This textbook is designed for the novice learner who is seeking to develop a foundational understanding of the complete subjective health assessment in the context of health and illness. The textbook deconstructs the categories of the complete subjective health assessment, providing learners with explanations and examples of what constitutes relevant subjective data. This textbook provides an opportunity to learn how to respond to normal, abnormal, and critical findings when completing a complete subjective health assessment.
Learning Outcomes and Legend
This textbook is best viewed online in the “Read Book” format available through Pressbooks. The Read Book format enables all Accessible multimedia content. Users can also download a PDF or request a print copy through eCampusOntario’s Open Library.
Learning Outcomes
Learning Outcomes
By the end of this book, you will:
Describe the categories of a complete subjective health assessment.
Explain the relevance for conducting a complete subjective health assessment across the lifespan.
Formulate questions based on categories of a complete subjective health assessment.
Recognize the sequence of subjective data collection.
Appraise normal, abnormal, and critical subjective findings.
Legend
Throughout this text you will encounter various learning–teaching strategies. Here is a short summary:
Textual information describes the content.
Points of Consideration provide additional information to push your thinking beyond the main point to consider in practice. Points of consideration are visually separated from the rest of the textual information using a text box.
Findings that require intervention, highlighted as take action, such as abnormal or critical findings or findings that require health promotion.
Activities give you an opportunity to evaluate your learning.
Videos and podcasts help you understand the information in a different way.
Important phrases are bolded.
Unfamiliar and complex terms are bolded and included in the glossary at the end of the book. If reading the book online, hover your cursor over a bolded word to reveal the definition.
About eCampusOntario and Authors
About eCampusOntario
eCampusOntario is a not-for-profit corporation funded by the Government of Ontario. It serves as a centre of excellence in online and technology-enabled learning for all publicly funded colleges and universities in Ontario and has embarked on a bold mission to widen access to post-secondary education and training in Ontario. This textbook is part of eCampusOntario’s Open Library, which provides free learning resources in a wide range of subject areas. These open resources can be assigned by instructors for their classes, downloaded by learners to electronic devices or printed through the University of Waterloo print on demand service. These free and open resources are customizable to meet a wide range of learning needs, and we invite instructors to review and adopt the resources for use in their courses.
About the Authors
Jennifer L. Lapum, RN, BScN, MN, PhD, Professor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, ON, Canada
Oona St-Amant, RN, BScN, MScN, PhD, Assistant Professor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, ON, Canada
Michelle Hughes, RN, BScN, MEd, Professor, Centennial College, School of Community and Health Studies, Toronto, ON, Canada
Paul Petrie, RN, BScN, MScN, Professor, George Brown College, Sally Horsfall Eaton School of Nursing, Toronto, ON, Canada
Sherry Morrell, RN(EC), BScN, MN, PhD(c), Lecturer, Faculty of Nursing, University of Windsor, Nurse Practitioner, Windsor Regional Hospital, Windsor, ON, Canada
Sita Mistry, RM, BHScM, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
For more information:
Dr. Jennifer L. Lapum
Ryerson University
jlapum@ryerson.ca
415-979-5000 ex. 6316
350 Victoria St.
Toronto, ON M5B 2K3
Note to Teachers Using This Resource
We encourage you to use this resource and would love to hear if you have integrated it into your curriculum. Please consider notifying Dr. Lapum if you are using it in your course, identifying the healthcare discipline and the number of students. Please help us support future OER efforts by reporting your adoption of this resource at https://openlibrary.ecampusontario.ca/report-an-adoption/
Acknowledgments
Multimedia Consultant
Neal MacInnes, BA, MA, Academic Information and Communication Technology Supervisor, Lawrence S. Bloomberg Faculty of Nursing, University of Toronto, Toronto, ON, Canada
Medical Artist
Hang Yu Lin, BSc., Master of Science in Biomedical Communications student, University of Toronto University of Toronto, Toronto, ON, Canada
Video Editing and Support
Jing Cai Han, BTech, Video editor, Office of eLearning, Ryerson University, Toronto, ON, Canada
eCampusOntario team
Lindsay Woodside, HBA, OCT, MA, Program Manager, Nursing OER, eCampusOntario
Lena Patterson, BA, MA, Senior Director, Programs and Stakeholder, eCampusOntario
Emily Carlisle, BA, MLIS, Editorial Lead, Open at Scale, eCampusOntario
Film Clip Appearances
Siobhan Doyle, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Toronto, ON, Canada
Michelle Hughes, RN, BScN, MEd, Professor, Centennial College, School of Community and Health Studies, Toronto, ON, Canada
Jennifer L. Lapum, RN, BScN, MN, PhD, Professor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, ON, Canada
Sita Mistry, RM, BHScM, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Sherry Morrell, RN(EC), BScN, MN, PhD(c), Lecturer, Faculty of Nursing, University of Windsor, Nurse Practitioner, Windsor Regional Hospital, Windsor, ON, Canada
Paul Petrie, RN, BScN, MScN, Professor, George Brown College, Sally Horsfall Eaton School of Nursing, Toronto, ON, Canada
Oona St-Amant, RN, BScN, MScN, PhD, Assistant Professor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, ON, Canada
License
This textbook is licensed under a Creative Commons Attribution-ShareAlike 4.0 International (CC BY-SA) license, which means that you are free to:
SHARE – copy and redistribute the material in any medium or format.
ADAPT – remix, transform, and build upon the material for any purpose, even commercially.
The licensor cannot revoke these freedoms as long as you follow the following license terms:
Attribution: You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use. ShareAlike: If you remix, transform, or build upon the material, you must distribute your contributions under the same license as the original. No additional restrictions: You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits. Notice: You do not have to comply with the license for elements of the material in the public domain or where your use is permitted by an applicable exception or limitation. No warranties are given: The license may not give you all of the permissions necessary for your intended use. For example, other rights such as publicity, privacy, or moral rights may limit how you use the material.
Chapter 1: Introduction to the Complete Subjective Health Assessment
II
The Complete Subjective Health Assessment
The complete subjective health assessment is commonly referred to as a health history. It provides an overview of the client’s current and past health and illness state. You conduct it by interviewing the client as illustrated in Figure 1.1, asking them questions, and listening to their narrative.
Figure 1.1: Nurse interviewing the client
This information is often shared verbally with you or in the way that the client can best communicate. It is also sometimes collected through a standardized form that the client completes. In some cases, it also includes information shared by a family member, friend, or another health professional when the client is unable to communicate.
Points of Consideration
Clients are sometimes accompanied by care partners. Care partners are family and friends who are involved in helping to care for the client. You may hear care partners being referred to as “informal caregivers” or “family caregivers,” but “care partner” is a more inclusive term that acknowledges the energy, work, and importance of their role.
The complete subjective health assessment is part of assessment, the first component of the nursing process (assessment, analysis/diagnosis, planning, implementation and evaluation) outlined in Figure 1.2.
Figure 1.2: The nursing process
As illustrated in Figure 1.2, the assessment phase of the nursing process involves collecting subjective data (information that the client shares) and objective data (information that you collect when performing a physical exam). See Table 1.1 for an overview and examples of subjective and objective data. This book focuses on subjective data collection in the context of the complete subjective health assessment.
Data
Example
Subjective
Information that the client shares with you spontaneously or in response to your questions.
The client states, “I have had a rash on my ankle and leg for the last two weeks.”
The parent states, “My eight-month-old son is having trouble breathing.”
The client’s reason for seeking care is “diarrhea for 10 days.”
The client types, “I feel sick to my stomach.”
Objective
Information that you observe when conducting a physical assessment, and lab and diagnostic results.
You observe that a client has a bright red rash on the dorsal side of the foot, the lateral malleolus, and anterior and lateral side of the lower leg.
You observe the client sitting upright, leaning forward, breathing fast with eyes wide open.
You take the client’s blood pressure and report it as 112/84 mm Hg and pulse at 84 beats per minute.
Lab test results: K+ 4.0 mmol/L, fasting glucose 4.8 mmol/L.
Chest X-ray report: Lungs well inflated and clear. No evidence of pneumonia or pulmonary edema.
Table 1.1: Overview and examples of subjective and objective data
As the word “subjective” suggests, this type of data refers to information that is spontaneously shared with you by the client or is in response to questions that you ask the client. Subjective data can include information about both symptoms and signs. In the context of subjective data, symptoms are something that the client feels, as illustrated in Figure 1.3 (e.g., nausea, pain, fatigue). You won’t know about a symptom unless the client tells you. Signs are something that the health professional can observe, such as a rash, bruising, or skin perspiration, also illustrated in Figure 1.3. Although you can observe signs, in the context of a subjective assessment, the client shares this subjective information with you. For example, a rash is both subjective and objective data as it could be something that the client shares with you, but it is also something that you can observe. On the other hand, if the client says that the rash is itchy, that would be considered subjective data and, in this case, it would be a symptom because it is something the client feels and you can’t observe.
Reasons for Conducting a Complete Subjective Health Assessment
The aims of the nursing process are to identify main health and illness concerns, determine the underlying issues/etiology, collaborate with the client to address and resolve these concerns and issues, and engage in health promotion. To meet these aims, you engage in a process of diagnostic reasoning by critically exploring and analyzing both subjective and objective data to identify the health needs of the client. The complete subjective health assessment is an important component of this process as it allows insight into the client’s state of health and illness. Depending on the context and the client’s main health needs, the complete subjective health assessment may occupy the bulk of your time with the client.
You should conduct a complete subjective health assessment when a comprehensive overview of the client’s health and illness is needed. For example, you may conduct a complete subjective health assessment when a client moves into a long-term care institution, and depending on the institution, this may be repeated monthly. This assessment is also conducted when a client is admitted to a hospital, and a shortened version of it is often completed at the start of each shift. However, how frequent and how comprehensive the assessment is depends on the client’s needs, the situation, and the institution’s policies.
More focused assessments are required when collecting specific subjective data based on the health issues and/or need to clarify or follow up on previous information provided. Situations that warrant a focused assessment as opposed to a complete subjective health assessment include:
An emergency (i.e., a situation with imminent catastrophic risk if untreated). In this case, you focus on collecting data that is vital to stabilizing a life-threatening illness; it may be specific to airway, breathing, and circulation. An example is a client who arrives at the emergency department reporting “crushing chest pain.” In this case, a focused assessment is conducted that attends to the reason for seeking care and may focus on questions about the cardiac and respiratory system.
A continual in-hospital assessment. In this case, you assess a client several times throughout your shift. The assessment focuses on the client’s current main health issues and following up on health issues that were previously addressed.
Primary care assessment. In this case, you focus your assessment on an emergent issue that has arisen for a client (e.g., a rash, pain in their knee, a fever). However, some primary assessments require a complete subjective health assessment particularly if this is a client you are meeting for the first time or they have a complex health issue.
Categories of the complete subjective health assessment (as illustrated in Figure 1.4) vary depending on the framework you follow, but generally include:
Introductory information: Demographic and biographic data.
Main health needs (reasons for seeking care).
Current and past health.
Mental health and mental illnesses.
Functional health.
Preventive treatments and examinations.
Family health.
Cultural health.
Figure 1.4: Categories of the Subjective Health Assessment
You begin the assessment by collecting information about demographic and biographic data and then, main health needs. Afterwards, there is no specific order in which these categories must be assessed. Often it depends on the client’s main health needs or reasons for seeking care. Sometimes it depends on the natural flow of conversation that occurs with the client. Usually, you assess sections that involve sensitive questions as well as cultural health towards the end when you have had the opportunity to develop a level of trust with the client.
In addition to these categories, you may incorporate subjective questions specific to each of the body’s systems; this phase is called a Review of the Systems. These questions give you insight into each body system (e.g., skin, eyes, cardiovascular, musculoskeletal). Depending on the client’s response and the reporting of cues that prompt your concern, you may probe further with more specific questions. In other readings, you will learn about subjective questions related to each body system.
Clinical Tip
Always ask one question at a time.
Influencing Factors
Influencing factors constitute common situational issues that can arise during a subjective data assessment. Always consider factors that may influence how you ask questions and the validity and reliability of the subjective data collected. These situational factors can be difficult to both assess and address in certain cases (see Table 1.2).
Factors
Strategies
Clients may be hyperaware of the situation and wonder why you are asking certain questions.
Begin by sharing with the client why you are asking these types of questions.
Encourage the client to ask you questions if they are uncertain about why certain information is being sought.
Normalize sensitive questions by stating: “I ask all clients about X so that I can better understand the context of their health and illness.”
Clients may downplay or exaggerate what they tell you.
Seek clarification.
Reframe the questions you ask.
Paraphrase what the client says and ask if you have captured their meaning correctly.
Clients may withhold information because they fear sharing information, feel judged by sharing certain information, and/or have a condition that is often stigmatized.
Emphasize confidentiality.
Introduce sensitive questions later in the interview once you have established a therapeutic and trusting relationship.
Clients may not be fully conscious or oriented due to a physical injury, a mental health condition, a traumatic event, or substance use.
It is important to be patient and give clients time to think and respond to your questions.
You may need to delay asking some questions until the client begins recovering.
If appropriate, ask other people who can share information about the client to corroborate it.
Note: With a client who is under the influence of a substance, it is important to avoid prejudice, remain nonjudgmental, treat them with respect, speak slowly and clearly with simple language, provide a safe environment for them, and continue to monitor while observing changes in behaviour and level of consciousness.
Clients may function at a developmental age (as opposed to actual age). Developmental age is the age that a client functions at on a cognitive, physical, emotional, and social level. You need to consider this factor with all ages across the lifespan.
Tailor your language and tone of voice to the client’s developmental age.
Always use a respectful and professional tone.
Create space for others to be involved and/or invite a care partner to be present.
Table 1.2: Influencing factors and strategies
Points of Consideration
It is important to document who provides the subjective data. Usually, subjective data is provided by the client (primary source), but in some situations it may be collected from the client’s chart, family members, friends, co-workers, care partners, or interpreters
(secondary sources). In certain cases, the client may be unable to speak or share information, or may speak a different language than you, or be unconscious. Additionally, a care partner (such as a family member) may need to provide subjective data for a newborn or a client with developmental, cognitive, or mental health states that prohibit them from speaking.
What type of data do you collect when completing a complete subjective health assessment?
How do you differentiate symptoms from signs?
When should you conduct a complete subjective health assessment?
What strategies should you use to address influencing factors of common situational issues that can arise during a complete subjective data assessment?
Chapter 2: The Complete Subjective Health Assessment
III
Introductory Information: Demographic and Biographic Data
“Introductory information” refers to the demographic and biographic data that you collect from the client. This data provides you with basic characteristics about the client, such as their name, contact information, birthdate and age, gender and preferred pronouns, allergies, languages spoken and preferred language, relationship status, occupation, and resuscitation status.
Although this data is brief and succinct, the intent of collecting it is not to be reductionist or to label clients. Rather, it is meant as a brief overview of the client and to provide the information you need to reach next of kin in an emergency, to be attentive to allergies at a glance, and to tend to the client in a caring manner. See Film Clip 2.1 of a nurse conducting an assessment of a client’s demographic and biographic data. See Table 2.1 for suggested questions and statements you can use to collect this data in an inclusive and caring manner, as well as an example of a demographic and biographic form below.
Film Clip 2.1: Nurse assessing demographic and biographic data
Data
Questions and Statements
Name/contact information and emergency information
What is your full name?
What name do you prefer to be called by?
What is your address?
What is your phone number?
Who can we contact in an emergency? What is their relationship to you? What number can we reach them at?
Birthdate and age
What is your birthdate?
What is your age?
Gender
Tell me what gender you identify with.
What are your preferred pronouns? (If the person asks you to use a pronoun that you are not familiar with, it is okay for you to respectfully respond, “I am not familiar with that pronoun. Can you tell me more about it?”)
Allergies
Do you have any allergies?
If so, what are you allergic to?
How do you react to the allergy
What do you do to prevent or treat the allergy?
Note: You may need to prompt for information on medications, foods, etc.
Languages spoken and preferred language
What languages do you speak?
What language do you prefer to communicate in (verbally and written)?
Note: You may need to inquire and document if the client requires an interpreter.
Relationship status
Tell me about your relationship status.
Note: Avoid questions such as “Are you married?” or “Do you have boyfriend?” or “Do you have a wife?” as they assume normative behaviour and heterosexuality.
Occupation/school status
What is your occupation? Where do you work?
Do you go to school?
Note: Reassure the client that this information provides insight into the nature of their work (e.g., the physical or mental impact) and environmental exposures, and that the question is not intended to evaluate the client.
Resuscitation status
We ask all clients about their resuscitation status, which refers to medical interventions that are used or not used in the case of an emergency (such as if your heart or breathing stops). You may need more time to think about this, and you may want to speak with someone you trust like a family member or friend. You should also know that you can change your mind. At this point, if any of this happens, would you like us to intervene?
Note: Depending on the client’s answer, you will need to collaborate with the broader healthcare team, explore the details of the client’s wishes further, and have them complete a requisite resuscitation form.
Table 2.1: Introductory information: Collecting demographic and biographic data
Demographic Information Form (Example)
Clicking the hyperlinked question mark (?) next to the example form fields will take you to some suggested questions to ask your patient.
The client’s main health needs are referred to in a variety of ways depending on the environment or institution that you work in. At first point of contact, “main health needs” are often referred to as “reasons for seeking care” or “chief concerns or issues.” In an institution where the client is already admitted, “main health needs” is more commonly used.
Whichever term is used, it recognizes that clients are complex beings, with potentially multiple co-existing health needs, and often there is a pressing issue that requires most immediate care. This is not to suggest that other issues be ignored, but rather it allows providers, clients, and care partners to stay focused.
Most often, providers will document in the client’s own words what the main health needs are. Table 2.2 offers example questions to ask to determine a client’s main health needs in different scenarios, along with sample responses.
Clinical Tip
It is important to avoid asking questions that begin with “why,” which may suggest to the client that they did something wrong or that they are to blame for what is happening to them.
Client
Assessment
Sample Responses
Presenting to a clinic or a hospital emergency or urgent care (first point of contact).
Tell me about what brought you here today.
Probes
Tell me more.
How is that affecting you?
“I have a rash”
“I have been feeling quite depressed lately”
“I’m having pain”
Already admitted, and you are starting your shift.
Tell me about your main health concerns today.
Probes
Tell me more.
How is that affecting you?
“When will I be discharged?”
“I’m really hungry, can I eat something today?”
Table 2.2: Determining main health needs (reasons for seeking care)
Take Action
As a health professional, you need to identify whether a client’s symptomology is considered: normal; abnormal and requiring intervention; or a critical finding that requires prompt intervention. Your subjective data assessment may be cut short if critical findings arise that require immediate intervention. In such a case, you focus on the critical finding and resume the complete subjective health assessment later, when appropriate. Some findings, even though normal, will require health promotion interventions.
Examples of subjective data that are identified as critical findings include but are not limited to:
Chest pain.
Severe difficulty breathing.
Sudden change in vision or ability to speak.
Sudden weakness or paralysis in a limb.
Uncontrollable bleeding.
Post-operative pain or vomiting not relieved by medication.
Suicidal or homicidal ideation with a plan.
Points of Consideration
“Door-handle conversations” describe the situation of a client sharing something with a health professional just as they are about to leave the room (their hand is on the door handle as illustrated in Figure 2.1). Often it is at the last minute when clients gather the courage to speak about a health issue that they are embarrassed or feel shameful about. It may be about something that is stigmatized, or they feel they may be judged on. In these cases, it is important to make time for the client and listen in a non-judgmental manner.
There are many tools to help you further explore a client’s symptoms or signs. A common one follows the mnemonic PQRSTU as illustrated in Figure 2.2, which offers a systematic approach to asking assessment questions without leaving out any details.
Figure 2.2: The PQRSTU assessment mnemonic
The mnemonic is often used to assess pain, but it can also be used to assess many signs and symptoms related to the client’s main health needs, and other signs and symptoms that are discussed during the complete subjective health assessment. Table 2.3 lists examples of prompting questions using this mnemonic.
PQRSTU
Questions Related to Pain
Questions Related to Other Symptoms
Provocative
What makes your pain worse?
What makes your breathing worse?
Palliative
What makes your pain feel better?
What makes your nausea better?
Quality
What does the pain feel like?
Note: If the client struggles to answer this question, you can provide suggestions such as “aching,” “stabbing,” “burning.”
What does the itching feel like?
Quantity
How bad is your pain?
How bad is the itching?
Region
Where do you feel the pain?
Point to where you feel the pain.
Where exactly do you feel the nausea?
Radiation
Does the pain move around?
Do you feel the pain elsewhere?
Do you feel the nausea elsewhere?
Severity
(severity scale)
How would you rate your pain on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain you’ve ever experienced?
Note: The severity scale is an important assessment of pain and when used can provide evaluation of a treatment’s effectiveness. After eliciting a baseline, you may provide some sort of pain control intervention and then reassess the pain to see if it was effective.
How would you rate your breathing issues on a scale of 0 to 10, with 0 being no problems and 10 being the worst breathing issues you’ve ever experienced?
Timing
When did the pain start?
What were you doing when the pain started?
Where were you when the pain started?
Is the pain constant or does it come and go?
If the pain is intermittent, when did it last occur?
How long does the pain last?
When did your breathing issues begin?
What were you doing when the itching first started?
Where were you when the itching first started?
Is the nausea constant or does it come and go?
If the nausea is intermittent, when did it last occur?
How long did the nausea last?
Treatment
Have you taken anything to help relieve the pain?
Have you tried any treatments at home for the pain?
Have you taken anything to relieve the itching better?
Have you tried any treatments at home for the itching?
Understanding
What do you think is causing the pain?
What do you think is causing the rash?
Table 2.3: The PQRSTU assessment mnemonic
The order of questions you ask will often depend on the symptom or sign and the flow of the conversation with the client. You will also want to be aware of responses that don’t seem to align. For example, if a client responds to the question about quantity of pain by saying “the pain isn’t too bad,” but then rates the severity of their pain as being 8/10, you should probe further. It is okay to say to the client, “I noticed you rated your pain fairly high, at 8/10, but you said it isn’t too bad. Can you tell me more about that?”
Clinical Tip
When using the PQRSTU mnemonic for assessment, be sure to apply it comprehensively so that you elicit a full understanding of a particular sign or symptom. See Film Clip 2.2 for effective demonstration of using the PQRSTU mnemonic, and Film Clip 2.3 for ineffective demonstration of using the PQRSTU mnemonic.
Film Clip 2.3: Ineffective use of the PQRSTU mnemonic
Developmental and Cultural Considerations
Younger children or clients with developmental delays or disabilities, or cognitive impairments, may not be able to answer the types of questions shown in Table 2.3. The care partner might be able to help answer some of these questions, and in that case, you should explore “why” and “how” questions. For example, if the care partner indicates that the infant’s pain started two weeks ago, you should ask “Why or how do you know that it started then?” Or if you are working with a young child, you will need to modify your language to be more understandable (e.g., “Where does it hurt?” “Where is your owie?”).
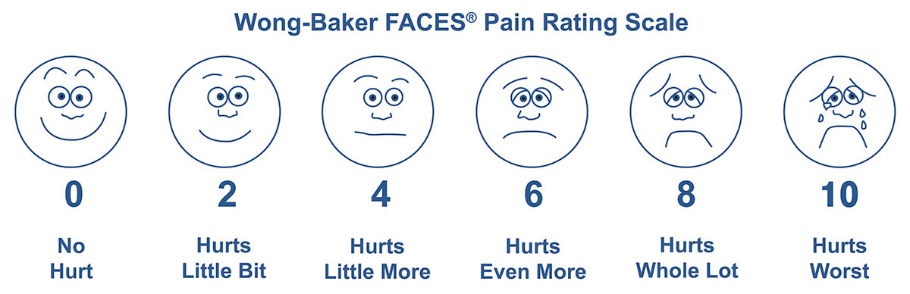
You can also assess pain in young children using the Wong-Baker FACES Pain Rating Scale (see Figure 2.3). When using this scale, ask the client to choose the face that best depicts the pain they are experiencing. You may need to explain what the faces mean: Face 0 doesn’t hurt at all, Face 2 hurts just a little bit, Face 4 hurts a little bit more, Face 6 hurts even more, Face 8 hurts a whole lot, and Face 10 hurts as much as you can imagine.
Figure 2.3: Wong-Baker FACES® Pain Rating Scale Wong-Baker FACES Foundation (2019). Wong-Baker FACES® Pain Rating Scale. Retrieved May 29, 2019, with permission from http://www.WongBakerFACES.org (see their website for licensing)
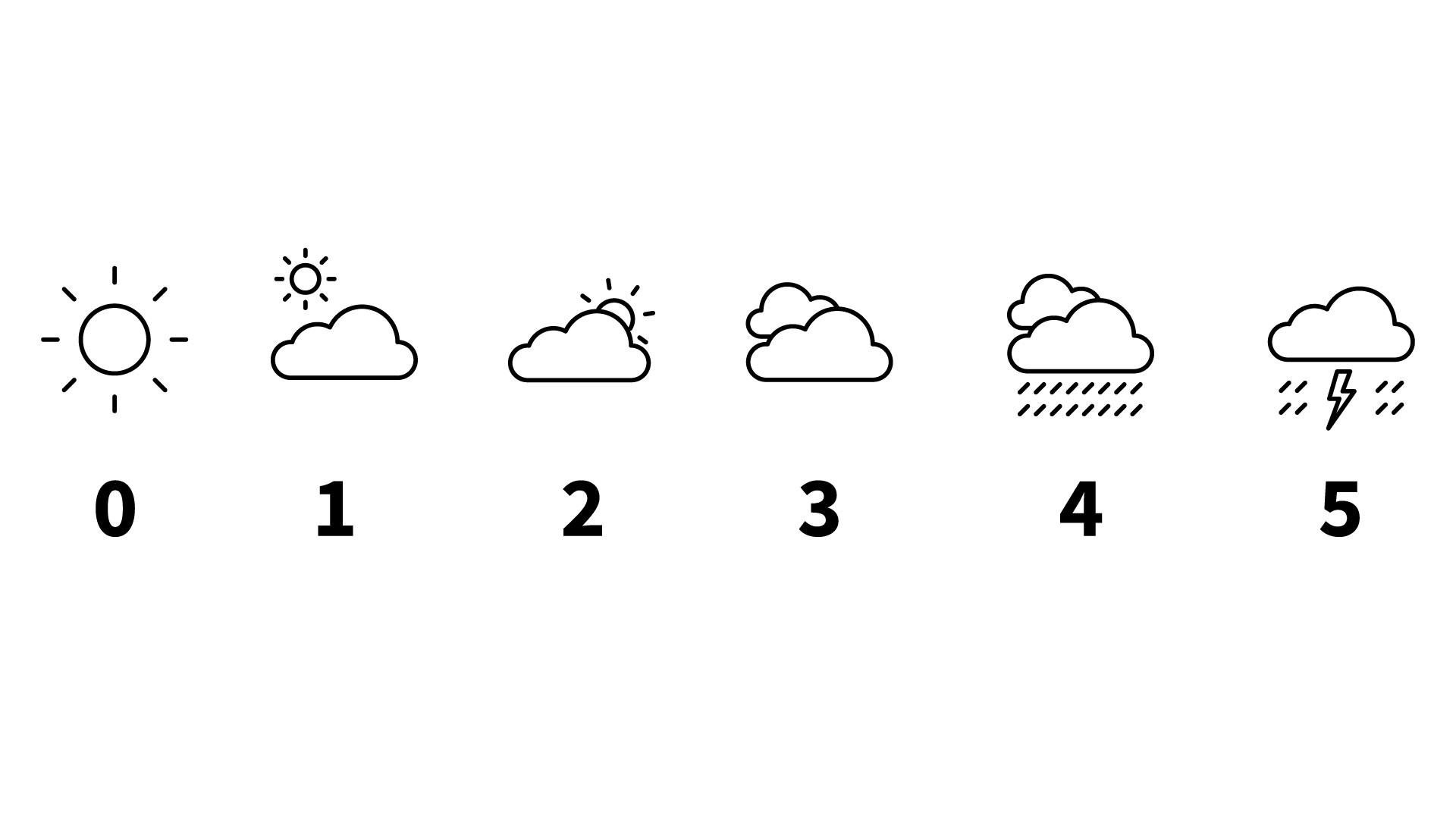
Alternative scales exist to assess pain and other symptoms that are more relevant to certain cultures. See Figure 2.4 for an example of a Sun-Cloud-Pain Scale. On this sliding scale, 0 indicates that the client feels very well whereas 5 indicates that the client is feeling very unwell.
Figure 2.4: Sun-Cloud-Pain Scale. Graphic Created Using Icons by Linseed Studio from the Noun Project.
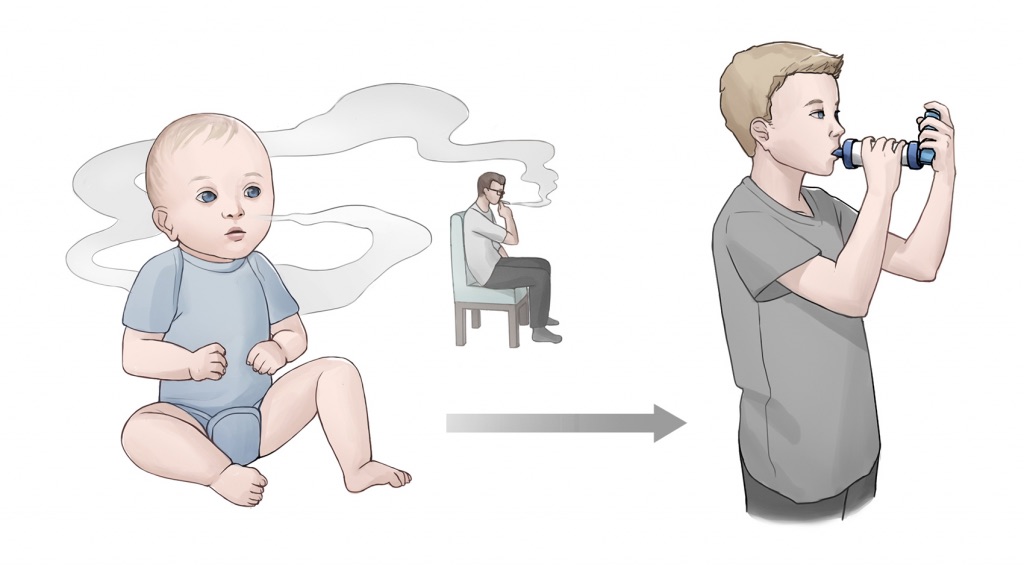
Understanding the client’s current and past health is important and may provide an explanation or rationale for the client’s current health status as illustrated in Figure 2.5. Furthermore, these data can provide insight into health promotion needs and co-morbidities. It is helpful to understand the current and past health profiles before assessing other aspects of health, as the information will inform subsequent questions.
Figure 2.5: The influence of past health on current health
The order of the questions about current and past health, and the detail elicited, often depends on the client’s main health needs and developmental status. Not all questions apply to every client; their use and phrasing is contingent on the individual client and their situation.
Clinical Tip
Your questions should also be based on the client’s response to the previous question.
As you develop your clinical judgment, which comes with practice, you will become more astute about which questions are appropriate and how to frame the questions. Table 2.4 provides sample questions for assessing current and past health, but other questions may arise that you may need to ask depending the client’s main health needs and their responses.
Health Items
Questions and Statements
Considerations
Current health
Issues other than their previously noted main health needs/reasons for seeking care.
Are there any other issues affecting your current health?
Probes
Tell me more.
How is that affecting you?
Although the client may not have made the connection, other health issues are sometimes related to their main health need. For example, they may report a fever in addition to an earache.
Tell me about any acute illnesses that you have had.
Tell me about any accidents or injuries you currently have or have had.
Probes
When did it occur?
Were you hospitalized? Where?
How was it treated?
Who was the treating practitioner?
Did you experience any complications?
Has it resulted in a disability?
How did it affect your day-to-day life?
Falls are an increasing health issue as a person ages or if they are taking several medications. This is partly related to decreases in muscle strength and balance and multimorbidity. It is important to assess the client’s risk for falls and fall prevention. Check out the Registered Nurses’ Association of Ontario (2017) best practice guideline: Preventing Falls and Reducing Injury from Falls
Obstetrical health
Number of pregnancies, full-term deliveries, pre-term deliveries, number of living children, fertility treatments, miscarriages, abortions, and other data related to current or past pregnancy
Have you ever been pregnant?
Do you have plans to get pregnant in the future?
Tell me about your pregnancies.
Have you ever had difficulty conceiving?
How was your labour and delivery?
Tell me about your postpartum experience.
Were there any issues or complications?
These questions do not apply to all clients. Additionally, you should be aware that the feelings about pregnancy can be complex and may not always be happy.
Table 2.4: Current and past health assessment
Clinical Tip
The parents or a care partner are often present during an assessment of an infant or child. The adult child or care partner are sometimes present during an assessment of an older adult, particularly if the client has an acute or chronic illness, or a cognitive impairment or developmental delay. Care partners are important advocates in care planning. Thus, a family-centred approach can help you assess the client, as well as the level of caregiver burden and the need for additional resources.
Take Action
In addition to a comprehensive assessment, you should engage in health promotion discussions about a client’s current and past health. For example, this may include helping the client to address any resolved issues associated with chronic and acute illnesses. Additionally, you should consider how the client can develop control over, and improve their physical, mental, and social well-being. You should assess and discuss with them their social and personal resources to do so. Also, evaluate and intervene with critical findings related to current and past health that include anything that puts the client’s life at risk.
A client’s mental health refers to their emotional and psychological well-being that affects their day-to-day functioning. The World Health Organization (2014) defines mental health as a “state of well-being in which every individual realizes … [their] own potential, can cope with normal stresses of life, can work productively and fruitfully, and is able to make a contribution to … [their] community.” Mental health is often underscreened, which reveals a significant gap considering that stress is pervasive in society.
Clinical Tip
Mental health is a component of every person—a state of well-being that fluctuates throughout life.
Mental illness includes conditions such as depression, anxiety, addiction, schizophrenia, post-traumatic stress disorder, among others. By definition, mental illness is a disruption in everyday function, which means a person’s employment, relationships, and civil participation can all be impaired by mental illness.
It is important to assess a client’s mental health, and if present, mental illnesses. You want to begin this component of the assessment with a statement such as, “Mental health is an important part of our lives and so I ask all clients about their mental health and any concerns or illnesses they may have.”
See Table 2.5 for a selection of questions and statements that you may ask clients to elicit data about their mental health. Note also that there are many other factors that influence mental health, such as violence and trauma, which are addressed under the next section, Functional Health.
Question or Statement
Considerations
Tell me about your mental health.
This question broadly focuses on health and invites a dialogue. The statement should not be asked in isolation or as a one-off question, as societally and culturally there are different meanings of what constitutes mental health and a client may not identify themselves as having mental health issues. If a client responds “Good,” consider probing a bit further with “Tell me about how so,” or “What do you mean by good?” which allows them to respond in more depth.
Tell me about the stress in your life.
Stress, by and large, is a relatable term that many clients have experienced and that is something they are likely more comfortable talking about than more difficult health issues because it is so ubiquitous. It’s important to be attentive to the client’s language and consider terms they may use, such as “extreme stress,” “severe stress,” “unmanaged stressed,” or “debilitating stress,” as these may indicate an underlying mental health issue or stress that requires intervention.
How does stress affect you?
Understanding how stress affects the client provides insight into the mental, physical, and social impact on them. You may need to probe about how stress affects the client physically, mentally, and socially.
How do you cope with this stress? (may include positive or negative coping strategies.)
This question invites discussion about coping strategies. It is important to be attentive to any self-harm coping strategies such as substance abuse, isolation/disengagement, food restriction, purging, cutting, compulsions, and phobias as these could indicate a mental health issue. Additionally, you want to use a strength-based approach to your assessment and facilitate the client’s capacity to identify and use positive coping strategies.
Have you experienced a loss in your life or a death that is meaningful to you?
Inviting discussions about loss and grief could be helpful for clients who have not had an outlet to speak openly about their emotions and the impact. Allowing for loss and grief to be talked about and understanding to what degree grief is affecting health is an important aspect of a mental health assessment.
Have you had a recent breakup or divorce?
Estrangement, emancipation, disruption, or severance of a relationship are not necessarily an indication of a mental illness. However, a pattern in relational disruption may indicate underlying issues such as, but not limited to, ineffective relationship skills, poor coping, or low self-esteem. Assess further if the client reports a breakup or divorce.
Have you recently lost your job or been off work?
Many clients define themselves through their work, and job loss can be disruptive to everyday life. Understanding the meaning of loss of employment is an important dimension of mental health.
Have you recently had any legal issues?
Asking about legal issues should be purposeful, not invasive. For example, a pattern of driving under the influence or possession of illicit drugs could indicate an underlying addiction. Use your clinical judgment when asking questions about legal issues, and be sure to convey an unconditionally accepting way of being with the client.
Have you purchased any weapons?
The purchase of weapons by itself is not an indication of mental illness. In Canada, some people enjoy hunting and other recreational activities that involve weapons. However, the purchase of weapons in response to threats to personal safety or to feelings of self-harm could indicate an underlying mental illness.
Table 2.5: Mental health and illness assessment
If the client identifies that they have a mental illness, you want to assess the onset of it, and the associated impacts, treatments, hospitalizations, complications, and disabilities. Here are some questions and statements that you may use to elicit more information about the client’s well-being in light of having a mental illness:
How does that illness affect you?
How does that illness affect your day-to-day life?
How do you cope with the illness?
What resources do you draw upon to cope with your illness?
When were you diagnosed?
Who was the treating practitioner?
Have you been hospitalized? Where?
Tell me about your treatment (e.g., medications, counselling).
Have you experienced any complications?
Has the illness resulted in a disability?
Do you have any concerns that have not been addressed related to your illness?
Take Action
Health promotion is a vital component of all mental health assessments. You should collaborate with the client on how to develop healthy behaviours to promote their mental health. Also, chronic and sustained stress is an influencing factor of certain diseases such as heart disease and cancer. Furthermore, some coping behaviours related to stress, such as using alcohol and cigarettes, can exacerbate the onset of these diseases. Thus, assessment and collaborative interventions are important.
You also need to be attentive to critical findings that require intervention. For example, if a client talks about feeling despair, hopeless, or depressed, it is important to screen for suicidal thinking. You should begin with a general probing question, such as “Have you ever felt like hurting yourself?” If the client responds with a “yes,” then you should progress with more exploratory and specific questions that assess the immediacy and the intensity of the feelings. For example, you may say, “Tell me more about that feeling. Have you been thinking about hurting yourself today? Have you put together a plan to hurt yourself?”
Points of Consideration
The client most at risk is one who has a specific plan about self-harm, specifying how and when, particularly if it is within 48 hours. The age of the client is not a factor in this determination. Under these circumstances, you should not leave the client alone. You should collaborate with them about an immediate emergency plan of care.
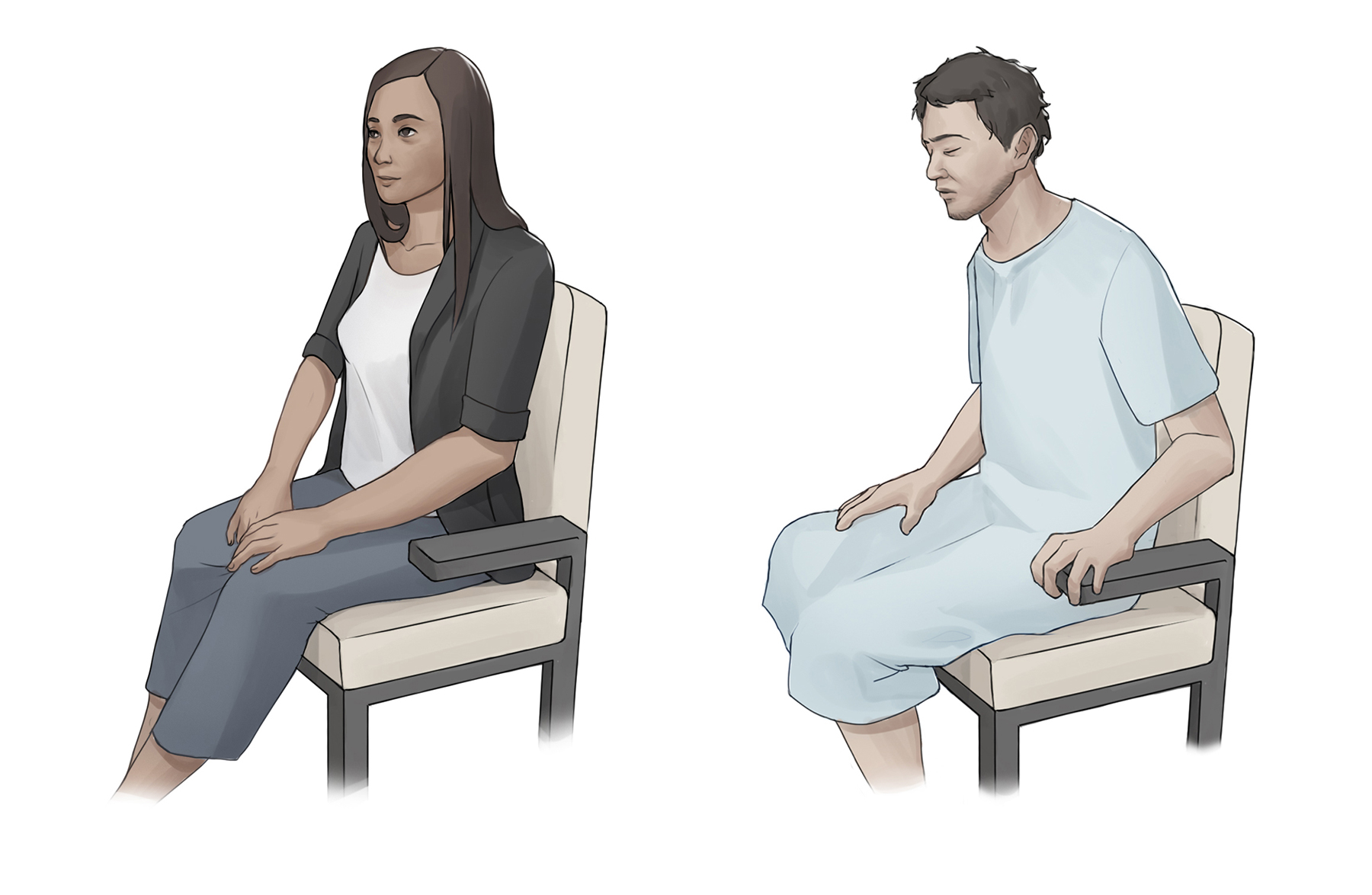
It is important that you not make assumptions about a client’s mental health based on their appearance, facial expression, and capacity to function in their daily life. For example, you shouldn’t assume that a person dressed nicely with a smile or neutral expression is mentally healthy or that a dishevelled person in a gown (see Figure 2.6) has mental health issues.
Figure 2.6: A person dressed nicely with a neutral expression, and a person who appears dishevelled in a gown
Functional Health
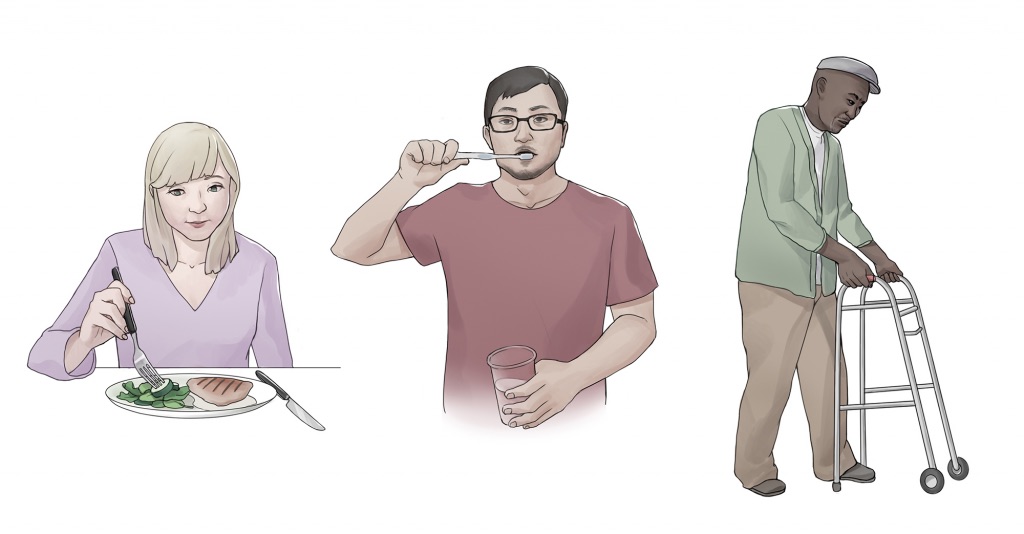
Functional health involves the assessment of the client’s physical and mental capacity to participate in day-to-day activities. It includes assessment of:
Activities of Daily Living (ADL) as illustrated in Figure 2.7 are daily basic tasks that are fundamental to everyday functioning (e.g., hygiene, elimination, dressing, eating, ambulating/moving).
Instrumental Activities of Daily Living (iADL) as illustrated in Figure 2.8 are more complex daily tasks that allow clients to function independently (e.g., managing finances, paying bills, purchasing and preparing meals, managing one’s household, taking medications, facilitating transportation). Assessment of iADL may be particularly important to inquire about with adolescents or young adults who have just moved into their first place and clients who are older and/or have disabilities.
Figure 2.7: Activities of daily living
Figure 2.8: Instrumental activities of daily living
It is important to assess functional health because the data collected could expose an opportunity for preventive action and health promotion, palliation, or assistance. Because health extends beyond the absence of disease, it is important to consider broader dimensions of health as a holistic and complete assessment.
You may start this section of the interview by saying, “Next, I would like to ask you some questions related to your day-to-day life and factors that affect your ability to function in your day-to-day life.” Table 2.6 outlines possible questions and statements to apply to the various sub-categories of functional health, along with some considerations. For interview demonstrations, see Film Clip 2.4 about elimination and Film Clip 2.5 about substance use.
Film Clip 2.5: Interview demonstrating assessment of substance use
Items
Questions and Statements
Considerations
Nutrition
Refers to food and fluid intake, financial ability to purchase food, time and knowledge to prepare and make meals, and appetite or change in appetite. You also want to elicit data related to a client’s usual diet and goals related to their nutrition. Additionally, you need to probe so that an adequate amount of detail is obtained.
Take action
This is an opportune time to engage in health promotion discussions about healthy eating. It is also important to be aware of risks for malnutrition and obesity, specifically assessing for patterns of rapid and excessive weight loss or weight gain.
Tell me about your diet.
What foods do you eat?
What fluids do you drink? (Probe about caffeinated beverages, pop, and energy drinks.)
What have you consumed in the last 24 hours? Is this typical of your usual eating pattern?
Do you purchase and prepare your own meals?
Tell me about your appetite. Have you had any changes in your appetite?
Do you have any goals related to your nutrition?
Do you have the financial capacity to purchase the foods you want to eat?
Do you have the knowledge and time to prepare the meals you want to eat?
The types of questions asked and the level of detail required depends on the developmental age or health of the client.
Infants: Breast milk or formula, amount, frequency, supplements, problems and introductions of new foods.
Pregnant women: nutritional intake and presence of nausea and vomiting, intake of folic acid, iron, omega-3 fatty acids, vitamin D, and calcium.
Older adults or clients with disabling illnesses: Ability to purchase and cook their food, decreased sense of taste, ability to chew or swallow foods, loss of appetite, enough fibre and nutrients.
Elimination
Refers to the removal of waste products through the urine and stool. Healthcare providers refer to urinating as “voiding.” Stool is referred to as a “bowel movement.” You want to assess urine concentration, frequency, and odour. For stool, you want to assess frequency, colour, and consistency. You want to use terminology that clients understand. Thus, you may find yourself using less medicalized terms, such as “pee” and “poo” when speaking with some clients.
Take action
Findings that require further investigation include pain or difficulty upon urination, blood in the stool, melena (black, tarry stool), constipation; diarrhea, excessive laxative use.
How often do you urinate each day?
What colour is it (amber, clear, dark)?
Have you noticed a strong odour?
How often do you have a bowel movement?
What colour is it (brown, black, grey)?
Is it hard or soft?
Do you have any problems with constipation or diarrhea? If so, how do you treat it?
Do you take laxatives or stool softeners?
Toilet training takes several months, occurs in several stages, and varies from child to child. It is influenced by culture and depends on physical and emotional readiness, but most children are toilet trained between 18 months and three years.
Constipation and diarrhea are common symptoms associated with aging and medication usage. Thus, health promotion is needed in this area particularly related to safe food preparation, drinking enough water, sufficient activity, and fibre intake (e.g., fruits and vegetables).
Sleep and rest
Refer to a client’s pattern of rest and sleep and any associated routines or aids. Although it varies for everyone, it is suggested that people should get approximately eight hours of sleep per night.
Take action
Findings that require further investigation include disruptive sleep patterns and reliance on sleeping pills or other sedative medications.
Tell me about your sleep routine.
Probes
How much do you sleep?
Do you wake up at all?
Do you feel rested when you wake? What do you do before you go to bed? (e.g., use the phone, watch TV, read)
Do you take any sleep aids?
Do you have any rests during the day?
Disruption in sleep patterns can occur across the lifespan. Assessing sleep patterns and routines will contribute to collaborative interventions. The use of social media and phones prior to bed can disrupt sleep patterns.
Mobility, activity, exercise
Mobility refers to a client’s ability to move around (e.g., sit up, sit down, stand up, walk).
Activity and exercise refer to informal and/or formal activity (e.g., walking, swimming, yoga, strength training).
Note: In addition to exercise, it is important to assess activity because some people may not engage in exercise but still have an active living lifestyle (e.g., walking to school, working in a physically demanding job).
Take action
Findings that require further investigation include insufficient aerobic exercise and strength training and identified risk for falls.
Tell me about your ability to move around.
Do you have any problems sitting up, standing up or walking?
Do you use any mobility aids (e.g., cane, walker, wheelchair)?
Tell me about the activity and/or exercise that you engage in. What type? How frequent? For how long?
Type of mobility and activity depends on developmental age and a client’s health and illness status. With infants, it is important to assess their ability to meet specific developmental milestones at each well baby visit. Mobility can become problematic for clients who are ill or are aging and can result in self-care deficits. Thus, it is important to assess how their mobility is affecting their ADL.
Violence and trauma
There are many types of violence, including abuse and neglect, physical, sexual, psychological, and financial. Trauma can be a result of violence or other distressing events in a life.
Take action
Collaborative intervention with the client is required when violence and trauma are identified. In Ontario, you are legally mandated to report suspected cases of child abuse or neglect to a children’s aid society. You are also legally mandated to report suspected cases of elder abuse when the client resides in a long-term care or retirement home to the Ministry of Health and long-term care director. You are also required to report to the College of Nurses of Ontario if you suspect that a nurse has abused or sexually abused a client. At any time, if you or the client is in immediate danger, call the police.
Many clients experience violence or trauma in their lives. Can you tell me about any violence or trauma in your life?
How has it affected you?
Tell me about the ways you have coped with it.
Have you ever talked with anyone about it before?
Would you like to talk with someone?
People respond in different ways to trauma. It is important to use a trauma-informed approach when caring for clients who have experienced trauma. For example, a client may respond to the situation in a way that seems unfitting (such as laughter, ambivalence, denial). This does not mean the client is lying; such a response could be symptoms of trauma.
To reduce the effects of trauma, it is important to include social and psychological assessments of recent traumatic events (e.g., sudden loss, near-death experience, gravely ill child) and, more importantly, collaborative interventions to support clients experiencing trauma.
The gendered and racialized experience of violence and trauma are important to assess. In addition to children, people with disabilities, and elderly people, there are other cohorts who are more at risk and respond to violence and trauma based on their identity.
Relationships and resources
Refer to influential relationships in the client’s life, whether positive or negative.
Take action
Findings that require further investigation include indications that a client does not have any meaningful relationships or has “negative” or abusive relationships in their lives. Sometimes the action involves providing a safe space for the client to talk about their experiences and working with them to identify goals.
Tell me about the most influential relationships in your life.
Tell me about the relationships you have with your family.
Tell me about the relationships you have with your friends.
Tell me about the relationships you have with any other people.
Probes
How do these relationships influence your day-to-day life? Your health and illness?
Who are the people that you talk to when you require support or are struggling in your life?
It is not the number of social contacts, but the social interconnectedness and meaning in relationships that is most important. Some clients can have a lot social contacts but not describe any of them as meaningful.
Intimate and sexual relationships
Refer to sexual feelings, attractions, and preferences toward other people. It involves a combination of emotional connection and, physical companionship (holding hands, hugging, kissing) and sexual activity. It is also linked with a person’s identity and part of their physical and mental health.
Take action
Assess further if a client describes, or if you observe, a partner who is controlling, reinforces stereotypical gendered roles (domineering), acts jealous or possessive, or has volatile moods. Although you are not legally responsible for reporting abuse in the adult context, it is important to fully assess and work with the client in developing a safety plan.
I always ask clients about their intimate and sexual relationships. To start, tell me about what you think is important for me to know about your intimate and sexual relationships.
Tell me about the ways that you ensure your safety when engaging in intimate and sexual practices.
Do you have any concerns about your safety?
Gender is a social construction that exists along a continuum. It is a way of being with other people and not a binary . Gender is different than sexuality. It is important to be attentive to your language and expectations related to gendered roles within a relationship and not make assumptions about things such as who drives, who takes care of the children, or who earns the family income within a relationship.
Substance use and abuse
Refers to the intake of alcohol, tobacco products (e.g., smoking, chewing tobacco), cannabis, or any illegal drugs (e.g., cocaine, heroin, meth, inhalants, fentanyl). Assess the type, frequency, quantity, patterns, making a distinction between use and abuse. Substance abuse typically constitutes a disruption in everyday function because of a dependence on a substance (e.g., loss of employment, deterioration of relationships, loss of home or precarious living circumstances).
Take action
Action is needed if clients indicate that they have a problem with substance use or show signs of dependence, addiction, or binge drinking.
To better understand a client’s overall health, I ask everyone about substance use such as tobacco, herbal shisha, alcohol, cannabis, and illegal drugs.
Do you or have you ever used any tobacco products (e.g., cigarettes, pipes, vaporizers, hookah)? If so, how much?
When did you first start? If you used to use, when did you quit?
Do you drink alcohol or have you ever? If so, how often do you drink?
How many drinks do you have when you drink?
When did you first start drinking? If you used to drink, when did you quit?
Do you use or have you used any cannabis products? If so, how do you use them? How often do you use them?
When did you first start using them?
Do you purchase them from a regulated or unregulated place?
If you used to use cannabis, when did you quit?
Do you use any illegal drugs? If so, what type? How often do you use them?
Tell me about the ways that you ensure your safety when using any of these substances.
Have you ever felt you had a problem with any of these substances?
Do you want to quit any of these substances?
Have you ever tried to quit?
It is important to use a non-judgmental approach when assessing a client’s use of substances so they feel accepted and not stigmatized. Substance (mis)use can affect people of all ages. Binge drinking is a health issue that sometimes affects adolescents and young adults. Also, use of some substances can influence the effectiveness of prescription medication.
Environmental health and home/occupational/school health
Environmental health refers to the safety of a client’s physical environment, which is a determinant of health. Examples include exposure to community violence, air pollution, and insect infestations. This may include health and safety in the school and workplace (e.g., hazardous materials, noise, body mechanics).
Take action
Findings that require further investigation include a client being exposed to unsafe environments. This includes prolonged exposure to second- and third-hand cigarette smoke, which is particularly hazardous for children (e.g., smoking in vehicles with children in the car).
Tell me about any factors in your environment that may affect your health. Do you have any concerns about how your environment is affecting your health?
Tell me about your home. Do you have any concerns about safety in your home or neighbourhood?
Tell me about your workplace and/or school environment.
What activities are you involved in or what does your day look like?
Note: These questions will help you determine if probing, detailed questions are needed. For example, if a student or an office worker indicates they are on the computer most of the day, you may need to probe about ergonomics. If a client is working in a healthcare setting, you may need to probe about hazardous materials.
It is important to understand exposure to environmental hazards as nuanced. Not all exposure is the same. For example, during pregnancy, a client may be more attentive to environmental exposures. Some municipalities have banned pesticide use as even small dose exposure can have long-term health effects. It is important to ask about clean and safe water, more so in particular areas than others.
Self-concept and self-esteem
Self-concept refers to all the knowledge a person has about themselves that makes up who they are (i.e., their identity). Self-esteem refers to a person’s self-evaluation of these items as being worthy or unworthy. It is best to assess these items toward the end of the interview because you will already have collected data that potentially contributes to an understanding of the client’s self-concept and self-esteem.
Take action
Findings that require further investigation include a client having low self-esteem, which can be inextricably related to mental health and wellness. Indeed, a criterion for diagnosing mental illness includes low-self-esteem, which can contribute to illnesses such as depression and anxiety.
The factors that contribute to self-concept and self-esteem vary from person to person, so it is assessed best by using open-ended statements. You may need to prompt a client’s responses by saying, “Tell me more” or “Please explain.”
Tell me what makes you who you are.
Are you satisfied about where you are in your life?
Can you share with me your life goals?
The factors that influence a client’s self-concept vary from person to person. Often these items involve valued elements of life such as talents, education, accomplishments, family, friends, career, stability and financial status, and spirituality and religion.
Other iADL
Refers to more complex daily tasks that allow clients to function independently.
Take action
Findings that require further investigation include risk for falls in the home for clients with mobility limitations. These falls can occur while the client is trying to take care of their home (e.g., when cleaning or cooking). A previous history of falls is an important predictor of future falls. If the client reports a fall at home, brainstorm with them to identify hazards in the home (e.g., loose rugs, wet floors, socks without traction) and strategies for safety (e.g., mobility devices, removing tripping hazards, installing handrails).
Tell me about how you take care of yourself and manage your home.
Do you have sufficient finances to pay your bills and purchase food, medications, and other needed items?
Do you have any current or future concerns about being able to function independently?
Avoid making assumptions about a client based on their age. It is important to maintain an optimistic view and work collaboratively with the client.
Assessing for other preventive treatments and examinations includes gathering data on medications, examination and diagnostic tests, and vaccinations. See Table 2.7 for sample questions and statements, along with specific considerations. You might begin this section by asking the client, “What are the ways that are most important for you to optimize your health?” (you may have already discussed this as part of the functional health section).
It is important to ask the client about their current, past, and known future medication regime, examinations, and immunizations to form a profile of the treatment that the client has received and plans to receive. This information will tell you a lot about the client’s current health status based on the care they have and will receive.
Note: The client may refer to items that have already been discussed as part of the functional assessment or other items not yet discussed. You may need to probe with statements such as, “Tell me more,” and “How does that affect you?”
Items
Questions and Statements
Considerations
Medications
Name, dose, frequency, reason for taking it, when they first started taking it, and whether they take it as prescribed. This applies to both prescribed and over-the-counter medications, such as vitamins, pain relievers, homeopathic medicines, and cannabis.
Take action
Medication misuse refers to taking medications outside their prescribed purpose. It can include snorting or injecting medications or taking excessive (large) non-prescribed dosages of medications such as opioids, sedatives, stimulants, and hypnotics. Assess further if you suspect medication misuse.
Do you have the most current list of your medications?
Do you have your medications with you? (If not, you should ask them to list each medication they are prescribed and if they know the dose and frequency.)
Can you tell me why you take this medication?
How long have you been taking this medication?
Do you take the medications as prescribed? (If they answer “no” or “sometimes,” ask them to tell you the reasons for not taking the medications as prescribed.)
Some clients and their care partners are active in their care and will be able to answer all these questions. Other clients may not be able to answer all these questions particularly in the context of multimorbidity and polypharmacy.
Sometimes, clients do not take the medications as prescribed because they are experiencing adverse effects, have insufficient income to purchase the medications, and/or have received insufficient health promotion education and discussions when the medication was prescribed.
Examination and diagnostic dates
Primary care provider (physician or nurse practitioner), specialists, blood pressure, blood tests, chest radiographic, electrocardiogram, dental, vision or hearing. (See Appendix A for a list of links to screening recommendations.)
Take action
Assess further if the client is an older adult who has never received any screening such as blood pressure. It is important to explore with the client the reasons they have not received prior screening.
When was the last time you saw [name the primary care provider, nurse or specialist]?
Can you share with me why you saw them?
When was the last time you had your [name screening] tested?
Do you know what the results were?
This is an opportune time for health promotion, particularly if you identify that examinations such as dental or vision have not been completed based on screening recommendations.
Genetic screening during pregnancy is optional. In collaboration with their health professionals, some parents choose to screen for any abnormalities and others do not. A finding of an abnormal result can be extremely difficult for some parents to experience, and some will decide not to act on such a result.
Vaccinations
Type, date received, and any significant reactions (check the provincial or territorial immunization schedule). Immunization schedules for Ontario and immunization requirements for school attendance in Ontario can be found at Immunizations.
Schedules for other provinces and territories are also available on the Internet.
Take action
Follow up on clients whose immunizations are not up-to-date.
Can you tell me about your immunization status?
Can you tell me what immunizations you have had, the dates you received them, and any significant reactions?
Do you have your immunization record?
When was your last flu vaccine?
If the client’s immunizations are not up-to-date or you noted vaccination hesitancy, you may ask:
Can you tell me the reasons that your immunizations are not up-to-date?
Can you tell me why you are hesitant to receive immunizations? (You may need to explore this further.)
Depending on the client’s age and main health needs/reasons for seeking care, you may ask about specific immunizations such as:
Tetanus if they have an injury or wound in which the skin is not intact.
Childhood vaccinations and adult boosters.
Vaccines for older adults such as influenza, pneumococcal, and shingles.
Vaccine hesitancy is a current global issue referring to the delay or refusal of vaccinations. Nurses and other health professionals play a vital role in addressing this issue. You should use a non-judgmental approach and work in partnership with your client to better understand their concerns. Using a relational inquiry approach will allow you to understand what is important to the client and, thus, be able to address existing knowledge gaps.
Some clients who are immune-compromised cannot receive vaccinations. During times of outbreaks, they are at risk for exposure.
Table 2.7: Preventative treatments and examinations
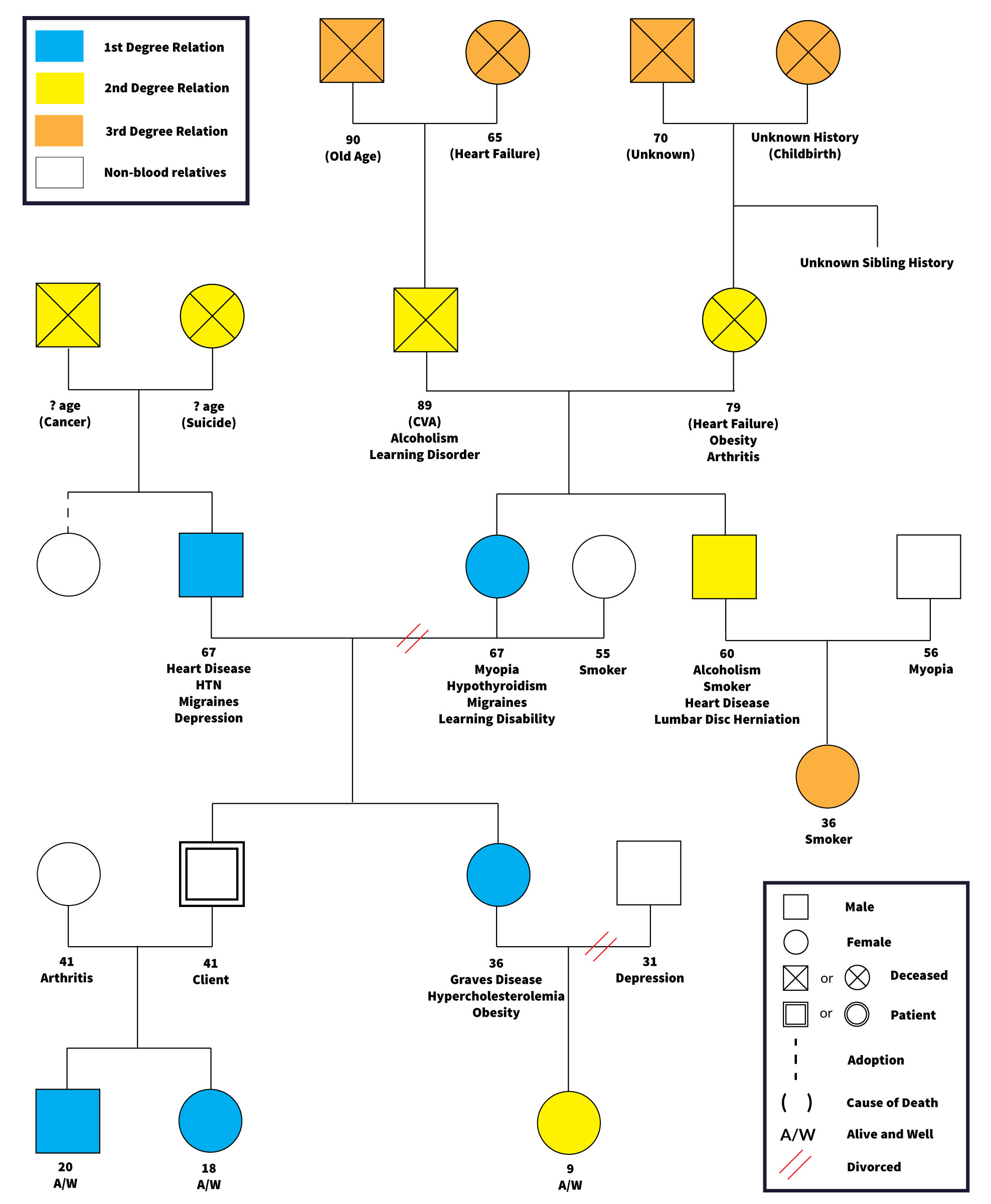
Assessing the current and past health of a client’s family is important because diseases sometimes have a genetic component. These data provide you with a risk profile for inherited conditions. While it is important to understand the risk and likelihood of illness based on family health, these factors do not determine health and wellness. Sometimes health professionals construct genograms to document this information as illustrated in Figure 2.9. There are various ways to construct genograms, this is one example.
You want to ask questions that elicit information about the health status, age, and if applicable, cause of death and age at time of death of blood relatives (parents, grandparents, siblings, children, nieces, nephews). Questions to ask include:
Tell me about the health of your blood relatives.
Do they have any chronic or acute diseases (e.g., cardiac, cancer, mental health issues)?
Have any of your blood relatives died?
If so, do you know the cause of death?
And at what age did they die?
You also want to assess the health status of non-blood relatives and individuals that clients have had close encounters with or live with; this can be an important part of the assessment particularly in terms of communicable diseases (i.e., diseases spread through air, food, physical contact, contaminated surfaces, and insect and animal bites). Questions to ask include:
Tell me about the health status of those you live with.
Has anyone been sick recently?
If so, do you know the cause?
What symptoms have they had?
Have you been around anyone else who was sick recently (e.g., at work, at school, in a location that involved a close encounter such as a plane or an office)?
Figure 2.9: A genogram for a 41 year old client
Points of Consideration
Many people seek genetic information to better understand their family health. This information may be available from genetic counsellors, who are health professionals who offer informational and supportive resources for persons seeking to better understand their genetic health history and risk for genetic disorders and inherited conditions. Also popular today are the DNA tests available commercially to determine family ancestry and health predispositions. Despite their popularity, the accuracy and privacy risks of this latter type of testing is questionable.
Assessing cultural health involves gathering data on factors related to a person’s cultural background that may influence their health and illness status.
An open-ended question allows the client to share what they believe to be most important. For example, you may ask, “I am interested in your cultural background as it relates to your health. Can you share with me what is important about your cultural background that will help me care for you?”
It is best to let clients spontaneously answer this question. Give them time to think. You should explore further any factors that they choose to share (e.g., “Tell me more.” “How does that affect your health and illnesses?” “Is there anything else you want to share about how these factors act as resources in your life?”)
Assessing cultural health once meant having a checklist about different cultural groups. This approach is antiquated because it assumes culture is static and measurable. It is important to encourage each client to speak about what is important to them. You may find that clients speak about information related to how they grew up and their way of life, their values and beliefs, traditions related to food, their spirituality or religion, among many other things.
Points of Consideration
It is important to let the client tell you their cultural health information without interruption or assumption.
How should you begin a complete subjective health assessment?
What are the categories of a complete subjective health assessment?
What mnemonic should you use to assess a client’s reason for seeking care?
Chapter 3: Cultural Safety and Care Partners
IV
Cultural Safety
It is important to conduct the complete subjective health assessment in a culturally safe manner. Cultural safety refers to the creation of safe spaces for clients to interact with health professionals without judgment, racial reductionism, racialization, or discrimination.
Cultural safety begins with an understanding of dominant cultural structures that serve to exclude persons based on their cultural practices (e.g., beliefs, attire, language) or cultural identity (e.g., ethnicity). For example, dominant structures overtly reproduce exclusion when services are only available in English or French. The system covertly reproduces exclusion when persons are made to feel different, or “other,” for their beliefs or views about health.
When seeking cultural health information or any subjective data from a client, it is important to bring a critical lens that acknowledges colonial history, power inequity, and injustice. Consider why you are asking information: is it for racial reductionism or to better understand the client health and illness profile? As described in Table 3.1, today, a critical self-reflective approach is more appropriate, where the health professional questions their own assumptions and challenges stereotypes.
Self-reflective questions
Rationale
How do I describe my own culture?
Reflecting on how you would respond to a question that you pose to a client is always good practice when self-analyzing. Consider whether you are clear or confused by the question. Dig deep to think about how you define and think about culture. We all practise culture, some being more closely aligned with dominant culture than others. For some, when they align with the dominant culture, they may perceive themselves as not having a culture or not recognizing their own culture. Reflect on what it means to be closely aligned or not with the dominant culture and how this may be perceived in your nursing practice.
What assumptions or biases do I hold about culture?
Bias becomes problematic when it is acted upon and taken up as legitimacy. Reflecting on how assumptions and bias have influenced your thinking about culture, including primary language, mainstream knowledge, and concepts about health and illness, is important for you to understand how to create culturally safe spaces. In addition to thinking about “setting aside” your bias or assumptions, give thought to the belief system that has contributed to your own biases. What has informed your thinking?
How might historical legacies affect and inform the healthcare I provide?
Historically, healthcare was a vehicle for imperial and religious practices, and these legacies have contributed to the context of healthcare today. Western healthcare embodies a belief system predicated on empirics, while elsewhere on the globe other practices are taken up. Recognizing that all clients bring a historical cultural context to their interactions with health professionals is helpful in creating cultural safe spaces.
How does my use of language affect cultural safety?
We all become indoctrinated to language. It is often emblematic of a greater belief system. This indoctrination influences how we practise (e.g., how we refer to people and our interactions with clients). For example, labelling someone by their race or religion reinforces “othering,” where their identity is imposed on them. “Objectified language” refers to language that leads to the objectification of someone (e.g., “the diabetic,” “the alcoholic”) implying that the person is devoid of nuance beyond their pathology and defined by a biomedical system. When thinking about your own language, consider its effects on the client.
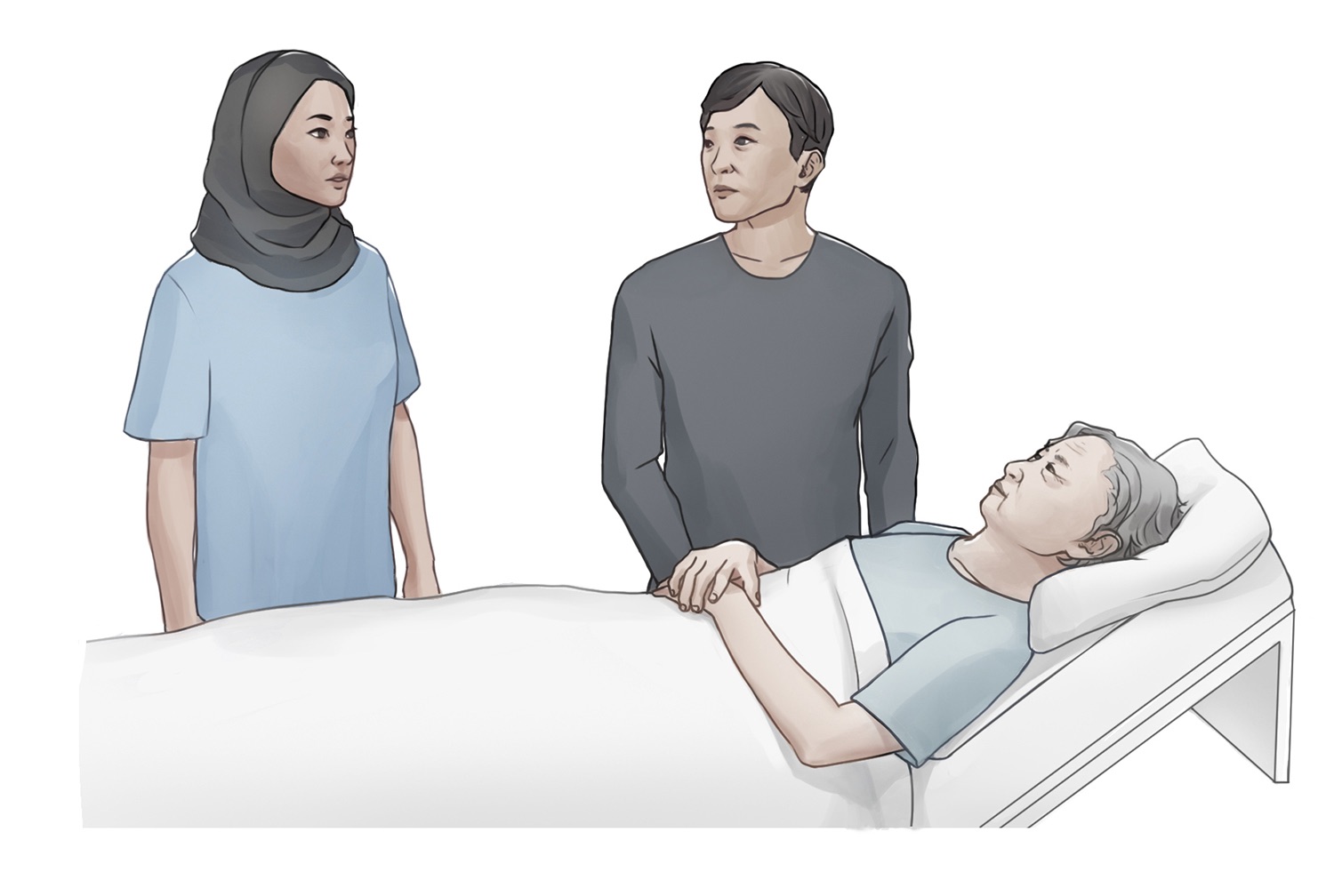
Care partners (as illustrated in Figure 3.1) contribute significant unpaid care work that helps the care recipient while also sustaining the healthcare system. They often interact with the healthcare system in a multitude of ways (e.g., providing care, navigating care services, advocating for better care, coordinating services, and communicating with health professionals).
Figure 3.1: Care partner present with the client and health professional
Certain cohorts of the population take up the role of care partner more than others. Most often care partners are women and older adults. Many adult children are also care partners, who are sometimes referred to as the “sandwich generation” because they are “sandwiched” between caring for their aging parents as well as their own young children.
In your assessment, you should consider families as the recipients of care, not just the individual client. This way of practice is important considering that care work can take a toll on the physical and mental well-being of care partners. The well-being of the client and thus, the intensity of care work, can influence a care partner’s well-being. Likewise, a care partner’s well-being can influence the well-being of the client. This influence becomes more pronounced with aging and with home care where there is a strong reliance on each other for well-being.
Reflective Questions
3
If a health professional was conducting a complete subjective health assessment of you, what would you want them to do in order to create a safe and comfortable environment?
How should you include care partners when conducting a complete subjective health assessment of a client?
Chapter 4: Summary
V
Health History Summary
There are two main components to concluding the complete subjective health assessment. First, you want to provide a brief summary to the client of their subjective health. This summary may include main health issues that require intervention as well as the client’s health strengths and coping strategies. Second (after the summary), you should ask the client whether there is anything else that is important for them to share. You may phrase the question as, “Is there anything else that you think I should know about your current and/or past health and illnesses in order to care for you?”
Reflective Questions
How do you conclude a complete subjective health assessment?
Practise conducting a complete subjective health assessment on a peer, a friend, or a family member. Afterwards, ask them what made them feel comfortable and uncomfortable during the assessment, or ask, “As your healthcare provider, how could I have made the experience better for you?” You should also ask yourself three questions: “What did I do well?” “What did I struggle with?” and “How can I improve?”
Key Takeaways
In this book, you learned about the nature of subjective data and the timing and comprehensiveness of a complete subjective health assessment. This book provided you with the opportunity to both understand the categories of a complete subjective health assessment and reflect on how questions are formulated and meaningfully taken up in the context of the assessment. In summary, it is important to recognize the diversity of a client’s experiences within the healthcare system and how to create a culturally safe, inclusive, and responsive environment while conducting a complete subjective health assessment.
Appendix A: Links to Common Screening Recommendations and Organizations
1
General
Up-to-date recommendations based on the current evidence: Canadian Task Force on Preventive Health Care, established by the Public Health Agency of Canada, offers clinical practice guidelines that support primary care providers in delivering preventive health care: Canadian Task Force on Preventive Health Care Guidelines
Provincial/territorial government programs and services, including coverage and recommendations for screening. Search for your region (e.g., the Ontario Ministry of Health and Long Term Care: Ontario Ministry of Health and Long Term Care).
Canadian Dental Association (CDA): Recommendations for dental screening, cleaning, and X-rays vary based on several factors such as your dental health and age. The CDA suggests a dental exam approximately every six months. They are not specific about the frequency of X-rays other than to say that if a client has not had any problems, such as cavities for a couple of years, then an X-ray is not required at every appointment. See Canadian Dental Association
American Dental Association: Recommendations for X-rays are every two to three years if the client has good oral health and minimal risk of dental problems.
Vision
Canadian Ophthalmological Society: Recommendations are for an eye exam at six months of age and then frequency based on the client’s eye health and risk of eye problems. They note that a client should see an ophthalmologist when they experience vision problems or changes to the eye: Canadian Ophthalmological Society
Appendix B: The Complete Subjective Health Assessment – Interview Guide
2
Introductory Information: Demographic and Biographic Data
Name/contact information and emergency information
What is your full name?
What name do you prefer to be called by?
What is your address?
What is your phone number?
Who can we contact in an emergency? What is their relationship to you? What number can we reach them at?
Birthdate and age
What is your birthdate?
What is your age?
Gender
Tell me what gender you identify with.
What are your preferred pronouns? (If the person asks you to use a pronoun that you are not familiar with, it is okay for you to respectfully respond, “I am not familiar with that pronoun. Can you tell me more about it?”)
Allergies
Do you have any allergies?
If so, what are you allergic to?
How do you react to the allergy?
What do you do to prevent or treat the allergy?
Note: You may need to prompt for information on medications, foods, etc.
Languages spoken and preferred language
What languages do you speak?
What language do you prefer to communicate in (verbally and written)?
Note: You may need to inquire and document if the client requires an interpreter.
Relationship status
Tell me about your relationship status?
Occupation/school status
What is your occupation? Where do you work?
Do you go to school?
Resuscitation status
We ask all clients about their resuscitation status, which refers to medical interventions that are used or not used in the case of an emergency (such as if your heart or breathing stops). You may need more time to think about this, and you may want to speak with someone you trust like a family member or friend. You should also know that you can change your mind. At this point, if any of this happens, would you like us to intervene?
Main Health Needs (Reasons for Seeking Care)
Presenting to a clinic or a hospital emergency or urgent care (first point of contact)
Tell me about what brought you here today.
Probes
Tell me more.
How is that affecting you?
Already admitted, and you are starting your shift
Tell me about your main health concerns today.
Probes
Tell me more.
How is that affecting you?
The PQRSTU Mnemonic
Provocative
What makes your pain worse?
Palliative
What makes your pain feel better?
Quality
What does the pain feel like?
Quantity
How bad is your pain?
Region
Where do you feel the pain?
Point to where you feel the pain.
Radiation
Does the pain move around?
Do you feel the pain elsewhere?
Severity
How would you rate your pain on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain you’ve ever experienced?
Timing
When did the pain start?
What were you doing when the pain started?
Where were you when the pain started?
Is the pain constant or does it come and go?
If the pain is intermittent, when did it last occur?
How long does the pain last?
Treatment
Have you taken anything to help relieve the pain?
Have you tried any treatments at home for the pain?
Understanding
What do you think is causing the pain?
Current and Past Health
Current health
Are there any other issues affecting your current health?
Childhood illnesses
Tell me about any significant childhood illnesses that you had.
When did it occur?
How did it affect you?
How did it affect your day-to-day life?
Were you hospitalized? Where? How was it treated?
Who was the treating practitioner?
Did you experience any complications?
Did it result in a disability?
Chronic illnesses
Tell me about any chronic illnesses you currently have or have had (e.g., cancer, cardiac, hypertension, diabetes, respiratory, arthritis).
Probes
How has the illness affected you?
How do you cope with the illness?
When were you diagnosed?
Who was the treating practitioner?
How was the illness being treated?
Have you been hospitalized? Where?
Have you experienced any complications?
Has the illness resulted in a disability?
How does the illness affect your day-to-day life?
Acute illnesses, accidents, or injuries
Tell me about any acute illnesses that you have had.
Tell me about any accidents or injuries you currently have or have had.
Probes
When did it occur?
Were you hospitalized? Where?
How was it treated?
Who was the treating practitioner?
Did you experience any complications?
Has it resulted in a disability?
How did it affect your day-to-day life?
Obstetrical health
Have you ever been pregnant?
Do you have plans to get pregnant in the future?
Tell me about your pregnancies.
Have you ever had difficulty conceiving?
How was your labour and delivery?
Tell me about your postpartum experience.
Were there any issues or complications?
Mental Health and Mental Illnesses
Mental health is an important part of our lives and so I ask all clients about their mental health and any concerns or illnesses they may have.
Mental health
Tell me about your mental health.
Tell me about the stress in your life.
How does stress affect you?
How do you cope with this stress? (this may include positive or negative coping strategies.)
Have you experienced a loss in your life or a death that is meaningful to you?
Have you had a recent breakup or divorce?
Have you recently lost your job or been off work?
Have you recently had any legal issues?
Have you purchased any weapons?
Mental illness
How does that illness affect you?
How does that illness affect your day-to-day life?
How do you cope with the illness?
What resources do you draw upon to cope with your illness?
When were you diagnosed?
Who was the treating practitioner?
Have you been hospitalized? Where?
Tell me about your treatment (e.g., medications, counselling).
Have you experienced any complications?
Has the illness resulted in a disability?
Do you have any concerns that have not been addressed related to your illness?
Functional Health
Nutrition
Tell me about your diet.
What foods do you eat?
What fluids do you drink? (Probe about caffeinated beverages, pop, and energy drinks.)
What have you consumed in the last 24 hours? Is this typical of your usual eating pattern?
Do you purchase and prepare your own meals?
Tell me about your appetite. Have you had any changes in your appetite?
Do you have any goals related to your nutrition?
Do you have the financial capacity to purchase the foods you want to eat?
Do you have the knowledge and time to prepare the meals you want to eat?
Elimination
How often do you urinate each day?
What colour is it (amber, clear, dark)?
Have you noticed a strong odour?
How often do you have a bowel movement?
What colour is it (brown, black, grey)?
Is it hard or soft?
Do you have any problems with constipation or diarrhea? If so, how do you treat it?
Do you take laxatives or stool softeners?
Sleep and rest
Tell me about your sleep routine.
Probes
How much do you sleep?
Do you wake up at all?
Do you feel rested when you wake? What do you do before you go to bed (e.g., use the phone, watch TV, read)?
Do you take any sleep aids?
Do you have any rests during the day?
Mobility, activity, exercise
Tell me about your ability to move around.
Do you have any problems sitting up, standing up or walking?
Do you use any mobility aids (e.g., cane, walker, wheelchair)?
Tell me about the activity and/or exercise that you engage in. What type? How frequent? For how long?
Violence and trauma
Many clients experience violence or trauma in their lives. Can you tell me about any violence or trauma in your life?
How has it affected you?
Tell me about the ways you have coped with it.
Have you ever talked with anyone about it before?
Would you like to talk with someone?
Relationships and resources
Tell me about the most influential relationships in your life.
Tell me about the relationships you have with your family.
Tell me about the relationships you have with your friends.
Tell me about the relationships you have with any other people.
Probes
How do these relationships influence your day-to-day life? Your health and illness?
Who are the people that you talk to when you require support or are struggling in your life?
Intimate and sexual relationships
I always ask clients about their intimate and sexual relationships. To start, tell me about what you think is important for me to know about your intimate and sexual relationships.
Tell me about the ways that you ensure your safety when engaging in intimate and sexual practices.
Do you have any concerns about your safety?
Substance use and abuse
To better understand a client’s overall health, I ask everyone about substance use such as tobacco, herbal shisha, alcohol, cannabis, and illegal drugs.
Do you or have you ever used any tobacco products (e.g., cigarettes, pipes, vaporizers, hookah)? If so, how much?
When did you first start? If you used to use, when did you quit?
Do you drink alcohol or have you ever? If so, how often do you drink?
How many drinks do you have when you drink?
When did you first start drinking? If you used to drink, when did you quit?
Do you use or have you used any cannabis products? If so, how do you use them? How often do you use them?
When did you first start using them?
Do you purchase them from a regulated or unregulated place?
If you used to use cannabis, when did you quit?
Do you use any illegal drugs? If so, what type? How often do you use them?
Tell me about the ways that you ensure your safety when using any of these substances.
Have you ever felt you had a problem with any of these substances?
Do you want to quit any of these substances?
Have you ever tried to quit?
Environmental health and home/occupational/school health
Tell me about any factors in your environment that may affect your health. Do you have any concerns about how your environment is affecting your health?
Tell me about your home. Do you have any concerns about safety in your home or neighbourhood?
Tell me about your workplace and/or school environment.
What activities are you involved in or what does your day look like?
Self-concept and self-esteem
Tell me what makes you who you are.
Are you satisfied about where you are in your life?
Can you share with me your life goals?
Probes
Tell me more.
Please explain.
Other iADL
Tell me about how you take care of yourself and manage your home.
Do you have sufficient finances to pay your bills and purchase food, medications, and other needed items?
Do you have any current or future concerns about being able to function independently?
Preventive Treatments and Examinations
Medications
Do you have the most current list of your medications?
Do you have your medications with you? (If not, you should ask them to list each medication they are prescribed and if they know, the dose and frequency.)
Can you tell me why you take this medication?
How long have you been taking this medication?
Do you take the medications as prescribed? (If they answer “no” or “sometimes,” ask them to tell you the reasons for not taking the medications as prescribed.)
Examination and diagnostic dates
When was the last time you saw [name the primary care provider, nurse or specialist]?
Can you share with me why you saw them?
When was the last time you had your [name screening] tested?
Do you know what the results were?
Vaccinations
Can you tell me about your immunization status?
Can you tell me what immunizations you have had, the dates you received them, and any significant reactions?
Do you have your immunization record?
When was your last flu vaccine?
If the client’s immunizations are not up-to-date or you noted vaccination hesitancy, you may ask:
Can you tell me the reasons that your immunizations are not up-to-date?
Can you tell me why you are hesitant to receive immunizations. (You may need to explore this further.)
Family Health
Tell me about the health of your blood relatives.
Do they have any chronic or acute diseases (e.g., cardiac, cancer, mental health issues)?
Have any of your blood relatives died?
If so, do you know the cause of death?
And at what age did they die?
Tell me about the health status of those you live with.
Has anyone been sick recently?
If so, do you know the cause?
What symptoms have they had?
Have you been around anyone else who was sick recently (e.g., at work, at school, in a location that involved a close encounter such as a plane or an office)?
Cultural Health
I am interested in your cultural background as it relates to your health. Can you share with me what is important about your cultural background that will help me care for you?
Probes:
Tell me more.
How does that affect your health and illnesses?
Is there anything else you want to share about how these factors act as resources in your life?


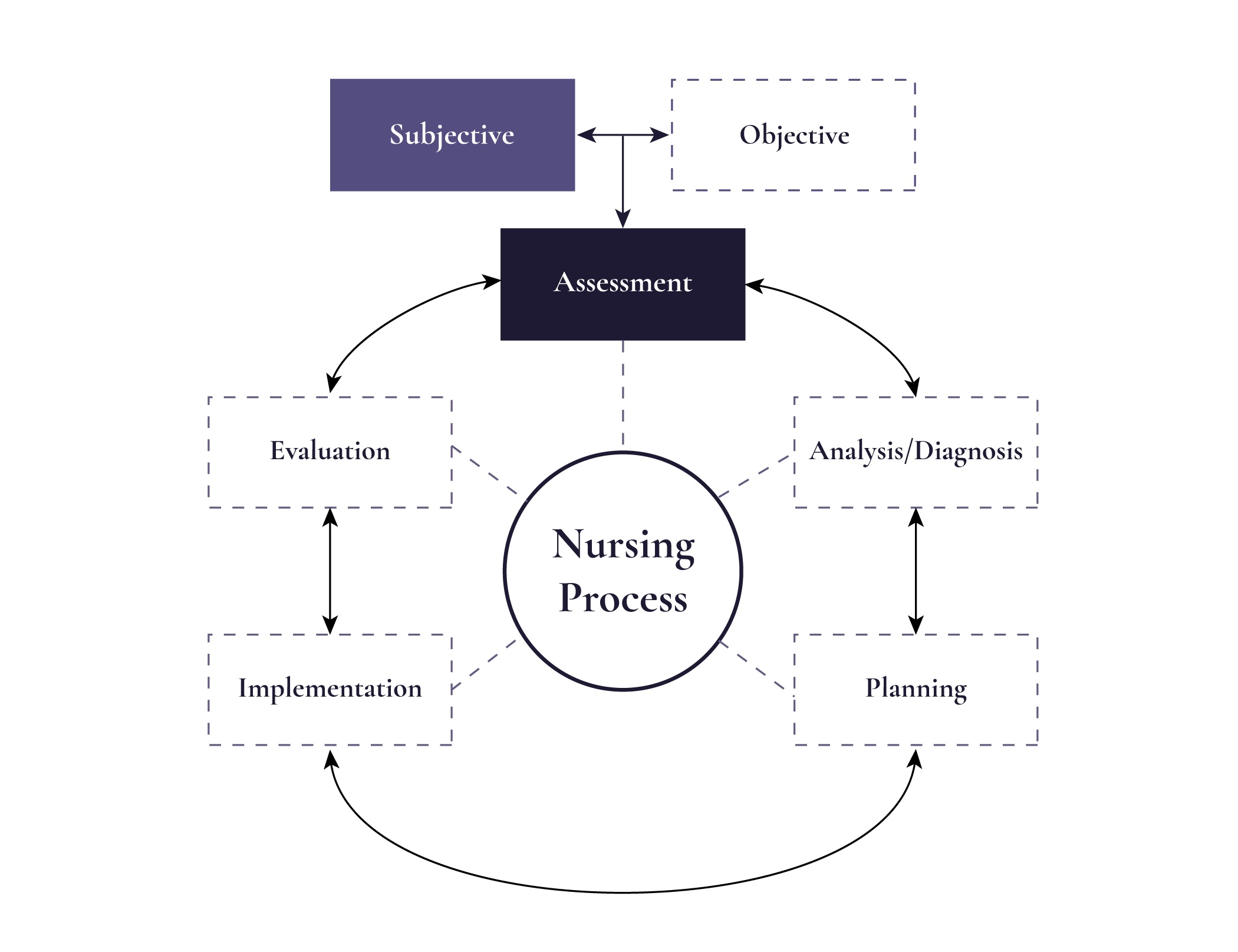





")