Vaccine Practice for Health Professionals: 1st Canadian Edition
Vaccine Practice for Health Professionals: 1st Canadian Edition
Oona St-Amant
Jennifer Lapum
Vinita Dubey
Karen Beckermann
Che-Sheu Huang
Carly Weeks
Kate Leslie
Kim English
Vaccine Practice for Health Professionals: 1st Canadian Edition
Vaccine Practice for Health Professionals: 1st Canadian Edition by Oona St-Amant, Jennifer Lapum, Vinita Dubey, Karen Beckermann, Che-Sheu Huang, Carly Weeks, Kate Leslie, and Kim English is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License, except where otherwise noted.
Preface
I
This open access textbook is intended to guide best practices in vaccine delivery in Canada. This resource is designed for students in post-secondary health profession programs, including nursing. It may also be useful for graduate students and healthcare providers. This textbook provides information related to clinical practice, including the administration of vaccine, and communication with clients.
Legend
1
This textbook is best viewed online in the “Read Book” format available through Pressbooks. The Read Book format enables all Accessible multimedia content. Users can also download a PDF or request a print copy through eCampusOntario’s Open Library.
Throughout this text you will encounter various learning–teaching strategies. Here is a short summary:
Textual information describes the content.
Points of Consideration provide additional information to push your thinking beyond the main point to consider in practice. Points of consideration are visually separated from the rest of the textual information using a text box.
Activities give you an opportunity to evaluate your learning.
Videos and podcasts help you understand the information in a different way.
Important phrases are bolded.
Unfamiliar and complex terms are bolded and included in the glossary at the end of the book. If reading the book online, hover your cursor over a bolded word to reveal the definition.
About eCampusOntario and Authors
2
About eCampusOntario
eCampusOntario is a not-for-profit corporation funded by the Government of Ontario. It serves as a centre of excellence in online and technology-enabled learning for all publicly funded colleges and universities in Ontario and has embarked on a bold mission to widen access to post-secondary education and training in Ontario. This textbook is part of eCampusOntario’s Open Library, which provides free learning resources in a wide range of subject areas. These open resources can be assigned by instructors for their classes, downloaded by learners to electronic devices or printed through the University of Waterloo print on demand service. These free and open resources are customizable to meet a wide range of learning needs, and we invite instructors to review and adopt the resources for use in their courses.
About the Authors
Oona St-Amant, PhD, MScN, BScN, RN, Assistant Professor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, Ontario, Canada
Jennifer L. Lapum, PhD, MN, BScN, RN, Professor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, Ontario, Canada
Vinita Dubey, MD, MPH, CCFP, FRCPC, Associate Medical Officer of Health, Toronto Public Health, Ontario, Canada
Kim English, RN, BScN, MN, Professor, Trent/Fleming School of Nursing, Trent University, Peterborough, Ontario, Canada
Karen Beckermann, RN, BSc, MSc(A), DPA, Associate Director, Vaccine Preventable Diseases, Toronto Public Health, Toronto, Ontario, Canada
Che-Sheu (Sue) Huang, RN, BScN, Health Promotion Specialist, Toronto Public Health, CDC – Vaccine Preventable Diseases Program, Toronto, Ontario, Canada
Carly Weeks, BA, MA, Health Reporter, The Globe and Mail, Toronto, Ontario, Canada
Kathleen Leslie, PhD, JD, RN, Assistant Professor, Faculty of Health Disciplines, Athabasca University, Athabasca, Alberta, Canada
For more information:
Dr. Oona St-Amant
Ryerson University
ostamant@ryerson.ca
415-979-5000 ex. 7986
350 Victoria St.
Toronto, ON M5B 2K3
Note to Teachers Using This Resource
We encourage you to use this resource and would love to hear if you have integrated it into your curriculum. Please consider notifying Dr. St-Amant if you are using it in your course, identifying the healthcare discipline and the number of students. Please help us support future OER efforts by reporting your adoption of this resource at https://openlibrary.ecampusontario.ca/report-an-adoption/.
Acknowledgements
3
Multi-media Consultant
Abigael Krueger, MA, BA, Master of Information student, Faculty of Information (iSchool), University of Toronto, Toronto, Ontario, Canada
Medical Artist
Taeah Kim, H.B.Sc., Master of Science in Biomedical Communications student, University of Toronto, Toronto, Ontario, Canada
Video Editing and Support
Dan Charlebois, Owner and Lead Producer, Bloom Media, Guelph, Ontario, Canada
Roye Cohen, Bachelor of Arts in Image Arts: Integrated Digital student, Ryerson University, Toronto, Ontario, Canada
eCampusOntario team
Lindsay Woodside, HBA, OCT, MA, Program Manager, Nursing OER, eCampusOntario
Lena Patterson, BA, MA, Senior Director, Programs and Stakeholder, eCampusOntario
Emily Carlisle, BA, MLIS, Editorial Lead, Open at Scale, eCampusOntario
Special thank you to video participants:
Sita Mistry, RM, BHScM, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Manjot Salh, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Jamie Spiegel, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Daniel Acdal, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
A Note from Toronto Public Health
4
Vaccinations save lives. The success of vaccines means people have forgotten the consequences of diseases like polio, tetanus, and measles. A growing number of parents are questioning the safety of vaccines over what vaccines protect their children against. This Open Educational Resource will provide healthcare professionals and students some background on the issues of vaccine hesitancy and how to talk with vaccine hesitant clients.
It has been a privilege to contribute to a free and open online resource that is accessible to all nursing students and other health professionals. Toronto Public Health is grateful for this joint collaboration with eCampusOntario and educators across Ontario to enhance the capacity for new health professionals to rebuild and sustain public trust in vaccines.
License
5
This textbook is licensed under a Creative Commons Attribution-ShareAlike 4.0 International (CC BY-SA) license, which means that you are free to:
SHARE – copy and redistribute the material in any medium or format.
ADAPT – remix, transform, and build upon the material for any purpose, even commercially.
The licensor cannot revoke these freedoms as long as you adhere to the following license terms:
Attribution: You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use. ShareAlike: If you remix, transform, or build upon the material, you must distribute your contributions under the same license as the original. No additional restrictions: You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits. Notice: You do not have to comply with the license for elements of the material in the public domain or where your use is permitted by an applicable exception or limitation. No warranties are given: The license may not give you all of the permissions necessary for your intended use. For example, other rights such as publicity, privacy, or moral rights may limit how you use the material.
Chapter 1: Introduction to Immunizations
II
By Oona St-Amant, Jennifer Lapum, and Kim English
Learning Outcomes
6
Learning Outcomes
By the end of this chapter, you will be able to:
Define immunity, immunization, vaccines, and vaccination.
Differentiate innate, passive, and active immunity.
Immunity refers to the body’s ability to prevent the invasion of pathogens. Pathogens are foreign disease-causing substances, such as bacteria and viruses, and people are exposed to them every day. Antigens are attached to the surface of pathogens and stimulate an immune response in the body. An immune response is the body’s defense system to fight against antigens and protect the body.
There are several types of immunity, including innate immunity, passive immunity, and acquired/active immunity. Image 1.1 is a visual showing active immunity as a process of exposing the body to an antigen to produce an adaptive immune response, while passive immunity “borrows” antibodies from another person.
Innate immunity is general protection that a person is born with, including physical barriers (skin, body hair), defense mechanisms (saliva, gastric acid), and general immune responses (inflammation). This type of immunity is considered non-specific (Khan Academy, n.d). Although the immune system does not know exactly what kind of antigen is invading the body, it can respond quickly to defend against any pathogen.
Passive immunity is the body’s capacity to resist pathogens by “borrowing” antibodies. For example, antibodies can be transferred to a baby from a mother’s breast milk, or through blood products containing antibodies such as immunoglobulin that can be transfused from one person to another. The most common form of passive immunity is that which an infant receives from its mother. Antibodies are transported across the placenta during the last one to two months of pregnancy. As a result, a full-term infant will have the same antibodies as its mother. These antibodies will protect the infant from certain diseases for up to a year, and act to defend against specific antigens. Although beneficial, passive immunity is temporary until the antibodies are gone (wane), since the body has not produced the antibodies.
Acquired (adaptive) immunity is a type of immunity that develops from immunological memory. The body is exposed to a specific antigen (which is attached to a pathogen) and develops antibodies to that specific antigen (Khan Academy, n.d.). The next time said antigen invades, the body has a memory of the specific antigen and already has antibodies to fight it off. Acquired immunity can occur from exposure to an infection, wherein a person gets a disease and develops immunity as a result. Acquired immunity also occurs from vaccination wherein the vaccine mimics a particular disease, causing an immune response in the vaccinated individual without getting them ill.
Vaccines are a product given orally, nasally, or by injection to prevent people from acquiring specific diseases. The types of diseases that are prevented by vaccines are called “vaccine-preventable diseases.” Examples of these diseases include chickenpox (varicella) and human papilloma virus (HPV) – though vaccine-preventable diseases will be discussed in detail in Chapter 2.
As noted by the World Health Organization (n.d.), vaccines are a safe and proven tool to prevent life-threatening infectious diseases. “Vaccines work by taking advantage of antigen recognition and the antibody response” (Khan Academy, n.d., under Vaccines). “A vaccine contains the antigens of a [specific] pathogen that causes disease” (Khan Academy, n.d., under Vaccines). For example, the measles vaccine contains the antigens specific to measles. When a person is vaccinated against measles, the immune system responds by stimulating antibody-producing cells that make measles antibodies. As a result, if the body comes into contact with measles infection in the future, the body is prepared to fight it. See Video Clip 1.1 for a description of what vaccines are and how they work.
Video Clip 1.1: “What are vaccines and how do they work?” by Oregan State University Ecampus. CC BY-NC-SA 4.0
Vaccines play an important role in healthy communities for several reasons:
First, they stimulate a person’s immune system to develop antibodies against diseases for protection against that disease.
Second, they protect others by limiting the spread of disease (community immunity). This is important in order to protect vulnerable individuals such as infants, older adults, and those who are ill and unable to receive vaccines for a variety of reasons, including weakened immune systems.
Points of Consideration
The act of administering a vaccine is called “vaccination” and the substance administered is called the “vaccine.” “Immunization” is the process of developing an immune response; it is what happens to a person’s body after a vaccination. When a vaccine is introduced into the body, it stimulates the body to develop antibodies against that disease and protects the body against the disease if exposed to it. “Immunity” involves being protected from a disease and a person is “immune” when they are protected from the disease. If a person does not have immunity and is not protected, then they would be deemed “susceptible”.
Community immunity, also known as herd immunity, is a concept referring to “protection from contagious disease that an individual benefits from as a result of living in a community where a critical number of people are vaccinated” (Boyd, 2016, para 2). This means that vaccination provides protection to the vaccinated person and also the whole community. In general, more than 90% of the population needs to be immune in order to protect those who are not eligible to be vaccinated; however, the level of herd protection required also depends on the disease. For example, contagious diseases such as measles, which is spread through the air, requires more than 95% protection for community immunity. See Image 1.2 illustrating community immunity through the visual of ‘group protection’ that is acquired when more than 90% of the population is immunized. Video Clip 1.2 explains community immunity in further detail.
Image 1.2: Community Immunity
Community immunity makes it more difficult for contagious disease to enter and spread across a population, thereby significantly reducing the chances of an outbreak. It is important as it affords some protection for vulnerable people who cannot receive vaccines or do not have an effective immune response to certain vaccines. Certain people cannot receive vaccines, including infants, pregnant people, people with immuno-compromising conditions, people on immunosuppressants, and other vulnerable groups.
Video Clip 1.2: “Herd Immunity and Immunizations” by North Carolina School of Science and Mathematics. CC-BY-NC-SA
Not all vaccines are the same. The way in which the body responds to a vaccine depends on the type of vaccine being administered. It is important for health professionals to understand the type of vaccines being administered and how it induces an immune response. This section includes descriptions of different types of vaccines.
Live-attenuated Vaccines
Live-attenuated vaccines induce an immune response that mimics a natural infection which often creates an effective and longer-lasting immunity. Live-attenuated vaccines use a weakened form of the infectious agent (virus or bacteria) to produce an immune response without causing illness. In general, clients who receive these vaccines can have lifetime protection after one or two doses.
Before administering live-attenuated vaccines, health professionals need to consider the following:
Clients with immunocompromising diseases or conditions.
Clients who take immunosuppressant agents.
Clients for whom immunity is uncertain.
Clients who are or may be pregnant.
Individuals with immune deficiency, such as those on immunosuppressant agents or with underlying conditions such as uncontrolled HIV, have a weakened immune system and can get very sick with live-attenuated vaccines. In general, people who are undergoing chemotherapy, who are severely immunocompromised, or who have an uncertain immune status should not receive live vaccines because of the risk of disease caused by vaccine strains. Health professionals should consult the most responsible provider before vaccination. Health professionals should refer to the Vaccination of Specific Population of the Canada Immunization Guide for specific information.
Screening Questions for Immunizing with Live Vaccines
1. Does the vaccine recipient have any immunocompromising conditions, or have they taken any medications in the past three months that cause immunosuppression, including corticosteroids?
2. If giving a live vaccine to young child (note: live vaccines are not given to infants (<12 months of age), consider:
Is there a known or suspected family history of congenital immunodeficiency disorder, HIV infection, or a history of failure to thrive AND recurrent serious infections?
3. Has the vaccine recipient received any other live vaccines in the past four weeks?
4. Has the vaccine recipient received any transfusions of blood or blood products in the last year?
Inactivated/Killed Vaccines
Inactivated vaccines, sometimes referred to as killed vaccines, are composed of either whole or partial pathogens that are not alive and therefore cannot replicate. Pathogens become inactivated through exposure to heat, chemicals, and other purification processes. These types of vaccines prevent diseases caused by bacteria and viruses.
In this case, inactivated/killed vaccines refer to whole pathogen vaccines. Inactivated vaccines use the killed version of the pathogen and its antigens to induce an immune response. Typically, these vaccines provide immune protection that is not as effective as live-attenuated vaccines and often require multiple doses over time in order to sustain immunity as the antibody titers diminish. Generally, the first dose of an inactivated vaccine serves to prime the immune system, while protective immunity (antibody) is provided after the second or third dose. Inactivated vaccines are safer for use in immunocompromised individuals since the vaccine contains inactivated or killed pathogens.
Toxoid (inactivated toxin) Vaccines
Toxoid vaccines are used to prevent diseases caused by bacteria. The vaccine uses a toxin (rendered harmless) made by the pathogen that causes the disease. As a result, the body produces an immune response targeted to the toxin rather than the pathogen itself. It is important to note that toxins are typically responsible for symptoms of a disease, such that exposure to the toxin can elicit immunity.
Toxoid vaccines are safe because they cannot cause the disease. Toxoid vaccines typically require booster vaccinations to sustain immunity.
Subunit Vaccines: Recombinant, Polysaccharide and Conjugate Vaccines
Subunit vaccines use a piece of the pathogen, such as its protein, sugar, or capsid, to provoke an immune response. These vaccines elicit a strong and targeted response to a part of the pathogen and are typically suitable for anyone, including immunocompromised individuals. For sustained immunity, clients typically need multiple doses of vaccine.
While recombinant, polysaccharide, and conjugate are all forms of subunit inactivated vaccines, each target a particular molecular structure. Polysaccharide vaccines consist of long-chained sugar molecules attached to the surface of bacteria such as pneumococcus and meningococcus. Recombinant vaccines are genetically engineered vaccines, whereby pathogenic agents have been cloned, expressed, and purified into a vaccine.
There are several different types of vaccines available, each with a different set of properties and uses. Scientific advances and new technology will continue to change and improve the vaccine landscape. Table 1.1. offers examples of some of the vaccines associated with the various vaccine types.
Table 1.1: Vaccine Types
Vaccine type
Vaccines
Live-attenuated
Measles, mumps, rubella (combined vaccine)
Varicella (chickenpox), Zoster (shingles)
Influenza (nasal spray)
Oral Polio Vaccine (OPV)
Rotavirus
Yellow fever
Inactivated/Killed
Polio (IPV)
Hepatitis A
Rabies
Toxoid (inactivated toxin)
Diphtheria
Tetanus
Subunit/Conjugate
Hepatitis B
Influenza (injection)
Haemophilus influenza type b (Hib)
Human papillomavirus (HPV)
Pertussis
Pneumococcal
Meningococcal
Zoster (shingles)
Points of Consideration
The body produces a greater immune response the more analogous the vaccine is to the original disease-causing pathogen. Live-attenuated vaccines more closely resemble their pathogen, making ongoing vaccinations less likely to achieve sustained immunity. Most live-attenuated vaccines in Canada are viral; however, there are two bacterial attenuated vaccines (typhoid and tuberculosis) that are available under special circumstances.
Content in Table 1.1 was adapted, with editorial changes, from https://www.vaccines.gov, which is in the public domain.
Vaccine Components
12
The components of vaccines used in Canada are extremely safe. See Image 1.4 for an illustration of vaccine components and Table 1.2 for a description of the components.
Image 1.4: Vaccine Components
Serious side effects like allergic reactions are very rare. Chemicals used in vaccines enhance their effectiveness, preserve or stabilize the pathogen, kill unwanted viruses, or act as a suspension to hold the product. Some vaccines contain trace amounts of culture material like egg protein used to grow the virus or bacteria. It is important for health professionals to familiarize themselves with some of the common components (also referred to as ingredients) in vaccines, particularly if a client has an allergy or expresses concern in this regard. For a comprehensive list of vaccines and their components visit Canadian Immunization Guide, Key Immunization Information.
Table 1.2: Vaccine Components
Component
Description
Antigen
The active component of the vaccine that causes an immune response.
Adjuvants
Component that enhances the vaccines’ effectiveness. Most vaccines use aluminum-based adjuvants. They induce a range of inflammatory factors to the injection site which helps the immune response. Aluminum is removed from the body in urine via the kidneys.
Preservatives
Preservatives stop unwanted contamination of a vaccine. The most common preservative is 2-phenoxyethanol, which is also used in a range of cosmetics, baby care products, eye and ear drops.
Clients may be concerned about the presence of Thimerosal, a mercury-containing preservative used in multi-dose vaccines to prevent contamination of virulent bacteria or fungus. Contrary to popular belief, most vaccines in Canada do not contain Thimerosal. School-required vaccines have not contained Thimerosal since 2001.
Stabilizers
Stabilizers, such as gelatin, stop chemical reactions from occurring in the vaccine and prevent the components from separating. Other stabilizers include amino acids (the building blocks of proteins), potassium, sodium, and lactose.
Buffers
A buffer solution resists changes in pH when small quantities of an acid or an alkali are added to it. Buffers keep the vaccine at a similar pH to the body. Often the buffer will be a salt.
Adjusting tonicity
To keep the vaccine isotonic (to reduce local reactions) a salt may be added. Often this will be Sodium Chloride (common table salt).
Surfactants and emulsifiers
These agents act like a detergent. A commonly used surfactant is called Polysorbate 80 or Tween®. This is made from sorbitol (a sugar alcohol) and Oleic acid (an omega fatty acid). Polysorbate is often used in foods such as ice cream.
Formaldehyde
Formaldehyde is used to detoxify or inactivate the live germ or toxin used in some vaccines. It is mostly removed during the purification process. It is important to note that trace amounts of Formaldehyde is found in all human bodies and is required for the synthesis of DNA. Formaldehyde breaks down very quickly both in the environment and in the body. Additionally, there is about ten times the amount of formaldehyde in a baby’s body than there is in a vaccine.
Antibiotics
Some vaccines contain antibiotics to prevent bacterial growth during storage of the vaccine.
Points of Consideration
There is a common misconception about the types of mercury contained in vaccines and the levels of toxicity. As health professionals, it is important to resolve public misconceptions through accurate information about the type of mercury used in vaccines and the varying degrees of toxicity and risk.
Ethylmercury is sometimes present in vaccines. It does not stay in the body for long (about seven days) and is excreted through the gut which makes it less harmful to vital organs.
Thimerosal is a mercury-containing preservative used in multi-dose vaccines to prevent contamination of virulent bacteria or fungus. Contrary to popular belief, most vaccines in Canada do not contain Thimerosal. School-required vaccines have not contained Thimerosal since 2001.
Methylmercury is not found in vaccines. This type of mercury can be toxic in high doses and is commonly found in certain kinds of fish. It has a half-life of 45 days, meaning it stays in the system for longer periods, increasing risk of toxicity. For this reason, the federal government regulates methylmercury in the environment to limit exposure.
What concerns and questions do you think clients will have about the components of vaccines? How should health professionals respond to these concerns and questions?
Key Takeaways
14
The key takeaways of this chapter are:
Immunity is the capacity of the body to resist pathogens.
There are several types of immunity, including innate immunity, passive immunity, and acquired/active immunity.
Vaccination is a safe and effective way to achieve acquired immunity.
Community immunity (also known as herd immunity) refers to protection from contagious disease that an individual gains as a result of living in a community where a critical number of people are vaccinated.
More than 90% of the population needs to be immune in order to protect those who are not eligible to be vaccinated.
The more analogous the vaccine is to the original disease-causing pathogen, the greater the body’s immune response.
Vaccine components are extremely safe and are important to enhance effectiveness, preserve and stabilize the vaccine, prevent unwanted contamination, and detoxify or inactivate the live germ or toxin in some vaccines.
Vaccines are our best defense against many diseases. Vaccine-preventable diseases (VPDs) are diseases caused by bacteria and viruses that can be prevented by vaccines. VPDs can spread through different routes such as the air, respiratory droplets, and bodily contact. Some diseases, such as measles, are extremely contagious. For example, it is possible to contract measles two hours after a person with measles has left the room.
Many of the diseases prevented by vaccines have dramatically declined since the introduction of vaccination programs. However, awareness of VPDs continues to be a priority so that members of the public and health professionals understand why it is important to keep vaccinating against those diseases. When people stop vaccinating, VPDs, such as measles, can recur and spread rapidly around the world.
Image 2.1: Vaccine-Preventable Diseases
When a disease is eradicated around the world, vaccines are no longer needed. For example, smallpox was eradicated in 1979. As a result, the smallpox vaccine is no longer provided in routine vaccination programs. Diseases are eliminated when the disease is reduced to zero, or close to zero, in a defined geographical area. Polio, for example, is eliminated in North America and South America.
The immunization schedule includes the recommended timing of all vaccine doses in order to be considered fully protected. There are many determinants that influence the schedule including: burden of disease in the province or territory, effectiveness and safety of vaccines, acceptability, ease of implementation, equity, and cost. When individuals are not on the routine schedule, the likelihood of missing doses and having incomplete vaccinations is increased. It also puts the individual at risk for getting the disease because they are not fully vaccinated. Catch-up schedules are available. If vaccination records are not available, assume the person is unvaccinated and use a catch-up schedule based on current age.
Accelerated immunization schedules are also available under necessary conditions such as outbreaks and unplanned travel. The interval between recommended doses can also often be lessened; however, health professionals should consult the Canadian Immunization Guide for vaccine-specific minimum dose intervals.
Points of Consideration
Being vaccinated on time is ideal. For people who start their vaccines later, health professionals can use a ‘catch-up’ schedule which depends on the person’s age. For people with an unknown vaccine history (e.g. newcomers, refugees), the best practice is to treat the person as if they are unimmunized and begin a new immunization schedule.
Timing and Spacing of Vaccines
If vaccines are given before the recommended age or with less than the minimal spacing between doses, adequate immune response may not be achieved. Modifications to the recommended schedule may be necessary because of missed appointments or illness; however, for the most part, disruptions in the schedule do not necessitate restarting a vaccine series.
Community Immunity / Herd Immunity
By keeping up to date with vaccines, we can prevent the spread of disease to those who may be more likely to contract them, such as:
babies.
young children.
pregnant people.
people who are severely immunosuppressed.
Recall the discussion of community immunity, also known as herd immunity, from Chapter 1, in which we learned that in general, more than 90% of the population needs to be immune in order to protect those who are not eligible to be vaccinated (shown in the image below).
90% need to be vaccinated to protect others who are vulnerable or can’t be vaccinated.”" width="500" height="375" srcset="https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity.jpeg 1024w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-300x225.jpeg 300w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-768x576.jpeg 768w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-65x49.jpeg 65w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-225x169.jpeg 225w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-350x263.jpeg 350w" sizes="(max-width: 500px) 100vw, 500px">
Image 2.3: Community Immunity
Ages and Vaccines
20
Infants and Toddlers
A child’s immune system is not fully developed at birth. In the first year of life, an infant’s immune system develops. This makes an infant more vulnerable to communicable diseases. This is also why infants need many doses of vaccines in the first year of life, to prime the immune system and develop immunity. Vaccines protect infants and children when they are most vulnerable and work best when children are immunized on time. These strategies have significantly reduced infant mortality rates in Canada and across the world.Table 2.1 is an example of a routine government-funded vaccine schedule in early childhood.
Table 2.1: Routine Vaccines During Early Childhood in Ontario
Age
Vaccine
Vaccine-Preventable Illness
2 months
DTaP-IPV-Hib
Diphtheria, Tetanus, Pertussis, Polio, Haemophilus Influenzae type B (Hib)
Pneu-C-13
Pneumococcal
Rota
Rotavirus
4 months
DTaP-IPV-Hib
Diphtheria, Tetanus, Pertussis, Polio, Haemophilus Influenzae type B (Hib)
Pneu-C-13
Pneumococcal
Rota
Rotavirus
6 months
DTaP-IPV-Hib
Diphtheria, Tetanus, Pertussis, Polio, Haemophilus Influenzae type B (Hib)
Rota
Rotavirus
12 months
Men-C-C
Meningococcal Disease
MMR
Measles, Mumps, Rubella
Pneu-C-13
Pneumococcal
15 months
Var
Varicella (chickenpox)
18 months
DTaP-IPV-Hib
Diphtheria, Tetanus, Pertussis, Polio, Haemophilus Influenzae type B (Hib)
There is variation in how each province and territory approaches vaccine exemptions. In Ontario, for example, under the Ontario Child Care and Early Years Act (2014), children who attend child care centres are required to either be immunized against the diseases listed in Table 2.1 or have a valid exemption. A medical exemption form is completed by a legally qualified medical provider (i.e. physician or nurse practitioner). A parent who has a philosophical or religious objection may complete a different exemption form. In Ontario, exemptions are granted on the grounds that immunizations conflict with the sincerely held convictions of the parents’ religion or conscience or that a legally qualified medical provider gives medical reasons to the child care centre as to why the child should not be immunized (Ontario Child Care and Early Years Act, Reg. 137/15s).
School Age Children
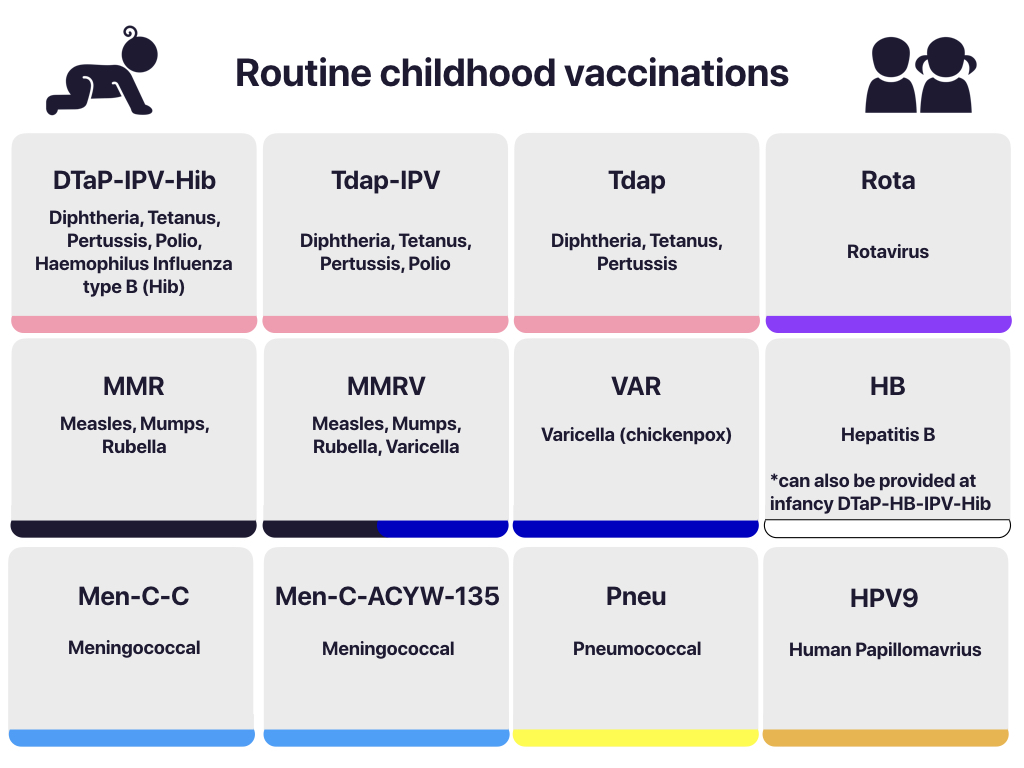
By school entry, students should be up to date with most routine childhood vaccinations. Contagious diseases can spread quickly in a school setting, so it is important to ensure that school aged children are up to date with their immunizations. Table 2.2 is an example of a government-funded vaccine schedule for school-age children.
Table 2.2: Vaccine Schedule for School Age Children in Ontario
Age
Vaccine
Vaccine-Preventable Illness
4-6 years
MMRV
Measles, Mumps, Rubella, Varicella (chickenpox)
Tdap-IPV
Diphtheria, Tetanus, Pertussis, Polio
Grade 7
HB
Hepatitis B (2 or 3 doses)
HPV9
Human Papillomavirus (2 doses)
Men-C-ACYW-135
Meningococcal Disease
14-16 years
Tdap
Tetanus, Diphtheria, Pertussis
In Ontario, under the Immunization of School Pupils Act (1990), students who attend school are required to provide proof of immunization against the following diseases: diphtheria, tetanus, polio, measles, mumps, rubella, meningococcal disease, pertussis, varicella (children born 2010 or later) or have a valid exemption. Parents need to provide a record of their child’s immunization status to the local Public Health Unit. A medical exemption form is completed by a legally qualified medical provider. A parent who has a philosophical or religious objection must attend a mandatory education session and complete the standardized Ministry approved exemption form.
Image 2.4: Routine childhood vaccinations
Healthy Adults
Vaccinations are not just for children. Vaccines are safe and protect you and those around you from vaccine-preventable diseases. As we get older, the protection we had from previous vaccinations can decrease for some diseases. Getting another dose, known as a booster, can increase our immunity to provide the best protection. Some adults may have missed one or more of their vaccines when they were a child. They may need to catch up and get these vaccines now. There are also diseases that are more common in adults—even healthy adults—such as shingles. This is why additional vaccines are needed as we get older.
Many Canadian adults are not up to date with their vaccines. Healthcare providers can assess what is needed to be fully protected. The following table is an example based on the Ontario provincial immunization schedule. Table 2.3 is an example of recommended vaccines for health adults.
Table 2.3: Ontario Vaccine Schedule for Healthy Adults
The National Advisory Committee on Immunization (NACI) recommends recombinant subunit vaccine (2 doses) for people >50 years of age due to greater efficacy.
Inf
Influenza
Annually
Pneu-P-23
Pneumococcal
65 years
HA
Hepatitis A
Not publicly funded for healthy adults (2 doses)
HB
Hepatitis B
Not publicly funded for healthy adults (3 doses)
HPV9
Human Papillomavirus (HPV)
Not publicly funded for healthy adults (3 doses)
Specific Populations and Vaccines
21
Pregnancy
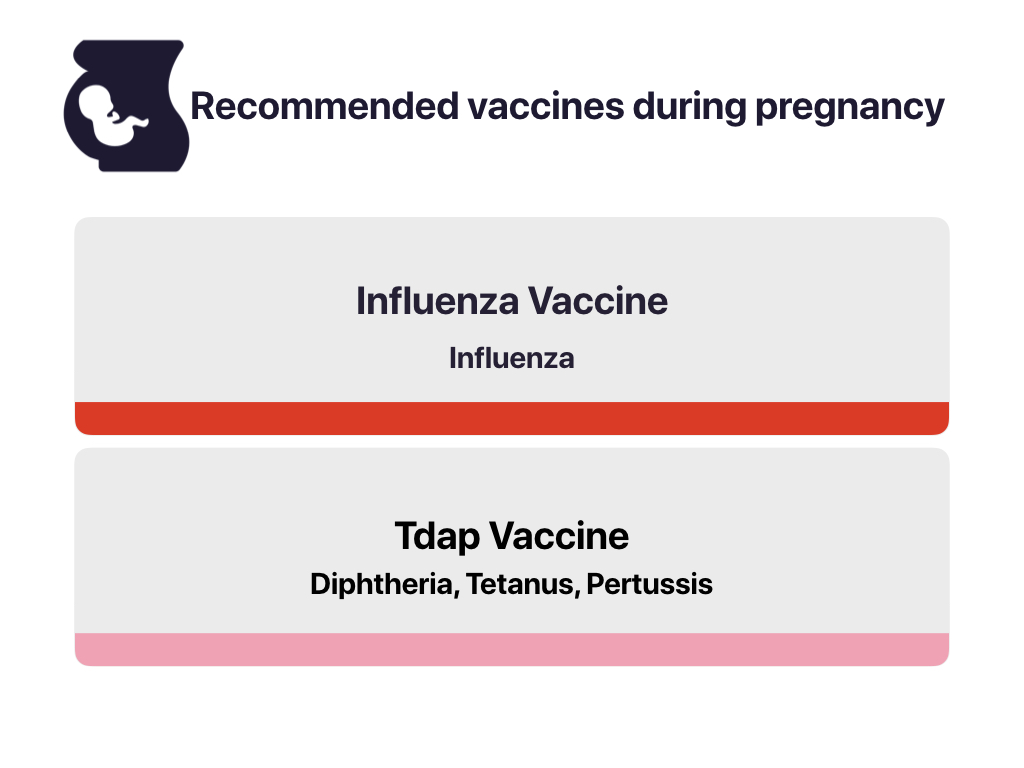
Pregnancy may lead to altered immune responses that increase risk for infection. Vaccinating in pregnancy prevents disease for the pregnant person and their baby. For example, vaccinating with an inactivated flu is safe and recommended in all pregnancies during flu season. The vaccine lowers the risk of complications from flu during pregnancy and protects infection after the baby is born. See Table 2.4 for routine vaccines during pregnancy.
Image 2.5: Recommended vaccines during pregnancy
The other reason to vaccinate during pregnancy is to increase the newborn’s immunity. Because newborn babies are born with rudimentary immune systems, health professionals try to protect the baby in the event of exposure. One method is to vaccinate the pregnant person during pregnancy with, for example, the pertussis vaccine. Another method, called ‘cocooning,’ means vaccinating those around the infant, including the parent and other family members, to ensure they will not infect the newborn. Cocooning can be difficult to do and as a result may not be the preferred strategy.
Table 2.4: Routine Vaccines During Pregnancy
Vaccine
Vaccine-Preventable Illness
Considerations
Influenza Vaccine
Influenza
The flu vaccine is safe and recommended for all pregnant people at any stage of pregnancy. It is especially important if the client will be in the later stages of pregnancy during flu season (November to April). The risk of hospitalization from flu complications increases later in pregnancy and is highest in the third trimester.
The flu shot also helps protect the baby during the first six months after birth. This is important because babies are at higher risk for flu complications that can result in hospitalizations, and babies under six months of age are too young to be vaccinated.
Tdap Vaccine
Pertussis
Immunization for pregnant people is ideally recommended at 27-32 weeks of gestation for each pregnancy, irrespective of previous Tdap immunization history or the interval between pregnancies due to rapid waning maternal antibody.
Breastfeeding and Vaccinations
All routine vaccines that are provided in Canada are safe for women who are breastfeeding. Some less common vaccines, like yellow fever and Bacillus Calmette-Guerin (BCG) vaccine for tuberculosis, should not be administered to breastfeeding women. This is because an infection can be passed to the baby through breast milk.
Travel
Talk to your clients about travelling outside of Canada as they may be at risk for vaccine-preventable diseases. Travel health clinics often provide accurate travel advice that takes the destination and the person’s current health status into consideration. It is important to discuss travel plans as far ahead of travel arrangements as possible, preferably six weeks in advance. See Table 2.5 for common global diseases that can be prevented. Review the immunization history with your client. Ensure your client is up to date with the provincial immunization schedule. Discuss any other trip-related health concerns and ways to keep healthy while travelling.
Table 2.5: Common Global Vaccine-Preventable Diseases
Disease
Vaccine
Cholera and travellers’ diarrhea
E.coli
Hepatitis A
HA
Hepatitis B
HB
Japanese encephalitis
JE
Meningococcal
Men-C-ACYW
MenB
Rabies
Rabies
Typhoid
Typh
Yellow fever
YF
As with routine childhood vaccines, travel vaccines can sometimes come in combined formulations.
The National Advisory Committee on Immunization (NACI) is a multi-disciplinary committee of scientific, medical, and public health experts that make recommendations for current and newly approved vaccines in Canada. The Canada Immunization Guide (CIG) is based on NACI recommendations and other factors. NACI’s work focuses on vaccines while the CIG is a comprehensive resource on immunization. The CIG includes information for all health professionals who administer vaccines or manage immunization programs.
In Canada, immunization programs are a shared responsibility across national, provincial, and local public health agencies. See Tables 2.6, 2.7, and 2.8 for a list of these responsibilities. Public health agencies in Canada use a population health approach to improve the health of all Canadians and create healthier communities, including controlling infectious diseases through immunization strategies. While vaccines are a national issue, each level of government has a specific role and there are differences in how immunization programs are implemented across provinces and communities. For example, provincial public health agencies make determinations about the immunization schedule based on the NACI recommendations while the local public health agencies implement and deliver local services. This strategic and systematic approach to immunization allows for a population health approach while simultaneously ensuring outreach at a local level. As a health professional, it is important to familiarize yourself with the role and mandate of various organizations to ease system navigation, including where and when to access information. Furthermore, having a contextual understanding of program implementation allows you to see both the big picture and the local perspectives when thinking about vaccine-preventable illnesses. Video Clip 2.1 provides additional information about the role of public health nurses and vaccines practice in Ontario.
Video Clip 2.1: Interview about Vaccines and the Role of Public Health
Table 2.6: Organizational Landscape of Vaccine Research, Delivery, and Evaluation – Federal
Federal
Organization
Role in Immunization Delivery
National Advisory Committee on Immunizations in Canada (NACI)
Reports to Assistant Deputy Minister of Infectious Disease Prevention and Control.
Makes recommendations about current and newly approved immunization practices in Canada.
Develops and updates the Canada Immunization Guide (CIG).
Public Health Agency of Canada
Prevents and controls infectious diseases in Canada.
Develops the National Immunization Strategy (NIS).
Identifies under and unimmunized populations in Canada.
Sets goals for vaccine-preventable disease reduction in Canada.
Centre for Immunization and Respiratory Infectious Diseases (CIRID)
Works collaboratively with the provinces and territories to implement the National Immunization Strategy (NIS).
Enhances Canada’s response to and management of infectious diseases and respiratory infections.
Works together with other countries to develop immunization programs and disease prevention strategies.
Immunize Canada
National coalition of non-governmental, professional, health, government, and private sector organizations.
Provides reliable information regarding immunization practices recommended by the NACI.
Promotes and supports the use of vaccines and public health policies to control vaccine-preventable diseases through promotional products and media campaigns.
Canadian Public Health Association
Launched the Creation of a Canadian Immunization Resource Centre in July 2017 that resulted in CANVax, an online database of curated resources to support immunization planning and promotion activities to improve vaccine acceptance and uptake in Canada.
Offers access to latest evidence-informed products, resources, and tools on immunization.
Canadian Pediatric Society (CPS)
Provides online education opportunities and clinical guidelines for vaccine providers.
Provides parents and caregivers information regarding vaccinations.
Canadian Association for Immunization Research and Evaluation (CAIRE)
Supports vaccinology research and the development and evaluation of immunization programs in Canada.
Biologics and Genetic Therapies Directorate (BGTD), Health Canada
Regulates and assesses the use of bacterial and viral vaccines.
Collaborates with other branches/directorates in Health Canada and the Public Health Agency of Canada to monitor safety and effectiveness.
Table 2.7: Organizational Landscape of Vaccine Research, Delivery, and Evaluation – Provincial
Provincial and Regional
Organization
Role in Immunization Delivery
Public Health Ontario
Provides annual surveillance reports on immunization coverage, vaccine safety, etc.
Provides resources on vaccine-preventable disease.
Local Public Health Units
Provides annual surveillance reports on immunization coverage and vaccine-preventable diseases.
Provides immunization clinics and resources for healthcare providers, parents and caregivers.
Table 2.8: Organizational Landscape of Vaccine Research, Delivery, and Evaluation – International
International
Organization
Role in Immunization Delivery
World Health Organization (WHO)
Provides annual surveillance reports on global immunization coverage, and global vaccine action plan reports.
Provides guidelines and recommendations on immunization standards, immunization schedules, vaccine quality, vaccine reference preparations, and regulation.
Organizes World Immunization Week campaign.
Centre for Disease Control (American)
Establishes National Vaccine Advisory Committee (NVAC).
Advises on Immunization Practices.
Pan American Health Organization (PAHO) (WHO for the Americas)
Prevents and controls vaccine-preventable diseases through mandates and strategies.
Reports immunization coverage and number of vaccine-preventable diseases in the Americas.
Provides communication materials on vaccine-preventable diseases.
Health professionals are trusted sources of information and their recommendations for vaccination go a long way in motivating clients to get vaccinated. Based on age and risk factors, health professionals should consider which vaccines are required for an individual and a family. To obtain informed consent for vaccination, the individual should know about the disease that the vaccine will prevent and the side effects, benefits, and risks of vaccinating. The health professional should notify the patient before the vaccination visit and share materials about vaccine-preventable diseases (VPD) wherever possible. For example, expecting parents can start the conversation about a vaccination series for their infant in the pre-natal period.
On the Day of Vaccination
Begin the visit asking if the client has any questions about the vaccine. Use a presumptive statement, meaning assume the client is ready to vaccinate. This approach is recommended because it normalizes vaccines as an everyday occurrence that is recommended by the healthcare provider rather than an uncommon, fearful event. For example, “Today you will get your vaccine to protect against tetanus.” Clients may respond with hesitancy if they sense the health professional is unsure or not confident about immunization. The best way to convey confidence is by being a knowledgeable provider.
See Table 3.1 about steps and considerations involved in the pre-vaccination checklist. For further information about effective communication strategies, visit Chapter 5 on Vaccine Hesitancy.
Table 3.1: Pre-Immunization Checklist
Steps
Considerations
Assess the client’s current health status.
Is the client pregnant?
Is the client immunocompromised or immunosuppressed? Does the client have any acute or chronic immunocompromising conditions including HIV?
Is there a (suspected) family history of congenital immunodeficiency disorder? (e.g., has the child had failure to thrive and recurrent serious infections?)
Has the client taken any immunosuppressants, including corticosteroids, in the past 3 months or during a current pregnancy?
Has the client received any blood transfusions or blood products in the last year?
Discuss benefits and risks of receiving or not receiving the vaccine.
Has information been provided regarding administration of the vaccine?
Have all questions about benefits and risks been answered completely?
Assess for contraindications and precautions.
Does the client have a history of anaphylactic reaction to vaccines or a component of a vaccine?
Does the client have severe asthma?
Does the client have congenital malformation of the GI tract or history of intussusception (for rotavirus vaccine)?
Has the client had Guillain-Barré syndrome with an onset within 6 weeks of immunization?
Is the client immunocompromised?
Is the client pregnant?
Does the client have active, untreated tuberculosis?
Note: Health professionals need to inform themselves of contraindications for each vaccine respectively. Also assess for client’s health status including age, comorbid conditions, risk factors and travel plans .
Evaluate reactions to previous vaccines.
Has the client ever had a serious reaction (anaphylactic reaction) after receiving a vaccine or is the client aware of any allergies to components of the vaccine (e.g., gelatin, neomycin, thimerosol) or to latex?
Discuss frequently occurring minor adverse events and potential rare severe adverse events.
Have you talked to your client about what to do if they experience an adverse event?
Are you able to identify types of adverse events (e.g., injection site, systemic, allergic, neurological, and other reactions) that require reporting?
Have you familiarized yourself with the most likely timing of these events?
Points of Consideration
A common misconception among health professionals is that vaccination should be postponed in the event of minor or moderate acute illness such as upper respiratory tract infections, otitis media, and mild gastrointestinal illness, or in persons on antibiotic therapy. Generally, clients experiencing mild to moderate acute illness (even with fever) can be vaccinated. The health professional should use their clinical judgment to assess the risk, benefits, and health profile of the client when making a decision to delay vaccination.
Health professionals should obtain consent from the client or the Substitute Decision Maker (SDM) prior to vaccinating. Consent must be informed, voluntary, related to the treatment being proposed, and not obtained through misrepresentation or fraud (College of Nurses of Ontario, 2017). Health professionals should consult their respective regulatory association for further information and guidelines on obtaining consent.
Preparation
Health professionals should ensure the client has met the criteria to vaccinate and screen for any contraindications, potential drug interactions, or precautions (see Chapter 4 on Vaccine Safety). Table 3.2 details criteria the health professional should actively verify prior to immunization. Remind the client that they will need to remain at the healthcare facility for a minimum of 15 minutes after receiving the vaccine in order for potential side effects to be monitored.
Table 3.2: Health Professional Criteria Before Vaccine Administration
Criteria
Ask yourself
The right client, informed consent, and contraindications
Have I confirmed the client’s name and date of birth (DOB)?
In the case of a substitute decision maker (SDM), have I learned their relationship to the client?
Is it appropriate for the SDM to provide consent?
Why am I giving this vaccine?
What is the client’s immunization history?
Have I ensured the client meets the criteria?
Have I verified contraindications, drug interactions, and precautions?
Have I asked about history of allergy and anaphylaxis?
The right age
How old is the client and when should they receive the vaccine?
Have I followed the vaccine schedule?
The right vaccine or diluent
Am I giving the right vaccine?
Does the vaccine need to be reconstituted?
If reconstituting:
Am I using the right diluent provided by the manufacturer?
Has the vaccine been appropriately reconstituted/mixed?
If applicable, have I achieved a uniform suspension?
Have I maintained asepsis when reconstituting and drawing the vaccine into the syringe?
The right dose
Do I know the client’s weight?
Is the dosage appropriate for the client?
The right interval
Have I checked the client’s vaccination history?
Do I know when they last received a live-attenuated vaccine?
The right route, needle length, and technique
Do I know the client’s age?
Have I selected the proper needle length and gauge?
Have I verified the right route for administration?
Does the client have significant nasal congestion if administering intranasal vaccine?
The right site
Have I considered the client’s preference?
Have I assessed the client’s injection site for appropriateness?
The right time
Is now the best time to give the vaccine?
Can I reduce the number of visits for the client?
Is the client eligible for a vaccine given their current health status?
Can I use this opportunity to update the client’s immunization status?
The right storage
Have I verified the identification label of the vial?
Have I checked that the vaccine was stored properly?
Have I checked the expiry date?
Have I checked the lot number?
Is the vaccine in the original packaging?
Does the vial have any irregularities, damage, or noticeable contamination?
The right comfort
Have I properly ensured comfort for the client?
Have I given the client and/or caregiver instructions to reduce pain and/or anxiety?
Have I assessed for anxiety and/or concern?
The right documentation
Have I properly documented the vaccination, site, lot number, and expiry date?
Did I give the client a copy of the vaccination for their own records?
Did I notify the client about watching for side effects and who to notify if they have any?
Health professionals are responsible for minimizing the spread of illness and disease and should incorporate routine infection control practices before, during, and after administering vaccines. Perform hand hygiene at regular intervals, like before preparing the vaccine, after removing gloves, when hands are soiled, etc. Gloves are not routinely used when vaccinating unless your own hands are not intact (e.g., your hands have an open wound, rash), or if the client has an open wound, rash, or bodily fluids near the injection site. Use of gloves may prevent proper hand hygiene between patients. Keep a safe and clean environment. Avoid surfaces that are dirty or potentially contaminated. Separate empty vials and dispose in designated waste management system (sharps container). Before injection, cleanse the skin with an alcohol preparation pad and allow for the alcohol to dry. If alcohol is unavailable, use soap and water.
Vaccine Preparation
When preparing vaccines, it is important for healthcare professionals to follow aseptic technique when accessing vials. Vaccines must be withdrawn from the vial immediately before use and generally should be administered by the same person. Do not pre-load syringes as a routine practice. Pre-loading syringes has the potential to disrupt vaccine stability, increase vaccine administration errors and wastage, as well as increase risk of contamination. Before withdrawing content of a vial into the syringe, wipe the access diaphragm (also referred to as the stopper) with an alcohol preparation pad (70% alcohol) while using friction. Allow the alcohol to dry before inserting the syringe. Always use a sterile syringe to withdraw from vial. When withdrawing, hold the vial upside down and aspirate required quantity into syringe. Once the vaccine is drawn, immediately withdraw the needle from the vial and expel any air bubbles. Safety-engineered needles are preferable to avoid needle stick injuries. If vaccines are pre-filled by the manufacturer, do not transfer to safety-engineered syringe.
Single-dose Vials
Single-dose vials are manufactured for one-time use. They should not be reused, and the leftover contents should not be pooled. Single-dose vials are preferred because they minimize the risk of transmission of pathogens and vial contamination.
Multi-dose Vials
Multi-dose vials contain more than one dose of the vaccine and often contain an antimicrobial preservative to prevent bacterial growth. The number of doses per vial varies. For example, IMOVAX Polio multi-dose vial contains ten doses. Health professionals should always label the date of first use and discard open multi-dose vials according to the manufacturer monograph or within 28 days, whichever is shorter. If contamination is suspected, discard multi-dose vials immediately.
Vaccine Reconstitution
Reconstitution is the process involved when vaccines need to be mixed with a diluent. Some manufacturers use concentrated freeze-dried powder (also called lyophilized vaccine) that requires a liquid diluent. Vaccines should always be reconstituted per manufacturer guidelines with the diluent provided by the manufacturer. Examples of diluents are sterile water, sodium chloride and an adjuvant suspension. The majority of vaccines must be administered immediately after reconstituting. Some vaccines can last up to 24 hours after reconstitution (example Hiberix [Hib]). Health professionals should consult the monograph for recommended time between reconstitution and use. When reconstituting vaccines, the health professional should introduce the diluent down the side of the vaccine vial and not directly into the vaccine powder. Mixing should be done carefully in a swirling motion until the suspension is uniform.
Points of Consideration
A separate sterile needle and syringe should be used for each injection. Health professionals should not mix vaccines in the same syringe unless explicitly specified by the manufacturer.
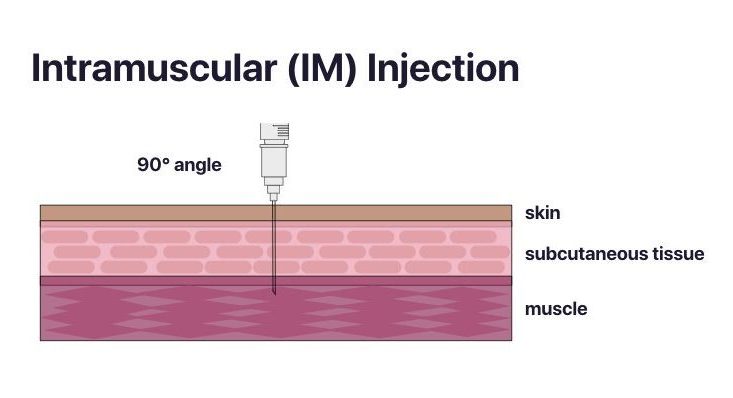
Depending on the vaccine dose, health professionals should use a 1 mL or 3 mL syringe. Depending on the site of administration, it is important to select the right needle size to optimize the immune response and reduce the risk of injection site reactions. For example, vaccines with adjuvants need to be injected into the muscle and not the subcutaneous tissue to prevent inflammation and formation of granulomas. Furthermore, vaccine absorption can be impaired if the vaccine is inadvertently injected into lymphatic circulation. When selecting a needle length for an intramuscular (IM) injection, consider a length that is long enough to reach deep tissue without involving underlying bone, nerves, or blood vessels. Longer needles often result in less redness and swelling when compared to shorter needles. The selection of the right needle should be determined by: 1) route of administration; 2) the client’s age and size of muscle mass; 3) viscosity of the vaccine or passive immunizing agent. Table 3.3 offers needle selection guidelines to inform clinical judgement, which are then visualized in Images 3.2 and 3.3. It is important to note that the needle size recommendations are based on the practice of having the skin stretched flat between thumb and forefinger at the time of administration.
Table 3.3: Needle Selection Guidelines
Route of Administration
Needle Gauge
Age of vaccine recipient
Site of injection
Needle Length
Intradermal (ID)
26-27
All ages
1.0 cm
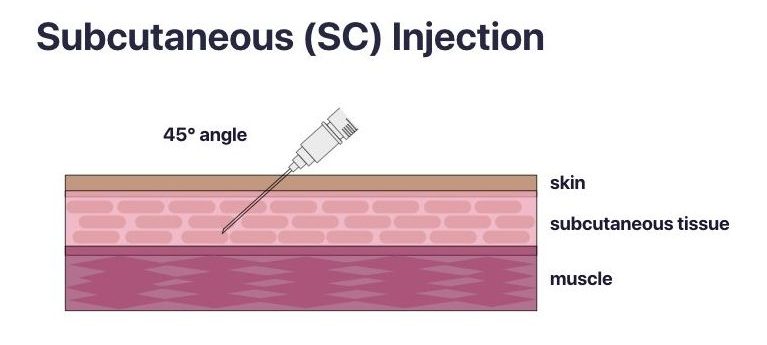
Subcutaneous (SC)
45 degree angle
25
All ages
< 1 year: anterolateral thigh
≥ 1 year: upper triceps area or anterolateral thigh
1.6 cm
Intramuscular (IM)
90 degree angle
22-25
Newborn (>28 days) and preterm infants
Anterolateral thigh
1.6 cm
Infants (1 – 12 months)
Anterolateral thigh
2.2 – 2.5 cm
Young children (>12 months – 3 years)
Deltoid muscle
1.6 – 2.5 cm
Anterolateral thigh
2.5 – 3.5 cm
Children (>3 – 12 years)
Deltoid muscle
1.6 – 2.5 cm
Anterolateral thigh
2.5 – 3.5 cm
Adolescents (>12 years – 18 years)
Deltoid muscle
Consult weight-based recommendations
Anterolateral thigh
2.5 – 3.2 cm
Deltoid muscle
For those weighing <130 lbs (<60 kg):
1.6 cm – 2.5 cm (⅝ inch – 1 inch)
Males weighing 130 – 260 lbs (60 – 118 kg)
and females weighing 130 – 200 lbs (60 – 90 kg):
2.5 cm (1 inch)
Males weighing >260 lbs (118 kg) and females weighing >200 lbs (90 kg):
Health professionals should indicate the vaccine type, route, amount, expiry date, and lot number when documenting. As per professional standards, all documentation should be legible, descriptive, specific, and signed. Health professionals should also document the client’s reaction to the vaccine and update the client’s immunization card if available.
Site and Route
32
The recommendations for the site and route for each vaccine are evidence-informed. Health professionals should adhere to instructions outlined in the vaccine monograph. Vaccine efficacy may decrease and the risk for local adverse events may increase if not administered correctly. See Table 3.4 for additional considerations for route of administration.
Table 3.4: Considerations for Route of Administration
Route
Consideration
Intramuscular
Inactivated vaccines are typically administered via IM injection because most contain adjuvants that can cause exaggerated local pain, swelling, and redness if not injected into the muscle.
In general, vaccines containing adjuvants are administered IM to reduce local adverse effects, such as skin irritation.
Insert needle at a 90 degree angle.
Subcutaneous
Pinch up a fold of skin to more easily access the fatty tissue above the muscle. Avoid injecting into the muscle tissue.
Always inject at a 45 degree angle.
Intradermal
This route is product-specific and should only be administered according to the product monograph.
Hold the skin taut. Place the needle almost flat against the patient’s skin with bevel up. Insert needle at a 5 to 15 degree angle.
Oral
Oral vaccines should be given prior to injectable vaccines. If an incomplete dose is given for any reason, a replacement dose should not be given. Oral vaccines may be given through a client’s NG or NJ tube.
Intranasal
The live-attenuated influenza vaccine is the only intranasal vaccine in Canada. It should be administered by a health professional (not a parent). If the client sneezes (or spits up) a repeat dose is not necessary. Intranasal vaccines should be deferred if the client has severe nasal congestion.
Points of Consideration
When immunizing young children, it is helpful for health professionals to remind parents or substitute decision makers (SDMs) about the upcoming vaccination and explain the site and route anticipated for the next visit. This will allow parents who want to prepare their children with analgesic patches to place them in the correct location (should be applied one hour before vaccine administration). It will also allow a parent to talk to the child about the vaccination before hand.
Health professionals play an important role in minimizing pain and distress for clients. Indeed, if comfort measures are not addressed, it can lead to fear and avoidance for future interventions. According to Health Canada, it is estimated that 25% of adults have a fear of needles and as many as 10% have a needle phobia. Often persons develop fears of needles in early childhood. Healthcare providers should provide the most painful vaccine last, administer simultaneous vaccines as one if possible, and instruct clients to avoid aspirin or other blood thinners before vaccines. Table 3.5 lists specific pain management strategies by age group.
Coach the parent/caregiver to remain calm (e.g. take deep breaths). Babies and children feel what their parents feel.
Offer praise. Positive reinforcement works for kids of all ages.
Infants and young children (≤ 3 years)
Educate parent/caregiver about pain management before and on the day of immunization.
Parents/caregivers may purchase over-the-counter topical anesthetics prior to vaccine injection. It is important to communicate the injection site to parents/caregivers and to place anesthesia patch in advance.
Encourage parent/caregiver to stay with child during vaccine injection.
Parents can make it easier for their baby by cuddling, distracting them with singing, and breastfeeding before, during and after vaccine injection (≤ 2 years of age).
If the infant/young child is not breastfed during vaccine injection a combination of other strategies may be used, such as:
Skin-to-skin contact during vaccine injection (≤1 month of age).
Holding during vaccine injection.
Administration of a sweet-tasting (sucrose or glucose) solution 1-2 mins prior to vaccine injection (≤ 2 years of age).
Toddlers
Educate parent/caregiver about pain management before and on the day of immunization.
Parents/caregivers may purchase over-the-counter topical anesthetics prior to vaccine injection. It is important to communicate the injection site to parents/caregivers and place anesthesia patch in advance.
Parents/caregivers can help their toddler by holding them in a comforting hug, distracting them with a favourite toy, blanket, song, or book, and telling them they may feel a ‘poke or pinch’ for a few seconds.
Encourage parent/caregiver to stay with child during vaccine injection (≤ 10 years of age).
Have toddler sit up during vaccine injection.
Children (3-12 years)
Educate parent/caregiver about pain management before and on the day of immunization.
Educate individual about pain management for vaccine injection on the day of immunization.
Parents/caregivers may purchase over-the-counter topical anesthetics prior to vaccine injection. It is important to communicate the injection site to parents/caregivers and place patch in advance.
Clients/parents/caregivers can make it easier by bringing something distracting, taking deep breaths, and telling them they may feel a ‘poke or pinch’ for a few seconds.
Encourage parent/caregiver to stay with child during vaccine injection (≤ 10 years of age).
Have child sit up during vaccine injection.
Adolescents (12-17 years)
Educate parent/caregiver about pain management before and on the day of immunization.
Educate individual about pain management for vaccine injection on the day of immunization.
Encourage the client to have something distracting like music or a mobile device.
Have adolescent sit up during vaccine injection. If there is a risk of fainting, then consider vaccination while supine, or have adolescent lay supine after vaccination.
Adults (≥ 18 years)
Educate individual about pain management for vaccine injection on the day of immunization.
Have adult sit up during vaccine injection.
Points of Consideration
Give the most painful vaccine last. Vaccines that are known to cause the most injection site pain are pneumococcal-C-13, MMR, and HPV vaccines. These vaccines should be administered last, after other vaccines if multiple vaccines are given at one visit.
If the health professional has administered a vaccine by injection, apply light pressure to the site for several seconds with a dry cotton ball to minimize bleeding. Adhesive bandages or cotton balls with tape are optional but avoid any blood from staining clothing. Clients should be kept under observation for at least 15 minutes after vaccination and preferably 30 minutes when a specific concern is present. Inform client to take oral analgesics such as acetaminophen or ibuprofen as needed for minor adverse reactions following vaccination. Health professionals should remind clients to report any concerns following immunization. The provider can assess the concerns and determine if it is appropriate to report an adverse event following immunization (AEFI).
Vaccine Storage and Handling
35
Vaccines must be carefully stored and handled from the time of manufacturing to administration. Health professionals need to be cognizant of the harmful impact that excessive heat and cold can have on vaccines, rendering them ineffective or destroyed. Errors in storage or handling also contribute to vaccine wastage. Consult the product monograph or local public health authority for information on proper storage conditions for each vaccine, including temperature. As a health professional, it is important to review the policies and procedures developed by the Public Health Agency of Canada (PHAC) (2015) and your provincial/territorial Ministry of Health and Local Public Health organization.
PHAC (2015) outlines a set of procedures to follow when handling and storing vaccines. These procedures include but are not limited to:
Each office/location should have an identified staff member who is the primary vaccine coordinator and another member as a backup. Both should be fully trained in vaccine storage and handling protocols.
Always refer to the vaccine product monograph for the most current information about storage information.
Refrigerators and freezers, used for vaccine storage, must be dedicated to the storage of vaccines only. They should be placed in an area that is not accessible to the public.
Refrigerators and freezer units must have a calibrated temperature monitoring device that provides continuous recording or minimum/maximum temperatures that are properly monitored, i.e. checked and documented twice a day.
The majority of vaccines should be stored in a refrigerator at temperatures of +2 to +8 degrees Celsius. Some vaccines must be kept in a freezer at temperatures of -15 degrees Celsius or lower. Doors of units should be kept closed and opened a limited number of times.
Units should have a sign that says: “Do not adjust refrigerator or freezer temperature controls. Notify primary vaccine coordinator or the backup/delegate coordinator if adjustments are necessary.”
Vaccines should be placed in labelled, mesh baskets and stored in the middle of the unit rather than in doors or drawers. Stock should be rotated so that vaccines with approaching expiry dates are positioned at the front and used first.
Vaccines are stored in their original packaging.
Some vaccines are light sensitive and health professionals should refer to the product information of each vaccine to determine restrictions.
Each site must have a contingency plan in place for vaccine storage in the event of electricity disruptions or unit malfunctions. If procedures have not been adhered to, and/or the temperature decreases in the required unit, notify the primary vaccine coordinator at your site and the local public health unit.
Canada has one of the best vaccine safety programs in the world. There is a strong system in place to monitor the safety of vaccines. Every batch of vaccine is tested according to strict guidelines for safety and quality before it is used. After vaccines are given, severe or unusual reactions are monitored by public health agencies at the local, provincial, and national level.
Health professionals play an important role in the implementation and evaluation of vaccines throughout the vaccine life cycle. When health professionals are knowledgeable about the rigour of vaccine testing both pre and post-licensure, it positions them to have informed conversations with clients and respond to concerns related to vaccine safety. Before any vaccine is approved for use in Canada, it must meet numerous requirements including in-depth scientific reviews on efficacy, stability, teratogenicity, toxicity, and safety. After vaccines have been licensed for use, rigorous evaluation continues to ensure ongoing safety. Post-marketing surveillance of adverse events following immunization add to the continuous safety checks following vaccine licensure.
Before Health Canada issues a notice of compliance (NOC) (commonly known as a “license”) the vaccine must meet a number of sequential tests. During clinical trial phases, the number of subjects participating in the vaccine study increases incrementally, making the population being studied more heterogenous as the phases advance. Regulatory oversight occurs at each stage to ensure safety and identify possible risk. A condensed version of the various stages of pre-license approval are described in Table 4.1. The vaccine is considered for licensing (also referred to as “authorized for marketing”) once it has a proven positive benefit-to-risk profile.
Table 4.1: Pre-License Evaluation Stages
Life Cycle Phase
Regulatory Requirements
Description
Pre-clinical testing
Food and Drugs Act and Regulations, Good Laboratory Practice (GLP)
Provides information on efficacy and safety in laboratory and animal testing.
Clinical trials
Food and Drugs Act and Regulations, Good Clinical Practice (GCP)
Provides safety and efficacy data on humans in different phases of trial.
Phase I (10-99 subjects): very common adverse reactions (occurring in 10% or more of doses).
Phase II (100-1,000 subjects): common adverse reactions (occurring in 1% to less than 10% of doses).
Phase III (1,000-30,000 subjects): uncommon (occurring in 0.1% to less than 1% of subjects) and some rare (occurring in 0.01% to less than 0.1% of subjects) adverse reactions.
Validation of manufacturing process and control
Food and Drugs Act and Regulations, including Good Manufacturing Practice (GMP) as well as World Health Organization, International Conference on Harmonization, and other international quality guidelines
Assesses quality of vaccine production process.
Applies to all steps in the manufacturing process from seed lot production to delivery as well as quality control tests. Documentation on production process, quality control, and facilities must be submitted to the regulator for review prior to approval.
On-site evaluation of the manufacturing process
Food and Drugs Act and Regulations, including Good Manufacturing Practice (GMP) as well as with World Health Organization, International Conference on Harmonization, and other international quality guidelines
Monitors and ensures quality of vaccine production. Health Canada product specialists are sent to the manufacturing site to assess the manufacturing process.
Consistency testing
Food and Drugs Act and Regulations, including Good Manufacturing Practice (GMP)
Ensures quality of vaccine. Samples from at least three consecutive lots are tested in Health Canada laboratories to ensure that the product is manufactured consistently.
Establishing licensing
Food and Drugs Act and Regulations, including Good Manufacturing Practice (GMP)
Ensures that the facilities in which the product (the active pharmaceutical ingredient) is manufactured are appropriate to the specifications that apply to that product.
Under the Food and Drugs Act (1985) and Regulations, pharmaceutical companies are legally required to report serious adverse reactions related to a vaccine. The Canada Vigilance Program offers oversight after vaccines have been licensed, with systemic safeguards to ensure that vaccines have continued monitoring. The program includes safety reports, surveillance systems, risk management plans, and product risk/benefit assessments.
Safety Reports
According to the Food and Drugs Act (1985), pharmaceutical companies are required to prepare an annual report that comprehensively analyzes all adverse drug reactions occurring anywhere in the world. Drug companies are also responsible for notifying Health Canada if they become aware of any significant issues that could affect the benefit-risk profile.
Canadian Adverse Events Following Immunization Surveillance System (CAEFISS)
All health professionals must report adverse events following immunization (AEFI) to local authorities, who report to provincial authorities, who in turn report to federal authorities. CAEFISS is responsible for using this information for ongoing safety monitoring and AEFI investigations in Canada. An AEFI may or may not have a causal relationship to the use of the vaccine.
Evaluation of Vaccines Post-License
The safety profile of a vaccine is heavily scrutinized before licensure. Rigorous monitoring and evaluation continues once the vaccine is available to the general population to identify potential rare side effects and frequency of adverse events following immunization. This period is often referred to as the post-marketing period because the vaccine continues to be monitored after it is licensed. Table 4.2 outlines the various stages of post-license evaluations.
Table 4.2: Post-License Evaluation Stages
Life Cycle Phase
Regulatory Requirements
Description
Lot release program
Food and Drugs Act and Regulations
Ensures that each marketed lot of vaccine does not differ from vaccine lots shown to be safe and effective in clinical trials.
Establishment inspections
Food and Drugs Act and Regulations, including GMP
Ensures that the facilities in which the product (the active pharmaceutical ingredient) is manufactured are appropriate to the specifications that apply to that product. Generally, inspections occur every two to three years; however, inspections can be more or less frequent depending on the activity and product.
Post-marketing studies
Not required by regulation, but suggested by Health Canada. Researchers may conduct large studies to test causal relationship between a vaccine and adverse events.
Phase IV (≥ 100 thousand subjects). Expand data on vaccine safety profile in target population to identify rare adverse events not detected during pre-marketing phase.
Assess safety profile in special populations not studied as part of pre-authorization trials (e.g., immunocompromised, diabetics, etc.).
Study possible interactions with other vaccines.
Adverse Events Following Immunization (AEFI) surveillance systems
Food and Drugs Act and Regulations by market authorization holders. CAEFISS activities are undertaken voluntarily, although some jurisdictions require AEFI reporting as part of public health legislation.
Detect new vaccine safety signals which could be:
increased severity or frequency of previously known adverse reactions.
unexpected adverse reactions.
Conduct special investigations to determine root cause of vaccine safety signals.
Studies designed to test hypotheses related to vaccine adverse event association
May be requested by regulators in response to new safety signals.
Test hypothesis that a vaccine can cause an AEFI, including very rare events.
AEFIs should be reported:
When the event has a temporal association with a vaccine. A causal relationship does not need to be proven before reporting.
When the event is serious or unexpected (e.g., life threatening or results in death, requires hospitalization or prolongation of an existing hospitalization, results in residual disability, or causes congenital malformation).
If there is any doubt as to whether or not an event should be reported, health professionals should always choose to report the event.
Table 4.3 is an example of a protocol for reporting adverse events. Each province and territory has their own reporting system outlining local and provincial/territorial activities. It is important that health professionals know what and how to report in their jurisdiction. The Public Health Agency of Canada has a national reporting form that is available. Completed forms are sent to the local public health unit. All reports are eventually reported up to CAEFISS at a national level.
Table 4.3: Adverse Event Type Requiring Reporting
Adverse Event Type
TEMPORAL CRITERIA
for Non-live vaccines
TEMPORAL CRITERIA
for Live vaccines
Injection Site Reactions
Pain, redness, or swelling lasting 4 days or more OR extending beyond the nearest joint
0 to 48 hours
0 to 48 hours
Infected abscess
0 to 7 days
0 to 7 days
Sterile abscess
0 to 7 days
0 to 7 days
Nodule
0 to 7 days
0 to 7 days
Cellulitis
0 to 7 days
0 to 7 days
Systemic Reactions
Rash
0 to 7 days
5 to 42 days
Adenopathy/lymphadenopathy
0 to 7 days
5 to 42 days
Severe vomiting/diarrhea
0 to 72 hours
0 to 42 days
Parotitis
N/A
5 to 30 days
Hypotonic-hyporesponsive episode (HHE); under 2 years of age only
0 to 48 hours
0 to 48 hours
Persistent crying/screaming; under 2 years of age only
0 to 72 hours
0 to 72 hours
Allergic reactions
Event managed as anaphylaxis (i.e., epinephrine administered)
0 to 24 hours
0 to 24 hours
Oculorespiratory Syndrome (ORS)
0 to 24 hours
0 to 24 hours
Allergic skin reaction (e.g., hives)
0 to 48 hours
0 to 48 hours
Neurologic events
Convulsions/seizure
0 to 72 hours
5 to 42 days
Encephalopathy/encephalitis
0 to 15 days
5 to 42 days
Meningitis
0 to 15 days
5 to 42 days
Anaesthesia/paraesthesia
0 to 15 days
0 to 42 days
Paralysis
0 to 15 days
5 to 42 days
Myelitis/acute disseminated encephalomyelitis
0 to 15 days
5 to 42 days
Guillian Barré Syndrome (GBS)
1 to 8 weeks
1 to 8 weeks
Bell’s palsy
0 to 3 months
0 to 3 months
Other events of interest
Arthritis/arthralgia
0 to 15 days
1 to 3 weeks
Intussusception
N/A
0 to 42 days
Thrombocytopenia
0 to 30 days
0 to 30 days
Syncope (fainting) with injury
0 to 30 minutes
0 to 30 minutes
Other severe/unusual events
Reportable regardless of timeline
Reportable regardless of timeline
As a health professional, it is important to monitor adverse events and follow the steps below:
Step 1
Advise clients to contact you or your team if they experience an adverse event after vaccination.
Step 2
Complete either the local form or the Public Health Agency of Canada form for reporting an AEFI. A user guide is available.
Submit the completed form to the local public health unit or consult them if you have any questions.
Table 4.3 was adapted with editorial changes from “Adverse Event Following Immunization Reporting for Health Care Providers in Ontario” by Public Health Ontario. Contact the copyright holder for appropriate permission.
Non-Severe Events
44
It is always important to assess the client after administering a vaccine. Health professionals need to recognize the difference between severe events such as anaphylaxis (see next section) and non-severe events that may occur immediately after vaccine administration. Table 4.4 outlines some symptoms that may seem severe and mimic the signs of anaphylaxis but do not pose a life-threatening risk.
Table 4.4: Non-Severe Events
Non-Severe Event
Description
Management
Fainting
A client who faints suddenly becomes pale, diaphoretic (sweaty), nauseous, and may collapse or experience brief loss of consciousness.
Fainting may occur before or after an injection. Fainting is sometimes accompanied by a brief clonic seizure activity (i.e., rhythmic jerking of the limbs).
PREVENT: If you observe early signs of fainting, encourage the client to sit on the floor or lay down to avoid injury from fall in the event of loss of consciousness.
RECOGNIZE: Recovery of consciousness usually occurs within a minute or two, but the person may remain pale, diaphoretic, and mildly hypotensive for several minutes.
RESPOND: Put the client in the recumbent position. Assess the client for injury.
REASSURE: Reassure client and family.
Anxiety
A client experiencing anxiety may appear fearful, pale, and diaphoretic (sweaty). They may also indicate feeling light-headed, dizzy, and numb or tingly in the face and/or extremities. The client may hyperventilate.
PREVENT: If you observe early signs of anxiety, offer the client reassurance and let them know you will not leave them alone.
RECOGNIZE: Symptoms of acute anxiety are stressful for the client but will pass.
RESPOND: Demonstrate calm breathing (diaphragmatic breathing) for the client and encourage them to do the same. It will help the client slow down their breath.
Breath-holding
Young children may hold their breath when they are upset and crying hard. The child may appear suddenly silent but visibly agitated. Facial flushing and perioral cyanosis deepen as breath-holding continues.
PREVENT: Use comfort and evidence-informed measures to prevent pain from injection.
RECOGNIZE: Some spells end with resumption of crying, but others end with a brief period of unconsciousness during which breathing resumes.
RESPOND: Encourage parent/caregiver to distract the child if possible. Never scold a child for breath-holding.
Points of Consideration
Health professionals are encouraged to be proactive and report adverse events when they are uncertain whether the event is caused by the vaccine. Expected and mild events that do not require reporting include: fever without any other symptoms, injection site reaction that lasts less than four days, vasovagal syncope (fainting) without injury, or events that are clearly related to other causes.
Anaphylaxis
45
Anaphylaxis is a potentially life-threatening allergic reaction resulting from exposure to an allergen. Although anaphylaxis is extremely rare (one per one million doses administered), health professionals who administer vaccines need to know the signs and symptoms of anaphylaxis and how to administer appropriate interventions without delay.
Signs and symptoms of anaphylaxis (see Table 4.5) typically develop within minutes of exposure to an allergen. In fact, most instances of anaphylaxis occur within the first 30 minutes of exposure to an allergen, although some reactions may develop later. Clinical signs involve at least two body systems to classify the reaction as anaphylaxis. It is important for providers to recognize that symptoms of anaphylaxis vary, but the treatment is the same. Severe anaphylaxis includes obstructive swelling of the upper airway with bronchospasms and hypotension. A sudden drop in blood pressure can cause shock and loss of consciousness. If a client loses consciousness it is rarely the only manifestation of anaphylaxis and is typically a late event.
Table 4.5: Anaphylaxis Signs and Symptoms
Body System
Likelihood system is part of anaphylactic response
Signs and Symptoms
Skin/Mucosa
80-90%
Itchy, urticaria (hive) rash.
Progressive, painless swelling (angioedema) around the face and mouth, which may be preceded by itchiness, tearing, nasal congestion, or facial flushing.
Respiratory
70%
Sneezing, coughing, wheezing, labored breathing, and upper airway swelling (indicated by hoarseness and/or difficulty swallowing) possibly causing airway obstruction.
Gastrointestinal
45%
Crampy abdominal pain, nausea, and vomiting.
Cardiovascular
Up to 45%
Chest pain, palpitations, tachycardia, sudden reduction in blood pressure, or symptoms of end-organ dysfunction (e.g. hypotonia and incontinence). In infants symptoms may also include fussiness, irritability, drowsiness, or lethargy.
Central Nervous System
Up to 15%
Uneasiness, altered mental status, dizziness, or confusion.
Points of Consideration
During the consent phase, all clients should be screened for contraindications, including a previous history of anaphylaxis to any vaccine. Screening for contraindications is of utmost importance. All clients should be reminded to stay for at least 15 minutes after vaccination to monitor for side effects.
Responding to Anaphylaxis
Health professionals should review their institutional policies for medical directives in the management of anaphylaxis and know where to access an anaphylaxis management kit. Epinephrine is the treatment of choice for anaphylaxis. Prompt administration of epinephrine is the priority and should not be delayed because failure to administer epinephrine promptly could result in serious anaphylaxis. The risk of administering epinephrine inappropriately is less severe than anaphylaxis. If uncertain, err on the side of treatment; there are no contraindications to the use of epinephrine. If time is lost early in the treatment of an acute anaphylactic episode, subsequent management can become more difficult.
Some basic procedures for responding to anaphylaxis are outlined in Table 4.6.
Table 4.6: Procedure for Responding to Anaphylaxis
Assess
Assess for airway, breathing and circulation (ABCs), level of consciousness (LOC)/mental status, and approximate body weight.
*Respond to ABC and LOC as per the program specific policies and procedures outlined by your institution.
Call for Assistance
Depending on your institutional policies, calling for assistance may require you to call 9-1-1, use the emergency call bell, or call for a colleague. Be prepared and know what you should do in an emergency.
Position
If the client is in respiratory distress, place them in the recumbent position or a position of comfort. If the client is vomiting or unconscious place them on their side. If the client is pregnant place them in a semi-recumbent position on their left side with legs elevated.
Intervention
Refer to your institutional policies for protocols on the management of anaphylaxis. Know who is responsible for injecting epinephrine intramuscularly. Refer to guidelines and site protocol. Record time and dose. Monitor for repeat dose.
A general guide is:
Inject epinephrine intramuscularly in the mid-anterolateral aspect of the thigh: 0.01 mg/kg body weight of 1:1000 (1 mg/mL) solution
ADOLESCENT or ADULT: maximum – 0.5 mg
CHILD: maximum – 0.3 mg
Monitoring
If applicable, notify the client’s next of kin. Monitor and record vital signs every five minutes and reassess frequently. Ensure client remains in recumbent position until transfer. Sudden death can occur quickly if the client sits, stands, or is placed in an upright position suddenly after giving epinephrine. Therefore, it is important for the client to be placed in the recumbent position with their lower extremities elevated and monitored closely after epinephrine is given.
This section was remixed with editorial and content changes from the Canadian Immunization Guide by the Government of Canada and is reproduced under non-commercial conditions.
Vaccine Facts
46
It is important for health professionals to equip themselves with the correct information about vaccines and vaccine safety. Table 4.7 provides quick facts for health professionals to promote evidence-informed discussions about vaccine safety.
Table 4.7: Quick Facts for Vaccine Safety
Quick Fact
Description
Vaccines are the most effective way to protect against vaccine-preventable diseases.
Vaccines protect individuals and communities, especially people who are unable to receive vaccines due to medical conditions or age.
Vaccines are a cost-effective strategy.
Vaccines train the immune system to defend rapidly against vaccine-preventable diseases.
Children are naturally exposed to many antigens; vaccines do not significantly add to their daily exposure.
Vaccines help the body develop defenses against serious diseases.
Vaccines are safe.
Vaccines have been extensively tested in Canada.
Health Canada supervises all aspects of vaccine production by manufacturers to ensure safety, efficacy, and quality.
Vaccines are rigorously monitored after being authorized for marketing.
Every batch of vaccine is tested for safety and quality.
Canada has a comprehensive vaccine safety monitoring system to alert public health to trends in reporting adverse events following immunization.
Ongoing quality and safety monitoring occurs after vaccines have been administered.
The risks of vaccine-preventable diseases are many times greater than the risk of serious adverse reaction following immunization.
Serious adverse events are rare and are outweighed by the risk of the diseases and their complications.
Effective treatments for many vaccine- preventable diseases such as polio do not exist.
Most adverse events are minor and resolve quickly (e.g. injection site reaction).
Vaccine recipients are observed for 15 minutes to watch for signs and symptoms of adverse reactions.
Vaccines are not linked to chronic conditions like autism, multiple sclerosis, asthma, or sudden infant death syndrome.
There is no evidence that any vaccines cause chronic illnesses. This has been tested in large population studies and continues to be studied.
Multiple injections are an effective way of ensuring up to date immunization.
Evidence has shown that multiple injections at one visit cause less pain, discomfort, and disruption than waiting several days between vaccines.
Generally, infants have similar immune responses whether vaccines are given at the same time or different visits.
Vaccine-preventable diseases can occur at any time.
Even if a disease is uncommon in Canada, it can be imported from other countries to Canada by travellers. For example, outbreaks of measles in Canada continue to occur from importation of measles cases abroad.
Unvaccinated people have a much greater chance of getting a vaccine-preventable disease.
It may not be possible to avoid exposure to a vaccine-preventable disease. For example, an unvaccinated person can get measles by breathing the air in a room that was occupied hours before by a measles-infected person.
Vaccine-preventable diseases re-appear quickly if immunization coverage drops.
There is potential for re-emergence of vaccine-preventable diseases when vaccine coverage rates are low.
Vaccines may contain additional substances to ensure effectiveness and safety. These substances are safe.
The main ingredients of vaccines are killed or weakened viruses or bacteria or their parts. Parts are called antigens and they train the immune system to recognize and prevent disease.
Additional substances may be required in the vaccine to ensure effectiveness and safety.
Very small amounts of preservatives, such as phenol, 2-phenoxyethanol, or thimerosal, may be added to a vaccine to prevent the growth of other disease-causing microbes in the vaccine when it is used.
What do health professionals need to know about vaccine safety?
How can health professionals best communicate information about vaccine safety to clients?
Key Takeaways
48
The key takeaways of this chapter are:
Vaccine safety is a highly regulated, scrutinous process in Canada.
Vaccines undergo various stages of research before receiving license issuance by Health Canada.
Vaccine evaluation is ongoing, even after licensure. Post-marketing surveillance is important to ensure vaccines continue to be safe and to detect rare or serious adverse events.
Health professionals are required by law to report adverse events following immunization.
Adverse events following immunization should be reported when the event is serious or unexpected, and there is no other clear cause for the event. A causal relationship is not required to report the adverse event.
Vaccine hesitancy is the reluctance or refusal to vaccinate despite the availability of vaccines (WHO, 2019). The term ‘vaccine hesitancy’ is intentionally used to depolarize antivaccine rhetoric (Larson et al., 2014). Several factors have been cited as contributing to vaccine hesitance including heuristic thinking, the success of vaccination, the perceived unnaturalness of vaccines, the scientific method that can sometimes produce conflicting results, the suspicion of pharmaceuticals or biological materials, the presence of adjuvants in vaccines, and loss of public confidence (Jacobson, Sauver, Rutten, 2015). It is important for health professionals to recognize that given all these factors, there is no singular form of vaccine hesitancy. Instead, it remains a complex and context specific phenomenon that varies across time, place, and vaccine. People who are vaccine hesitant may not refuse all vaccines. They may ask to delay some vaccines or accept vaccines on a different schedule.
Effects of Vaccine Hesitancy
Vaccine hesitancy has been reported in 90% of countries in the world (WHO, 2019). Outbreaks of preventable diseases such as influenza, varicella, pneumococcal disease, measles, and pertussis have been linked to communities with high vaccine refusal rates. In Ontario, vaccine refusal has been linked to resurgences of rubella and measles outbreaks. Even small declines in vaccine coverage rates translate into significant outcomes. An American study found that a 5% reduction in Measles, Mumps, and Rubella (MMR) vaccination in children aged 2-11 led to a three-fold increase in measles cases with an estimated $2.1 million cost to the public healthcare sector (Lo & Hotez, 2017). Dubé and MacDonald (2016) remind health professionals that while vaccine hesitancy is an important public health issue, it should not eclipse the need for continued encouragement and support the majority of people who vaccinate. Video Clip 5.1 is a recreation of a conversation between healthcare providers exhibiting vaccine hesitancy related to the flu shot.
Video Clip 5.1: Conversation on Vaccine Hesitancy among Health Professionals
In Canada, about 20% of the population is vaccine hesitant, meaning they have some concerns about vaccination but are not firm vaccine refusers (Dubé et al., 2016). They are distinct from vaccine refusers who make up less than 5% of the population.
According to the World Health Organization (WHO) (2019) vaccine hesitancy is influenced by factors such as: confidence, complacency and, convenience.
Confidence
Refers to a lack of trust in the effectiveness and safety of vaccines, the system that delivers them – including the reliability of the health professional – and/or the motivations of policy-makers who make determinations about vaccines.
Complacency
Refers to a low perceived risk of vaccine-preventable diseases and therefore it is assumed vaccines are not needed. Other issues are considered more important.
Convenience
Refers to the degree to which the comfort, convenience, time, place, and quality of a vaccine affects uptake of the vaccine. This continuum ranges from total acceptance to complete refusal. The concern is that hesitancy can lead to refusal, and unvaccinated clusters may emerge as disease outbreaks (Gangarosa et al., 1998; Jansen et al., 2003).
The success of vaccines means that many parents today have not witnessed the serious consequences of vaccine-preventable diseases like polio, diphtheria, tetanus, and measles. This has led parents to worry more about vaccine adverse effects than the consequences of the diseases themselves. Misinformation on social media and the internet about vaccine ingredients and side-effects may also contribute to lack of vaccine confidence.
Points of Consideration
Some parents believe that natural immunity obtained from illness is better than vaccination, giving rise to a controversial phenomenon referred to as “pox parties.” People use pox parties to deliberately infect their children with chickenpox. Children who catch chickenpox at a pox party will experience the full illness with the hopes to avoid the vaccine. Even in healthy children, there is still a risk of complications which may include skin infections, flesh eating disease, pneumonia, encephalitis, or septicemia. Chickenpox also carries greater risks to newborns, pregnant people, adults, and individuals with weakened immune systems. Complications aside, why expose children to the unpleasant experience of fever, itching, difficulty sleeping, scarring, and missing school?
Image 5.1: Nurse and Parent Dialogue about Vaccines
When communicating with a client, it is best to focus your responses on the specific questions or concerns rather than overwhelming the client with too much information. Image 5.1 demonstrates the disconnect that can exist between provider and client priorities and perceptions. It has been well-documented that merely correcting misinformation with more information may not be an effective strategy to increase vaccine uptake. Health professionals should avoid strategies that may reinforce misinformation, such as handouts that describe vaccine myths, repeating misinformation to parents, or using elaborate arguments to contest misinformation (Lewandowsky, Ecker, Seifert, Schwarz, & Cook, 2012). Spending too much time talking about myths can strengthen the myth for the client (McClure, Cataldi, & O’Leary, 2017). Instead, health professionals should invite clients to have healthy skepticism towards vaccine hesitant sources, to focus on facts, and to keep their language simple and clear.
Health professionals are the most trusted advisor and influencer of vaccination decisions. It is important that you have the knowledge, attitude, and skills to work with clients who have questions about vaccines and it is important to understand and acknowledge the client’s concerns. Effective communication is the best way for health professionals to address vaccine hesitancy. Always speak positively about vaccination. If a health professional appears unsure about vaccine safety or cannot explain why vaccination is important, you can contribute to the client’s hesitancy. Here are some tips (Table 5.1) for effectively communicating with all clients about vaccines. See also Video Clip 5.2 for a recreation of a discussion between the healthcare provider and parents displaying vaccine hesitancy.
Table 5.1: Communication Tips to Address Vaccine Hesitancy
Communication Tip
Pointers
Adopt a client-centered approach
Use open body language when talking about vaccines.
Listen to the client’s concerns carefully. Do not interrupt.
Work towards sustained and trusted partnerships with clients.
Take a positive approach towards vaccine behaviours.
Respect difference of opinion about immunizations
Educate yourself about vaccines and common vaccine perceptions in order to engage in knowledgeable discussions.
Understand vaccine safety, schedules, policies, and relevance to best relay this information to your client.
Take a non-judgmental and non-confrontational tone.
Clarify concerns respectfully.
Be patient.
Represent the risks and benefits of vaccines fairly and openly
Be candid when providing an analysis of the risks and benefits.
Familiarize yourself with vaccine safety standards so you can speak accurately and confidently.
Use appropriate language that is understandable.
Compare risks to benefits rather than analyzing risks individually – including risk for vaccine-preventable diseases.
Use clear communication informed by current evidence-informed approaches
Assess the client’s understanding without assumption (including educational status, occupation, lifestyle).
Present evidence in a clear and understandable way.
Use a variety of information formats to introduce or reinforce information.
Reduce stress related to vaccines as much as possible through vaccination pain reduction strategies and combination vaccines when available.
Video Clip 5.2: Health Professional Discussion with Parents who have 2-month old child
There is no panacea to address vaccine hesitancy. Instead, health professionals need to access a variety of tools and approaches to best collaborate with their clients. Presumptive statements and motivational interviewing have been identified as effective tools for communicating about vaccines.
Presumptive Statements
Presumptive statements reinforce vaccination as a normative choice, without inadvertently suggesting that clients should be worried about vaccines. Healthcare professionals can use presumptive statements such as “your child’s next vaccine is due in two months…” or “I see your child is getting the one-year vaccines today.”
Motivational Interviewing
Motivational interviewing (MI) emerged in the 1980s as an approach to establish a safe and open environment for persons managing substance abuse. It is a client-centered approach that supports clients’ motivations to change and addresses internal ambivalence (Miller & Rollnick, 2013). MI was recently applied to vaccine hesitancy because of its appreciative-inquiry qualities. Appreciative-inquiry privileges strengths and motivations of clients, rather than focusing on the negativity of antivaccination. Health professionals should consider the principles of MI as a tool among other strategies. There are five principles of MI: 1) express empathy through reflection; 2) develop discrepancy between client goals, values, and behaviours; 3) avoid argument and direct confrontation; 4) adjust to client resistance rather than opposing it directly; 5) encourage self-efficacy and optimism (Miller & Rollnick, 1991, p. 51-52). This approach relies on health professionals collaborating with clients and actively encouraging their participation in decision making, see Table 5.2 for motivational interviewing tips.
Table 5.2: Motivational Interviewing Tips
Motivational Interviewing Principle
Pointers
Talking Quotes
Express empathy through reflection
Convey respect for the client’s view.
Avoid talking ‘at’ the client, as if a one-way stream of information.
Convey nonjudgment and be mindful of body language and tone.
Recognize that ambivalence is normal.
“I can understand that you want what is best for your child.”
“Tell me more about your concern.”
“Perhaps I can provide some information for you.”
Develop discrepancy between client goals, values, and behaviours
Explore awareness for consequences of not vaccinating (without engaging in scare tactics).
Ask client to consider consequences of not vaccinating.
“Let’s talk about some of the risks of not vaccinating.”
Avoid argument and direct confrontation
Avoid defensiveness and do not take a response personally.
Avoid the use of labels like “anti-vaxer.”
“Let me see if I am understanding you correctly …”
“Let’s talk about your concerns some more.”
Adjust to client resistance rather than opposing it directly
Be hopeful for shifting perceptions.
Recognize that the client is a valuable resource for finding a solution.
“I can appreciate your resourcefulness; let’s talk more about [a specific issue].”
Encourage self-efficacy and optimism
Recognize self-determination.
Focus on positive shifts rather than negative outcomes.
“I think it is positive that you are seeking clarification.”
Table 5.3 provides an overview of helpful strategies for providers to implement when communicating with someone who is vaccine hesitant compared to someone who has refused a (or multiple) vaccines. This is not suggest that these are mutual exclusive ways-of-being, but to highlight that your strategies may shift as a healthcare provider.
Table 5.3: How to respond to vaccine hesitancy vs. vaccine refusal
Vaccine Refuser
Vaccine Hesitant
Do not dismiss
Work on building trust
Do not engage in a debate
Avoid unidirectional information
Ask questions
Do not make assumptions
Listen and understand
Do not overestimate concerns
Engage in active listening
Tailor responses to specific concerns
Addressing Vaccine Hesitancy
56
Although parents use the internet and social media for medical information, they still look to healthcare providers for trusted advice. It is important that health professionals have the knowledge, attitude, and skills to counsel clients who have questions about vaccines. Respectful dialogue between parents and their child’s healthcare provider is crucial to address vaccine hesitancy. Most often, parents express concerns related to vaccine safety and efficacy, and therefore healthcare providers are an important informational resource. It is important to clearly identify the risks and benefits of vaccines.
Growing Your Communication Skills
Effective communication skills can be developed with practice. When learning about the power of one-to-one conversations, you can make use of a number of techniques to strengthen your skills. First, it is important to look within and understand your personal bias. You should have a good sense of population diversity and societal beliefs. Always aim for simplicity and tailor information to match your client’s needs. Use story-telling to make an impact and understand that an emotional perception may be stronger than logic or fact. People may not remember what you said, but they remember what they thought you said.
When Communicating with Parents…
Be presumptive that their child will be vaccinated.
Maintain trust. Be non-judgmental.
Take time to listen. Keep lines of communication open.
Validate parental concerns and correct misinformation.
Acknowledge benefits and risks of vaccines in contrast to risk of disease.
Frame data clearly and positively.
Use clear language that is relevant to your client’s context.
Show parents how the stress of vaccination for their baby/child can be lessened.
Encourage clients to seek credible sources for more information.
Use every visit as an opportunity to discuss vaccines.
When Communicating with Adults…
Use every visit as an opportunity to discuss vaccines.
Include vaccination in adult health education and assessment.
Be presumptive that the client will be vaccinated.
Be non-judgmental.
Listen to your client’s concerns.
Validate concerns and correct misinformation.
Frame data clearly and positively.
Acknowledge benefits and risks of vaccines in contrast to risk of disease.
Use clear language that is relevant to your client’s context.
Encourage clients to seek credible sources for more information.
Address waning immunity in diseases more common to adults.
Assess client risks based on occupation, travel habits, underlying illness, lifestyle, and/or age.
Acknowledge that vaccines for adults may not prevent the onset of disease but will at least reduce disease severity.
Reflective Questions
57
What is vaccine hesitancy and what role do health professionals play in addressing it?
How can health professionals effectively communicate with clients about vaccine hesitancy?
What facts can best support an evidence-informed discussion about vaccines?
Key Takeaways
58
The key takeaways of this chapter are:
Vaccine hesitancy is complex and nuanced. Strategies to address it should reflect this reality.
It is important to communicate effectively with clients through presumptive statements, motivational interviewing, and therapeutic relationship building.
Clear, simple, evidence-informed language about vaccines is an important strategy to mitigate vaccine hesitancy.
Health professionals play an important role in addressing vaccine hesitancy.
Dubé, E., Bettinger, J. A., Fisher, W. A., Naus, M., Mahmud, S. M., & Hilderman, T. (2016). Vaccine acceptance, hesitancy and refusal in Canada: Challenges and potential approaches. Canada Communicable Disease Report, 42(12), 246-251.
Dubé, E., & MacDonald, N.E. (2016). Managing risks of vaccine hesitancy and refusals. Lancet. Infectious Diseases, 16(5), 518-9.
Gangarosa, E. J., Galazka, A. M., Wolfe, C. R., Phillips, L. M., Miller, E., Chen, R. T., & Gangarosa, R. E. (1998). Impact of anti-vaccine movements on pertussis control: the untold story. The Lancet, 351(9099), 356-361.
Jacobson, R.M., Sauver, J.L., Rutten, L.J.F. (2015). Vaccine Hesitancy. Mayo Clin Proc. 90(11), 1562-1568.
Jansen, V. A., Stollenwerk, N., Jensen, H. J., Ramsay, M. E., Edmunds, W. J., & Rhodes, C. J. (2003). Measles outbreaks in a population with declining vaccine uptake. Science, 301(5634), 804-804.
Larson H, Jarrett C, Eckersberger E, et al. (2014) Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature: 2007-2012. Vaccine, 32, 2150–2159.
Lewandowsky, S., Ecker, U. K., Seifert, C. M., Schwarz, N., & Cook, J. (2012). Misinformation and its correction: Continued influence and successful debiasing. Psychological Science in the Public Interest, 13(3), 106-131.
Lo, N.C. & Hotez, P. J. (2017). Public Health and Economic Consequences of Vaccine Hesitancy for Measles in the United States. JAMA Pediatrics, 171(9), 887-892.
MacDonald, N. E., Harmon, S., Dubé, E., Taylor, B., Steenbeek, A., Crowcroft, N., & Graham, J. (2018). Is physician dismissal of vaccine refusers an acceptable practice in Canada? A 2018 overview. Paediatrics & child health, 24(2), 92-97.
McClure, C. C., Cataldi, J. R., & O’Leary, S. T. (2017). Vaccine hesitancy: where we are and where we are going. Clinical therapeutics, 39(8), 1550-1562.
Miller, W. R., & Rollnick, S. (1991). Motivational interviewing: Preparing people to change addictive behavior. New York, NY, US: The Guilford Press.
Miller, W. R., & Rollnick, S. (2013). Applications of motivational interviewing. Motivational interviewing: Helping people change (3rd edition).New York, NY, US: Guilford Press.
R Shen S, Dubey V. (2019). Addressing vaccine hesitancy: Clinical guidance for primary care physicians working with parents. Canadian Family Physician, 65(3), 175-181. http://www.cfp.ca/content/65/3/175
Vaccines are one of the greatest achievements in the history of medicine and continue to save millions of lives every year. But a persistent group of voices – the anti-vaccination movement – is undermining those public health successes by spreading fear and misinformation. In recent years, cases of vaccine-preventable diseases, such as measles, have started to surge in Canada and some developing countries, due in large part to vaccine hesitancy, which the World Health Organization (WHO) has declared a top global health threat.
To understand the risks posed by anti-vaccination activists and how public health professionals can combat the rising tide of misinformation, it is important to examine how this movement evolved and why the methods of anti-vaccination activists are often effective.
The Roots of Anti-Vaccine Activism
The anti-vaccination movement has been around since the invention of vaccines in the late 1700s when the first successful vaccine was developed for smallpox, an infectious disease that killed three out of every ten infected. Throughout the 19th century, anti-vaccination groups formed and held rallies, protests, and even riots to bring attention to false beliefs about vaccines.
Those early anti-vaccine activists argued the vaccine was unsafe and that focusing on better sanitation and hygiene were the real keys to combatting smallpox. The anti-vaccination advocates were well-organized and gained significant public support, as well as favourable coverage in the media, which hampered the rollout and delivery of vaccination programs.
Points of Consideration
In Canada, the smallpox vaccine was discontinued as a routine immunization in 1972 since vaccination campaigns successfully led to the elimination of endemic smallpox in Canada by 1946. The final laboratory-confirmed case of smallpox in Canada was in 1962 (Government of Canada, 2014). Through worldwide vaccination efforts, naturally occurring smallpox disease was globally eradicated by 1977 (Government of Canada, 2014). When infectious diseases are eradicated worldwide because of vaccines, the vaccination programs can be stopped.
Today’s anti-vaccine movement is similar to those early activists in terms of the false messages they send about the supposed dangers of vaccines. One marked difference is the platform that current anti-vaccination advocates use to promote messaging. The Internet – and the rise of social media, in particular – have allowed activists to speak on a large, global stage and develop sophisticated methods to influence and persuade audiences.
The dawn of the Internet age in the 1990s coincided with the publication of a now-infamous research paper that falsely connected the measles, mumps, and rubella (MMR) vaccine to autism. That paper, by disgraced former doctor Andrew Wakefield, was highly flawed and would eventually be debunked and retracted. Despite these measures, Wakefield’s paper continues to circulate online and has attracted legions of followers.
Social media plays an increasingly large role in the way people access information. A 2018 study published by the Pew Research Center found that nearly 70% of Americans got news from social media. Of those, 43% reported Facebook as the top source of daily news.
These findings pose a challenge to vaccine programs, as Facebook and other social media sites do not discriminate between legitimate news organizations and those that promote misinformation. Unlike traditional media outlets, social media pages do not need to abide by editorial codes of conduct, follow the tenets of accountability and transparency, or even stick to facts. In the context of vaccinations, this has resulted in the proliferation of social media pages that attempt to persuade the public using any means, even if it involves veering far from the truth.
Points of Consideration
In 1998, Andrew Wakefield and 12 co-authors published a study entitled “Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorders in children” in the Lancet, a renown medical journal. This paper speculated environmental triggers that led to chronic enterocolitis and regressive developmental disorders. Only 12 children were included in the study (n=12). The study used a non-controlled retrospective research design that concluded an illogical link between the MMR vaccine and autism. This paper was later retracted by the Lancet along with a statement reporting no causal link between the MMR and autism, citing insufficient data. Furthermore, it was later discovered that Andrew Wakefield failed to disclose his financial interests in his paper. He had been funded by lawyers who had been engaged by parents in a lawsuit. It was also discovered that he had misreported sampling techniques and falsified facts. Numerous large and credible studies have since refuted the link between autism and MMR. Video Clip 6.1 offers a historical perspective by Dr. Health MacDougall on vaccine hesitancy and how it has emerged as a current topic today.
Video Clip 6.1: Interview about the History of Vaccine Hesitancy
The legacy of Wakefield’s flawed research lives on today, with many anti-vaccine activists falsely claiming a connection between the MMR vaccine and autism. But the criticisms of vaccines have also evolved and are now much broader. Some of the more common misinformation about vaccines includes:
The human papillomavirus (HPV) vaccine causes sterility.
The current vaccine schedule is responsible for a wide range of chronic childhood illnesses, from asthma to attention deficit hyperactivity disorder (ADHD) to learning disabilities.
Vaccines cause brain damage.
Vaccines are the real cause of sudden infant death syndrome (SIDS).
Anti-vaccine activists falsely claim there are vast conspiracies to suppress this information and that governments, health officials, and the media are being paid by pharmaceutical companies to conceal the truth.
Not everyone who hears these messages will believe them. But research shows that exposure to such ideas can influence how people think. A 2014 study by Daniel Jolley and Karen M. Douglas found that people who listened to anti-vaccine messages said they would be much less likely to vaccinate their children afterward. These messages are ubiquitous online and have permeated everyday thinking. A survey conducted by Angus Reid in 2019 found that 30% of parents said the science on vaccines is not clear. About one in four survey respondents said vaccines come with a serious risk of adverse events.
Points of Consideration
Cognitive dissonance is a term frequently taken up in vaccine psychology, referring to inconsistency in one’s beliefs and behaviours towards a topic (knowing something to be true but not acting on it). Cognitive dissonance related to vaccines occurs when clients are provided facts and information about vaccines but respond with hesitation or refusal. Research has shown that, although it is important to clarify misinformation for clients and engage in public discourse to counter false and misleading information, challenging the credibility of sources on a one-to-one basis may not prove useful. Storytelling is an important alternative for countering the anti-vaccination narrative alongside pertinent information related to vaccines.
How is the Anti-Vaccine Movement Gaining Traction?
65
Anti-vaccine activists are not concerned with the truth. They routinely twist facts and use false data to promote misinformation. But one of the most effective tools is the use of emotionally charged stories about children who have supposedly died or been irreparably harmed by vaccines. Most, if not all, of these stories are fabricated. For instance, the family of a Newfoundland girl who died of cancer discovered that their daughter’s image was being used on the social media page of an anti-vaccine group. The group falsely claimed the girl died as the result of vaccines.
While vaccines carry a risk of serious adverse events, including febrile seizure and cellulitis (less than two per million in 2017), according to Public Health Ontario (2018) the overall incidence of harm is small, particularly compared to the risks of contracting a vaccine-preventable illness. About one in 20 children with measles will develop pneumonia and about one in 1,000 will develop encephalitis—inflammation of the brain.
The use of personal stories is an effective response because they connect with people on an emotional level. Public health vaccination campaigns typically focus on the importance of immunization. Those messages are easily drowned out by the photo of a smiling young child depicted by anti-vaccine activists as a “victim” of vaccination. Video Clip 6.2 is an interview with Globe and Mail reporter, Carly Weeks, describing trends in vaccine hesitancy today.
Del Bigtree is a prominent anti-vaccine activist and an illuminating example of how the movement uses misinformation to spread fear and create mistrust of health professionals. Bigtree rose to prominence as a colleague of Andrew Wakefield’s who helped him develop a film about vaccines. He is a regular speaker at anti-vaccine rallies in the United States and, at times, in Canada. His Facebook page has more than 140,000 likes and his weekly podcast draws thousands of listeners.
Bigtree describes himself as a medical journalist, which lends him a “sense of authority” to discuss issues around vaccines. He speaks forcefully and uses shocking stories to persuade his audience. For instance, at a recent rally, he pinned a yellow star to his clothing and compared the victimization of anti-vaccine activists to the victims of the Holocaust.
Like many others, Bigtree does not simply say “vaccines are bad.” He frames his messages as though he is a protector of public health who must inform individuals about dangers that governments and pharmaceutical companies are conspiring to cover up. He is the head of an organization, called the Informed Consent Action Network, whose stated mandate includes “fighting for parents’ rights,” “protecting children,” and “science-based inquiry.”
These sound like laudable goals. However, the messages he delivers are rife with misinformation, fabrications, and outright lies. For instance, Bigtree claims that no placebo-controlled trials of vaccines have ever been conducted, which he says is proof vaccines are not safe. However, this is false. The reason vaccines are not typically tested against a placebo is that it is unethical to knowingly expose a control group to the risks of a vaccine-preventable illness. No such trial would be ethically approved. This is just one example of an artificial, manufactured controversy employed by anti-vaccination advocates to manipulate, influence, and persuade. Anti-vaccine activists are dedicated to growing audiences on social media and figuring out how to maximize the total number of clicks, likes, and shares. Rising rates of measles outbreaks in unvaccinated populations of developing countries shows that these messages are having an impact.
Image 6.2 provides an example of a mock anti-vaccine website. Notable about this image is the subtle messaging like ‘vaccine awareness’ and ‘informed consent.’ which are intentionally cryptic to allure readership while disguising the ultimate anti-vaccine agenda.
Image 6.2: Mock page of an anti-vaccine website
Points of Consideration
Bigtree’s tactics to confuse the public and garner mistrust in science through inaccurate claims about placebo drugs are not novel. Indeed, tobacco companies in the 1960s popularized similar falsehoods by obscuring the link between smoking and lung cancer.
Health professionals are in a position to counter misinformation campaigns with evidence-based arguments. But most are busy focusing on the safe, effective delivery of care, not waging social media battles. Furthermore, many health professionals are uncertain of how to address concerns over vaccination and may be reluctant to confront anti-vaccination advocates. But the resurgence of measles and growing concern over vaccine hesitancy demonstrates a need for nurses, doctors, pharmacists, and other health professionals to play a more significant role in promoting public confidence in vaccines.
The anti-vaccine movement uses emotional stories to spread fear about vaccination, but health professionals can play an important role in reminding the public about the very real risk of vaccine-preventable disease. Many people have never seen a case of measles and did not grow up with a fear of polio. Health professionals can leverage scientific and historical knowledge to promote vaccines as a way of keeping those diseases in the past. You can also reflect on your own experiences to share stories about the harms of not vaccinating. It may be effective to share a story about your individual choice to vaccinate yourself and your family. Health professionals are the gatekeepers of the healthcare system and can make an important difference in the current misinformation battle over vaccines.
Expanding the Scope of Practice for RNs to Include Prescribing Authority
73
A number of jurisdictions across Canada have implemented or are working towards expanding the scope of practice so that registered nurses (RNs) can prescribe certain medications (including vaccines) to better meet population health needs and improve timely access to appropriate health care (Canadian Nurses Association, 2015). This shift is part of a global trend towards nurse prescribing as countries look for ways to increase access to care in resource-constrained environments and improve efficiencies in complex health systems (Ladd & Schober, 2018). RN prescribing can also support cost effectiveness and innovative practice models (College and Association of Registered Nurses of Alberta, 2019). In Ontario, expanding the RN scope of practice to include certain prescribing powers aligns with the vision of a patient-oriented health care system (Hoskins, 2015).
Regulation of health professionals falls under provincial/territorial jurisdiction in Canada. This chapter focuses specifically on Ontario health professionals. If you are planning to practice in another jurisdiction, you should refer to the regulatory body in that province or territory for current information on scope of practice for vaccine prescribing and administration.
Looking Ahead to RN Prescribing in Ontario
74
Image 7.1: Health Professional Team
In May 2017, the Ontario government made changes to the Nursing Act, 1991 to permit RNs to prescribe certain medications (Government of Ontario, 2017). As of September 2019, the College of Nurses of Ontario (CNO) has created a draft regulation for RN prescribing, but this regulation still needs to be passed by the government prior to RN prescribing authority being enacted in Ontario (CNO, 2019b).
RN prescribing will not be an entry-to-practice level competency for RNs in the general class in Ontario (CNO, 2018b). In order to gain the authority to prescribe medications, RNs will be required to complete additional CNO-approved education programs and are accountable for ongoing competence for safe prescribing (CNO, 2018b). Even after completing a CNO-approved education program, RNs will only be able to prescribe medications if their practice environment supports RN prescribing (CNO, 2019a). For instance, RNs in a hospital setting will not be allowed to prescribe medications because the Public Hospitals Act does not currently allow it (CNO, 2019a).
Future RN prescribers will be different from RNs who are registered in CNO’s extended class, commonly known as nurse practitioners (NPs). NPs currently practice autonomously with respect to assessment, diagnosis, and prescription, and an NP’s expanded scope of practice will continue to be broader than what is proposed for RN prescribers.
Points of Consideration
As a starting point towards RN prescribing, the CNO has authorized other medications in addition to vaccines that authorized RNs will be able to prescribe. This list was determined in consultation with Ontario stakeholders such as clients, RNs, and employers, and takes into consideration government direction and current legislative parameters. The list includes:
Some contraceptives.
Some travel medications such as anti-malarial and anti-bacterial medications.
Some topical medications for wound care.
Some smoking cessation medications.
Over-the-counter medications.
Miscellaneous medications such as epinephrine for anaphylaxis.
Controlled substances are governed under federal law, due to their high risk for misuse, addiction, and diversion. RNs are not permitted to prescribe controlled substances at this time.
Immunization competencies for healthcare providers
75
Any healthcare professional prescribing vaccines requires specific competencies in order to ensure that vaccines, like other medications, are provided in a safe, effective, and ethical manner. In order to promote safe and competent practice, the Public Health Agency of Canada (PHAC) developed a handbook in 2008 entitled Immunization Competencies for Health Professionals. These foundational competencies include:
Explaining how vaccines work using basic knowledge of the immune system.
Understanding the rationale and benefits of immunization.
Integrating into practice knowledge about the main steps in vaccine development and evaluation.
Applying knowledge of the components and properties of immunizing agents as needed for safe and effective practice.
Applying relevant principles of population health for improving immunization coverage rates.
Communicating effectively about immunization.
Implementing guidelines for safe storage and handling of vaccines.
Preparing and administering immunization agents correctly.
Anticipating, identifying, and managing adverse events following immunization.
Understanding documentation requirements for immunizations.
Recognizing and responding to the unique immunization needs of certain population groups.
Demonstrating an understanding of the immunization system in Canada.
Addressing immunization issues using an evidence-based approach.
Acting in accordance with legal and ethical standards in all aspects of immunization practice (PHAC, 2008).
Health professionals need to be able to anticipate, identify, and manage adverse events that may occur following immunizations (PHAC, 2008). As you have learned in earlier chapters of this resource, adverse events following immunizations are rare. Although these events are rare, monitoring vaccine safety through mandatory adverse event reporting is an important aspect of the immunization program in Ontario. Adverse events following immunization can be reported with a form from the PHAC, which can be submitted to the local public health agency where the patient lives.
Optimizing the Role of Ontario RNs in Immunization Through RN Prescribing
Pending government approval of the proposed CNO regulation, RN prescribing will be authorized for certain medications that will allow RNs to manage non-complex patient care needs (CNO, 2019b). In the first phase of RN prescribing in Ontario, these medications will include some vaccines (CNO, 2019b).
While RNs in Ontario have typically participated in immunization as front-line providers in schools and community settings, this change will allow RNs to not only administer vaccines but prescribe them as well. Given the important role RNs play in primary health care and health promotion, a strategic focus on maximizing the involvement of RNs in immunization should help advance the public health goal of immunization for everyone across the life cycle (International Council of Nurses, 2013).
Scope of Practice for Other Health Professionals Involved in Immunizations
76
While Ontario is in the process of expanding the scope of practice for RNs to include prescribing authority for vaccines, NPs and physicians can currently prescribe vaccines to individual patients and may also develop directives that authorize other healthcare providers (such as RNs or registered practical nurses, or – if the ordering practitioner is a physician – physician assistants) to administer vaccines to a larger client population when certain conditions are met and specific circumstances exist. Directives must include a number of detailed components and should be supported by certain facility policies prior to implementation (CNO, 2018a).
To improve influenza vaccination rates, Ontario pharmacists, pharmacy students, and pharmacy interns became authorized to prescribe and administer influenza vaccines in 2012 to clients over the age of five. These pharmacists and pharmacists-in-training need to complete specific injection training requirements and be practicing at a pharmacy registered with Ontario’s Universal Influenza Immunization Program (Ontario College of Pharmacists, n.d.). In December 2016, this scope was expanded to include other vaccines including Hib, hepatitis A, hepatitis B, herpes zoster, HPV, Japanese encephalitis, meningitis, pneumococcal disease, rabies, tuberculosis, typhoid, varicella, and yellow fever (Ontario College of Pharmacists, 2016). In April 2019, the Ontario government announced it may further expand the scope of practice to allow pharmacists to administer influenza vaccines to children under five years of age (Jones, 2019).
Midwives in Ontario need to be aware of current guidelines for vaccination recommendations for pregnant people, who are at greater risk than non-pregnant people for more severe illness from some vaccine-preventable diseases (Association of Ontario Midwives, 2018). Midwives in Ontario may prescribe and administer certain vaccines to their clients, such as hepatitis B and MMR vaccines (College of Midwives of Ontario, 2014). However, other vaccines recommended in pregnancy, such as pertussis and influenza, may require a referral to another primary care provider. Similarly, providing routine childhood immunizations falls outside the midwifery scope of practice in Ontario. As you learned earlier in this resource, vaccinations typically begin at two months of age, and clients and their infants are discharged from midwifery care at six weeks postpartum. Clients may wish to discuss immunizations with their midwives in the prenatal period, and during their postpartum/newborn visits. As a result, midwives, like other health professionals, should be aware of the childhood immunization schedule in Ontario and where clients can find evidence-based information.
Conclusion
77
Ontario is in the process of implementing RN prescribing for various medications, including vaccines. This shift is meant to support patient access to health care by optimizing scope of practice for safe and effective care by RNs and follows a similar trend for pharmacists in Ontario. Policy action that supports nurse prescribing of vaccines is an important step in increasing vaccination rates across the life cycle (International Council of Nurses, 2018). Achieving higher vaccine coverage rates to improve population health is an important goal and Ontario is taking steps towards this through implementing RN prescribing authority for vaccines.
Reflective Questions
78
Why are certain jurisdictions expanding the RN’s scope of practice to include prescribing medications?
How do RNs know whether they are able to prescribe medications such as vaccines? What criteria need to be met before an RN is permitted to prescribe a vaccine?
Key Takeaways
79
The key takeaways of this chapter are:
Expanding the scope of practice for RNs to include prescribing medications such as vaccines is meant to improve access to care and better address population health needs.
As of September 2019, the CNO has created a draft regulation for RN prescribing that, once passed by the government, will enable RNs to prescribe certain medications to their clients.
RN prescribing in Ontario will not be an entry-to-practice level competency for RNs in the general class; practicing RNs will be required to complete additional CNO-approved education programs before being authorized to prescribe.
Vaccines will be among the medications that authorized Ontario RN prescribers may prescribe to their clients.
When prescribing vaccines, health professionals are accountable for ensuring they are competent to prescribe vaccines in a safe, effective, and ethical manner.
References
80
Association of Ontario Midwives. (2018). Vaccinations in pregnancy. Retrieved from https://www.ontariomidwives.ca/vaccinations-pregnancy
Jones, A. (2019, April 18). Ontario may let pharmacists prescribe treatments for minor issues like pink eye. Toronto CityNews. Retrieved from https://toronto.citynews.ca/2019/04/18/ontario-pharmacists-treatments-health-care/
Ladd, E., & Schober, M. (2018). Nurse prescribing from the global vantage point: The intersection between role and policy. Policy, Politics, & Nursing Practice, 19(1-2), 40-49. https://doi.org/10.1177/1527154418797726
Ontario College of Pharmacists. (n.d.). Administering injections. Retrieved from http://www.ocpinfo.com/practice-education/practice-tools/collection/administering-injections/.

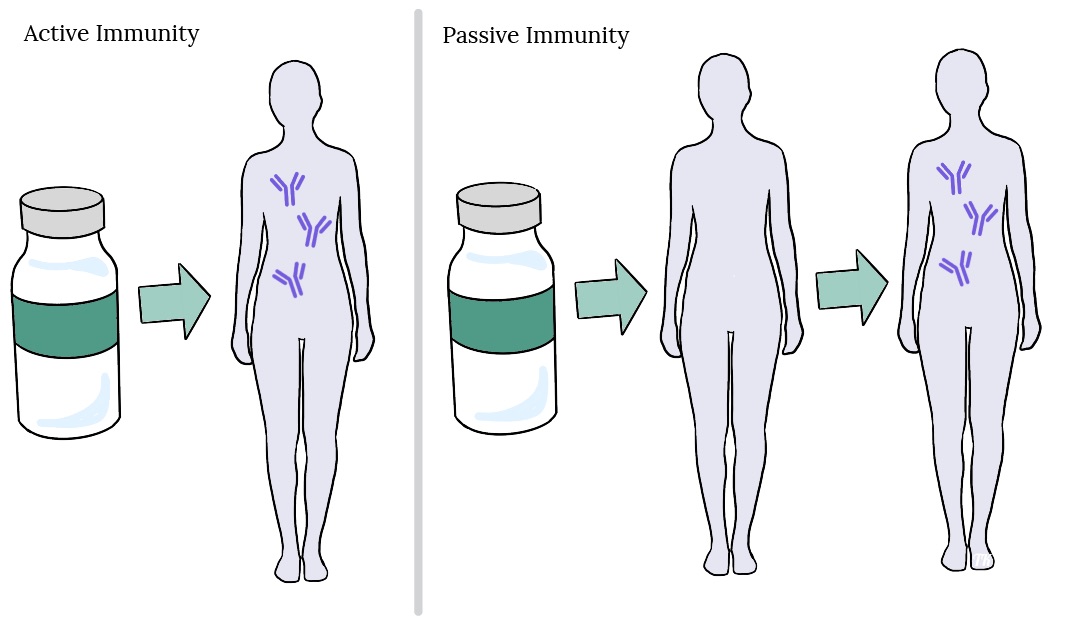

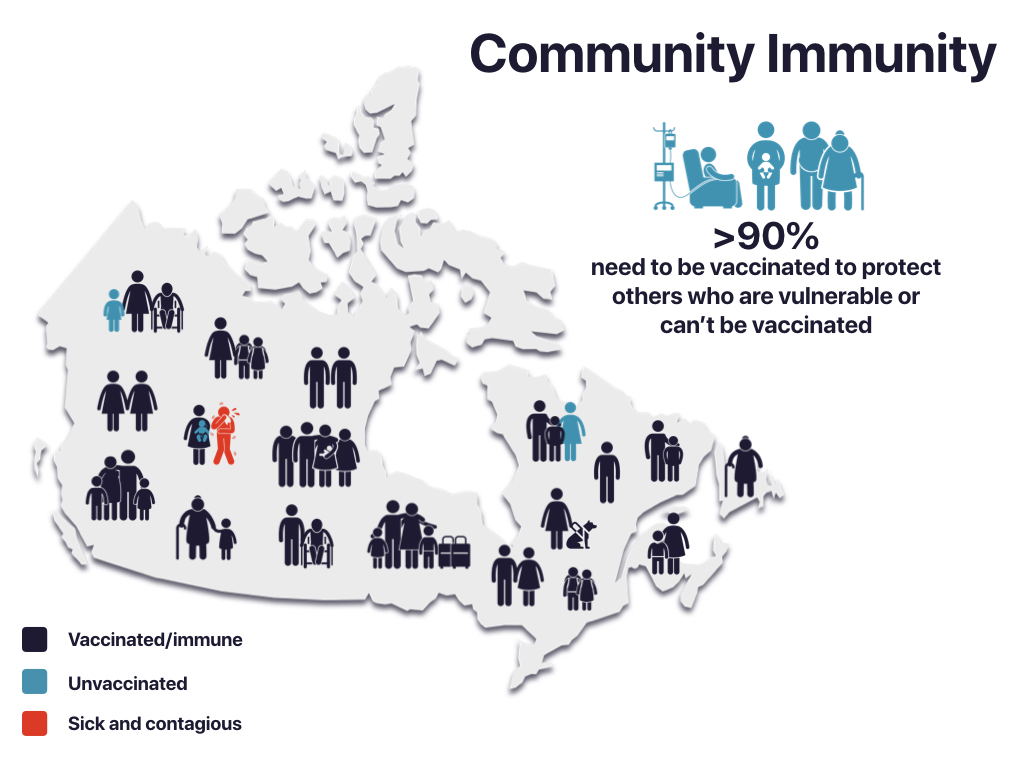

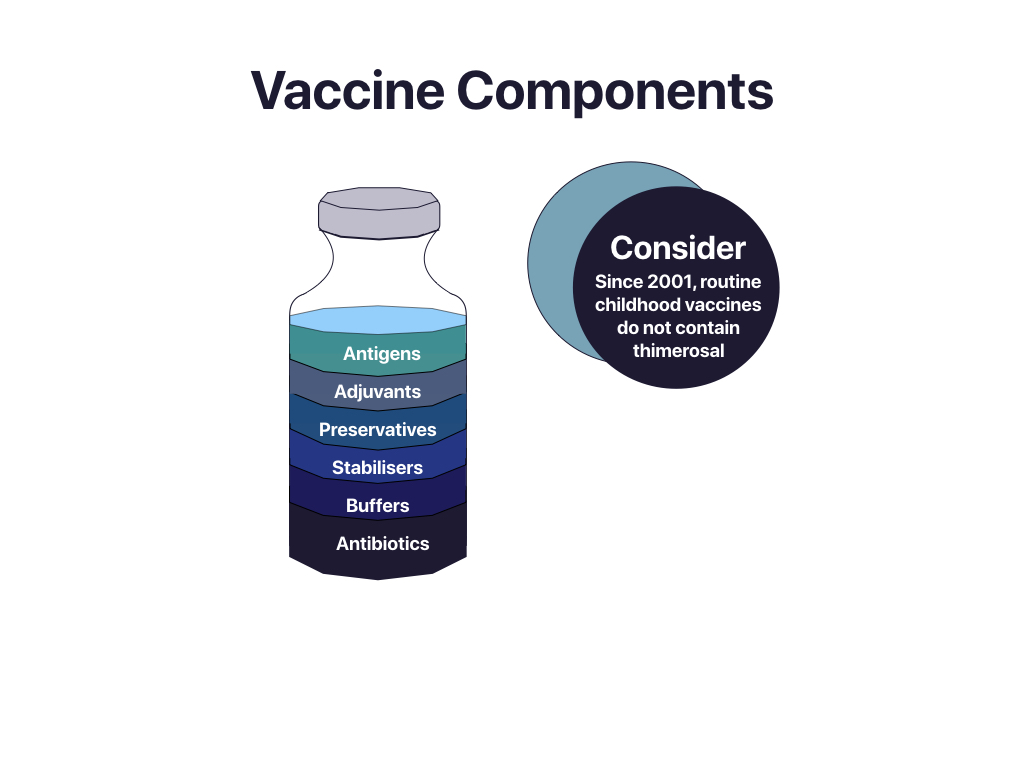
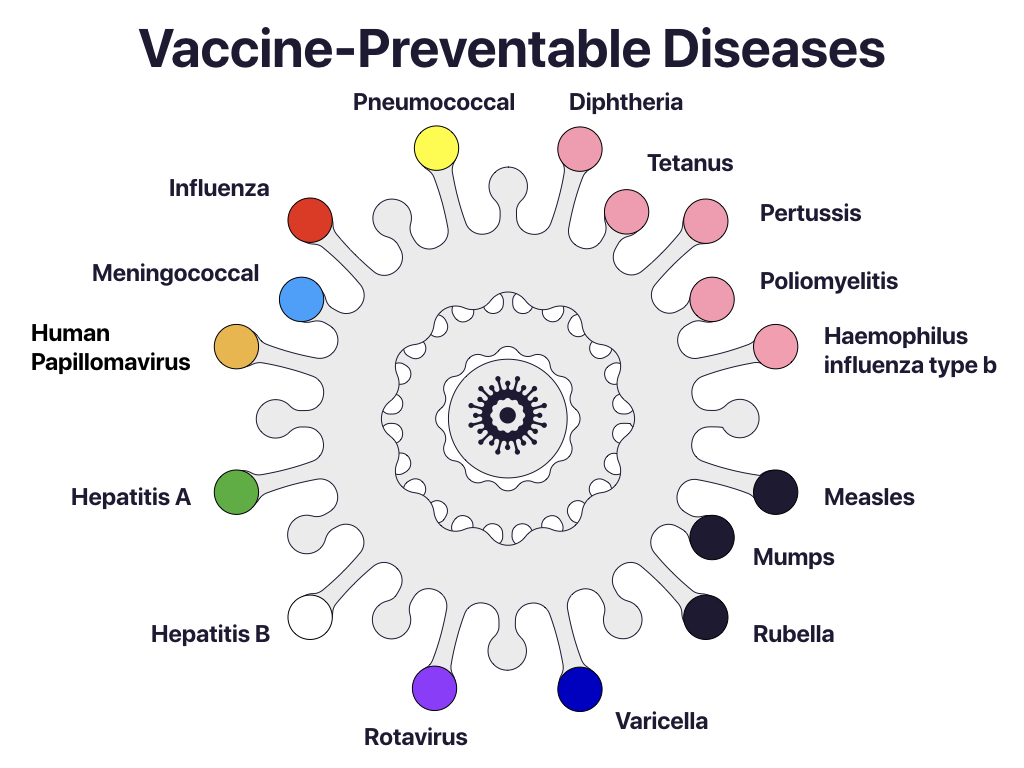

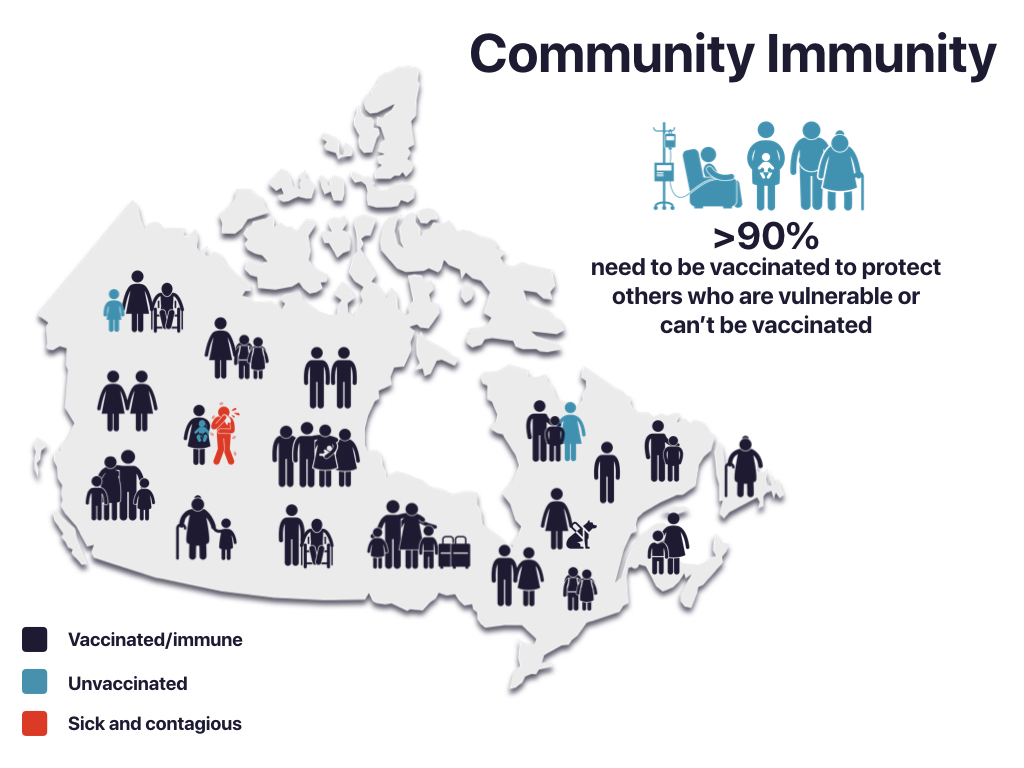 90% need to be vaccinated to protect others who are vulnerable or can’t be vaccinated.”" width="500" height="375" srcset="https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity.jpeg 1024w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-300x225.jpeg 300w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-768x576.jpeg 768w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-65x49.jpeg 65w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-225x169.jpeg 225w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-350x263.jpeg 350w" sizes="(max-width: 500px) 100vw, 500px">
90% need to be vaccinated to protect others who are vulnerable or can’t be vaccinated.”" width="500" height="375" srcset="https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity.jpeg 1024w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-300x225.jpeg 300w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-768x576.jpeg 768w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-65x49.jpeg 65w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-225x169.jpeg 225w, https://ecampusontario.pressbooks.pub/app/uploads/sites/483/2019/09/Community-Immunity-350x263.jpeg 350w" sizes="(max-width: 500px) 100vw, 500px">