calming presence, helping with tasks that appear to be overwhelming, such as completing paperwork or online scheduling of appointments or directions.
When possible the HCA can provide a relaxing place. When providing a calm environment, the message sent to the client is that one cares about their privacy and is interested in attentively listening to how the client feels and their status physically and emotionally. A soothing space may be a quiet corner of a quiet room or a comfortable chair, low lights, a flexible door that can be closed or kept open, a source of quiet music. Alternatively, it could be a room with plants or flowers, videos of beautiful scenery, a radio or CD player, and space for writing. Different things will be soothing at different times and to different types of clients and department settings.
Once again, the HCA can provide information about trauma. Trauma will disrupt a person’s sense of well-being, and it has direct effects on the brain and causes changes in how the person perceives and experiences the world and how they perceive danger (Haskill & Randell, 2019). Learning about trauma triggers can help clients to understand and manage their feelings and increase their sense of control and autonomy.
It is essential for the HCA to provide clear information and avoid surprises. When clients feel emotionally unsafe, they may wonder which people have the power or authority in the health care setting. They may be concerned about what the professionals will do with their information. Providing clear and accurate information about policies, procedures, rules, plans, and activities helps support emotional safety (Schladale, 2013).
The HCA may be able to help trauma survivors feel comforted and in control. Each survivor has a pattern of needs related to emotional safety. For example, one survivor may find it reassuring to have clear directions or information from staff who speak with authority and expertise. For someone else, withdrawing from external stresses to explore their thoughts and feelings will be the jump start they need to plan for their future. An essential aspect of helping survivors feel comforted and in control is ensuring that survivors know they can ask for what they need. Such as asking for tissue, and they may express their opinions and wishes—for example, seeing a particular health care professional or appointment date and time. (OASH, 2021; National Child Trauma Stress Network (NCTSN), 2008).
Understanding Symptoms as Adaptations
In trauma-informed settings, a survivor’s behaviour reflects adaptations to a world that has not always been safe. Instead of trying to fix a client’s behaviour, one needs to understand multiple variables such as brain chemistry, genetic tendencies, and life experience as well as the person’s access to resources) affect how the world looks to them, what feels safe, what they think may happen, and how they ask for and use healthcare services (National Center on Domestic Violence, Trauma & Mental Health, 2011). If survivors have a mental illness, they know that they neither have to hide it nor disclose it to get the help they are seeking.
Of course, this does not mean that the HCA will not have reactions if a person’s behaviour is troublesome, disrespectful, or dangerous. It does mean that the way the HCA communicates their reactions should not shame or embarrass the client. Saying, “We want everyone to be safe and comfortable here. You have been shouting for a while, and that worries some of us,” is better than saying, “You cannot keep making all that noise; you need to sit down and please be quiet.” (National Center on Domestic Violence, Trauma & Mental Health, 2011). Both statements let the client know that people are reacting to their behaviour, but be respectful and acknowledge that the survivor is doing the best they can (Haskell & Randall, 2019).
The Impact of Trauma on LGBTQ2S+ Youth
The following video introduces the HCA to the needs of lesbian, gay, bisexual, transgender, queer, questioning, two-spirited, and other (LGBTQ2S+) youth who have experienced trauma. This video discusses creating safe, welcoming and inclusive environments for youth who have experienced trauma and identify as LGBTQ2S+.
What can the HCA do? By using focused eye contact and engaging body language can create open non-threatening communication. The HCA can ask open-ended questions to answer the who, what, when, where and how of discussed topics. When the client speaks, avoid interruptions, judgment and do not try to fix things. Also, remember to focus on behaviours and not the person. (National Child Trauma Stress Network (NCTSN), 2008; National Child Trauma Stress Network (NCTSN), 2020; Family Violence Prevention Fund, 2004).
Table 11.1. Trauma-Informed Communication: Do and Do Not
Do
Do Not
Speak with a normal, controlled voice
Shout or lose control of one’s emotions.
Invoke a sense of calm
Express kindness, patience and acceptance.
Use your phone: remain present with the client.
Use engaging eye contact and positive body language.
Interrupt, judge, or try to fix things.
Ask open-ended questions that answer the who, what, when, where and how of topics being discussed.
Use confrontational body language, such as putting hands on your hips, crossing your arms, getting too close to others or backing them into a corner. This can cause already stressful situations to escalate
Respect personal space
Use physical touching.
Considerations
When using trauma-informed communication, the HCA should be aware:
trauma can happen to anyone
the response to trauma is very individual
consider that all clients have life experience or history, thus may have differing triggers
assess each client and modify your communication to the client’s need
Developed the understanding of a trauma-informed approach to communication.
Developed a trauma-informed approach in the health care settings.
Developed an awareness of the client’s reactions or behaviours that may be related to past trauma.
Created safe and less traumatic environments for clients who may have experienced trauma.
Key Terms:
Active listener: The act of listening carefully.
Adaptations: The act of changing to fit in.
Adverse Effects: Something that can go wrong during a treatment that can affect an individual for the rest of their life.
Attentively: The act of being observant.
Authority: The power an individual has to give orders and make rules.
Autonomy: An individual acting differently and separating from others (Merriam Webster, n.d).
Circumstances: Something happening where nobody has control of it.
Clientele: Customers/clients.
Conducive: The act of being more flexible for a client.
Disrespectful: The act of being rude and going against the rules.
Emotional Safety: A feeling that your innermost thoughts, feelings, and experiences are, and will be, honoured as one honours themselves.
Empathic: The act of being understanding.
Environment: The place you are surrounded by.
Event: Something happening.
Genuine: The act of being real, truthful and sincere.
Helping Interview: An interview with a person seeking help and the people providing that help.
Interactions: The involvement with another individual.
Judgment: To make considered decisions or come to conclusions about another based on past experience, stereotyping or prejudice.
Multigenerational: Being related to multiple generations.
Perceive: The act of being aware of something.
Reaction: A response to words and actions.
Severe: Very bad/ serious.
Shame: A feeling of humiliation.
Spontaneity: The state of being spontaneous (Merriam Webster, n.d).
Survivor: To continue to function after a traumatic experience.
Tendencies: An individual’s thoughts and actions. (Marriam-Webster, n.d.)
Trauma: Pertains to a deeply distressing or disturbing experience. A psychological or physical injury (Merriam Webster, n.d).
Trauma-informed: The act of recognizing trauma within individuals.
Traumatic: The act of being emotionally stressed to the point where it can affect an individual mentally and emotionally.
Triggers: Something that causes an individual to have trauma.
Troublesome: Being difficult.
Well-being: Being happy and healthy (Merriam Webster, n.d).
References
Center for Health Care Strategies. (2019, January 23). What is trauma-informed care? [Video]. YouTube. https://youtu.be/fWken5DsJcw
City of San Diego. (n.d.). Trauma informed resources. Commission on Gang Prevention and Intervention. https://www.sandiego.gov/gangcommission/directory/trauma
National Child Trauma Stress Network (NCTSN). (2020). Child welfare trauma training toolkit: Supplemental handouts questions for mental health providers. https://www.nctsn.org/print/1145
National Child Traumatic Stress Network (NCTSN). (2017, July 17). Safe spaces, safe places: Creating welcoming and inclusive environments for traumatized LGBTQ youth [Video]. YouTube. https://www.youtube.com/watch?v=8zNbQ_8KRew
OASH. (2021). Meaningful youth engagement. Office of Population Affairs. https://opa.hhs.gov/adolescent-health/positive-youth-development/meaningful-youth-engagement
Substance Abuse and Mental Health Administration (SAMHSA). (2019, August 2). Trauma and violence. U.S. Department of Health & Human Services. https://www.samhsa.gov/trauma-violence
Have you ever been in an uncomfortable situation where you continued to ponder the exchange or incident? Did you: (Select all that apply)
Create other resolutions to the incident
Think about the incident for the day
Think about the incident before falling asleep
Discuss the incident with others more than once
The correct response is option one, two, three and four. Remember we can all respond is differing ways when pondering an uncomfortable situation. What one feels is not wrong.
Question 2
Have you ever been exposed to something where it reminded you of a past experience?
Such as a smell that reminded you of a place or person. The response to the scent may create a trigger, good or bad, and is very individual to their individual experience. How do you feel when you smell pizza? (select all that apply)
it reminds me of my friends
it makes me feel happy
it makes me feel hungry
it reminds me of my family
it makes my stomach feel upset
It makes my mouth water
The correct response is all of the above. Often smells will remind us of something. How we feel or interpret the feeling will differ between individuals. How one feels is not wrong. Return to Activity
Explore professional accountability influencing the role of the Health Care Administrator.
Recognize the importance of professional boundaries in the therapeutic relationship.
Explain legal matters within the context of health care and communications.
Explore the link between patient/client safety and effective communication.
Introduction
Health professionals know the importance of quality care and the delivery of health services provided. For many health professionals, their scope of practice is regulated through governing bodies who apply legislation (law) to ensure protection in the interest of the public. For example, the Regulated Health Professions Act, 1991, S.O. 1991, c. 18 in Ontario outlines the regulations which the governing bodies implement. Governing bodies are often referred to as colleges, such as the College of Physicians and Surgeons (CPSO) and the College of Nurses. Health Care Administrators (HCAs) have the duty and responsibility to protect health information and support client safety.
Providers of health services recognize how services are regulated and ensure protocols and procedures are in place to comply with standards of care. Legal issues arising in the health care environment can often be attributed to poor communication management leading to undesirable outcomes. Client-centred therapeutic communications provide for shared decision making, understanding of common goals, and supports the engagement of the patient and their families. This chapter will focus on legal matters relevant to the health care environment and considerations involving the role of the HCA.
Every client has the right to anticipate and expect information obtained and discussed within the health care environment will be kept confidential by all members of the health care team. Sensitive information is often exchanged in the therapeutic relationship. Unauthorized individuals should not have access to the appointment schedule, patient personal health information (PHI), and related information. The role of the HCA encompasses a custodian like approach to guard information and protect data. To take it an additional step forward consider again the importance of trust in the therapeutic relationship. A client will trust the HCA will keep their PHI safe.
Personal Information Protection and Electronic Documents Act (PIPEDA) and Privacy Act
According to the Office of the Privacy Commissioner of Canada (2018), personal information is data about an “identifiable individual”. It is information that can identify you as an individual on its own or combined with other pieces of data. PIPEDA largely encompasses how businesses handle personal information. Several provinces in Canada have their own privacy laws as they relate to health care which is substantially aligned with PIPEDA, while other provinces and territories have privacy acts not considered directly aligned with PIPEDA.
Circle of Care Model
The “circle of care” is considered the group of healthcare providers treating a patient who share information to provide that care. The concept of the circle of care allows the sharing of patients’ health information between healthcare providers who are providing care to that patient, without seeking the patient’s express consent every time information needs to be exchanged. This allows for the provision of clinical information to colleagues when consulted (Canadian Medical Protective Association, 2021).
The circle of care model extends to include sharing information, consent, information sharing with the family, leaving information on voice mail, and third party requests for information. The HCA should be mindful to operate within the circle of care model throughout the therapeutic relationship, involving others outside the circle of care is considered a direct violation of this care model and can be considered a privacy breach of information as discussed further. Consider a privacy breach as a breaking of the trust assigned to members within the health care environment.
Health Privacy Breach
A privacy breach occurs when PHI is collected, used or disclosed without authorization. Examples of this include, loss, theft or unauthorized copying, modification or disposal (Information and Privacy Commissioner of Ontario, 2018). Strategies helping to prevent a breach can include:
Protect documents and files
Return files as soon as possible to their storage system
Care conferences should be held in quiet locations away from others not involved in the client care
Develop a response mechanism to address any data loss if it occurs
Information Breach Situations to Consider
Review the following:
Employed in a primary care physician’s office and the patient paper file goes missing.
New HCA working in a hospital setting writes down their passcode on paper for accessing Patient Health Information (PHI) systems and someone reads this information and uses it to access or hack electronic patient files.
Leaving sensitive information about clients available to be read or seen by those outside of the circle of care.
Reflective questions:
What is the common element in the situations explored here?
Are these direct legal violations if so, in what ways?
Most health care providers are regulated under the Regulated Health Professions Act (RHPA) and the Medicine Act, 1991 (Ontario Government). Health care administrators (HCAs) are not regulated professionals and follow the policy and procedures set by the regulated health care provider for which they work. HCAs may be assigned tasks that do not involve controlled acts.. It is important that HCAs are aware of their scope of practice and if there is doubt regarding the performance of a task or expression of behaviours, then the HCA should check with their immediate supervisor or the health care provider for which they work. You may be wondering how this applies to communicating therapeutically? Let’s review these examples:
The use of therapeutic communication in the context of providing a client with psychological therapy treatment would fall outside of HCA scope of practice and should be left to the health care provider.
Actively listening to and acknowledging the stress a client is experiencing, while they express the impact that caring for their father (who suffers from Alzheimer’s disease) is on their daily life, may fall within the scope of the HCA. The caveat is that the observations made are shared with the health care provider for further assessment.
Professional Intimacy and Boundaries of Therapeutic Relationships
When a patient discloses their personal information to a HCA or others members of the health care team this is an example of professional intimacy. As a HCA professional intimacy is an inherent element of the therapeutic relationship. Professional boundaries are essential in identifying parameters of the therapeutic relationship. Maintaining professional boundaries is an expectation regardless of a patient’s actions or requests. Remember, a HCA is accountable for setting the boundaries of the therapeutic relationship.
At times, the temptation to cross professional boundaries may arise, these could include revealing personal information about yourself, calling a patient at home with the intention of establishing a personal relationship, or failure to disclose your professional status.
Boundary violations occur when the patient’s/clients needs are no longer the focus. Think of this as the reversal of roles.
The following list is examples of unacceptable behaviours in a therapeutic relationship:
Examples of Boundary Crossing Actions
Review this list and consider the impact these actions have on the therapeutic relationship:
Oversharing your personal information as an HCA with clients and families.
Volunteering to complete tasks outside of your role such as running a personal errand for a client.
Seeking support from a client or patient as a reversal of role.
Involving yourself in a client’s personal affairs such as buying and selling items with clients.
Policies and Protocols
In most environments within the health care, various policies dictate the overarching manner in which health care is accessed and delivered. An example of health policy in Canada is the Canada Health Act provides universal health insurance coverage funded at the federal, provincial, and territory levels. The Canada Health Act (policy) defines medical services with a goal to sustain health, prevent illness, and methods for diagnosing and treatments available. Many facilities and settings set policies in place to support quality patient outcomes. An HCA should be informed of the organizational policies governing their actions to ensure compliance and alignment.
Protocols in health care are described as a set of instructions or guidelines to follow surrounding client care. Clinical protocols reflect the appropriate level of care provided based on a set of health findings. An example could be a clinical trial of a new medication in development to treat a specific illness or condition. Using therapeutic communications in a clinical setting is an example of following a protocol to support client care and outcome.
Client Safety
Client safety refers to taking the steps necessary to prevent client harm during the process of accessing health care and services. To ensure a caring and just culture is established at all levels of the Canadian healthcare system (Canadian Patient Safety Institute, 2019). These guiding principles form an element within the policy framework presented by the Canadian Patient Safety Institute (CPSI) and developed as a strategic initiative to secure safe patient practices. Every member of the health care team has an obligation to practice in a safe manner to support patient safety. Figure 12.1 details the full framework for patient safety as developed by the CPSI with a goal for Canada to create the safest in the world.
Figure 12.1. Policy Framework for Patient Safety in Canada. From Canadian Safety Institute, 2019. [Image Description]
Ensuring client safety falls to all members of the health care team. When the HCA communicates in a therapeutic manner the client feels at ease. This openness creates trust and supports a client-centred safe space. When using therapeutic communication techniques in a goal-oriented manner the focus remains on client health care needs. Listening to understand supports the decision-making process of the client thereby increasing the safety of the client.
Explored relevant legal matters within the context of health care.
Reviewed the role of the HCA in connection to operating within their scope of practice following the policies and procedures set out.
Recognized the importance of establishing professional boundaries while communicating in a therapeutic manner was emphasized throughout the chapter content.
Explored the link between patient safety and effective communication.
Key Terms
Alignment: The state of being agreed and matched with something or someone (Merriam-Webster, n.d)
Boundaries: A limit of activity.
Breach: Break, violate (Merriam-Webster, n.d).
Caveat: A caution, warning, qualification, or forewarning.
Circle of Care:: The group of healthcare providers treating a patient who share information to provide that care.
Compliance: The act of fulfilling requirements (Merriam-Webster, n.d).
Custodian: A person who has a responsibility.
Disclosed: To expose or make public (Merriam-Webster, n.d).
Governing: Having the authority to conduct the policy.
Inherent: Existing as something of an essential characteristic.
Intimacy: Close familiarity.
PHI: Personal health information.
Standards of care: A duty determined by a set of circumstances relevant to a particular patient at a given time.
Figure 12.1: This image details the policy framework for patient safety in Canada using intersecting circles to show the components involved in the initiative. Permission is granted to redistribute this document, in whole or part, for educational, non-commercial purposes providing that the content is not altered and that the Canadian Patient Safety Institute is appropriately credited for the work. [Return To Image]
Assessing What You Already Know (Text-based Activity)
Question 1
Recall the video at the start of this chapter. Consider the exchange between the HCA and the patient. How could we view the response by the HCA? Select all responses that apply:
Offering medical advice
Nothing, this exchange is fine
Crossing professional boundaries
Oversharing
Solution. The correct response is option three and option four. This is an example of crossing professional boundaries by using personal experience to answer a question the client asked. Explore this chapter further to read about professional boundaries. Oversharing is providing information based on a personal experience can be viewed as an oversharing. The HCA mentioned a personal relationship in the response.
Question 2
Two Health Care Administrators are talking about a client’s health history near a patient waiting room. How would you perceive this? Select which apply:
Data breech of patient information
Normal practice when teams are working together
This sharing of information may assist with patient care
The correct response is option one. Others could overhear identifying data about the client and therefore confidential information could be released resulting in a data breech. Return to Activity
Check Your Understanding (Text-based Activity)
Question 1
Examples of PHI breach are? (more then one may be correct)
Loss
Theft
Disposal.
For filing purposes.
Patient requested a copy
The correct response includes options one, two and three. Privacy breaches can occur when the personal health information is lost, stolen or disposed of incorrectly.
Question 3
Maintaining professional boundaries is for the HCA to set
True
False
The correct response is option one, true. The HCA should be very aware of their professional boundaries. Return to Activity
Glossary
1
Appendix
2
This is where you can add appendices or other back matter.


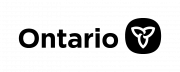
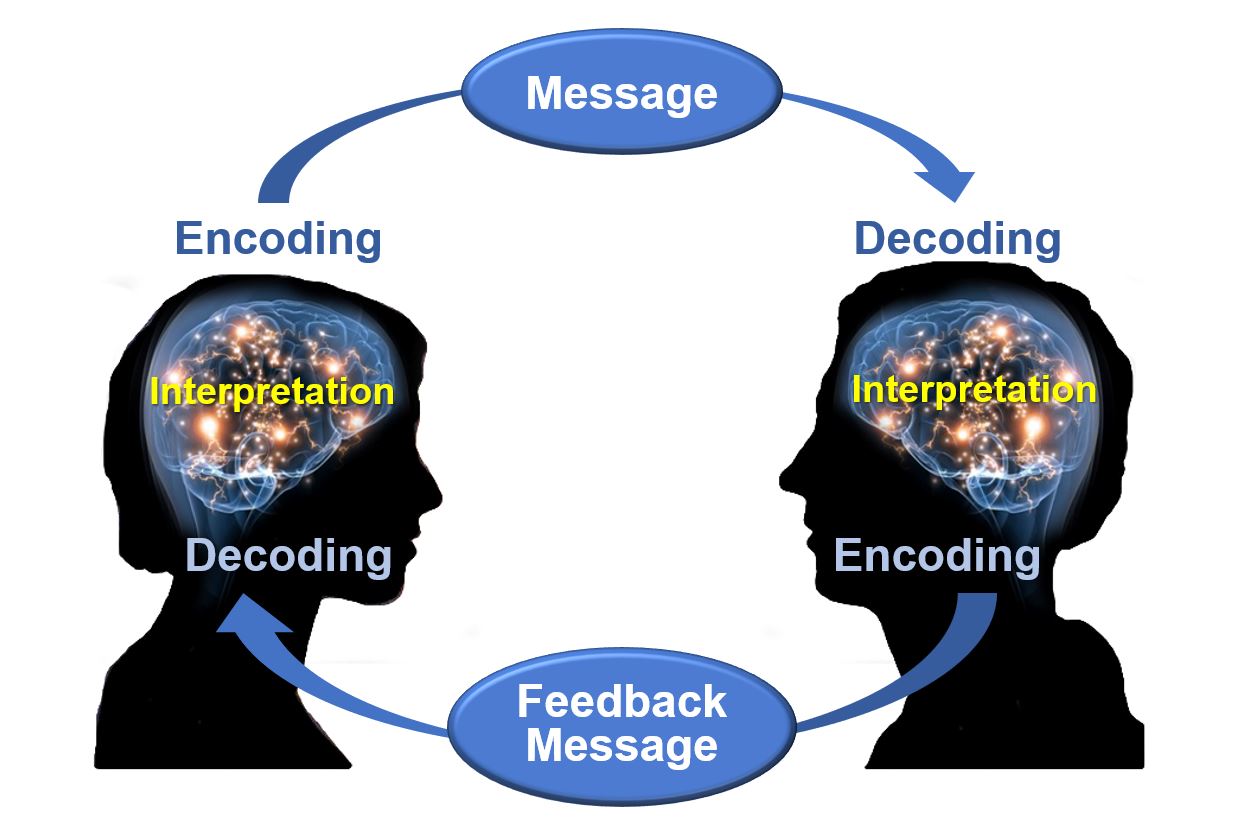

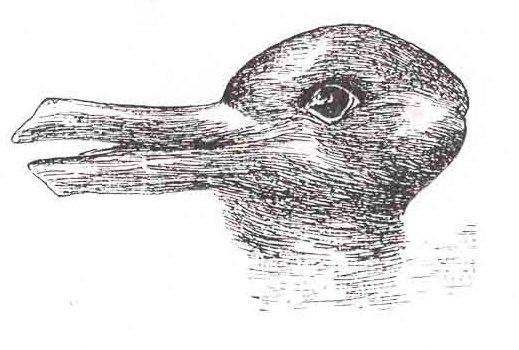




{kind=link}