This project would not have been possible without the Teaching Innovation Fund (TIF) grant from the Centre for Teaching and Learning at Ontario Tech University. This grant funded a project coordinator to oversee case study materials.
These materials would not have been possible without the knowledge and expertise of Ontario Tech University faculty collaborators, including: Drs. Robert Balogh, Laura Banks, Adam Cole, Mika Nonoyama, Elita Partosoedarso, and Otto Sanchez. Their ability to provide feedback and synthesize new ideas contributed to the final version of this publication.
We are grateful to Ms. Brenda Barth, our Project Coordinator at Ontario Tech University, for leading the case study development. We are also thankful to Ms. Jill Thompson, an Indigenous Cultural Advisor at Ontario Tech University, for providing guidance related to the development of our case study family. Lastly, we would like to acknowledge staff from the Open Education Lab at Ontario Tech University, for their assistance in the preparation and publication of this project as an open educational resource.
Caption: OER Equal Love
Thank You!
Thank you to the students employed by the OE Lab for working hard to make this book a reality. Congratulations on your achievement!
Suggested Attribution for This Work: Banks, L., Barth, B., Balogh, R., Cole, A., Nonoyama, M., Partosoedarso, E., & Sanchez, O. Multi-Course Case Studies in the Health Sciences. OE Lab at Ontario Tech University, 2021, licensed under a CC BY NC SA 4.0 International License, unless otherwise noted.
About the Open Education (OE) Lab
Ontario Tech University is proud to host the OE Lab – a student-run, staff-managed group that brings content and technological expertise to the timely creation of high quality OER that will be used directly in an Ontario Tech course by Ontario Tech students.
If you adopt this book, you will be using a work created by students as an experiential learning and employment opportunity. Please let us know if you are using this work by emailing oer@ontariotechu.ca.
In 2020, our team of six (6) faculty collaborators Ontario Tech University received a Teaching Innovation Fund (TIF) grant to develop a multi-course approach to case-based learning in the health sciences. Case studies may prepare students for their future careers by connecting theoretical concepts to community practice with the application of knowledge.
Our team has developed ten (10) interconnected, multidisciplinary cases exploring health and disease across the lifespan in an extended family living in Canada. These cases have been designed for use in multiple undergraduate courses to facilitate scaffolding of student knowledge with increasingly complex case analyses. This novel approach may enable students to apply critical knowledge from a biological, behavioural and sociological perspective into unified clinical situations. As students review the cases, several perspectives should be considered, including:
Biological Perspectives
Normal anatomy and physiology
Pathophysiology
Growth, development, and aging
Behavioural Perspectives
Health behaviours
Mental health
Health-related quality of life
Sociological Perspectives
Social determinants of health
Age
Sex and gender
Sexual orientation
Race
Cultural norms
Intersectionality
Content Organization
These case studies have been organized with the following resources available for use:
Ten (10) multi-disciplinary case study readings and presentations
Academic content with links to peer-reviewed publications
In 1946, Ojibwe parents in Northwestern Ontario brought a son into the world. At the age 6 years he was forcibly removed from his home on the reserve and sent to a Residential school run by a religious organization and given the name ‘Jack’. The school focused on instruction in trades and agriculture. He was often subjected to harsh discipline, malnutrition, poor healthcare, physical, emotional, and sexual abuse, and the deliberate suppression of his culture and language.
Jack recalls that first day; he was loaded onto a bus and drove him to the school. He thought he was just going for a drive for a few hours and would be returning home. That first day after he arrived, he didn’t know what was going on. They gave him clothes and a shower, it was difficult for him to stay there. His parents told him that he was going to a school, but Jack thought it was just going to be for the day, and he would be returning home to his parents and community. When allowed outside to play, the boys were segregated from the girls in the yard.
A typical day at the residential school consisted of waking up at about 6:00 a.m., having breakfast, taking a shower, and then going to church. He remembers praying more than going to school. In the early days when Jack spoke his own language, the teachers would pull his ear and hit him with a ruler. They would make him kneel down in the church as additional punishment for speaking his own language.
If he had stayed with his parents he would have been able to speak the language, understand them and their culture. However, the few times he returned to see his parents and community, he felt like an outsider, unable to understand the language, unable to communicate effectively with his family. Jack would describe his years at the Residential school as bad. It made him scared of regulations and rules. After Jack left the school, he was always getting in trouble with the police due to alcohol consumption. He would get picked up for being drunk and disorderly, and spend a few days in jail.
The thing Jack hated the most about his time at Residential school was the daily showers. They would dry the kids off, and rub powder all over them. Jack did not realize at the time that this was sexual abuse, he and his friends would laugh at teachers rubbing them.
He did not feel like he received a good education from the Residential school. When he first left, he lived on the streets. He found it difficult to gain employment, as his education lacked, and no one wanted to employ an “Indian”. Jack persevered, eventually finding odd jobs over the years. He worked as a farm-hand, in the local lumber yard, and finally got a permanent position working in the mine.
Based on the recorded story of Tim Antoine https://legacyofhope.ca/wherearethechildren/stories/
He met Mary in 1962 at the general store where she worked. He was away working in the mines for a few years, upon his return he rekindled his relationship with Mary and they married in 1969. Jack found a mining job close to home and worked there until he retired. Jack and Mary had two children. Mary attended church regularly with the children, however Jack refused to go with her as it brought back too many painful memories.
Jack often felt he had nothing to offer his children, he had lost his heritage years ago. Of Jack’s two children, he is closest to his daughter Nancy. He encouraged her to play sports, took her fishing and hunting, these were things he felt comfortable doing. Jack’s son, Phillip had no interest in any of these activities.
Jack worked hard to maintain the home that he has shared with his wife for almost 50 years. Over the last 5 years, Jack has been struggling with pain and numbness in his feet which has affected his ability to maintain his home. Jack started doing less and less as time went on due to the pain and numbness.
Jack was diagnosed with Type II diabetes mellitus just before he turned 50. Jack takes short-acting insulin with meals. Mary has been testing Jack’s blood glucose levels and giving him his insulin injections routinely for the last 25 years.
A Turn of Events…
While Mary was in hospital for 7 days, Jack struggled with meal prep, testing his blood glucose levels, and giving himself his insulin injections. As Mary’s discharge from hospital approaches, it is decided that Jack and Mary will move in with Nancy and Paul.
A few days prior to Mary’s discharge, Nancy travels up to the family home to help pack up what her mother and father will need while they stay at her house.
Nancy is shocked at the disrepair of her childhood home and the unkempt look of her father. Nancy quickly assesses that Jack is unwashed, appears to be slightly short of breath (SOB), limping slightly, and there is a strange odor coming from her father.
Jack admits that he has been struggling since Mary went into hospital. He has not been eating or managing his blood sugars and insulin well. He is also embarrassed to admit he has not bathed since Mary has gone due to his inability to access the bathtub safely on his own.
Nancy prepares lunch for Jack and checks his blood glucose levels (12.4 mmol/L). Nancy administers the required amount of insulin and eats their lunch.
After lunch, Nancy helps her father into the bathtub for a shower. Jack’s SOB increases slightly with exertion, he states he feels like his heart is racing and he can’t catch his breath. Nancy takes a radial pulse, and is pretty sure it is 130 BPM. Although Jack is embarrassed that Nancy is helping him, he allows her to help him undress and get into the tub.
As Jack’s socks are removed, the odd odor increases. Nancy now sees the source of that odor, an open, oozing wound on her father’s right foot. After Jack finished bathing, Nancy settled him with a snack and a cup of tea while she went to call his family doctor.
Upon hearing the circumstances Nancy had found her father in, the family physician told Nancy to bring her father into the emergency department of the local hospital. The physician called ahead to let the ED know Jack was coming.
Jack was seen by the emergency physician and diagnosed with new onset of atrial fibrillation. Jack was admitted with a referral to the cardiologist for the newly developed atrial fibrillation and the endocrinologist to provide appropriate care for Jack’s Type II diabetes. A referral was sent for the wound-care nurse.
Medications
Lovenox
Propranolol: beta blocker
Cardizem: calcium channel blocker
Nancy was now in a dilemma as both of her parents were in hospital. Her mother was due to be discharged the next day. The plan had been for Nancy to take both of her parents to stay with her while her mother recuperated. She needed to get home to her son, husband and her studies.
Nancy spoke with the discharge planner and explained the situation. Mary would be kept in hospital until Jack was ready for discharge. Nancy then drove back to Toronto, awaiting her parents discharge.
Four days after admission, Jack was ready for discharge. He had explicit discharge instructions for follow-up:
Wound care nurse to come daily to change foot dressing and assess healing
Blood sugar monitoring four times each day, values to be recorded
Insulin to be adjusted based on blood sugars, and given by Nancy
Medications to be taken as prescribed
Follow-up appointments with cardiology and endocrinology in 4 weeks
Jack had now been in his daughter’s house for a week and had noticed the tension between Nancy and her husband. He did not understand what was wrong with Sam, but could not help but think they should be able to return the sick child they had adopted, this is not what Nancy and Paul had signed up for.
He constantly felt like a burden with all the care he required and spent most of his time in the room that he and Mary shared. He was concerned about his wife’s recovery and wished that they could just go home.
Since Mary has been ill, Jack has had time to contemplate his life. He felt that if he had not gone to Residential school, he would have been a very different person, and led a very different life. The school took away his birthright, his culture and history. He stopped going back to the reserve to visit family shortly after he got married, as he felt like an outsider. Jack felt that he had let his children down, as he was not able to provide them with the rich heritage of the Ojibwe people.
Case Key Words
Aboriginal
Atrial Fibrillation
Cardiovascular-Conduction
Endocrine System
Foot Ulcer
Heart
Indigenous
Occupational Illness and Disease
Pancreas
Peripheral Circulation
Peripheral Neuropathy
Post-Traumatic Stress Disorder (PTSD)
Residential Schools
Type II Diabetes
Residential Schools and the Effects on Indigenous Health
New school opened October 3rd, 1935 & housed 140 pupils
The school focused on teaching trades & agriculture
Jack was often subjected to:
Harsh discipline
Malnutrition
Poor health
Physical, emotional, and sexual abuse
Deliberate suppression of his culture and language
Daily Schedule
5 AM
Bell rings; students rise, wash, & dress
5:30 AM
Breakfast, then prayers
6 – 9 AM
Boys work on farm; girls work in house
9 – 12 PM
School
12 – 1 PM
Lunch & recreation
1 – 3:30 PM
School
3:30 – 6 PM
Work on farm
6 PM
Dinner & prayers
Evening
Boys: school in winter; work on farm in summer
Girls: learn needlework
9 PM
Bedtime
Effects on Indigenous Health
Personal or familial residential school attendance is related to health in a multitude of ways. People who attended residential schools generally feel their health or quality of life has been negatively impacted.
General health: poorer overall self-rated health, less likely to seek health care
Physical health: chronic health conditions and infectious diseases
Mental health and emotional well-being: mental distress, depression, addictive behaviour, substance misuse, stress, and suicidal behaviours
Web of Being: Determinants and Indigenous People’s Health
Determinants of health can be conceptualized as either historical (distal) or contemporary (proximal). To understand the interconnectedness of these determinants and their combined influence on the general health of Indigenous peoples, one must look into the past.
Occupational Illness and Disease
Occupational health focused on the physical health – respiratory disease, the impact of noise, heat and vibration on the miners’ health. A significant number of miners are experiencing high levels of stress, anxiety, and depression (Centre for Research in Occupational Safety and Health).
Jack's Health: Type II Diabetes Mellitus
Jack was diagnosed with type II diabetes mellitus (DM) just before he turned 50 years of age.
Signs and Symptoms
Signs and symptoms of type II DM often develop slowly. You can live with type II DM for years and not know it. When signs and symptoms are present, they include:
Increased thirst
Frequent urination
Increased hunger
Unintended weight loss
Fatigue
Blurred vision
Slow-healing sores
Frequent infections
Numbness or tingling in hands or feet
Areas of darkened skin, usually in the armpits & neck
Causes
Type II DM is primarily the result of two interrelated problems:
Cells in muscle, fat, and the liver become resilient to insulin.
Because these cells don’t interact in a normal way with insulin, they don’t take in enough sugar.
The pancreas is unable to produce enough insulin to manage blood sugar levels.
How Insulin Works
Insulin is a hormone that comes from the pancreas and regulates how the body uses sugar in the following ways:
Sugar in the bloodstream triggers the pancreas to secrete insulin
Insulin circulates in the bloodstream, enabling sugar to enter the cells
The amount of sugar in the bloodstream drops
In response to this drop, the pancreas releases less insulin
Type
Examples
Appearance
Onset
Peak
Duration
Rapid-acting
Apidra (insulin glulisine)
Clear
10-15 mins
1-1.5 hrs
3.5-5 hrs
Fiasp (faster-acting insulin aspart)
Clear
4 mins
0.5-1.5 hrs
3-5 hrs
Humalog (insulin lispro)
Clear
10-15 mins
1-2 hrs
3-4.75 hrs
NovoRapid (insulin aspart)
Clear
9-20 mins
1-1.5 hrs
3-5 hrs
Short-acting
Entuzity (insulin regular)
Clear
15 mins
4-8 hrs
17-24 hrs
Humulin R, Novolin ge Toronto (insulin regular)
Clear
30 mins
2-3 hrs
6.5 hrs
Long-acting
Basaglar (insulin glargine biosimilar)
Clear
1.5 hrs
Does not apply
24 hrs
Lantus (insulin glargine U-100)
Clear
1.5 hrs
Does not apply
24 hrs
Levemir (insulin detemir U-300)
Clear
1.5 hrs
Does not apply
16-24 hrs
Toujeo (insulin glargine U-300)
Clear
1.5 hrs
Does not apply
Up to 30 hrs
Tresiba (degludec)
Clear
1.5 hrs
Does not apply
42 hrs
Insulin Mixtures
For convenience, there are premixed rapid- and intermediate-acting insulin. The insulin will start to work as quickly as the fastest-acting insulin in the combination. It will peak when each type of insulin typically peaks, and it will last as long as the longest-acting insulin.
Examples include:
30% regular and 70% NPH (Humulin 30/70, Novolin ge 30/70)
50% lispro and 50% lispro protamine (Humalog Mix 50)
25% lispro and 75% lispro protamine (Humalog Mix 25)
30% aspart and 70% aspart protamine (NovoMix 30)
The Role of Glucose
Glucose – a sugar – is a main source of energy for the cells that make up muscles and other tissue. The use and regulation of glucose includes the following:
Glucose comes from 2 major sources: food and the liver
Glucose is absorbed into the bloodstream, where it enters cells with the help of insulin
The liver stores and makes glucose
When glucose levels are low, the liver breaks down stored glycogen into glucose
In type II DM, this process does not work well. Sugar does not enter the cells, builds up in bloodstream. The beta cells in the pancreas release more insulin. Eventually these cells become impaired.
In type I DM, the immune system mistakenly destroys the beta cells, leaving the body with little to no insulin.
Risk Factors
Weight – being overweight or obese is a main risk
Fat distribution – storing fat mainly in the abdomen (men waist >40 inches, women waist >35 inches)
Inactivity – physical activity keeps weight done, and uses up glucose as energy, makes cells more sensitive to insulin
Family history – increases if parent or sibling has type II DM
Race and ethnicity – Black, Hispanic, Indigenous, Asian, Pacific Islanders
Blood lipid levels – increased risk associated with love levels of HDL cholesterol and high levels of triglycerides
Age – increases with age, especially after age 45
Prediabetes – blood sugars higher than normal, but not high enough to be classified as diabetes, if left untreated often progresses to type II DM
Pregnancy-related risks – increases if you develop gestational diabetes or if you give birth to a baby weighing > 9 pounds
Polycystic ovary syndrome – common condition characterized by irregular menstrual periods, excess hair growth and obesity-increases the risk of diabetes
Complications and Frequent Comorbidities
Heart and blood vessel disease – increase risk of heart disease, stroke, hypertension, and atherosclerosis
Neuropathy in limbs – overtime nerves are destroyed, resulting in tingling, numbness, burning pain or eventual loss of feeling. Begins at tips of toes or fingers and gradually spreads
Other nerve damage – damage to heart nerves can contribute to irregular heart rhythms. Digestive nerve damage may lead to nausea, vomiting, diarrhea or constipation. Men, erectile dysfunction.
Kidney disease – may lead to irreversible end-stage kidney disease
Eye damage – cataracts and glaucoma, may damage the blood vessels in the retina
Skin conditions – more susceptible to bacterial and fungal infections
Slow healing – cuts and blisters can become seriously infected, severe damage might require amputation
Hearing impairment
Sleep apnea – obstructive sleep apnea is common, obesity may be the main contributing factor. Not clear if treating sleep apnea improves blood sugar control
Dementia – seems to increase risk of Alzheimer’s disease and other dementia disorders. Poor blood sugar control linked to more-rapid decline in memory and thinking skills
Prevention
Monitor and/or lower blood pressure and cholesterol
30 minutes of activity per day five days per week helps lower risk of developing type II diabetes by 58%
Eat a healthy diet, including less fats, more fiber, whole grains, veggies, fruits, lean meats
Manage weight and BMI
Jack's Health: Diabetic Foot Ulcers
Jack’s Story Continues
Jack is found by his daughter unkempt, SOB, limping slightly, and has a strange odor coming from him
States he has not been eating or managing his blood sugars and insulin well
Has not bathed since his wife went to hospital (unable to access the bathtub safely)
Blood glucose level is 12.4 mmol/L
Heart rate 130 BPM
Daughter finds an open, oozing wound on Jack’s foot
Symptoms and Diagnosis
Wagner Ulcer Classification System:
0: no open lesions, may have healed lesion
1: superficial ulcer without penetration to deeper layers
2: deeper ulcer, reaching tendon, bone, or joint capsule
3: deeper tissues involved, with abscess, osteomyelitis, or tendonitis
4: gangrene in a portion of forefoot or heel
5: extensive gangrenous involvement of the entire foot
Causes
Poor circulation – blood does not flow to feet efficiently, also making ulcers more difficult to heal
Hyperglycemia – can slow healing process
Nerve damage – tingling and pain, decrease or loss of feeling
Irritated or wounded foot – reduced sensitivity results in painless wounds
Wearing inappropriate footwear – may be significant in wound progression
Treatment
Treatment primarily depends on the stage of the ulcer. Essential to start treatment as soon as possible – helps prevent infection and provides better results sooner
Antibiotics if applicable (C&S of wound site)
Shoes designed for individuals with DM
Debridement
Foot baths
Disinfecting the skin around the ulcer
Keeping the ulcer dry with frequent dressing changes
Dressings containing calcium alginates to inhibit bacterial growth
Surgical procedures – shave bone or removing foot abnormalities (bunions or hammertoes)
Other treatment options ineffective – amputation
Prevention
Washing feet every day
Keeping toenails adequately trimmed, but not too short
Keeping feet dry and moisturized
Changing socks frequently
Seeing a podiatrist for corn and callus removal
Wearing proper-fitting shoes
Jack's Health: Atrial Fibrillation
Jack’s Story Continues
Jack is found by his daughter unkempt, SOB, limping slightly, and has a strange odor coming from him
States it feels like his heart is racing and he can’t catch his breath
Radial pulse 130 BPM (irregular)
Jack is taken to the emergency department as per his family physician’s recommendation
Jack is diagnosed with new onset of atrial fibrillation
Admitted to hospital with a cardiologist and endocrinologist referral
Overview
In a normal heart rhythm, a tiny cluster of cells at the sinus node sends out an electrical signal. The signal then travels through the atria to the atrioventricular (AV) node and passes into the ventricles, causing them to contract and pump out blood. In atrial fibrillation, electrical signals fire from multiple locations in the atria (typically pulmonary veins), causing them to beat chaotically. Since the atrioventricular (AV) node doesn’t prevent all of these chaotic signals from entering the ventricles, your heart will beat faster and more irregularly than normal.
Atrial Fibrillation
Irregular and often rapid heart rate
Can increase risk of stroke, heart failure, other heart-related complications
The two atria beat chaotically and irregularly – out of coordination with the two ventricles
Episodes may come and go, or does not go away requiring treatment
Is not life-threatening but a serious medical condition that may require emergency treatment
Major concern is the potential to develop blood clots in the atria
These clots may circulate to other organs and lead to ischemia
May weaken the heart and lead to heart failure
Atrial fibrillation may be:
Occasional – paroxysmal A-fib comes and goes, usually lasting for a few minutes to hours. May last up to a week and happen repeatedly.
Persistent – heart rhythm does not go back to normal on its own. Will need treatment; medication or electrical shock to restore normal heart rhythm.
Long-standing persistent – continuous and lasts longer than 12 months.
Permanent – normal heart rhythm cannot be restored. Requires medication to control heart rate and to prevent clots.
Symptoms
Palpitations, sensations of a racing, uncomfortable, irregular heartbeat or a ‘flip-flopping’ in the chest
Weakness
Reduced ability to exercise
Fatigue
Lightheadedness
Dizziness
Shortness of breath
Chest pain
Possible Causes
Abnormalities or damage to the heart’s structure are the most common cause of A-fib.
Possible causes of A-fib include:
High blood pressure
Heart attack
Coronary artery disease
Abnormal heart valves
Heart defects (congenital)
Overactive thyroid gland or other metabolic imbalance
Exposure to stimulants – medications, caffeine, tobacco, alcohol
Sick sinus syndrome – improper functioning of the heart’s natural pacemaker
Lung diseases
Previous heart surgery
Viral infections
Stress due to surgery, pneumonia or other illnesses
Sleep apnea
Management
Treatment with Medication
Rate Control Medications
Rhythm Control Medications
Beta blockers (Metroprolol or Bisoprolol)
Amiodarone (Cordarone)
Calcium channel blockers (Diltiazem)
Dronedarone (Multaq)
Cardiac glycosides (Digitalis)
Flecainide (Tambocor)
Propafenone (Rythmol)
Sotalol (Sotacor)
Procedures for Rhythm Control
Electrical Cardioversion – delivering a shock to the heart, like defibrillation but a smaller amount of electricity. Cardioversion is a short-term solution. In most patients, the A-fib comes back.
Catheter Ablation – inserting thin wires into the veins in your groin or neck. The tip of the wire is directed towards the area in your heart that is firing irregular impulses. Once in position, a small jolt of radiofrequency electrical current is delivered to burn out the tiny areas.
Betts, J. G., Johnson, E., Young, K. a., Wise, j. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Cardiac Muscle and Electrical Activity, Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. a., Wise, j. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Tissue Injury and Aging, Anatomy and Physiology. OpenStax.
Andrade, J. G., Aguilar, M., Atzema, C., Wyse, D. G., & Macle, L. (2020). The 2020 Canadian Cardiovascular Society/Canadian Health Rhythm Society Comprehensive Guidelines for the Management of Atrial Fibrillation. Canadian Journal of Cardiology, 36(12), 1847-1948. https://doi.org/10.1016/j.cjca.2020.09.001
Barton, S. S., Anderson, N., & Thommasen, H. V. (2005). The diabetes experiences of Aboriginal people living in a rural Canadian community. Aust J Rural Health, 13(4), 242-246. https://doi.org/10.1111/j.1440-1584.2005.00709.x
Berbudi, A., Rahmadika, N., Tjahjadi, A. I., & Ruslami, R. (2020). Type 2 diabetes and its impact on the immune system. Current Diabetes Reviews, 16, 442-449. https://doi.org/10.2174/1573399815666191024085838
Cowan, K. (2020). How Residential schools led to intergenerational trauma in the Canadian Indigenous population to influence parenting styles and family structures over generations. Canadian Journal of Family and Youth, 12(2), 26-35. https://doi.org/10.29173/cjfy29511
Green, M. E., Shah, B. R., Slater, M., Khan, S., Jones, C. R., & Walker, J. D. (2020). Monitoring, treatment and control of blood glucose and lipids in Ontario First Nations people with diabetes. CMAJ, 192(33), e937-e945. https://doi.org/10.1503/cmaj.191039
Lung, C. W., Wu, F. L., Liao, F., Pu, F., Fan, Y., & Jan, Y. K. (2020). Emerging technologies for the prevention and management of diabetic foot ulcers. Journal of Tissue Viability, 29(2), 61-68. https://doi.org/10.1016/j.jtv.2020.03.003
Shah, B. R., Slater, M., Frymire, E., Jacklin, K., Sutherland, R., Khan, S., . . . Green , M. E. (2020). Use of the health care system by Ontario First Nations people with diabetes: A population based study. CMAJ Open, 8(2), E313-E318. https://doi.org/10.9778/cmajo.20200043
Society of Obstetricians and Gynaecologists of Canada. (2013). Social determinants of health among First Nations, Inuit, and Metis. Journal of Obstetrics and Gynaecology Canada, 35(6), S13-S23. https://doi.org/10.1016/S1701-2163(15)30703-9
Tanaka, H., Tatsumi, K., Matsuzoe, H., Soga, F., Matsumoto, K., & Hirata, K. I. (2021). Association of type 2 diabetes mellitus with the development of new-onset atrial fibrillation with non-ischemic dilated cardiomyopathy: Impact of SGLT2 inhibitors. The International Journal of Cardiovascular Imaging, 37, 1333-1341. https://doi.org/10.1007/s10554-020-02122-x
The General Synod of the Anglican Church of Canada. (2021). Anglican Residential Schools. The Anglican Church of Canada. https://www.anglican.ca/tr/histories/
Wilk, P., Maltby, A., & Cooke, M. (2017). Residential schools and the effects on Indigneous health and well-being in Canada – A scoping review. Public Health Reviews, 38(8). https://doi.org/10.1186/s40985-017-0055-6
Mary was born in 1948 in a small rural town in northern Ontario. After finishing grade eight, she went to work at the local general store to help her family out financially. Jack came into the store once a month when he got paid. Mary and Jack struck up a friendship and later got married.
The early years of their marriage were tough. Mary sensed that Jack had many ‘ghosts’ from his past, which he never spoke of. The few times Mary and Jack went to visit his family, she never felt comfortable or had the feeling that she or Jack were accepted. When she asked Jack about this, he refused to talk about it. So Mary settled into their marriage and worked hard at making a home for her husband and children. They had two children, Phillip and Nancy.
Five years after they got married, Mary and Jack could finally afford to buy their own home. It was a lovely two-story home, with three bedrooms and one bathroom on the second floor. It had a nice big backyard with lots of gardens, which Mary loved to tend. This home was Mary’s pride and joy, and a source of many happy memories for her: this is where she raised her children, took care of her husband, and entertained her lady friends from church. Mary was happy in life as a stay-at-home mother and housewife.
Over the last few years, Mary has been having difficulties with maintaining their home both inside and out. Mary has been slowing down with her indoor and outdoor activities due to joint pain and stiffness. Both of her children have moved far away, and Jack has health issues which affect how much he is able to help Mary with the upkeep of their home.
In 2012, Mary went to see her family physician because the OTC medications she had been taking were no longer relieving her joint pain and stiffness. After a thorough physical examination and some diagnostic tests, Mary was diagnosed with Stage 4 osteoarthritis (OA) and osteoporosis (OP).
Mary’s OA was affecting her mobility and her ability to perform basic activities of daily living (ADLs). Jack assisted Mary as much as possible, but was having some difficulties with his own ADLs. Jack would assist Mary downstairs in the morning. Mary wore an incontinence product as she was unable to get up the stairs to the bathroom in time.
Due to the pain Mary was having from her OA and OP, her physician prescribed hydrocodone for the pain. By 2018, Mary was having increased difficulty with mobility and required a walker. She seldom left the house anymore as getting around proved to be challenging. She missed gardening, going to church, and visiting with her friends.
In the spring of 2018, she experienced a fall in the bathroom, resulting in a fractured right hip. Surgical intervention was required, and Mary had a total right hip arthroplasty. The plan upon discharge from the hospital was that Mary and Jack would move in with Nancy and Paul in the GTA. Mary’s hospital stay was extended due to Jack’s hospitalization.
The weeks that followed Mary’s discharge and subsequent move to her daughter’s home saw Mary become more withdrawn, often spending the day in her pajamas, unwashed and distant from those around her. Mary is struggling with the many changes happening in her and Jack’s life.
Case Key Words
Bone
Depression
Elder fall
Fractured hip
Hip replacement
Joint
Mixed marriage
Opioids
Osteoarthritis
Osteoporosis
Mary's Health: Osteoarthritis (OA)
Mary was diagnosed with Stage 4 osteoarthritis (OA) and osteoporosis(OP) in 2012.
Diagnosis
Physical examination checks affected joints for tenderness, swelling, redness, and flexibility
Imaging tests
X-ray
Magnetic resonance imaging
Bone densitometry
Lab tests
Blood tests
Joint fluid analysis
Hand
Hip
Pain on ROM
Hypertrophic changes at distal and proximal interphalangeal joints (Heberden nodes-1 & Bouchard nodes-2)
Tenderness over carpometacarpal joint of thumb
Pain on ROM
Pain in buttock
Limitation of ROM, especially internal rotation
Shoulder
Foot
Pain on ROM
Limitation of ROM, especially external rotation
Crepitus on ROM
Pain on ambulation, especially at 1st metatarsophalangeal joint
Limited ROM of 1st metatarsophalangeal joint, hallux rigidus
Cartilage is affected, narrow gap between bone and joint
Joint becomes inflamed, discomfort with ADLs
OTC pain medication or prescription pain medications, hyaluronic injections
Stage 4 – Severe
Cartilage is almost completely gone, bone spurs have multiplied, very painful
Inflammatory response from the joint
OTC pain medication or prescription pain medications, hyaluronic injections
Bone realignment surgery for knee & hip
X-rays
Osteoarthritic Hip and Spine
Types of spinal degeneration. (a–b) Horizontal degeneration. Initial degeneration of the intervertebral disc (a) subsequently leads to the facet joint osteoartritis (b). (c–d) Adjacent segment disease. Severe degenerative changes on a segment result in abnormalities in the level above
Stepped-Care Approach for the Treatment of OA
OA cannot be reversed. However, treatments can reduce pain and improve movement.
Medications Commonly Used for OA
Medication
Typical Dosage
Acetaminophen
650 to 1000 mg QID
Celecoxib (Celebrix)
50 to 400 mg OD
Diclofenac/misoprostol (Arthrotec)
50 mg/200 mcg BID-TID
Ibuprofen (OTC)
400 to 600 mg TID
Meloxicam (Mobic)
7.5 to 15 mg OD
Nabumetone
500 mg BID
Naproxen (OTC) (Aleve)
220 to 440 mg BID
Oxaprozin (Daypro)
1200 mg OD
Sulindac (Clinoril)
150 to 200 mg BID
OTC Medications Aren’t Working…
Strong medications may be prescribed if OTC medications lose effectiveness:
Opioids
Low dosages and careful monitoring
May cause chronic constipation
Older patients at risk of falls
Intra-articular injections of corticosteroids or hyaluronic acid
Short-term relief lasting 4 to 8 weeks
May cause flare-up within the first 24 hours
Improvement from baseline at 48 hours
Mary's Health: Osteoporosis (OP)
Typically, there are no symptoms in the early stages of OP.
Mary though the back pain was part of growing old, along with the being a ‘bit shorter’ & the slight stoop in her posture.
Overview
Causes bones to become weak & brittle
A fall or even mild stress can cause a fracture
OP related fractures most commonly occur in the hip, wrist, or spine
Bone is living tissue that is constantly being broken down & replaced
OP occurs when the creation of new bone doesn’t keep up with the loss of old bone
OP affect men & women of all races
White & Asian women (especially post-menopause) are at higher risk
Causes
After the early 20s the process of making new bone slows
Most people reach their peak bone mass by age 30
How likely you are to develop OP depends partly on how much bone mass you attained in your youth
Peak bone mass is somewhat inherited and also varies by ethnic group
Intramembranous Ossification
Intramembranous ossification follows four steps:
Mesenchymal cells group into clusters, and ossification centers form.
Secreted osteoid traps osteoblasts, which then become osteocytes.
Trabecular matrix and periosteum form.
Compact bone develops superficial to the trabecular bone, and crowded blood vessels condense into red marrow.
Endochondral Ossification
Endochondral ossification follows six steps:
Mesenchymal cells differentiate into chondrocytes.
The cartilage model of the future bony skeleton and the perichondrium form.
Capillaries penetrate cartilage. Perichondrium transforms into periosteum. Periosteal collar develops. Primary ossification center develops.
Cartilage and chondrocytes continue to grow at ends of the bone.
Secondary ossification centers develop.
Cartilage remains at epiphyseal (growth) plate and at joint surface as articular cartilage.
Risk Factors
Modifiable Risks
Non-modifiable Risks
Alcohol
Age
Smoking
Ethnicity
Low body mass index (BMI)
Female gender
Poor nutrition
Family history of fractures
Eating disorders
Previous fractures
Insufficient physical activity
Menopause/hysterectomy
Low dietary calcium intake
Hormonal status
Vitamin D deficiency
Long-term glucocorticoid therapy
Frequent falls
Primary/secondary hypogonadism in men
Complications
Bone fractures:
Particularly in the spine or hip
Often caused by a fall & can result in disability
Increase risk of death within the first year after injury
Spinal fractures can occur without injury
Vertebrae can weaken to the point of crumpling
Prevention:
Good nutrition
Maintain a health body weight
Calcium
Vitamin D
Exercise
Limit alcohol consumption
Quit smoking
Mary's Health: Hip Fracture
Due to her existing OA and OP, Mary’s fall resulted in a fractured hip that required surgical repair.
Symptoms:
Inability to get up from a fall or to walk
Severe pain in hip or groin
Inability to weight bear on the affected side
Bruising & swelling in & around hip area
Shorter leg on the affected side
Outward rotation of the leg on the affected side
Surgical Repair
The type of repair depends on where & how severe the fracture is, displaced bone, age, & underlying health conditions.
Options include:
Internal repair using screws
Total hip replacement
Partial hip replacement
Rehabilitation
Out of bed and moving on the 1st day post-op
Physical therapy will initially focus on ROM and strengthening exercises
Home exercise program and follow-up PT appointments
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). Synovial Joints. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). The Functions of the Skeletal System. Anatomy and Physiology. OpenStax.
Clynes, M. A., Harvey, N. C., Curtis, E. M., Fuggle, N. R., Dennison, E. M., & Cooper C. (2020). The epidemiology of osteoporosis. British Medical Bulletin, 133(1), 105-117.
Bone Tissue and the Skeletal System. (2013). In J. G. Betts, K. A. Young, J. A. Wise, E. Johnson, B. Poe, D. H. Kruse, . . . P. DeSaix, Anatomy and Physiology. OpenStax. https://openstax.org/books/anatomy-and-physiology
Chow, Y. Y., & Chin, K. Y. (2020). The role of inflammation in the pathogenesis of osteoarthritis. Mediators of Inflammation, 1-19. https://doi.org/10.1155/2020/8293921
Clynes, M. A., Harvey, N. C., Curtis, E. M., Fuggle, N. R., Dennison, E. M., & Cooper C. (2020). The epidemiology of osteoporosis. British Medical Bulletin, 133(1), 105-117. https://doi.org/10.1093/bmb/ldaa005
Ghouri, A., & Conaghan, P. G. (2020). Prospects for therapies in osteoarthritis. Calcified Tissue International, 109, 339-350. https://doi.org/10.1007/s00223-020-00672-9
John M. Eisenberg Center for Clinical Decisions and Communications Science (2012). Preventing blood clots after hip or knee replacement surgery or surgery for a broken hip: A review of the research for adults. In: Comparative Effectiveness Review Summary Guides for Consumers. www.ncbi.nlm.nih.gov/books/NBK107165/
Yang, T. L., Shen, H., Liu, A., Dong, S. S., Zhang, L., Deng , F. Y., Zhao, Q., & Deng, H. W. (2020). A road map for understanding molecular and genetic determinants of osteoporosis. Nature Reviews Endocrinology, 16, 91-103. https://doi.org/10.1038/s41574-019-0282-7
Phillip was born in a small town in northern Ontario in 1979 to biracial parents. His father, Jack, was Ojibway, and his mother, Mary, was Anglican. He was six years old when he became a big brother to Nancy. Phillip was known as a ‘sensitive boy’ when he was younger. He did not have any interest in sports, much to his father’s dismay. Phillip loved to spend time with his mother: cuddling on her lap, helping her out in the kitchen, and watching her get ready for parties.
Once Phillip started school, some of the other children bullied him: calling him names, physically pushing him around, and ostracizing him when it came time for teamwork.
As the siblings grew older, Phillip watched his sister Nancy play numerous sports while his father cheered her on and commented to Phillip that “this was what he should be doing if he was a real boy.” Phillip’s self-esteem plummeted. He would often ask himself “what is wrong with me?”
Once he started high school, Phillip felt even more alone and more confused. He was not interested in sports or girls like his classmates. He secretly had a ‘crush’ on another boy at his high school but did not dare to act upon his feelings. By grade 11, Phillip could no longer take the bullying of his schoolmates, the whispers and comments from the small community in which he lived, and the disappointment he saw on his father’s face every day.
At 16, Phillip left his small hometown without a word to anyone, and headed for Toronto. There he soon found a community of individuals that accepted him. It was an exciting time for Phillip, with drinking, drugs, and multiple same-sex partners. This reckless lifestyle continued for many years. His drinking increased and eventually he began using IV drugs. Phillip went from one relationship to another, often having multiple partners at the same time. He had no contact with his family since he left home, and often wondered if they cared where he was and what he was doing. He had called home a number of times, but hung up as soon as someone answered the phone.
It was in the late fall of 2008 that Phillip came down with the “flu”.
Flu-like symptoms can include:
Fever
Chills
Rash
Night sweats
Muscle aches
Sore throat
Fatigue
Swollen lymph nodes
Mouth ulcers
These symptoms lasted a few weeks, but eventually Phillip started feeling better. His close friends were concerned about his weight loss and suggested that he get tested for HIV. Phillip was not concerned because he was feeling better, and thought to himself “I use condoms most times, HIV could not possibly happen to me.” He continued with his reckless lifestyle for another ten years.
Phillip had been feeling unwell again. He had lost even more weight, was tired all the time, and noticed ‘blotches’ on his face and in his mouth.
After three months with no improvement, Phillip went to a local medical clinic for assessment. The attending physician provided testing to confirm his suspicions of HIV/AIDS.
With positive results, Phillip was referred to a specialist trained in treating HIV.
The specialist ordered further testing to determine the stage of the disease and the best treatment options. He ordered other lab tests to check for a number of infections or complications often related to HIV.
Phillip was distraught over the diagnosis and treatment. He felt like this was a death sentence. After much consideration, he decided to reach out to his sister for support.
Nancy was sympathetic, but stated that there was not much she could do to help out as her ‘plate was overflowing’ at present. She did suggest that Phillip could come visit Nancy and her family once a month, but when he found out his parents were living there too, he quickly declined the offer.
Phillip contemplated trying to reach out to his father’s people. He had struggled all his life with feeling like he didn’t belong. Would they accept him?
Phillip is considered a two spirited person (both male and female spirits). Two spirited people were held in high regard. However, due to residential schools and the church’s influence on Indigenous people, many were taught that this type of lifestyle was unacceptable. While many communities would not accept Phillip, many others were now coming around and realizing that rejecting him for his gender and sexuality was not their traditional way. However, if the community was very traditional, Phillip’s drug use could also be a problem.
Case Key Words
Addiction
AIDS
Biracial
HIV
Homosexual
Indigenous
IV drug use
LGBTQ+
Risk behaviours
Self-identity
Barriers to LGBTQ+ Health
LGBTQ+ Risk Factors for Mental Health Problems
Harassment & Discrimination in Education
About three quarters of LGBTQ+ students report having been harassed at school; even worse, 35% have experienced physical assault, and 12% have been the victim of sexual violence at school.
Harassment and assault, especially when it occurs in what should be a safe and supportive setting, can have serious impacts on mental health such as fear, anxiety, depression, and post-traumatic stress disorder (PTSD).
Institutional Discrimination
The LGBTQ+ population experiences institutional discrimination in a variety of situations and settings such as the workplace and places of worship.
LGBTQ+ individuals are frequently denied career advancement or equal compensation compared with their gender-conforming peers, and their unemployment rate is double that of the general population.
Health Disparities
Discrimination in health care settings endangers LGBTQ+ people’s lives through delays or denials of medically necessary care. Transgender patients may require medical interventions such as hormone therapy and/or surgery.
Other common barriers are discrimination, lack of insurance, lack of cultural competence/sensitivity by health care providers, and socioeconomic barriers such as low income, lack of transportation, and inadequate housing.
Family Rejection
Family rejection can also lead to long-lasting psychiatric problems later in life.
Rejected individuals may develop depression and low self-esteem and may turn to alcohol, cigarettes, or drugs, smoking cigarettes to cope.
History of Trauma
Many individuals in the LGBTQ+ population have experienced past physical assault and harassment.
Past trauma compounds any current trauma, exacerbating anxiety about future safety, especially in a political climate that feels hostile.
Microtraumas/Microaggressions
People who identify as LGBTQ+ often experience brief, subtle expressions of hostility or discrimination.
While microaggressions are often associated with racial/ethnic minorities, they can also impact LGBTQ+ and other marginalized populations, and cumulatively they can take a toll on mental and physical health.
LGBTQ+ people who experience microtraumas may not meet diagnosable criteria for PTSD yet suffer tremendously from minority stressors such as from internalized phobia, rejection sensitivity, marginalization, and discrimination both in their personal life and health care settings.
Phillip's Health: HIV/AIDS
New Community…New Life
Phillip moved to Toronto
Found a community that accepted him
Exciting time for Phillip – drinking, drugs, multiple same-sex partners
Soon turned to IV drugs
No contact with his family
Phillip Catches the ‘Flu’
Phillip is now 29 years of age
Comes down with flu-like symptoms:
Fever
Chills
Rash
Night sweats
Muscle aches
Sore throat
Fatigue
Swollen lymph nodes
Mouth ulcers
These symptoms last a few weeks
He is feeling better
Close friends are concerned about Phillip’s weight loss and suggest he get tested for HIV
10 Years Later…
Phillip is feeling unwell
Lost even more weight
Tired all the time
Noticed ‘blotches’ on his face & in his mouth
Phillip sees a physician at a local clinic
Doctor orders tests to confirm his suspicions of HIV/AIDS
Overview
What is HIV?
HIV (human immunodeficiency virus) is a virus that attacks the body’s immune system
If HIV is not treated, it can lead to AIDS (acquired immunodeficiency syndrome)
There is currently no effective cure. Once people get HIV, they have it for life
But with proper medical care, HIV can be controlled
People with HIV who get effective HIV treatment can live long, healthy lives and protect their partners
Where did HIV come from?
HIV infection in humans came from a type of chimpanzee in Central Africa
The chimpanzee version of the virus (called simian immunodeficiency virus, or SIV) was probably passed to humans when humans hunted these chimpanzees for meat and came in contact with their infected blood
Studies show that HIV may have jumped from chimpanzees to humans as far back as the late 1800s
Over decades, HIV slowly spread across Africa and later into other parts of the world. We know that the virus has existed in the United States since at least the mid to late 1970s
Diagnostic Testing
Antigen/Antibody Tests
These tests usually involve drawing blood from a vein. Antigens are substances on the HIV virus itself and are usually detectable — a positive test — in the blood within a few weeks after exposure to HIV.
Antibodies are produced by your immune system when it’s exposed to HIV. It can take weeks to months for antibodies to become detectable. The combination antigen/antibody tests can take two to six weeks after exposure to become positive.
Antibody Tests
These tests look for antibodies to HIV in blood or saliva. Most rapid HIV tests, including self-tests done at home, are antibody tests. Antibody tests can take three to 12 weeks after you’re exposed to become positive.
Nucleic Acid Tests (NATs)
These tests look for the actual virus in your blood (viral load). They also involve blood drawn from a vein. If you might have been exposed to HIV within the past few weeks, your doctor may recommend NAT. NAT will be the first test to become positive after exposure to HIV.
Other Lab Tests
Tuberculosis
Hepatitis B or Hepatitis C virus infection
STIs
Liver or kidney damage
Urinary tract infection
Cervical and anal cancer
Cytomegalovirus
Toxoplasmosis
Further Testing
Determines the stage of the disease & the best treatment options.
CD4 T Cell Count
CD4 T cells are white blood cells that are specifically targeted and destroyed by HIV. Even if you have no symptoms, HIV infection progresses to AIDS when your CD4 T cell count dips below 200.
Viral Load (HIV/RNA)
This test measures the amount of virus in your blood. After starting HIV treatment the goal is to have an undetectable viral load. This significantly reduces your chances of opportunistic infection and other HIV-related complications.
Drug Resistance
Some strains of HIV are resistant to medications. This test helps your doctor determine if your specific form of the virus has resistance and guides treatment decisions.
Stages of HIV
Stage 1: Acute HIV Infection
People have a large amount of HIV in their blood. They are very contagious.
Some people have flu-like symptoms. This is the body’s natural response to infection.
But some people may not feel sick right away or at all.
If you have flu-like symptoms and think you may have been exposed to HIV, seek medical care and ask for a test to diagnose acute infection.
Only antigen/antibody tests or nucleic acid tests (NATs) can diagnose acute infection.
Stage 2: Chronic HIV Infection
This stage is also called asymptomatic HIV infection or clinical latency.
HIV is still active but reproduces at very low levels.
People may not have any symptoms or get sick during this phase.
Without taking HIV medicine, this period may last a decade or longer, but some may progress faster.
People can transmit HIV in this phase.
At the end of this phase, the amount of HIV in the blood (called viral load) goes up and the CD4 cell count goes down. The person may have symptoms as the virus levels increase in the body, and the person moves into Stage 3.
People who take HIV medicine as prescribed may never move into Stage 3.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). Leukocytes and Platelets. Anatomy and Physiology. OpenStax.
Back, D., & Marzolini, C. (2020). The challenge of HIV treatment in an era of polypharmacy. Journal of the International AIDS Society, 23(2), e25449. https://doi.org/10.1002/jia2.25449
Kelly, B. C., Carpiano, R. M., Easterbrook, A., & Parsons, J. T. (2012). Sex and the community: The implications of neighbourhoods and social networks for sexual risk behaviours among urban gay men. Sociology of Health & Illness, 34(7), 1085-1102. https://doi.org/10.1111/j.1467-9566.2011.01446.x
Kodadek, L. M., Peterson, S., Shields, R. Y., German, D., Ranjit, A., Snyder, C., . . . Haider, A. H. (2019). Collecting sexual orientation and gender identity information in the emergency department: The divide between patient and provider perspectives. Emergency Medicine Journal, 36(3), 136-141. https://doi.org/10.1136/emermed-2018-207669
Matthews A., K., Breen, E., & Kittiteerasack, P. (2018). Social determinants of LGBT cancer health inequities. Seminars in Oncology Nursing, 34(1), 12-20. https://doi.org/10.1016/j.soncn.2017.11.001
Mulé, N. J., Ross, L. E., Deeprose, B., Jackson, B. E., Daley, A., Travers, A., & Moore, D. (2009). Promoting LGBT health and wellbeing through inclusive policy development. International Journal for Equity in Health, 8(18), 1-11. https://doi.org/10.1186/1475-9276-8-18
Ryan, C., Jackson, R., Gabel, C., King, A., Masching, R., & Thomas, C. (2020). Successful aging: Indigenous men aging in a good way with HIV/AIDS. Canadian Journal on Aging, 39(2), 305-317. https://doi.org/10.1017/S0714980819000497
Nancy, born in 1985, was the second child of Mary and Jack. She lived with her parents and older brother, Phillip, in a small rural town in Northern Ontario. She was a very active child, to the point that some would call her a “Tomboy”. Nancy played many sports at school and in local leagues. She was quite competitive. Nancy enjoyed the company of her father, spending many days fishing and hunting with him.
Neither Nancy nor Phillip had many friends at school. They never really felt like they ‘fit in’ with the other kids. She was ‘too white’ for some kids and ‘too native’ for others. When she was younger she was often teased and called names. Between not fitting in and the pressure to fulfill her father’s desires to have an athlete in the family, Nancy pushed herself physically. She felt comfortable in her father’s quiet presence.
When Nancy reached her teenage years, she played basketball, hockey, ran a number of events in track and field, and competed in gymnastics. She loved to win, and had many trophies and ribbons in her bedroom. Her father was very proud of her accomplishments. With these sports taking up much of Nancy’s time, her school grades were average due to competing priorities.
Mary was concerned about her daughter’s health and wellbeing. She often discussed her concerns with Jack, but was dismissed as being overprotective. One day, Nancy’s school called and asked Mary to come and pick her up. Nancy had injured her leg during a 10 km run.
Mary took Nancy to the local emergency department, as Nancy was in considerable pain and unable to bear weight on her left leg. The emergency physician ordered an x-ray of Nancy’s left leg, blood work, and did a physical exam. The diagnosis was a stress fracture of the left tibia.
However, the physician was more concerned about Nancy’s appearance and her story. The physician followed-up with a more comprehensive history from both Nancy and her mother. What come to light was the following:
Fatigue (Nancy stated that she always felt tired, and would fall asleep if she sat still for more than 5 minutes)
Weight loss (Nancy’s BMI is 15.7)
Absent menstrual periods for the last six months (in the last year, Nancy had only 2 very light periods)
Periods of fasting, binging, and self-induced vomiting (purging)
Extreme exercise (Nancy ran 10 kilometers each day, had morning and after-school practices, games and competitions, and competed in a number of events each weekend)
Based on the clinical findings, the emergency physician diagnosed Nancy with Female Athlete Triad. It was explained to Nancy and her mother as an interrelationship of menstrual dysfunction, low energy availability (with or without an eating disorder), and decreased bone mineral density. It is relatively common among young women who participate in sports, but has the potential to be a serious condition. Diagnosis and treatment are complicated and often require an interdisciplinary team.
Nancy’s story continues…
Nancy met with all of the healthcare specialists that the emergency physician referred her to, and a multidisciplinary team for Nancy’s case was formed. They were all in agreement that Nancy should refrain from sports until she was cleared for return-to-play.
Her father did not see what all the fuss was about. He urged Nancy to get back to what she loved to do.
Nancy went to all her appointments to satisfy her mother and family doctor. However, she continued to binge and purge behind her mother’s back. She would often skip class to go running.
It took three years of hard work for Nancy to reach a healthy weight, eat well, and have a healthy outlook on exercise and activity. She continued with oligomenorrhea, however.
Nancy went away to university and began to work out and run again. After she graduated, she obtained a financial job in Toronto. She was working out and running twice a day to cope with the stress in her life. It was a lifestyle that she could not give up, and now that she was on her own, she had total control over her body. She was obsessed with maintaining an ‘ideal weight’ and fell back into the binging and purging of food.
She met Paul through mutual friends. They started dating in 2010, eventually marrying in 2012. About two years after they got married, they started talking about having a family. Paul had adopted twin girls from a previous marriage that they saw very infrequently.
Nancy and Paul began trying to conceive in 2013. By 2016, Nancy and Paul had seen fertility specialists. They were not hopeful that Nancy could conceive due to her history and ongoing struggle with exercise and eating, as well as the increased amount of stress in her life.
It was 2019, Nancy was successful in her career, and going to school for her CPA certification. She was relying on Paul to help out around the house, but had some concerns about his use of pain medication. Despite her concerns, Nancy wanted to be a mother and since they had no luck with conceiving or with costly in-vitro fertilization, they decided to adopt. In January 2020, they were notified that a toddler named Sam was available for adoption.
Shortly after Sam arrived to live with them, Jack called and told Nancy that Mary was in hospital. She had fallen and fractured her hip, and would be having a total hip replacement the next day. Jack stated that they would have to come and stay with Nancy and Paul while Mary recuperated from her surgery, as their family home was not suitable for Mary post-operatively. Nancy asked her father about staying with her brother Phillip, but Jack would not consider that as an option.
Nancy had no choice but to book time off work, and arrange for someone to come in and help with Sam, Paul, and the housework while she was away for a few days. She hoped to find the time to continue with her studies while she was away. She was not sure if her parents had internet, so her back-up plan was to go to the local library a few hours each day.
Nancy arrived a few days prior to her mother’s discharge to help pack up what her mother and father would need while they stayed at her house. Instead, she found her father in need of medical attention and brought him into the emergency department at the local hospital, where he was quickly admitted.
Nancy was now in a dilemma as both of her parents were in hospital. Her mother was due to be discharged the next day. The plan had been for Nancy to take both of her parents to stay with her while her mother recuperated. She needed to get home to her son, husband, and her studies.
Nancy spoke with the discharge planner and explained the situation. Mary would be transferred to the Alternative Level of Care Unit until Jack was ready for discharge. Nancy then called her husband Paul to discuss what she should do.
Nancy returned home the next day to prepare for her parents’ arrival. Over the next week, Nancy was consumed by the sheer amount of preparations required.
Meanwhile, Sam required multiple appointments, extra care, monitoring, and a special diet. Paul was not being helpful, instead often being distant with both Nancy and Sam.
To cope with the significant added stress in her life, Nancy fell back into her old behaviours: binge eating, then feeling guilty and purging. She was extremely stressed by all of the decisions she needed to make for her parents and her new son, along with dealing with her husband’s erratic behaviour and narcotics use.
Case Key Words
Adoption
Binge eating
Biracial
Eating disorders
Female Athlete Triad
In Vitro fertilization (IVF)
Stress eating
Stress fracture
Stress response
Nancy's Health: Stress Fracture
At age 15, Nancy injured her leg during a gymnastics practice.
She was in considerable pain & could not weight bear
Taken to the local emergency department by her mother
X-ray & blood work were ordered
Diagnosis: stress fracture of the left tibia
Causes
Many factors can contribute to stress fractures of the shin. Some can be managed and others can not.
Repetitive movements in high-intensity activities such as long-distance running, track & field, basketball, soccer, gymnastics, dance
Improper athletic technique or footwear
Increasing training or weight-bearing exercises too quickly
Not getting enough rest between workouts
Working out on a different type of surface than usual
Excessive alcohol consumption
Smoking
Being over- or underweight
Osteoporosis
Eating disorders
Low vitamin D levels
Calorie intake imbalance
Treatment
Physician will recommend a combination of treatments & lifestyle changes:
Taking a break from high-impact activity until you’re fully healed
Elevating your leg and applying ice for 10 minutes to ease pain and swelling
Taking over-the-counter (OTC) anti-inflammatory medicine
Using crutches to keep weight off your shin while you heal
Physical therapy
Severe stress fractures may require a cast or surgery to ensure proper healing
Take 4-12 weeks (sometimes longer) to heal
Increase activity slowly
Sports medicine specialist or qualified trainer can help redesign workout routine
Additional Tips for Healing
Rest
Start cross-training
Invest in proper footwear
Elevate and ice
Maintain a healthy diet
Manage your weight
Work with an experienced trainer
Nancy's Health: Female Athlete Triad
Nancy’s Story Continues…
The emergency physician was more concerned about Nancy’s appearance & how she injured herself.
A more comprehensive history & examination followed.
Assessment findings:
Extreme fatigue (stated she always felt tired, would fall asleep if she sat still for more than 5 minutes)
Weight loss (Nancy’s BMI is 15.7)
Absence of menstrual periods for the last 6 months (stated she had only 2 very light periods in the last year)
Eating disorder – fasting, binging, self-induced vomiting (indulged in all of these practices regularly)
Extreme exercise (Nancy ran 10km each day, had morning & after school practices, games & competitions, & competed in a number of events each weekend)
Based on clinical findings, Nancy was diagnosed with:
Female Athlete Triad
Low energy availability
Menstrual dysfunction
Poor bone health
Body Mass Index (BMI)
Person’s weight in kg divided by the square of height in meters.
Can be used to screen for weight categories that may lead to health problems.
However, it is not diagnostic of the body fatness or health of an individual.
It is recommended that screening for the Triad be part of the Pre-Participation Physical Evaluation.
Screening Questions:
Have you ever had a menstrual period?
How old were you when you had your first menstrual period?
When was your most recent menstrual period?
How many periods have you had in the past 12 months?
Are you presently taking any female hormones (oestrogen, progesterone, birth control pills)?
Do you worry about your weight?
Are you trying to or has anyone recommended that you gain or lose weight?
Are you on a special diet or do you avoid certain types of foods or food groups?
Have you ever had an eating disorder?
Have you ever had a stress fracture?
Have you ever been told you have low bone density (osteopenia or osteoporosis)?
Bone Mineral Density & Osteoporosis in Ages 15-19
The diagnosis of osteoporosis in children and adolescents requires the presence of both a clinically significant fracture history AND low bone mineral content or low bone mineral density
A clinically significant fracture history is one or more of the following:
Long bone fracture of the lower extremities
Vertebral compression fracture
Two or more long-bone fractures of the upper extremities
Treatment
The three components of the Triad recover at different rates with the appropriate treatment.
Recovery of energy status is typically observed after days or weeks of increased energy intake and/or decreased energy expenditure.
Recovery of menstrual status is typically observed after months of increased energy intake and/or decreased energy expenditure, which improves energy status.
Recovery of bone mineral density may not be observed until years after recovery of energy status and menstrual status has been achieved. IGF-1, insulin-like growth factor-1.
Nancy's Health: Eating Disorders
Nancy’s Story Continues…
Nancy met with her multidisciplinary healthcare team as scheduled
Her mother watched her closely, recording her food intake, physical activity, sleep patterns, and her menstrual cycles
Her father did not see what all the fuss was about… ”go back to doing what you love”
She went to her appointments to appease her mother and family doctor
She continued to binge & purge
She often skipped classes to go running
It took 3 years of hard work for her to get to a healthy weight, have a realistic view on exercise, & to having monthly menstrual periods
Overview
Eating disorders are persistent eating behaviours that negatively impact your health, emotions, & your ability to function.
Focuses on weight, body shape & food, leading to dangerous eating behaviours.
Eating disorders can harm the heart, digestive system, bones, teeth & mouth, & lead to other diseases.
Most common eating disorders are:
Anorexia nervosa
Bulimia nervosa
Binge-eating disorder
Symptoms
Anorexia Nervosa
Dramatic weight loss
Dresses in layers to hide weight loss or stay warm
Preoccupation with weight, food, calories, fat grams, and dieting. Makes frequent comments about feeling “fat”
Resists or is unable to maintain a body weight appropriate for their age, height, and build
Maintains an excessive, rigid exercise regime – despite weather, fatigue, illness, or injury
Bulimia Nervosa
Evidence of binge eating, including disappearance of large amounts of food in short periods of time or lots of empty wrappers and containers indicating consumption of large amounts of food
Evidence of purging behaviors, including frequent trips to the bathroom after meals, signs and/or smells of vomiting, presence of wrappers or packages of laxatives or diuretics
Drinks excessive amounts of water or non-caloric beverages, and/or uses excessive amounts of mouthwash, mints, and gum
Has calluses on the back of the hands and knuckles from self- induced vomiting
Dental problems, such as enamel erosion, cavities, discoloration of teeth from vomiting, and tooth sensitivity
Binge Eating Disorder
Secret recurring episodes of binge eating (eating in a discrete period of time an amount of food that is much larger than most individuals would eat under similar circumstances); feels lack of control over ability to stop eating
Feelings of disgust, depression, or guilt after overeating, and/or feelings of low self-esteem
Steals or hoards food in strange places
Creates lifestyle schedules or rituals to make time for binge sessions
Evidence of binge eating, including the disappearance of large amounts of food in a short time period or a lot of empty wrappers and containers indicating consumption of large amounts of food
Causes
Genetics & biology
Certain people may have genes that increase their risk of developing eating disorders. Biological factors, such as changes in brain chemicals, may play a role in eating disorders.
Psychological & emotional health
People with eating disorders may have psychological and emotional problems that contribute to the disorder. They may have low self-esteem, perfectionism, impulsive behavior and troubled relationships.
Risk Factors
Family history
Eating disorders are significantly more likely to occur in people who have parents or siblings who’ve had an eating disorder.
Other mental health disorders
People with an eating disorder often have a history of an anxiety disorder, depression or obsessive-compulsive disorder.
Dieting & starvation
Dieting is a risk factor for developing an eating disorder. Starvation affects the brain and influences mood changes, rigidity in thinking, anxiety and reduction in appetite. There is strong evidence that many of the symptoms of an eating disorder are actually symptoms of starvation. Starvation and weight loss may change the way the brain works in vulnerable individuals, which may perpetuate restrictive eating behaviors and make it difficult to return to normal eating habits.
Stress
Whether it’s heading off to college, moving, landing a new job, or a family or relationship issue, change can bring stress, which may increase your risk of an eating disorder.
Complications
Serious health problems
Depression & anxiety
Suicidal thoughts or behaviour
Problems with growth & development
Social & relationship problems
Substance use disorders
Work & school issues
Death
Nancy's Health: In Vitro Fertilization
Wanting to Conceive
Nancy is now in her early 30’s
She came to the point in her life where she wanted to have a baby
Paul & Nancy tried to conceive for a number of years
Nancy was unsure as ‘whose fault’ it was (Paul had adopted children from his first marriage)
The fertility specialist suggested IVF (in vitro fertilization)
IVF is the most effective form of assisted reproductive technology
Chances of conceiving using IVF depend on many factors (e.g. age & cause of infertility)
Can be time-consuming, expensive & invasive
Overview
During IVF, eggs are removed from mature follicles within an ovary
An egg is fertilized by injecting a single sperm into the egg or mixing the egg with sperm in a petri dish
The fertilized egg (embryo) is transferred into the uterus
Why IVF?
Fallopian tube damage or blockage
Ovulation disorders
Endometriosis
Uterine fibroids
Previous tubal sterilization or removal
Impaired sperm production or function
Unexplained infertility
A genetic disorder
Fertility preservation for cancer or other health conditions
Risks
Multiple births
IVF increases the risk of multiple births if more than one embryo is transferred to your uterus. A pregnancy with multiple fetuses carries a higher risk of early labor and low birth weight than pregnancy with a single fetus does.
Premature delivery and low birth weight
Research suggests that IVF slightly increases the risk that the baby will be born early or with a low birth weight.
Ovarian hyper stimulation syndrome
Use of injectable fertility drugs, such as human chorionic gonadotropin (HCG), to induce ovulation can cause ovarian hyper stimulation syndrome, in which your ovaries become swollen and painful.
Symptoms typically last a week and include mild abdominal pain, bloating, nausea, vomiting and diarrhea. If you become pregnant, however, your symptoms might last several weeks. Rarely, it’s possible to develop a more severe form of ovarian hyper stimulation syndrome that can also cause rapid weight gain and shortness of breath.
Miscarriage
The rate of miscarriage for women who conceive using IVF with fresh embryos is similar to that of women who conceive naturally — about 15% to 25% — but the rate increases with maternal age.
Egg-retrieval procedure complications
Use of an aspirating needle to collect eggs could possibly cause bleeding, infection or damage to the bowel, bladder or a blood vessel. Risks are also associated with sedation and general anesthesia, if used.
Ectopic pregnancy
About 2% to 5% of women who use IVF will have an ectopic pregnancy — when the fertilized egg implants outside the uterus, usually in a fallopian tube. The fertilized egg can’t survive outside the uterus, and there’s no way to continue the pregnancy.
Birth defects
The age of the mother is the primary risk factor in the development of birth defects, no matter how the child is conceived. More research is needed to determine whether babies conceived using IVF might be at increased risk of certain birth defects.
Cancer
Although some early studies suggested there may be a link between certain medications used to stimulate egg growth and the development of a specific type of ovarian tumor, more-recent studies do not support these findings. There does not appear to be a significantly increased risk of breast, endometrial, cervical or ovarian cancer after IVF.
Stress
Use of IVF can be financially, physically and emotionally draining. Support from counselors, family and friends can help you and your partner through the ups and downs of infertility treatment.
Preparing for IVF
Ovarian reserve testing
To determine the quantity and quality of your eggs, your doctor might test the concentration of follicle-stimulating hormone (FSH), estradiol (estrogen) and anti-mullerian hormone in your blood during the first few days of your menstrual cycle. Test results, often used together with an ultrasound of your ovaries, can help predict how your ovaries will respond to fertility medication.
Semen analysis
If not done as part of your initial fertility evaluation, your doctor will conduct a semen analysis shortly before the start of an IVF treatment cycle.
Infectious disease screening
You and your partner will both be screened for infectious diseases, including HIV.
Practice (mock) embryo transfer
Your doctor might conduct a mock embryo transfer to determine the depth of your uterine cavity and the technique most likely to successfully place the embryos into your uterus.
Uterine exam
Your doctor will examine the inside lining of the uterus before you start IVF. This might involve a sonohysterography — in which fluid is injected through the cervix into your uterus — and an ultrasound to create images of your uterine cavity. Or it might include a hysteroscopy — in which a thin, flexible, lighted telescope (hysteroscope) is inserted through your vagina and cervix into your uterus.
Important questions to discuss prior to beginning a cycle of IVF:
How many embryos will be transferred?
What will you do with any extra embryos?
How will you handle a multiple pregnancy?
Have you considered the potential complications associated with using donor eggs, sperm or embryos, or a gestational carrier?
What to Expect
Ovulation induction
At the start of a cycle, synthetic hormones are given to stimulate the ovaries to produce multiple eggs-rather than the single egg that normally develops each month.
Multiple eggs are needed, some eggs won’t fertilize or develop normally after fertilization.
Different medications that may be needed:
Medications for ovarian stimulation
To stimulate your ovaries, you might receive an injectable medication containing a follicle-stimulating hormone (FSH), a luteinizing hormone (LH) or a combination of both. These medications stimulate more than one egg to develop at a time.
Medications for oocyte maturation
When the follicles are ready for egg retrieval — generally after eight to 14 days — you will take human chorionic gonadotropin (HCG) or other medications to help the eggs mature.
Medications to prevent premature ovulation
These medications prevent your body from releasing the developing eggs too soon.
Medications to prepare the lining of your uterus
On the day of egg retrieval or at the time of embryo transfer, your doctor might recommend that you begin taking progesterone supplements to make the lining of your uterus more receptive to implantation.
Three days after fertilization, a normally developing embryo will contain about six to 10 cells.
By the fifth or sixth day, the fertilized egg is known as a blastocyst — a rapidly dividing ball of cells.
The inner group of cells will become the embryo.
The outer group will become the cells that nourish and protect it.
After the Procedure
After the embryo transfer, you can resume normal daily activities. However, your ovaries may still be enlarged. Consider avoiding vigorous activity, which could cause discomfort.
Typical side effects include:
Passing a small amount of clear or bloody fluid shortly after the procedure — due to the swabbing of the cervix before the embryo transfer
Breast tenderness due to high estrogen levels
Mild bloating
Mild cramping
Constipation
If you develop moderate or severe pain after the embryo transfer, contact your doctor. He or she will evaluate you for complications such as infection, twisting of an ovary (ovarian torsion) and severe ovarian hyperstimulation syndrome.
About 12-14 days after egg retrieval, a blood test will detect whether you are pregnant
Nancy's Health: Stress
Nancy’s Story Continues…
IVF was unsuccessful
Nancy’s stress levels were rising
After extensive discussions with Paul, they decided to adopt
They did not have to wait long
The adoption agency had a 2 year old boy – Sam
At about the same time Nancy’s mother fell and fractured her hip
She traveled north to assist her parents
She was shocked at the physical disarray her father was in
Her stress levels continued increasing with everything “on her plate”
She fell back into old eating habits
Eating was the one thing she felt she had control over
Overview
Stress is a natural physical & mental reaction to life experiences.
The body responds to stress by releasing hormones that increase your heart & breathing rates & ready your muscles to respond.
If your stress response doesn’t stop firing, it can take a toll on your health & overall well-being.
Irritability
Anxiety
Depression
Headaches
Insomnia
In response to stress, the hypothalamus (H) releases the corticotrophin releasing factor (CRF) into the anterior pituitary (P), causing the release of adrenocorticotropic hormone (ACTH) into the blood flow. ACTH stimulates the generation of glucocorticoids (cortisol in humans and corticosterone in mice) in the cortex of the adrenal gland (A), which are then released into the blood. Stress also activates the autonomic sympathetic nerves in the medulla of the adrenal gland to elicit the production of catecholamines, norepinephrine and epinephrine, which are then released into the blood. Glucocorticoids and catecholamines influence the generation of interleukins, which are involved in the viability and proliferation of immunocompetent gut cells via receptors.
Effects of Stress on the Body
Central Nervous and Endocrine Systems
CNS is in charge of the “fight or flight” response
The hypothalamus triggers the adrenal glands to release the stress hormones adrenaline & cortisol
Increasing heart rate & sending blood to the areas that need it the most (muscles, heart, other important organs)
When the perceived fear is gone, the hypothalamus tells all systems to go back to normal
If the stressor does not go away, the response will continue
Chronic stress is also a factor in behaviours such as overeating, not eating enough, alcohol, drug abuse, and social withdrawal
Respiratory and Cardiovascular Systems
Stress hormones affect the respiratory & cardiovascular systems
Breathing increases in an effort to quickly distribute oxygen-rich blood to the body
The heart pumps faster
Stress hormones cause the blood vessels to constrict & divert more oxygen to muscles
May also increase blood pressure
Frequent & chronic stress will make the heart work too hard for too long
Increase risk of stroke or heart attack
Digestive System
The liver produces extra blood sugar (glucose) to give a boost of energy
Under chronic stress, the body may not be able to keep up with the extra glucose surge
Chronic stress may increase the risk of developing type II diabetes
Rush of hormones, rapid breathing, increased heart rate may upset your digestive system
Can increase the risk for ulcers or cause existing ones to act up (ulcers are caused by a bacterium called H. pylori)
Stress may also affect the way food moves through the body, leading to diarrhea or constipation
May experience nausea, vomiting, stomachache
Muscular System
Muscles tense up to protect themselves from injury during stress
Once you relax they tend to release
Chronic stress may not give your muscles the chance to relax
Tight muscles cause headaches, back & shoulder pain, body aches
Over time this unhealthy cycle may affect your ability to exercise, & pain medication for relief may be used
Sexuality & Reproductive System
Not unusual to lose desire when under constant stress
Short-term stress may cause men to produce more testosterone, the effect doesn’t last long
Chronic stress will cause a man’s testosterone levels to drop
This can interfere with sperm production & cause erectile dysfunction or impotence
Chronic stress may increase risk of infection of male reproductive organs
For women, stress can affect the menstrual cycle
Irregular, heavier, or more painful menstrual periods
Chronic stress can also magnify the physical symptoms of menopause
Immune System
Stimulates the immune system, which is good for immediate situations
Over time, stress hormones weaken the immune system & reduce the body’s response to foreign invaders
Chronic stress causes more susceptibility to viral illnesses & other infections
Can increase the time it takes to recover from an illness or injury
Sandwich Generation
Nancy is now looking after a toddler & her parents
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). Connective Tissue Supports and Protects. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). Metabolism and Nutrition. Anatomy and Physiology. OpenStax.
Barrack, M. T., Gibbs, J. C., De Souza, M. J., Williams, N. I., Nichols, J. F., Rauh, M. J., & Nattiv, A. (2014). Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors. The American Journal of Sports Medicine, 42(4), 949-958. https://doi.org/10.1177/0363546513520295
De Souza, M. J., Nattiv, A., Joy, E., Misra, M., Williams, N. I., Mallinson, R. J., . . . Matheson, G. (2014). 2014 female athlete triad coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Fransisco, California, May 2012 and 2nd International conference held in Indianapolis, Indiana, May 2013. British Journal of Sports Medicine, 48(4). https://doi.org/10.1136/bjsports-2013-093218
Hay, P. (2020). Current approach to eating disorders: A clinical update. Internal Medicine Journal, 50(1), 24-29. https://doi.org/10.1111/imj.14691
Mallinson, R. J., & De Souza, M. J. (2014). Current perspectives on the etiology and manifestation of the “silent” component of the female athlete triad. International Journal of Women’s Health, 6(1), 451-467. https://doi.org/10.2147/IJWH.S38603
McKenzie, A. B. (2018). The grey zone: Growing up biracial in rural Canada. Journal of Historical Sociology, 31(1), e132-e138. https://doi.org/10.1111/johs.12198
Tenforde, A. S., Beauchesne, A. R., Borg-Stein, J., Hollander, K., McInnis, K., Kotler, D., & Ackerman, K. E. (2020). Awareness and comfort treating the female athlete triad and relative energy deficiency in sport among healthcare providers. German Journal of Sports Medicine, 71(3), 76-79. https://doi.org/10.5960/dzsm.2020.422
Sam was born in 2017, and adopted by Nancy and Paul when he was two. He is a typical toddler: good-natured and very inquisitive. Typically, before the finalization of an adoption, children are required to undergo a routine examination by a physician. However, the required examination is not meant to be a complete health screening, and many conditions are not even checked.
Patient History
There was little information available about Sam’s biological parents. However, it was known that they died in an automobile accident when Sam’s father suffered a massive heart attack, just before Sam turned 2. In the past two weeks since Sam was adopted, he has done very well adjusting to his new environment. Moreover, he has had all the proper immunizations for his age.
Sam’s adoptive parents have noticed some greasy/oily stools in his diapers. In addition, they are concerned about his wheezing when breathing. Nancy calls her family physician and gets a referral for Sam to see a pediatrician.
Initial visit
The initial visit with the pediatrician consisted of a physical examination, blood work, and a chest x-ray.
Follow-up visit
The weather was very hot and humid, which made it almost unbearable to be outside. Sam’s parents parked their car and brought Sam into the air-conditioned comfort of the Medical Centre pediatric clinic. Sam appears to be breathing easier once he is in the cool air.
They were immediately seen by the pediatrician, and Nancy expressed her concern over the colour of Sam’s sputum. She was upset that she had forgotten to tell the pediatrician the other day about this fact. The sputum Sam has been coughing up was green and viscid.
While talking with Nancy and Paul about Sam’s sputum, the pediatrician looked over at Sam and noticed a white ‘frosting’ on his face, an indication of salty build-up on the drying edge of sweat. The pediatrician asked Nancy and Paul if they had noticed this salty-build-up before.
“That must be why his skin tastes a bit salty when I kiss him on the cheek,” Nancy replied.
The pediatrician then went over the blood count and chest x-ray results with Nancy and Paul.
After describing the chest x-ray results to them, the pediatrician had a hypothesis about Sam’s condition. To test her hypothesis, the pediatrician ordered a sweat chloride test.
Sam was diagnosed with cystic fibrosis. Nancy and Paul would have to make many adjustments to care for Sam. He would require chest physical therapy, exercise, medications, digestive support, and psychosocial care.
Sam will most likely face significant challenges: frequent hospitalizations, complications such as CF-related diabetes, depression, anxiety, and time-consuming treatment plans that can take 2-3 hours each day.
Case Key Words
Adoption
Chest Physio
Cystic Fibrosis
Genetics
Immunizations
Lungs
Sam's Health: Cystic Fibrosis
Sam is a happy, energetic child and fully up to date on his immunizations.
Some Concerns
Nancy & Paul were concerned about the following:
They could hear Sam wheeze when he was breathing
Greasy/oily stools in his diaper
Family physician referred Sam to a pediatrician.
Initial Visit
Physical examination
Blood work
Chest x-ray
Physical Examination
Vital Signs
Age: 2 years, 6 months
Weight: 28 lbs. (lower 10%-tile)
Height: 3 ft. 1 inch
Pulse: 115 BPM
Respirations: 30 breaths per minute
Blood pressure: 95/60 mmHg
General Appearance
Happy, energetic child
Head and Neck
Runny nose but his ears are clear of fluid
No enlarged lymph nodes in neck
Lungs
Crackling sounds are present
Coughing and wheezing are audible
Cardiovascular
Normal
Abdominal
No swelling present
Genitourinary
Not assessed
Extremities
Full mobility is present
Pulse found in arms and legs
Neurological
Normal reflexes
Follow-up appointment scheduled for the next day.
Lab & Diagnostic Results
White blood cell count: values within normal limits
WBC differential: lymphocytes, monocytes, eosinophils, & basophils are within normal limits. There is a slight elevation of neutrophils.
Red blood cell count: values within normal limits
Hematocrit: values within normal limits
Platelet count: values within normal limits
Sweat chloride test: 40 mmol/L
Chest x-ray: some hyperinflation & bronchial wall thickening
Understanding Sweat Test Results
People with CF have more chloride in their sweat
Sweat chloride test will confirm the diagnosis
Enough sweat is needed to do the test
Full-term babies usually produce enough sweat by 2 weeks of age
To understand what the sweat test results mean, a chloride level of:
Less than or equal to 29 mmol/L = CF is unlikely regardless of age
Between 30 – 59 mmol/L = CF is possible and additional testing is needed
Greater than or equal to 60 mmol/L = CF is likely to be diagnosed
When sweat chloride test results fall between the range of 30-59 mmol/L, the sweat test is usually repeated.
Diagnosis
Cystic Fibrosis
Life-threatening genetic disease
Causes the body to create thick mucus
Mucus builds up & obstructs ducts U tubes in the lungs, digestive track & pancreas
May cause fatal infections & digestive issues
Affects the sweat glands & male reproductive system
Newborn Screening
Newborn screening (NBS) for cystic fibrosis is done in the first few days after birth. By diagnosing CF early, CF health care providers can help parents learn ways to keep their child as healthy as possible and delay or prevent serious, lifelong health problems related to CF.
Research shows that children who receive CF care early in life have better nutrition and are healthier than those who are diagnosed later. Early diagnosis and treatment can:
Improve growth
Help keep lungs healthy
Reduce hospital stays
Add years to life
Timing
Newborn screening is done during the first few days of a baby’s life — usually by a health care provider in the hospital. A few drops of blood from a heel prick are placed on a special card, called a Guthrie card.
This card with the baby’s information is mailed to a special state laboratory that will test the blood sample for certain health conditions, including CF. In some states, newborn screening involves two blood samples, one at birth and one a few weeks later.
Genetics of Cystic Fibrosis
Symptoms
Complications
Respiratory System
Recurrent attack of bronchitis & pneumonia
Damage to the airways → bronchiectasis
Nasal polyps
Coughing of blood (hemoptysis)
Pneumothorax
Respiratory failure
Digestive System
Malabsorption of nutrients
Diabetes mellitus (pancreatic damage)
Blockage of bile duct
Intestinal obstruction
Distal intestinal obstruction syndrome
Reproductive System
Infertility
Pregnancy may exacerbate the disease & cause complications
Other Systems
Increased risk of osteoporosis
Dehydration & electrolyte imbalances
Clubbing of fingers & toes
Treatment
At present there is no cure for CF. Treatment aims at alleviating the symptoms & reducing the incidence of complications. Careful follow-up & early & aggressive intervention is essential. It is advisable to obtain treatment at a centre that specializes in CF.
Aims of Treatment
Reducing incidence & successful treatment of respiratory infections
Providing sufficient nutrition
Removal of & loosening mucus plugs in lung & airways
Avoiding & treating intestinal obstruction
Chest Physical Therapy
Loosens thick mucus & aids in expectoration
Tapping the front & back of the chest with cupped hands
May be done up to 4 times a day
Patient can be sitting or lying on his abdomen
Breathing exercises – coughing or huffing
Aerobic exercise helps to loosen the mucus
increases loss of salt & minerals
Nutritional Therapy
Nutritional therapy can take care of the malnutrition & vitamin deficiency that is common to CF patients. It involves:
A well-balanced diet
Intake of oral pancreatic enzymes to help in digestion & absorption
Vitamin A, D, E, & K supplements
High-calorie nutrient-filled shakes
A high-salt diet or salt supplements (usually before exercise)
A feeding tube may be used at night to give more calories
Vitamin supplements – including fat soluble vitamins
New agents that improve chloride transport – IVACAFTOR
Disease Modifying Drug
Kalydeco G511D
(ivacaftor) a pill for people ages 6 and older who have the G551D mutation of CF which helps the defective CFTR protein work at the surface of the cell
Symptom Management
PULMOZYME (Dornase Alfa)
is an inhaled medication used to help thin the mucus
Hypertonic Saline
to draw more water into the airways and make it easier to cough out the mucus.
Ibuprofen
anti-inflammatory to slow the rate of lung function decline
CREON
pancreatic enzymes to help people with CF digest their food
COTAZYM
pancreatic enzymes to help people with CF digest their food
FLOVENT
inhaled steroid treatment Open benefit
ADVAIR
inhaled steroid treatment for asthma
Salbutamol (MDI or Nebules)
bronchodilator
Infection Control
CAYSTON
(aztreonam) inhaled antibiotic for the treatment of CF
Zithromax (Azithromycin)
is a commonly used antibiotic to treat pneumonia
COLY-MYCIN
antibiotic
TOBI Podhaler
(tobramycin) inhaled antibiotic with Podhaler device to help fight the germ Pseudomonas aeruginosa
TOBI Inhaled Tobramycin 300mg
(tobramycin) inhaled antibiotic to help fight the germ Pseudomonas aeruginosa
Ivacaftor increases the activity of the CFTR protein, while Lumacaftor improves protein folding of the CFTR protein.
Surgical Treatment
Removal of nasal polyps
Removal of mucus obstructing airways (endoscope)
Oxygen therapy
Alimentation through feeding tube
Relieving intestinal obstruction
Lung transplant
Caregiver Suggestions
CF symptoms may worsen over time
Managing CF takes a team approach
Staying organized makes treatment easier
Preventing infection is essential
Focusing on nutrition is a must
Exercise can keep everyone healthy
Emotional distress is real
Your loved one may need a lung transplant someday
It’s important to take steps to help your child transition to adulthood
You need to make time to take care of yourself, too
Ernst, M. M., Johnson, M. C., & Stark, L. J. (2010). Developmental and psychosocial issues in cystic fibrosis. Child Adolesc Psychiatr Clin N Am., 19(2), 263-283. https://doi.org/10.1016/j.chc.2010.01.004.
Grasemann, H. (2017). CFTR modulator therapy for cystic fibrosis. The New England Journal of Medicine, 377(21), 2085-2090. https://doi.org/10.1056/NEJMe1712335
Lang, R. L., Stockton, K., Wilson, C., Russell, T. G, & Johnston, L. M. (2020). Exercise testing for children with cystic fibrosis: A systematic review. Pediatric Pulmonology, 55(8), 1996-2010. https://doi.org/10.1002/ppul.24794
Peckham, D., McDermott, M. F., Savic, S., & Mehta, A. (2020). COVID-19 meets cystic fibrosis: For better or worse? Genes & Immunity, 21, 260-262. https://doi.org/10.1038/s41435-020-0103-y
Stolz, D. A., Meyerholz, D. K., & Welsh, M. J. (2015). Origins of cystic fibrosis lung disease. The New England Journal of Medicine, 372, 351-362. https://doi.org/10.1056/NEJMra1300109
Hugh was born in 1945 and grew up near Sunnybrook in Toronto. He went to private school and did well in his studies, with the goal of becoming a lawyer. He articled at a prestigious law firm in Toronto where he met Gladys, the daughter of one of the firm’s partners. He joined the law firm once he passed his bar exam and married Gladys shortly after.
Hugh worked long hours and within three years made junior partner. In 1971, he and Gladys’s son, Paul, was born. Hugh continued to work long hours and weekends, often missing out on Paul’s milestones.
Due to the demands of Hugh’s job and the couple’s social status, it was decided that Paul would be sent to boarding school once he started kindergarten.
Hugh and Gladys entertained often, socializing with the elite of Toronto. Rich foods and large amounts of alcohol were an everyday occurrence for this couple.
In 1990, Hugh was seen by his family physician for headaches, vision problems, fatigue, and occasional nose bleeds. Hugh was diagnosed with Stage 2 hypertension (blood pressure 150/90) and given instructions to change his lifestyle.
Hugh was put on a diuretic and angiotensin converting enzyme (ACE) inhibitor. He was able to manage his hypertension with these medications. However, he did not change his lifestyle as recommended by his physician.
Medications:
Furosemide (Lasix) – loop diuretic
Ramipril (Altace) – ACE inhibitor
In 2011, Hugh retired. Due to her cognitive and physical deterioration, Gladys required his attention. He needed to be home more to facilitate her care. Over time, Gladys had to move into a long-term care institute.
Hugh was now experiencing urinary issues that he had attributed to the normal aging process:
Frequent or urgent need to urinate
Increased frequency of urination at night (nocturia)
Difficulty starting urination
Weak urine stream or a stream that stops and starts
Dribbling at the end of urination
Inability to completely empty the bladder
Once again, Hugh decided to see his family physician. Physical examination and mildly elevated serum prostate-specific antigen (PSA) confirmed that Hugh had benign prostatic hyperplasia (BPH). BPH is a common condition as men age. An enlarged prostate gland can cause uncomfortable urinary symptoms, such as urine flow blockage out of the bladder. It can also cause bladder, urinary tract or kidney problems. His physician wanted Hugh to have a routine colonoscopy as Hugh’s fecal immunochemical test (FIT) was back positive.
FIT is a screening test for colon cancer. It tests for hidden blood in the stool, which can be an early sign of cancer. FIT only detects human blood from the lower intestines. Medications and food do not interfere with the test.
Given Hugh’s symptoms, he was scheduled for a transurethral resection of the prostate (TURP). A lighted scope is inserted into the urethra, and the surgeon removes all but the outer part of the prostate. TURP generally relieves symptoms quickly, and most men have a stronger urine flow soon after the procedure. After TURP a catheter may be temporarily needed to drain the bladder.
Hugh no longer had urinary issues, was sleeping better, had more energy, and was relieved that it was “nothing much”. Two months after his TURP, Hugh went in for his routine colonoscopy.
A colonoscopy lets a doctor look at the lining of the entire colon and rectum using an endoscope.
Abnormal results may show:
diverticulosis (abnormal pouches in the lining of the colon)
hemorrhoids
inflammatory bowel disease (ulcerative colitis or Crohn’s disease)
bleeding in the colon or rectum
polyps
cancer of the colon or rectum
Biopsies were taken during the colonoscopy for testing in the lab. The pathologist reported Stage I colon cancer. Hugh required a bowel resection which left him with a colostomy. With Gladys in long-term care, Hugh was living alone. Home care was instructed to teach him proper ostomy care.
Hugh’s self-image was suffering. He did not go out, and was not eating properly due to fear of leakage at the ostomy site. He led a very sedentary life. He also had concerns about the welfare of his son, Brian, who had Down syndrome and lived with Hugh at home: who would look after him once Hugh was gone? Hugh considered reaching out to his older son, Paul, but the two of them had not spoken in years. Ultimately, Hugh was unable to get Paul’s help in caring for Brian and himself.
Instead, Hugh spent time researching institutions where Brian could live. The only option Hugh could see for Brian’s wellbeing was sending him to a home for “people like him.”
Case Key Words
Alcohol
Cancer
Cardiovascular-circulation
Colon Cancer
Colostomy
High Blood Pressure
Hypertension
Prostate
Urinary System
Hugh's Health: Hypertension
Hugh was diagnosed with hypertension in 1990.
Components of Arterial Blood Pressure
The systolic pressure is the higher value and reflects the arterial pressure resulting from the ejection of blood during ventricular contraction, or systole.
The diastolic pressure is the lower value and represents the arterial pressure of blood during ventricular relaxation, or diastole.
Hypertension Medications
Systolic
Diastolic
Normal
90 – 129
60 – 79
Stage 1
130 – 139
80 – 89
Stage 2
140 – 179
90 – 109
Critical
Over 180
Over 110
Diuretics: get rid of excess sodium and water, often used with additional prescription therapies
Beta-blockers: reduce heart rate, workload, and output
ACE inhibitors: help to produce less angiotensin, blood vessels relax and open up
Angiotensin II receptor blockers: block the receptors so angiotensin fails to constrict blood vessels
Calcium channel blockers: prevents calcium from entering the smooth muscle cells of the heart & arteries and open up narrowed blood vessels
Alpha blockers: reduce artery resistance, relaxing the muscle tone of the vascular wall
Alpha-2 receptor agonists: decreasing the activity of the sympathetic portion of the involuntary NS
Combined alpha and beta-blockers: used IV for hypertensive crisis
Central agonists: decrease blood vessels’ ability to tense up or contract (different nerve pathway than α & β-blockers)
Peripheral adrenergic inhibitors: blocks neurotransmitters in the brain for smooth muscle contraction
Vasodilators: muscle in the blood vessel walls to relax → vessel dilation
Hugh’s Blood Pressure Medications
Furosemide (Lasix)-loop diuretic
Inhibits the NKCC2 cotransporter.
Inhibits the reabsorption of sodium.
The interstitium will lose its tonicity.
Affecting how much water is reabsorbed by the Loop of Henle and collecting ducts.
More water leaves via the filtrate rather than go back into the blood.
Ramipril (Altace)-ACE inhibitor
Reduce the activity of angiotensin-converting enzyme.
ACE is responsible for hormones that help control BP.
Narrowing effect on blood vessels that ↑BP.
ACE inhibitors limit this enzyme, making the blood vessels relax and widen.
Lowering BP and improving blood flow to the heart muscle.
Managing Hypertension
Exercising regularly
Eating a healthy diet
Decrease the salt in your diet
Maintain a healthy weight
Managing your stress
Limit alcohol
Don’t smoke
Hugh's Health: Benign Prostatic Hyperplasia
Hugh was diagnosed with benign prostatic hyperplasia (BPH) in 2011, and underwent a transurethral resection of the prostate.
Risk Factors
Aging
Family history
Diabetes or heart disease
Lifestyle
Diagnostics
Digital rectal exam. The doctor inserts a finger into the rectum to check your prostate for enlargement.
Urine test. Analyzing a sample of your urine can help rule out an infection or other conditions that can cause similar symptoms.
Blood test. The results can indicate kidney problems.
Prostate-specific antigen (PSA) blood test. PSA is a substance produced in your prostate. PSA levels increase when you have an enlarged prostate. However, elevated PSA levels can also be due to recent procedures, infection, surgery or prostate cancer.
Urinary flow test. You urinate into a receptacle attached to a machine that measures the strength and amount of your urine flow. Test results help determine over time if your condition is getting better or worse.
Post void residual volume test. This test measures whether you can empty your bladder completely. The test can be done using ultrasound or by inserting a catheter into your bladder after you urinate to measure how much urine is left in your bladder.
24-hour voiding diary. Recording the frequency and amount of urine might be especially helpful if more than one-third of your daily urinary output occurs at night.
Complications
Sudden inability to urinate
Urinary tract infection (UTI)
Bladder calculi
Bladder damage
Kidney damage
Medications
Alpha blockers. These medications relax bladder neck muscles and muscle fibers in the prostate, making urination easier. Alpha blockers — which include alfuzosin (Uroxatral), doxazosin (Cardura), tamsulosin (Flomax) and silodosin (Rapaflo) — usually work quickly in men with relatively small prostates. Side effects might include dizziness and a harmless condition in which semen goes back into the bladder instead of out the tip of the penis (retrograde ejaculation).
5-alpha reductase inhibitors. These medications shrink your prostate by preventing hormonal changes that cause prostate growth. These medications — which include finasteride (Proscar) and dutasteride (Avodart) — might take up to six months to be effective. Side effects include retrograde ejaculation.
Combination drug therapy. Your doctor might recommend taking an alpha blocker and a 5-alpha reductase inhibitor at the same time if either medication alone isn’t effective.
Tadalafil (Cialis). Studies suggest this medication, which is often used to treat erectile dysfunction, can also treat prostate enlargement.
Surgical Intervention
Under what circumstances is surgery a viable treatment for BPH?
Your symptoms are moderate to severe
Medication hasn’t relieved your symptoms
You have a urinary tract obstruction, bladder stones, blood in your urine or kidney problems
You prefer definitive treatment
Transurethral Resection of the Prostate (TURP)
Hugh's Health: Colon Cancer
In 2011, after a routine colonoscopy, Hugh was diagnosed with Stage I colon cancer. To treat it, he underwent a colostomy.
Stages of Colon Cancer
Stage 0 (Carcinoma in Situ)
Abnormal cells found in the mucosa of the colon wall.
These cells may become cancer and spread into nearby normal tissue.
Stage I Colon Cancer
Cancer has formed in the mucosa of the colon wall.
Has spread to the submucosa or to the muscle layer of the colon wall.
Stage II Colon Cancer
Is divided into stages IIA, IIB, and IIC:
Stage IIA
Cancer has spread through the muscle layer of the colon to the serosa of the colon wall.
Stage IIB
Cancer has spread through the serosa of the colon wall to the tissue that lines the organs in the abdomen.
Stage IIC
Cancer has spread through the serosa of the colon wall to nearby organs
Stage III Colon Cancer
Is divided into stages IIIA, IIIB, and IIIC:
Stage IIIA
Spread through the mucosa to the submucosa or the muscle layer and spread into 1 to 3 nearby lymph nodes or cancer cells have formed in tissue near the lymph nodes.
Or through the mucosa to the submucosa and spread to 4 to 6 nearby lymph nodes.
Stage IIIB
Spread through the muscle layer to the serosa or has spread through the serosa to the tissue that lines the organs in the abdomen.
Spread to 1 to 3 nearby lymph nodes or cancer cells have formed in tissue near the lymph nodes.
Spread to the muscle layer or to the serosa and to 4 to 6 nearby lymph nodes.
Through the mucosa to the submucosa or to the muscle layer and spread to 7 or more nearby lymph nodes.
Stage IIIC
Spread through the serosa to the tissue that lines the abdominal organs and spread to 4 to 6 nearby lymph nodes.
Through the muscle layer to the serosa or spread through the serosa to the tissue that lines the abdominal organs and spread to 7 or more nearby lymph nodes.
Spread through the serosa to nearby organs and spread to 1 or more nearby lymph nodes or cancer cells have formed in tissue near the lymph nodes.
Stage IV colon cancer
Is divided into stages IVA, IVB, and IVC:
Stage IVA
Spread to one area or organ that is not near the colon or a distant lymph node.
Stage IVB
Spread to more than one area or organ that is not near the colon or a distant lymph node.
Stage IVC
Spread to the tissue that lines the wall of the abdomen and may have spread to other areas or organs.
Risk Factors for Colorectal Cancer
Family history of colon or rectal cancer in a first-degree relative
A personal history of cancer of the colon, rectum, or ovary
Personal history of high-risk adenomas (colorectal polyps that are 1 cm or larger, or have abnormal cells)
Inherited changes in certain genes that increase the risk (familial adenomatous polyposis or Lynch syndrome)
Personal history of chronic ulcerative colitis or Crohn disease for 8 or more years
3 or more alcoholic drinks per day
Smoking cigarettes
Being black
Being obese
Older age
Symptoms
Change in bowel habits
Blood (either bright red or very dark) in the stool
Diarrhea, constipation, or feeling that the bowel does not empty
Stools that are narrower than usual
Frequent gas pains, bloating, fullness, or cramps
Weight loss for no known reason
Feeling very tired
Vomiting
Diagnostic Tests
Physical exam and health history
Digital rectal exam
Fecal occult blood test (FOBT)
Guaiac FOBT
Immunochemical FOBT
Barium enema
Sigmoidoscopy
Surgical Treatment
Resection of the colon with colostomy
Unable to sew the 2 ends of the colon together
A stoma (an opening) is made outside the body
Waste passes through this opening a bag is placed around the stoma to collect the waste
It can be reversed
Life Post-Colostomy
Monitor your medications. Some meds can cause constipation or diarrhea.
Eat a well-balanced diet. Avoid foods that cause a lot of gas.
Live your life.
Concerns:
Body image/self-esteem
Relationships
Self-care
Phases of Psychological Adaptation
Almost every patient goes through 4 phases of recovery following an accident or illness that results in loss of function of an important part of the body.
The patient and family go through these phases, varying only in the time required for each phase.
Some people may skip certain phases entirely and some may move up and down at different times.
Shock or panic: tearful, anxious and forgetful.
Defense/retreat/denial: denies or minimizes the significance of the event, defends themselves against the implications of the event.
Acknowledgement: begins to face the reality of the situation. Gives up the old life, and may enter a period of depression, of apathy, of agitation, of bitterness, and of high anxiety.
Adaptation/resolution: acute grief begins to subside. Coping in a constructive manner and begins to establish new structures. Develops a new sense of worth.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). Blood Flow, Blood Pressure, and Resistance. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013) . Epithelial Tissue. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., . . . DeSaix, P. (2013). The Small and Large Intestine. Anatomy and Physiology. OpenStax.
Bakris, G., & Sorrentino , M. (2018). Redefining hypertension – Assessing the new blood-pressure guidelines. The New England Journal of Medicine, 378(6), 497-501. https://doi.org/10.1056/NEJMp1716193
Raebel, M. A. (2011). Hyperkalemia associated with use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers. Cardiovascular Therapeutics, 30(3), e156-e166. https://doi.org/10.1111/j.1755-5922.2010.00258.x
Schilsky, R. L. (2018). A new IDEA in adjuvant chemotherapy for colon cancer. The New England Journal of Medicine, 378(13), 1242-1246. https://doi.org/10.1056/NEJMe1800419
Gladys was born in 1949 and grew up in the Bridle Path neighbourhood of Toronto. She was an only child whose parents provided her with everything she could ask for. She went to private schools, vacationed in foreign destinations, and never really had any worries.
Gladys met her future husband at a party in 1965 when she was home from school. Hugh was a friend of a friend, and part of Gladys’s socio-economic class. They got to know one another over the summer, and promised to stay in touch while Gladys was away finishing school. Despite her parents’ disapproval over her relationship with Hugh, she married him.
Gladys started smoking when she was 16 years old and continued to smoke over one pack per day until recently. She also continued her tradition of afternoon cocktails throughout her adult life. Gladys did not work outside of the home, hired a cleaning lady to come in once per week, and had a full-time cook. After their son Paul was born, Gladys and Hugh hired a nanny, who stayed with them until Paul started school.
Life was going well until 1989, when Gladys found out that she was pregnant again. Gladys continued to smoke and have afternoon cocktails during both pregnancies. Brian was born in late 1989 and diagnosed with Down syndrome. Shortly after his birth, Brian required a number of surgeries and he remained in hospital for approximately the first year of his life.
Gladys and Hugh visited Brian infrequently during his hospitalization. Brian was discharged home, where he had private care around the clock. Gladys went to see her son once each day, but did not interact with him.
Gladys was diagnosed with stage 2 COPD in 1999 and told to quit smoking. She tried many times without any success. In 2015, her illness worsened and she was prescribed oxygen therapy for stage 3 COPD.
Medications:
Formoterol and budesonide (Sybicort) – bronchodilator and inhaled steroid
As early as 2010, Hugh started noticing changes in Gladys. She was becoming increasingly forgetful and would often behave in ways that were not normal for her:
Memory loss
Poor judgment leading to bad decisions
Loss of spontaneity and sense of initiative
Taking longer to complete normal daily tasks
Repeating questions
Trouble handling money and paying bills
Wandering and getting lost
Losing things or misplacing them in odd places
Mood and personality changes
Increased anxiety and/or aggression
Hugh took her to see her family physician who diagnosed Gladys with Alzheimer’s disease.
Diagnosis of Alzheimer’s disease:
Physical and neurological examination
Reflexes, muscle tone and strength, coordination, balance, ability to sit, stand up, and move around the room, sense of sight, and hearing are all examined to study overall neurological health.
Laboratory test
Blood samples are collected to help detect if there are any alternative explanations for memory loss or confusion, such as vitamin deficiency or a thyroid disorder.
Brain imaging
Magnetic resonance imaging (MRI): Radio waves and a strong magnetic field are used to produce detailed images of the brain. MRI scans may also show brain shrinkage.
Computerized tomography (CT): It is a specialized X-ray technology that produces cross-section images of the brain.
Positron emission tomography (PET): A low-level radioactive tracer that is injected into the blood to reveal particular features of the brain.
Treatment of Alzheimer’s disease:
Cholinesterase inhibitor: boosts the level of cell-to-cell coordination which usually gets depleted in the brain. This drug helps to preserve a chemical messenger. Although improvement is modest, agitation and depression levels are moderated well.
Memantine (Namenda): slows the progression of symptoms and is at times combined with a cholinesterase inhibitor. This drug functions in another brain cell communication network, and in rare cases may cause side effects such as dizziness and signs of confusion.
Anti-depressants: to help control behavioural changes
Over the next few years, Gladys continued to deteriorate:
Increased memory loss and confusion
Inability to learn new things
Difficulty with language and problems with reading, writing, and working with numbers
Difficulty organizing thoughts and thinking logically
Shortened attention span
Problems coping with new situations
Difficulty carrying out multi step tasks, such as getting dressed
Problems recognizing family and friends
Hallucinations, delusions, and paranoia
Impulsive behavior, such as undressing at inappropriate times or places or using vulgar language
Inappropriate outbursts of anger
Restlessness, agitation, anxiety, tearfulness, and wandering – especially in the late afternoon or evening
Repetitive statements or movement, occasional muscle twitches
Hugh discussed Gladys’s care with her family physician as he wanted to keep Gladys at home. It was decided that the familiar surroundings of home would be beneficial to Gladys, however additional supervision and care would be necessary.
By 2018, Gladys’ symptoms had become even more severe:
Inability to communicate
Weight loss
Seizures
Skin infections
Difficulty swallowing
Groaning, moaning, or grunting
Increased sleeping
Loss of bowel and bladder control
A care conference was called with her primary care team, Hugh and Paul. It was decided that it was best for Gladys to be placed in a long-term care facility. Approximately nine months after admission, Gladys was diagnosed with aspiration pneumonia. The facility’s physician presented Hugh with the options of antibiotics to treat the pneumonia, and a feeding tube to provide Gladys with nutritional input while lowering the risk of aspiration.
Hugh weighed the benefits and risks of these treatment options. Based on what Hugh knew of Gladys’s values, however, he decided to withdraw all treatment and signed a DNR. Two weeks later, Gladys passed away in her sleep.
Gladys, a daily smoker since she was 16, was diagnosed with chronic obstructive pulmonary disease (COPD) in 1999. Her symptoms worsened over time, and she eventually began oxygen therapy in 2015.
Diagnosis
COPD is diagnosed through pulmonary (or lung) function tests. The most common of these tests is spirometry, which measures the amount of air you can inhale and exhale, and whether your lungs deliver enough oxygen to your blood.
During the test, you blow into a large tube connected to a small machine to measure how much air your lungs can hold and how fast you can blow the air out of your lungs.
Other pulmonary function tests include:
Pulse oximetry
Blood gases
End tidal CO₂
Peak expiratory flow rate
Bronchial challenge testing
Exercise tests
Respiratory muscle pressure measurement
Lung volumes by helium dilution
Diffusing capacity
Gladys’s Pulmonary Function Test Results
FEV₁ – the forced expiratory volume in 1 second
FVC – the forced vital capacity
Your FEV₁ is influenced by other factors including age, sex, height, and ethnicity. The FEV₁/FVC ratio is used to define obstructive defect and used to diagnose the disease progression.
Pulmonary Function Test
Instrument
Measures
Function
Spirometry
Spirometer
Forced vital capacity (FVC)
Volume of air that is exhaled after maximum inhalation
Forced expiratory volume (FEV)
Volume of air exhaled during one forced breath
Forced expiratory flow, 25-75 percent
Air flow in the middle of exhalation
Peak expiratory flow (PEF)
Rate of exhalation
Maximum voluntary ventilation (MVV)
Volume of air that can be inspired and expired in 1 minute
Slow vital capacity (SVC)
Volume of air that can be slowly exhaled after inhaling past the tidal volume
Total lung capacity (TLC)
Volume of air in the lungs after maximum inhalation
Functional residual capacity (FRC)
Volume of air left in the lungs after normal expiration
Residual volume (RV)
Volume of air in the lungs after maximum exhalation
Total lung capacity (TLC)
Maximum volume of air that the lungs can hold
Expiratory reserve volume (ERV)
Volume of air that can be exhaled beyond normal exhalation
Gas diffusion
Blood gas analyzer
Arterial blood gases
Concentration of oxygen and carbon dioxide in the blood
GOLD System of Grading COPD
GOLD stands for the Global Initiative for Chronic Obstructive Lung Disease. The National Heart, Lung, and Blood Institute, National Institutes of Health, and the World Health Organization started it in 1997.
The GOLD system bases the stage of COPD on several things:
Symptoms
How many times your COPD has gotten worse
Hospitalizations for COPD exacerbation
Spirometry results
COPD Stages
COPD Risk Factors Among Women
3.17 million deaths (5% of all global deaths) were caused by COPD in 2015
WHO reports a prevalence of 251 million cases of COPD in 2016
More women are being diagnosed with COPD
Higher mortality rates than men
Most common risk factors:
Smoking
Exposure to secondhand smoke
Air pollution
Occupational dust and fumes
Influence of sex on COPD involves several factors:
Differential susceptibility to the effects of tobacco
Anatomic, hormonal, and behavioural differences
Differential response to therapy
COPD and Food
The process of changing food to fuel in the body is called metabolism.
Oxygen and food are the raw materials of the process.
Energy and carbon dioxide are the finished products.
Carbon dioxide is a waste product that is exhaled.
Metabolism of carbohydrates produces the most carbon dioxide for the amount of oxygen used.
Metabolism of fat produces the least.
For some COPD patients, eating a diet with fewer carbohydrates and more fat helps them breathe easier.
Nutritional Guidelines
Choose complex carbohydrates.
Limit simple carbohydrates.
Eat 20 to 30 grams of fiber each day.
Eat a good source of protein.
Choose mono- and polyunsaturated fats.
Limit foods that contain trans fats and saturated fats.
Drink plenty of water – keeps you hydrated and keeps the mucus thin
Vitamins and minerals:
Steroids may increase your need for calcium
Calcium carbonate or calcium citrate with vitamin D
Sodium may cause edema and may increase blood pressure
Diet Tips
Rest before eating.
Eat more food early in the day if you are usually too tired to eat later on.
Avoid foods that cause gas or bloating. Tends to make breathing more difficult.
Eat 4 to 6 small meals a day. Enables the diaphragm to move freely and lets the lungs fill and empty more easily.
Drinking fluids with meals may make you feel too full. Drink an hour before or after meals.
Consider adding nutritional supplements at night to avoid feeling full during the day.
COPD and Exercise
Moderate exercise can improve:
The body’s use of oxygen
Energy levels
Anxiety, stress, and depression
Sleep
Self-esteem
Cardiovascular fitness
Muscle strength
SOB
Exercises help blood circulate, help your heart send oxygen to your body, and strengthen your respiratory muscles.
Types of Exercises for COPD
Pulmonary Rehabilitation consists of education and exercise classes that teach about lungs, the disease, and how to exercise and be more active with less SOB.
Examples include:
Stretching
Aerobic
Resistance
COPD and Emotional Health
Most COPD patients experience feelings of sadness, fear, and worry.
If those feelings start to affect ability to keep up with normal activities and life enjoyment, they may be symptoms of anxiety and depression.
Managing anxiety and depression can increase ability to stick with treatment, improve physical health, and reduce medical costs.
Things to do:
Talk to your healthcare team about your feelings
Take care of yourself
Connect with others who understand
Medications for COPD
Bronchodilators
Relax the muscles around the airways (short- and long-acting)
Beta₂-Agonists relax tightened muscles around airways, opening the airways, making breathing easier
Anticholinergics prevent the muscles around the airways from tightening, helps clear mucus from lungs
Anti-inflammatories
Known as corticosteroids or steroids
Inhaler device or oral pill
Reduces swelling and mucus production
Long-term use of steroids have serious side effects
Combination Medications
A corticosteroid, an anticholinergic, and a beta₂-agonist
Long-acting beta₂-agonist and long-acting anticholinergic
Long-acting beta₂-agonist, long-acting anticholinergic, and corticosteroid
Vaccinations
Influenza
Pneumonia
Gladys' Health: Alzheimer's
1999 – Diagnosed with COPD
2010 – Cognitive changes – diagnosed with Alzheimer’s disease
2015 – Oxygen therapy for COPD
2018 – Health and wellbeing deteriorated – placed in LTC facility
2019 – Dies due to complications of Alzheimer’s disease
Causes of Alzheimer’s Disease
People with AD gradually suffer memory loss and a decline in thinking abilities, as well as major personality changes. These losses in cognitive function are accompanied by changes in the brain, including the build-up of amyloid plaques and tau-containing neurofibrillary tangles, which result in the death of brain cells and the breakdown of the connections between them.
Amyloid plaques and neurofibrillary tangles are the primary hallmarks of Alzheimer’s disease. Plaques are dense deposits of protein and cellular material outside and around the brain’s nerve cells. Tangles are twisted fibers that build up inside the nerve cells. Scientists have known about plaques and tangles since 1906, when a German physician, Dr. Alois Alzheimer, first identified them in the brain of woman who had died after suffering paranoid delusions and psychosis.
Personality and Behaviour Changes
Common Changes in Personality & Behaviour
Getting upset, worried, and angry more easily
Acting depressed or not interested in things
Hiding things or believing other people are hiding things
Imagining things that aren’t there
Wandering away from home
Pacing a lot
Showing unusual sexual behaviour
Hitting others
Misunderstanding what they see or hear
Stops caring about how they look
Managing Personality Changes
Keep things simple; Ask or say one thing at a time
Have a daily routine
Reassurance that they are safe and you are there to help
Focus on their feelings rather than their words
Don’t argue or try to reason with them
Try not to show frustration or anger
Use humor when appropriate
Allow a safe environment for pacing
Try using music, singing, or dancing for distraction
Ask them to help (“let’s set the table” or “I need help folding the clothes”)
Changes in Communication Skills
Persons with Alzheimer’s may have problems with:
Finding the right word or losing their train of thought when speaking
Understanding what words mean
Paying attention during long conversations
Remembering the steps in common activities
Blocking out background noises
Frustration if communication is not working
Being very sensitive to the tone and loudness of voices
Making Communication Easier
Understand that Alzheimer’s causes changes in communication skills.
Try some tips that may make communication easier:
Make eye contact and use their name
Beware of your tone, loudness of voice, and body language
Encourage two-way conversation for as long as possible
Use other methods besides speaking, such as gentle touch
Try distraction if communication creates problems
Be patient
Offer simple step-by-step instructions
Try not to interrupt
Don’t talk to the person using “baby talk” or a “baby voice”
Medications
Drug Name
Drug Type & Use
How It Works
Common Side Effects
Manufacturer’s Recommended Dosage
Aricept® (donepezil)
Cholinesterase inhibitor prescribed to treat symptoms of mild, moderate, and severe Alzheimer’s
Prevents the breakdown of acetylcholine in the brain
Nausea, vomiting, diarrhea, muscle cramps, fatigue, weight loss
Tablet*: Initial dose of 5 mg once a day; may increase dose to 10 mg/day after 4-6 weeks if well tolerated, then to 23 mg/day after at least 3 months
Orally disintegrating tablet*: Same dosage as above (not available in 23 mg)
Exelon® (rivastigmine)
Cholinesterase inhibitor prescribed to treat symptoms of mild to moderate Alzheimer’s (patch is also for severe Alzheimer’s)
Prevents the breakdown of acetylcholine and butyrylcholine (a brain chemical similar to acetylcholine) in the brain
Capsule*: Initial dose of 3 mg/day (1.5 mg twice a day); may increase dose to 6 mg/day (3 mg twice a day), 9 mg/day (4.5 mg twice a day), and 12 mg/day (6 mg twice a day) at minimum 2-week intervals if well tolerated
Patch*: Initial dose of 4.6 mg once a day; may increase dose to 9.5 mg once a day and 13.3 mg once a day at minimum 4-week intervals if well tolerated
Namenda® (memantine)
N-methyl D-aspartate (NMDA) antagonist prescribed to treat symptoms of moderate to severe Alzheimer’s
Blocks the toxic effects associated with excess glutamate and regulates glutamate activation
Tablet*: Initial dose of 5 mg once a day; may increase dose to 10 mg/day (5 mg twice a day), 15 mg/day (5 mg and 10 mg as separate doses), and 20 mg/day (10 mg twice a day) at minimum 1-week intervals if well tolerated
Oral solution*: Same dosage as above
Extended-release capsule*: Initial dose of 7 mg once a day; may increase dose to 14 mg/day, 21 mg/day, and 28 mg/day at minimum 1-week intervals if well tolerated
Namzaric® (memantine and donepezil)
NMDA antagonist and cholinesterase inhibitor prescribed to treat symptoms of moderate to severe Alzheimer’s
Blocks the toxic effects associated with excess glutamate and prevents the breakdown of acetylcholine in the brain
Extended-release capsule*: Initial dose of 28 mg memantine/10 mg donepezil once a day if stabilized on memantine and donepezil
If stabilized on donepezil only, initial dose of 7 mg memantine/10 mg donepezil once a day; may increase dose to 28 mg memantine/10 mg donepezil in 7 mg increments at minimum 1-week intervals if well tolerated
Only 14 mg memantine/10 mg donepezil and 28 mg memantine/10 mg donepezil available as generic
Razadyne® (galantamine)
Cholinesterase inhibitor prescribed to treat symptoms of mild to moderate Alzheimer’s
Prevents the breakdown of acetylcholine and stimulates nicotinic receptors to release more acetylcholine in the brain
Tablet*: Initial dose of 8 mg/day (4 mg twice a day); may increase dose to 16 mg/day (8 mg twice a day) and 24 mg/day (12 mg twice a day) at minimum 4-week intervals if well tolerated
Extended-release capsule*: Same dosage as above but taken once a day
DNR and DNH Orders
Ontario nursing home DNR & DNH orders reduce inappropriate hospitalizations, but not entirely
3 in 5 nursing home residents had a DNR recorded on admission (Do Not Resuscitate)
1 in 7 had a DNH (Do Not Hospitalize)
Residents with a DNR or DNH were less likely to experience hospitalization or in-hospital death
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). The Respiratory System. Anatomy and Physiology. OpenStax.
Thomashow, B., Crapo, J. D., Yawn, B., McIvor, A., Cerreta, S., Mannino, D., . . . Rennard, S. (2014). The COPD foundation pocket consultant guide. Chronic Obstructive Pulmonary Diseases Journal of the COPD Foundation, 1(1), 83-87.
Albert, R. K., Au, D. H., Blackford, A. L., Casaburiq, R., Cooper, A., Criner, G. J., . . . Bailey, W. (2016). A randomized trial of long-term oxygen for COPD with moderate desaturation. The New England Journal of Medicine, 375(17), 1617-1627. https://doi.org/10.1056/NEJMoa1604344
Aryal, S., Diaz-Guzman, E., & Mannino, D. M. (2014). Influence of sex on chronic obstructive pulmonary disease risk and treatment outcomes. International Journal of Chronic Obstructive Pulmonary Disease, 9(1), 1145-1154. https://doi.org/10.2147/COPD.S54476
Barnes, P. J., Burney, P. G., Silverman, E. K., Celli, B. R., Vestbo, J., Wedzicha, J. A., & Wouters, E. F. (2015). Chronic obstructive pulmonary disease. Nature Reviews Disease Primers, 1. https://doi.org/10.1038/nrdp.2015.76
Celli, B. R., & Wedzicha, J. A. (2019). Update on clinical aspects of chronic obstructive pulmonary disease. The New England Journal of Medicine, 381, 1257-1266. https://doi.org/10.1056/NEJMra1900500
Pinto, L. M., Gupta, N., Tan, W., Li, P. Z., Benedetti, A., Jones, P. W., & Bourbeau, J. (2014). Derivation of normative data for the COPD assessment test (CAT). Respiratory Research, 15(68), 1-8. https://doi.org/10.1186/1465-9921-15-68
Querfurth, H. W., & LaFerla, F. M. (2011). Mechanisms of Disease: Alzheimer’s disease. The New England Journal of Medicine, 362, 329-344. https://doi.org/10.1056/NEJMra0909142
Thomashow, B., Crapo, J. D., Yawn, B., McIvor, A., Cerreta, S., Mannino, D., . . . Rennard, S. (2014). The COPD foundation pocket consultant guide. Chronic Obstructive Pulmonary Diseases Journal of the COPD Foundation, 1(1), 83-87. https://doi.org/10.15326/jcopdf.1.1.2014.0124
Paul was born to Gladys and Hugh in 1971 and grew up in an affluent area of Toronto. He had a nanny for his early years. Then, when it came time for him to attend school, he was sent away to a local boarding school. He only came home during summer and Christmas vacations. Once he was in high school, Paul was sent away again.
Paul had a large allowance during his high school years which allowed him the freedom to buy whatever he wanted. He started buying alcohol during his senior year when he went out with his friends. He partied a lot and his grades suffered. He did manage to graduate high school, however, and was accepted to a university in Quebec.
The party life continued, but Paul found that alcohol was no longer enough to give him the “high” that he craved. He started smoking marijuana and hashish during his second year at university. He no longer came home for summer vacation and spent that time with friends. By third year, Paul was using cocaine and alcohol on a daily basis. He was also struggling with the birth of his younger brother. In 1993, he dropped out of university before the end of third year, as he was failing all of his courses.
Paul’s parents intervened and sent Paul to a rehabilitation facility. Paul completed the program and went home to his parents. He wandered aimlessly through life over the next number of years, drinking, taking drugs, and revisiting rehabilitation facilities. It was in one of these facilities that he met his first wife in 1999. At the beginning of their relationship, they felt that they truly understood each other and could support each other’s efforts as they both struggled with addictions.
In 2002, Paul and his first wife adopted twin girls: Ella and Olivia. Paul worked odd jobs, but struggled to pay the bills while funding his cocaine habit. Paul’s parents wanted nothing to do with him or his young family. His first wife left him in 2008, taking the girls with her. This seemed to be the wake-up call Paul needed to get his life in order. He joined Narcotics Anonymous in 2009.
Paul was clean and sober for just over a year when he met Nancy. They started dating in 2010. Paul provided Nancy with a full disclosure about his past substance misuse, his previous marriage, and his twin girls. He worked for a construction company and seemed to enjoy it, stating that the physicality of the job helped him to stay clean. Paul and Nancy married in 2012. Shortly after they married, they decided to start trying to conceive. Life was going well for them.
In 2018, Paul had an accident at work, falling from scaffolding 2 stories high. He was taken by ambulance to the local hospital and diagnosed with injury to the ligaments and muscles in his back, along with three torn discs. One of the tears was quite large and required Paul to have a follow-up CT scan in six weeks.
Due to Paul’s history of substance abuse, Flexeril (muscle relaxant) and Ketoprofen (NSAID) were prescribed. He was sent home to rest and recuperate. Paul was not receiving adequate pain management from his prescription medications, so he called his family physician requesting something stronger. After much discussion, Paul’s doctor prescribed Tylenol 3 (acetaminophen 300 mg and codeine 30 mg). Paul was instructed to continue taking his prescribed medications and only take the Tylenol 3 if absolutely necessary. The physician also put the stipulation on the prescription that the pharmacy could only dispense four tablets each day. That meant that Nancy needed to stop by the pharmacy each night on her way home.
Upon arriving home at 7:30 pm on the third day after Paul started the Tylenol 3, Nancy found Paul agitated, sweating, and complaining that his back hurt more. When asked, Paul stated that he had his last Tylenol 3 at 9:00 am. He stated that he had needed them through the night, which left him only one for the day.
Over the next couple of years, Paul struggled with chronic back pain. He started self-medicating with alcohol and any prescription drugs he could get from walk-in clinics, eventually turning to the streets to obtain stronger pain medications. Paul was on long-term disability through WSIB. He was to begin a return to work program in a couple of weeks.
When Nancy’s parents, Jack and Mary, came to stay with them while Mary recovered from her surgery, Paul discovered that Mary had been prescribed Oxycodone-Acetaminophen (2.5 mg-325 mg) for pain. Her physician had prescribed 60 tablets, as she would be out of town for a number of weeks. Paul started sneaking a few pills a day from Mary’s prescription.
It was about two weeks after her parents’ arrival that Nancy noticed that the number of oxycodone tablets was much less than what it should have been. She couldn’t believe that Paul was back to using drugs. Nancy confronted Paul with her suspicions. After arguing for hours, Paul finally confessed to taking the pills.
He stated that he felt overwhelmed with everything going on in his life at the moment:
Out of work
Chronic back pain
Insomnia
The addition of Sam
Sam’s diagnosis
Mary and Jack living there
Lack of contact and support from his parents
Nancy going to school and working so much
Despite his relapse, Paul denied having a ‘pill problem.’ Nancy called Paul’s old NA sponsor for suggestions on what to do. Paul was angry at the world, blaming everyone else around him for how his life turned out.
Case Key Words
Addiction
Adoption
Alcoholism
Back Injury
Central Nervous System
Divorce
Muscles
Muscular System
Opioid Addiction
Opioid Crisis
Skeletal System
Support Groups
Vertebrae
Paul's Health: Back Injuries
After falling off of a 2 stories in 2018, he was diagnosed with back ligament and muscle injury. He ended up with three torn discs, one being quite large. He had a follow-up CT scan 6 weeks later, where he was told he had prescribed muscle relaxant & NSAID, due to substance abuse history. He did not receive adequate pain management, and Tylenol #3 was prescribed to him only when it became absolutely necessary. He was dispensing stipulation of 4 tablets each day.
Back Pain
Paul’s pack pain continued, was severe and did not improve with rest. He went to see a doctor, where he found out that it could possibly spread down one or both legs, especially if the pain extends below the knee. This causes weakness, numbness or tingling in one or both legs. These symptoms are accompanied by unexplained weight loss, fever, causes new bowel or bladder problems.
Causes of the pain
Muscle or ligament strain
Bulging or ruptured discs (leaking)
Arthritis
Osteoporosis
Risk factors of back injury
Age
Lack of exercise
Excessive weight
Diseases
Improper lifting
Psychological conditions (depression & anxiety will increase risk)
Prevention
Exercise
Build muscle strength & flexibility
Maintain a healthy weight
Quit smoking
Stand- sit- and lift smart
Paul's Health: Drug Addiction
Due to the results of substance abuse, Paul was often agitated, sweating, complaining of back pain. He was self-medicating with alcohol and prescription drugs, first from walk in clinics and eventually from the streets. At this point, he had long term disability. He was taking his mother-in-law’s post-op medications and denied having a “pill problem”. He stated that he was feeling overwhelmed with everything going on in his life.
What is drug addiction?
Drug addiction is an initial decision to take drugs is voluntary. Repeated drug use overwhelms receptor cells and can lead to brain changes that challenge self-control & resist urges. The natural capacity to produce dopamine in the reward center is reduced. Addictive drugs provide a shortcut to the brain’s reward center. Addicts may require higher doses and quicker passage into the brain.
The Brain’s Reward System
Addictive drugs provide a shortcut to the brain’s reward system by flooding the nucleus accumbens with dopamine. The hippocampus lays down memories of this rapid sense of satisfaction, and the amygdala creates a conditioned response to certain stimuli. The reward system may be more vulnerable, responses to stress more intense, or the formation of addictive habits quicker in some people, especially those suffering from depression, anxiety, or schizophrenia, and those with disorders like antisocial and borderline personality.
Why?
Biology
Genes account for about half of a person’s risk for addiction
Gender, ethnicity, and presence of other mental disorders
Environment
Family & friends
Economic status & general quality of life
Peer pressure, physical & sexual abuse
Early exposure to drugs, stress, and parental guidance
Development
Genetic & environmental factors interact with critical developmental stages
The earlier drug use begins, the more likely to become addicted
Teens’ brains are still developing (decision-making, judgment, and self-control)
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Axial Muscles of the Head, Neck, and Back. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). The Central Nervous System. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). The Vertebral Column. Anatomy and Physiology. OpenStax.
Arias-Carrión, O., Stamelou, M., Murillo-Rodriguez, E., Menéndez-González, M., & Pöppel, E. (2010). Dopaminergic reward system: A short integrative review. International Archives of Medicine, 3(24). https://doi.org/10.1186/1755-7682-3-24
Belzak, L., & Halverson, J. (2018). Evidence synthesis- The opioid crisis in Canada: A national perspective. Health Promotion and Chronic Disease Prevention in Canada, 38(6). https://doi.org/10.24095/hpcdp.38.6.02
Dassieu, L., Heino, A., Develay, E., Kaboré, J. L., Pagé, M. G., Moor, G., . . . Choinière, M. (2020). “They think you’re trying to get the drug”: Qualitative investigation of chronic pain patients’ health care experiences during the opioid overdose epidemic in Canada. Canadian Journal of Pain, 5(1), 66-80. https://doi.org/10.1080/24740527.2021.1881886
Brian was born in 1989 to affluent parents, Hugh and Gladys, who were in their early forties. Brian also had an older brother, Paul, who was away at boarding school when he was born.
When Gladys found out she was pregnant in her forties, her doctor suggested that Gladys be tested for Down syndrome. Gladys refused to have an amniocentesis done. Brian was diagnosed with Trisomy 21, one of the three types of Down syndrome. The diagnosis was suspected based on Brian’s physical appearance at birth, and confirmed by analysis of his chromosomes.
Gladys and Hugh were devastated by the news that their child was “less than perfect”. At first, they believed that a child with Down syndrome would require too much time and care for their lifestyle. And what would their friends and business associates think? They could not possibly bring this child home. Their view evolved and changed after reading about Down syndrome, learning the benefits of therapies like early intervention, and long discussions with peer groups (e.g. other parents of children with Down syndrome).
Brian had difficulty breathing and the physician noticed Brian had blue-tinged skin, and a heart murmur (an abnormal whooshing sound caused by turbulent blood flow). Several tests were ordered:
Echocardiogram
Electrocardiogram
Chest x-ray
Oxygen level measurement
Cardiac catheterization
Brian was diagnosed with Tetralogy of Fallot, a rare condition caused by a combination of four defects that are present at birth (congenital). These defects cause oxygen-poor blood to flow out of the heart and to the rest of the body.
Tetralogy of Fallot occurs during fetal growth, when the baby’s heart is developing. While factors such as poor maternal nutrition, viral illness, or genetic disorders might increase the risk of this condition, in most cases the cause of Tetralogy of Fallot is unknown.
The lungs of children with Down syndrome do not develop as fully as they do in the general population. Consequently, the growth of blood vessels throughout the lungs is limited. The narrowed arteries of the lungs hold potential for lasting consequences due to the increased pressure and flow of blood through the lungs.
Treatment
Surgery is the only effective treatment for Tetralogy of Fallot. Brian was two weeks old when he required temporary surgery due to his underdeveloped pulmonary arteries (hypoplastic). A bypass (shunt) was created between a large artery that branches off from the aorta and the pulmonary artery.
After six months, the cardiologist deemed Brian strong enough to undergo ‘intracardiac repair’. This is an open-heart surgery that involves several repairs:
Removal of the shunt
Patch over the ventricular septal defect to close the hole between the ventricles
Repair or replace the narrowed pulmonary valve and widens the pulmonary arteries to increase blood flow to the lungs
The surgery was a success and Brian was eventually discharged home. He had around-the-clock care which included:
Nursing
Physiotherapist
Occupational therapist
Play workers
Respiratory therapist
Tutor
Brian required regular medical follow-up to maintain good health:
Routine follow-up care – regular check-ups with a cardiologist, routine exams with his primary physician, prescription medications, routine dental care
Emotional health – may feel isolation, sadness, and frustration
Growing up, Brian’s only interactions were with the “hired help”. As a pre-teen and teen, he formed strong bonds with his workers and struggled with changes in staff and routine. This led to frustration and anger.
Case Key Words
Cardiovascular-circulation
Cardiovascular-heart
Down Syndrome
Fetal Development
Genetic Disorder
Heart Surgery
Intellectual Disability
Physical and Developmental Problems
Brian's Health: Down Syndrome
Down Syndrome Overview
There are 23 pairs of chromosomes, for a total of 46.
Half the chromosomes come from the egg, and the other half from the sperm.
This XY chromosome pair includes the X chromosome from the egg and the Y chromosome from the sperm.
In Down’s syndrome, there is an additional copy of chromosome 21, resulting in three copies instead of the normal two copies.
Trisomy 21 (also known by the karyotype 47,XX,+21 for females, 47,XY,+21 for males) is caused by a failure of the 21st chromosome to separate during egg and sperm development (nondisjunction).
Three Genetic Variations
Trisomy 21
About 95 percent of the time, Down syndrome is caused by trisomy 21 — the person has three copies of chromosome 21, instead of the usual two copies, in all cells. This is caused by abnormal cell division during the development of the sperm cell or the egg cell.
Mosaic Down syndrome
In this rare form of Down syndrome, a person has only some cells with an extra copy of chromosome 21. This mosaic of normal and abnormal cells is caused by abnormal cell division after fertilization.
Translocation Down syndrome
Down syndrome can also occur when a portion of chromosome 21 becomes attached (translocated) onto another chromosome, before or at conception. These children have the usual two copies of chromosome 21, but they also have additional genetic material from chromosome 21 attached to another chromosome.
Risk Factor
Advancing maternal age. A woman’s chances of giving birth to a child with Down syndrome increase with age because older eggs have a greater risk of improper chromosome division. A woman’s risk of conceiving a child with Down syndrome increases after 35 years of age. However, most children with Down syndrome are born to women under age 35 because younger women have far more babies.
Being carriers of the genetic translocation for Down syndrome. Both men and women can pass the genetic translocation for Down syndrome on to their children.
Having had one child with Down syndrome. Parents who have one child with Down syndrome and parents who have a translocation themselves are at an increased risk of having another child with Down syndrome. A genetic counselor can help parents assess the risk of having a second child with Down syndrome.
Screening During Pregnancy
First trimester combined two step test:
Blood test-measures levels of pregnancy-associated plasma protein-A (PAPP-A) and human chorionic gonadotropin (HCG). Abnormal levels of both may indicate a problem with the baby.
Nuchal translucency test-an ultrasound is used to measure a specific area on the back of the fetus’s neck. When abnormalities are present, more fluid tends to collect in this neck tissue.
Second trimester:
Blood test-measures four pregnancy-associated substances: alpha fetoprotein, estriol, HCG, and inhibin A.
If screening test results are positive or you are at high risk, more testing to confirm the diagnosis may be done.
Chorionic villus sampling (CVS)-cells are taken from the placenta and analyzed. Usually done in the 1st trimester. The risk of miscarriage is very low.
Amniocentesis-sample of amniotic fluid is withdrawn using a needle inserted into the uterus to analyze the fetus chromosomes. Done in 2nd trimester, risk of miscarriage is very low.
Brian's Health: Tetralogy of Fallot
Electrical Conduction System of the Heart
Sinoatrial node
Atrioventricular node
Bundle of His
Left bundle branch
Left posterior fascicle
Left anterior fascicle
Left ventricle
Ventricular septum
Right ventricle
Right bundle branch
Chambers & Circulation Through the Heart
Blood flows from the right atrium to the right ventricle, where it is pumped into the pulmonary circuit.
The blood in the pulmonary artery branches is low in oxygen but relatively high in carbon dioxide.
Gas exchange occurs in the pulmonary capillaries (oxygen into the blood, carbon dioxide out), and blood high in oxygen and low in carbon dioxide is returned to the left atrium.
From here, blood enters the left ventricle, which pumps it into the systemic circuit.
Following exchange in the systemic capillaries (oxygen and nutrients out of the capillaries and carbon dioxide and wastes in), blood returns to the right atrium and the cycle is repeated.
Facts About Tetralogy of Fallot
Birth defect that affects normal blood flow through the heart.
Happens when the heart does not form correctly as the baby grows & develops in the womb.
Made up of 4 defects of the heart and its blood vessels.
The 4 Abnormalities
Pulmonary valve stenosis
Pulmonary valve stenosis is a narrowing of the pulmonary valve — the valve that separates the lower right chamber of the heart (right ventricle) from the main blood vessel leading to the lungs (pulmonary artery).
Narrowing (constriction) of the pulmonary valve reduces blood flow to the lungs. The narrowing might also affect the muscle beneath the pulmonary valve. In some severe cases, the pulmonary valve doesn’t form properly (pulmonary atresia) and causes reduced blood flow to the lungs.
Ventricular septal defect
A ventricular septal defect is a hole (defect) in the wall (septum) that separates the two lower chambers of the heart — the left and right ventricles. The hole allows deoxygenated blood in the right ventricle — blood that has circulated through the body and is returning to the lungs to replenish its oxygen supply — to flow into the left ventricle and mix with oxygenated blood fresh from the lungs.
Blood from the left ventricle also flows back to the right ventricle in an inefficient manner. This ability for blood to flow through the ventricular septal defect reduces the supply of oxygenated blood to the body and eventually can weaken the heart.
Overriding aorta
Normally the aorta branches off the left ventricle. In tetralogy of Fallot, the aorta is shifted slightly to the right and lies directly above the ventricular septal defect.
In this position the aorta receives blood from both the right and left ventricles, mixing the oxygen-poor blood from the right ventricle with the oxygen-rich blood from the left ventricle.
Right ventricular hypertrophy
When the heart’s pumping action is overworked, it causes the muscular wall of the right ventricle to thicken. Over time this might cause the heart to stiffen, become weak and eventually fail.
Treatment
Surgery is the only effective treatment for tetralogy of Fallot.
Intracardiac repair:
Usually done within the 1st year after birth, involves several repairs
Patch over the ventricular septal defect to close the hole between the ventricles
Repairs or replaces the narrowed pulmonary valve and widens the pulmonary arteries
The right ventricle will go back to normal thickness (doesn’t need to work as hard)
Temporary surgery:
May be done if premature birth or pulmonary arteries are undeveloped (hypoplastic)
A shunt is inserted between a large artery that branches off the aorta and the pulmonary artery
Intracardiac surgery will be performed when baby is ready and shunt will be removed
After Surgery
Long-term complications are common:
Chronic pulmonary regurgitation (right ventricle)
Other heart valve problems
Continued leaks after the patch repair, may require a re-repair
Enlarged right ventricle or left ventricle
Arrhythmias
Coronary artery disease
Aortic root dilation (ascending aorta enlarges)
Sudden cardiac death
On-going Care
Lifelong care with a cardiologist trained in treating congenital heart disease
Routine follow-up appointments which include physical exam, blood tests, echocardiogram, ECG
Monitor physical activity if there is any pulmonary leakage or obstruction or arrhythmias
Antibiotics for dental procedures to prevent endocarditis
Coping and Support
Support groups-provide hope, encouragement and support
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Fetal Development. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Patterns of Inheritance. Anatomy and Physiology. OpenStax.
Bull, M. J. (2020). Down Syndrome. The New England Journal of Medicine, 382(24), 2344-2352.
Chitty, L. S. (2015). Use of cell-free DNA to screen for Down syndrome. The New England Journal of Medicine, 372(17), 1666-1667. https://doi.org/10.1056/NEJMe1502441
During his first marriage to an African-Canadian woman, Paul adopted identical twin Asian daughters: Ella and Olivia. The girls were 5 years old when their adopted parents divorced. Since that time, Paul has seen the girls sporadically. Ella is in her first year of university. She is on the bus heading home to spend Thanksgiving and reading week with her mom and sister. She is planning on a quick visit with her dad and his new family during the holidays.
Ella and Olivia used to have so much fun together, but things have changed recently. Ella is worried about Olivia and the serious health troubles she had been having for over a year and a half. Ella can’t help but wonder if these same troubles are heading her way.
The Diagnosis
Ella stared out the bus window as it traveled down the highway. She recalled last June when her mother shared the fateful news about Olivia: “Olivia has been diagnosed with schizophrenia,” was what her mother had said.
She had known that something was wrong with her sister. Over a year ago, Ella had started to notice changes in Olivia’s behaviour. Olivia had quit a job that she loved. She seemed withdrawn and unmotivated, and had also unexpectedly decided not to attend university despite Ella’s and their mother’s efforts to convince her otherwise. But Ella had left in the summer for university and had not seen the worst of Olivia’s behaviours. Olivia had begun having hallucinations, and could not seem to carry on a coherent conversation in the way that she used to.
Ella had done some research about schizophrenia after hearing of her sister’s diagnosis. She did not like what she found. Apparently, schizophrenia had a tendency to run in families. In fact, studies indicated that a sibling of a schizophrenic was 10 times more likely to develop schizophrenia than the general population. Ella began to worry about her own mental health. She decided she would do some further investigation into the disease once she was home for reading week.
Just how “identical” are we?
Ella had been home from university for a couple of days and was still preoccupied with Olivia’s diagnosis and her own potential risk for mental illness. Ella expressed her anxiety and concerns to her mother one night after dinner. “Ella,” her mother said, “your concerns are perfectly valid and you have every reason to want to get more information. Why don’t we make an appointment to consult with a psychiatrist?” Ella made the appointment the next day.
Ella left Dr. Jacobson’s office feeling that some of the weight had been lifted from her shoulders. On the car ride home, she thought about the things that Dr. Jacobson had said to her during their consultation.
“It was good of you to come in to see me, Ella. You are absolutely right to have concerns for yourself when your identical twin has been diagnosed with schizophrenia. Research shows that schizophrenia is almost 50% heritable, and since you share nearly identical DNA with your sister, that puts you at a higher risk for developing this disease as well.”
“Fifty percent may sound like a scary number, but remember that schizophrenia is a very complex disease, and 50% of what causes schizophrenia is due to things other than your DNA.”
“Like what? What else could be contributing to Olivia’s schizophrenia that wouldn’t necessarily affect me?” Ella asked.
Dr. Jacobson replied, “There are many, many environmental influences that seem to play a role in the development of this disease, such as increased stress and anxiety, or difficult relationships with other people. Interestingly, there is some research that suggests that the environment itself might even play a role at influencing one’s DNA at the molecular level. It’s a concept called epigenetics. An example of epigenetics in nature is the calico cat. Each calico cat has a unique orange and black fur colour pattern because of alterations, called epigenetic changes, which occur within the cells that produce coat colour during the cat’s development. Research in the field of epigenetics suggests that individuals with schizophrenia appear to have some of these epigenetic changes to their DNA that are due to environmental influences, and that these alterations could be contributing to their development of mental illness.”
“But wouldn’t I also have these ‘epigenetic alterations’ in my DNA?” Ella asked.
“Not necessarily, because you and Olivia have not experienced completely identical environments throughout your lives. For example, you and Olivia have had different teachers and jobs throughout high school. And I also understand that you spent many childhood summers with a friend and her family out in the Rocky Mountains, while your sister was off at swim camps. If you are interested, I can give you some literature to read about this subject.”
Ella was definitely interested. She took the articles and headed home.
What really is “epigenetics”?
Ella felt like she was back in school. The more she read about the topic of epigenetics, the more fascinated she became, and she found herself spending most of her days on the Internet doing research. Ella had learned about genetics in her general biology class and thought she had a pretty good idea of how the Laws of Mendel worked, but this whole field of epigenetics seemed to take the idea of inheritance to another level. She was particularly fascinated by an article that Dr. Jacobson had given her regarding epigenetic differences between identical twins. The article suggested that during one’s lifetime, epigenetic changes occur to one’s DNA that can affect gene expression, and therefore whether or not one will express a certain trait. These epigenetic changes are influenced by one’s environment and behaviors, so despite having identical DNA, identical twins will not always have the same epigenetic changes, and therefore, will not always express the same traits.
Case Key Words
Central Nervous System
Epigenetics
Inheritance
Mental Health
Schizophrenia
Ella and Olivia's Health: Schizophrenia
Olivia’s Diagnosis
Olivia was diagnosed with Schizophrenia. Schizophrenia is classified as a psychotic disorder, in which a person goes into an abnormal state of consciousness. The higher functions of the mind are disrupted. Some combination of a person’s perceptions, thought processes, beliefs, and emotions become disconnected from reality. Symptoms may come and go.
Positive Symptoms of Schizophrenia
Positive symptoms are those that are present in someone with schizophrenia that someone without schizophrenia or another mental health condition would not experience.
Delusions:
False beliefs that don’t make sense in context to a person’s culture. Obsessive quality.
Hallucinations:
False sensory experiences that have no basis in the external world. Fully awake and not under the influence of alcohol or drugs. (auditory, visual, tactile).
Disorganized speech:
Words are linked together based on sound, rhyme, puns, or free association.
Disorganized behaviour:
Not goal-directed. Laughing inappropriately. Adopting strange postures or freezing (catatonic behaviours).
Negative Symptoms of Schizophrenia
The person is experiencing an absence or reduction of certain traits that are often present in healthier individuals. Feels like something is being taken away or disappearing.
Flattened affect
Anhedonia
Reduced speech
Lack of initiative
Cognitive Symptoms of Schizophrenia
Cognitive symptoms are not used to diagnose schizophrenia.
Pursue self-help & therapy that helps you manage your symptoms
Set and work towards the goal
Tip 2: Get active
Aim for 30 minutes per day
Rhythmic exercise that uses both arms and legs
Focus on how your body feels as you move
Tip 3: Seek fact-to-face support
Turn to trusted friends & family
Stay involved with others
Meet new people
Find a supportive living environment
Take advantage of support services
Tip 4: Manage Stress
Know your limits
Use relaxation techniques
Manage your emotions
Tip 5: Take care of yourself
Get plenty of sleep
Avoid alcohol & drugs
Eat healthy, balanced diet
Tip 6: Understand the role of medication
Medication is not a cure
Only treats some of the symptoms
Don’t put up with disabling side effects
Ella and Olivia's Health: Epigenetics
What is Epigenetics?
Genes play an important role in your health; So do your behaviours and environment. Epigenetics is the study of how your behaviours and environment can cause changes that affect the way your genes work. Epigenetic changes are reversible and do not change your DNA sequence. They change how your body reads a DNA sequence. Gene expression refers to how often or when proteins are created from the instructions within your genes. While genetic changes can alter which protein is made, epigenetic changes affect gene expression to turn genes “on” and “off.”
How Does Epigenetics Work?
Epigenetic changes affect gene expression in different ways. Types of epigenetic changes include:
DNA Methylation
DNA methylation works by adding a chemical group to DNA. Typically, this group is added to specific places on the DNA, where it blocks the proteins that attach to DNA to “read” the gene. This chemical group can be removed through a process called demethylation. Typically, methylation turns genes “off” and demethylation turns genes “on.”
Histone modification
DNA wraps around proteins called histones. DNA wrapped tightly around histones cannot be accessed by proteins that “read” the gene. Some genes are wrapped around histones and are turned “off” while some genes are not wrapped around histones and are turned “on.” Chemical groups can be added or removed from histones and change whether a gene is unwrapped or wrapped (“on” or “off”).
Non-coding RNA
Your DNA is used as instructions for making coding and non-coding RNA. Coding RNA is used to make proteins. Non-coding RNA helps control gene expression by attaching to coding RNA, along with certain proteins, to break down the coding RNA so that it cannot be used to make proteins. Non-coding RNA may also recruit proteins to modify histones to turn genes “on” or “off.”
How Can Epigenetics Change?
Your epigenetics change as you age, both as part of normal development and aging and in response to your behaviours and environment.
Epigenetics and Development
Epigenetic changes begin before you are born. All your cells have the same genes but look and act differently. As you grow and develop, epigenetics helps determine which function a cell will have, for example, whether it will become a heart cell, nerve cell, or skin cell.
Epigenetics and Age
Your epigenetics change throughout your life. Your epigenetics at birth is not the same as your epigenetics during childhood or adulthood.
Epigenetics and Reversibility
Not all epigenetic changes are permanent. Some epigenetic changes can be added or removed in response to changes in behavior or environment.
Epigenetics & Health
Epigenetic changes can affect your health in different ways:
Infections
Germs can change your epigenetics to weaken your immune system. This helps the germ survive.
Cancer
Certain mutations make you more likely to develop cancer. Likewise, some epigenetic changes increase your cancer risk. Epigenetics can be used to help determine which type of cancer a person has or can help to find hard to detect cancers earlier. Epigenetics alone cannot diagnose cancer, and cancers would need to be confirmed with further screening tests.
Nutrition During Pregnancy
A pregnant woman’s environment and behavior during pregnancy, such as whether she eats healthy food, can change the baby’s epigenetics. Some of these changes can remain for decades and might make the child more likely to get certain diseases.
Resources
Text Resources
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Central Processing. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). Patterns of Inheritance. Anatomy and Physiology. OpenStax.
Betts, J. G., Johnson, E., Young, K. A., Wise, J. A., Poe, B., Kruse, D. H., … DeSaix, P. (2013). The Central Nervous System. Anatomy and Physiology. OpenStax.
Boyadjieva, N., & Varadinova, M. (2012). Epigenetics of psychoactive drugs. Journal of Pharmacy and Pharmacology, 64(10), 1349-1358.
Evans, L., Engelman, M., Mikulas, A., & Malecki, K. (2021). How are social determinants of health integrated into epigenetic research? Social Science & Medicine, 273, 1-17. https://doi.org/10.1016/j.socscimed.2021.113738
Xing Tan, T., & Jordan-Arthur, B. (2012). Adopted Chinese girls come of age: Feelings about adoption, ethnic identity, academic functioning, and global self-esteem. Children and Youth Services Review, 34(8), 1500-1508. https://doi.org/10.1016/j.childyouth.2012.04.001

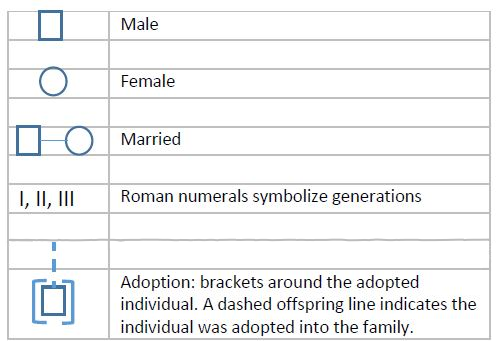
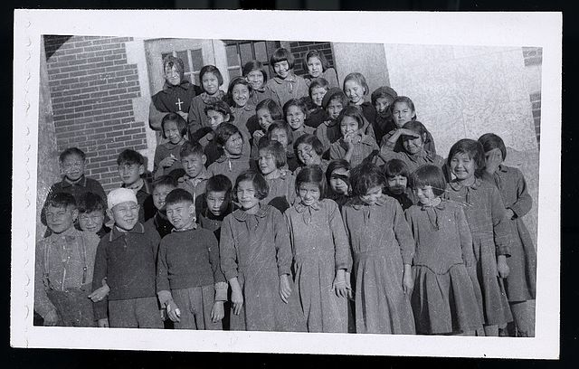

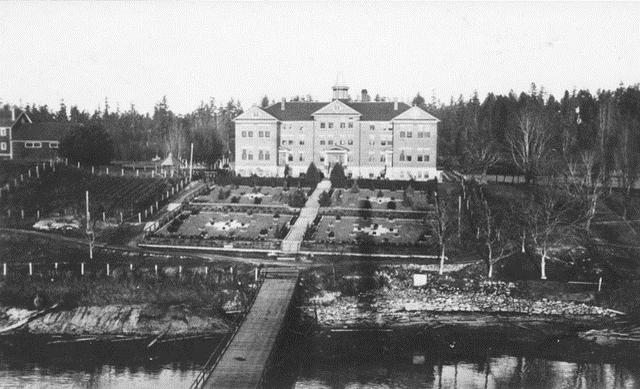

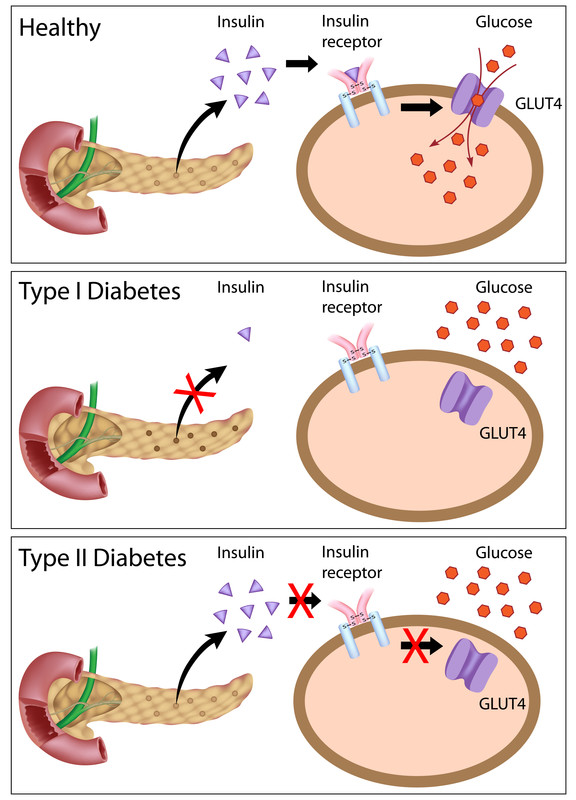
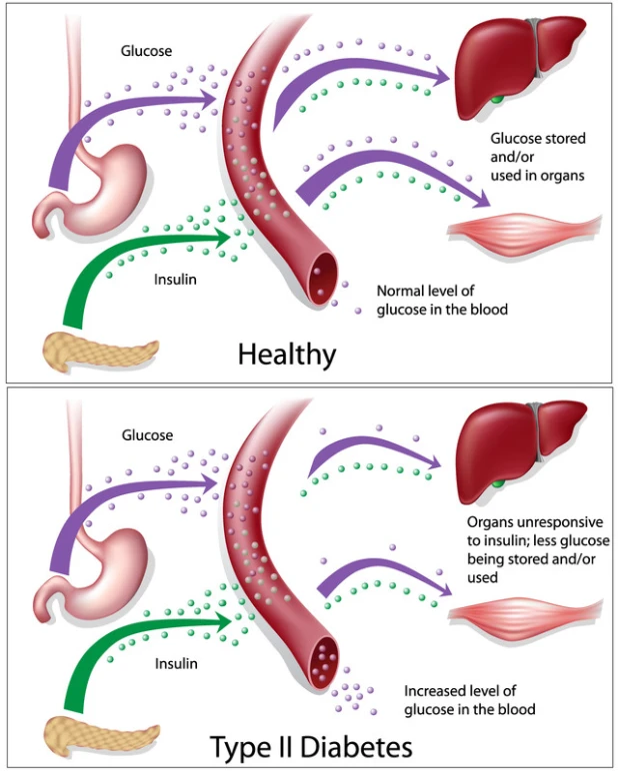
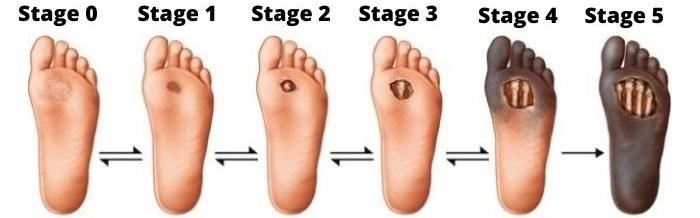


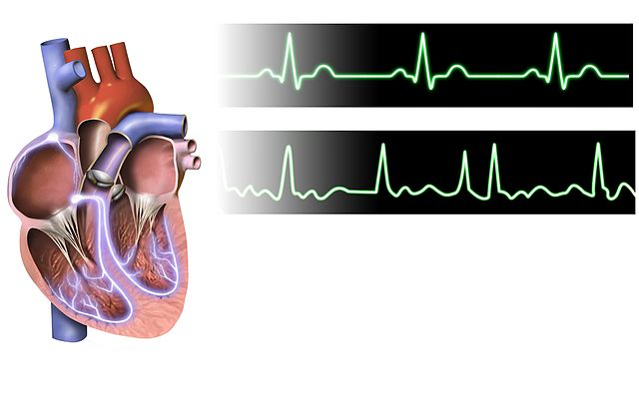
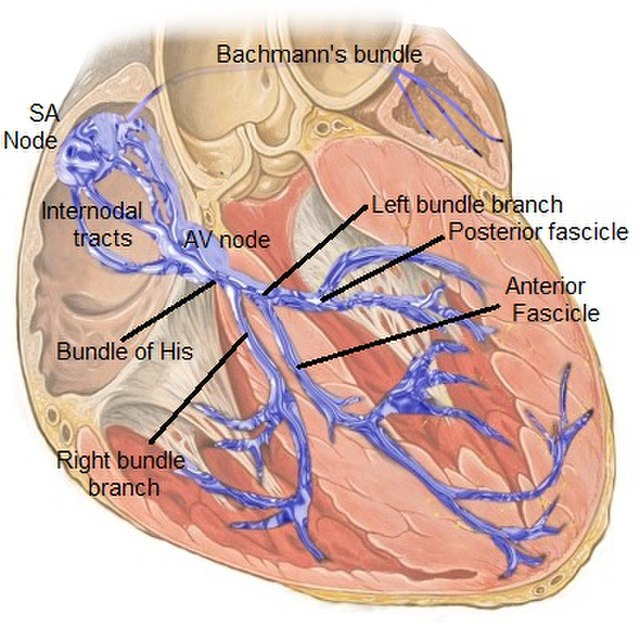
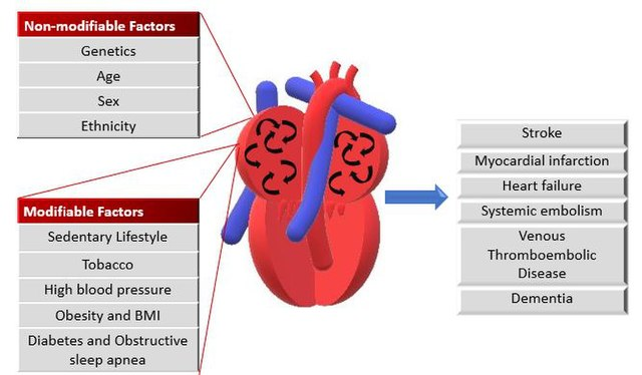
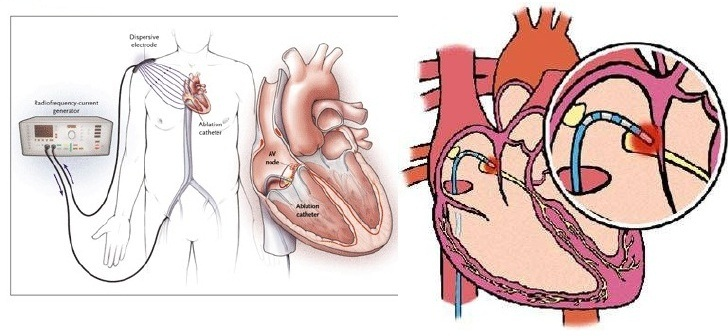


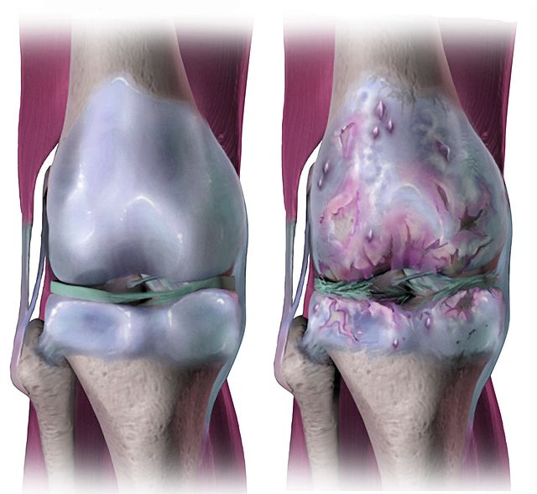
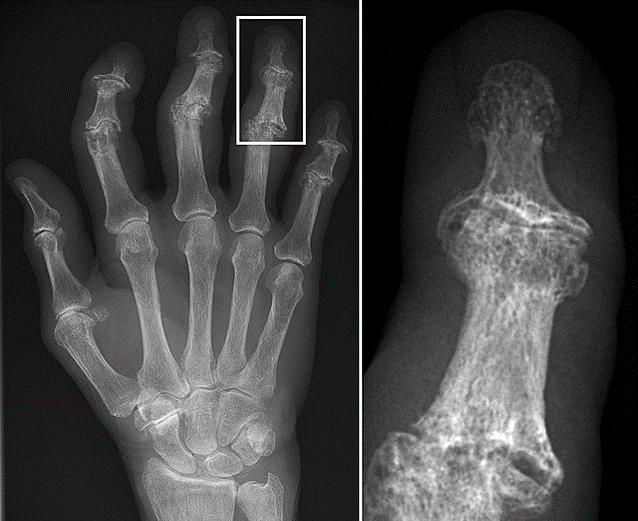
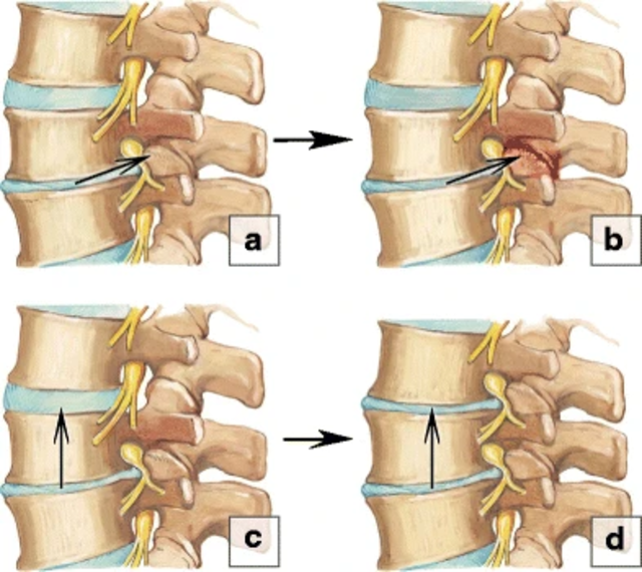
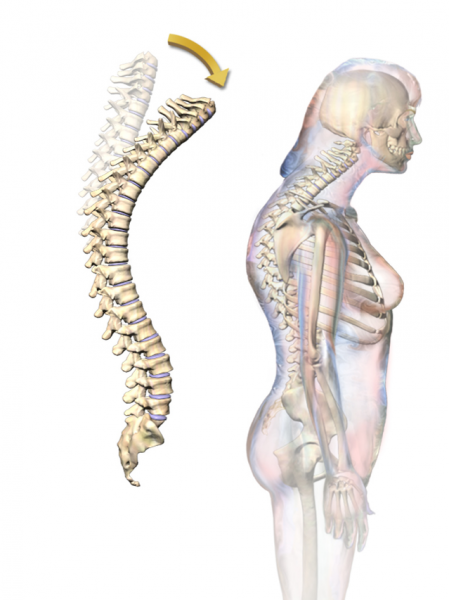
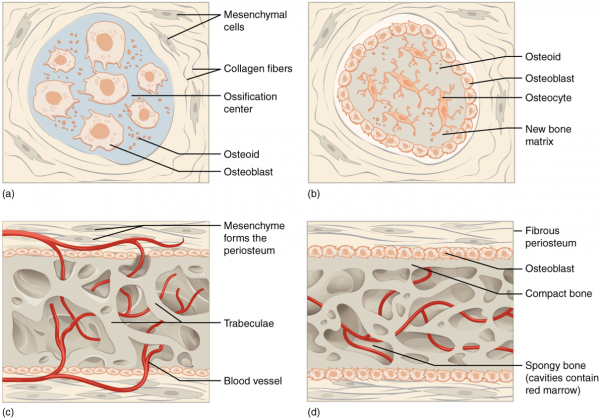
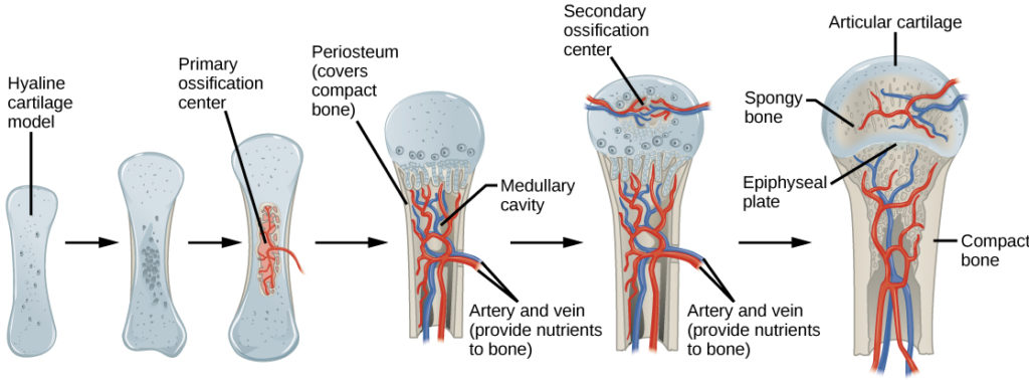
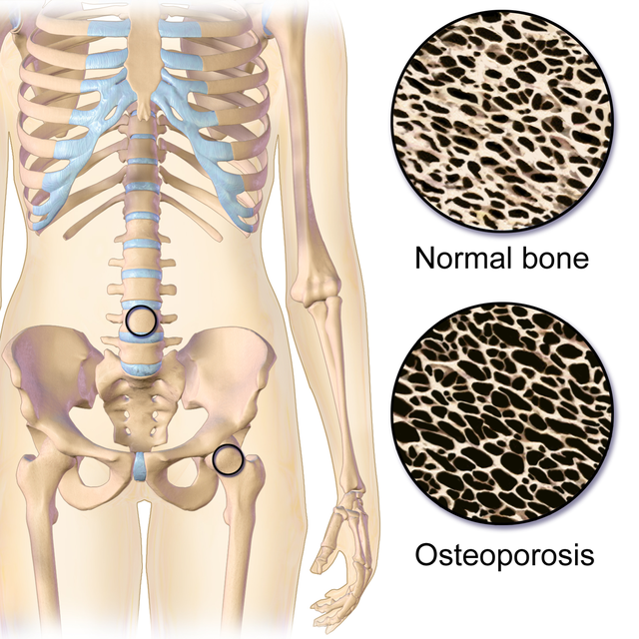
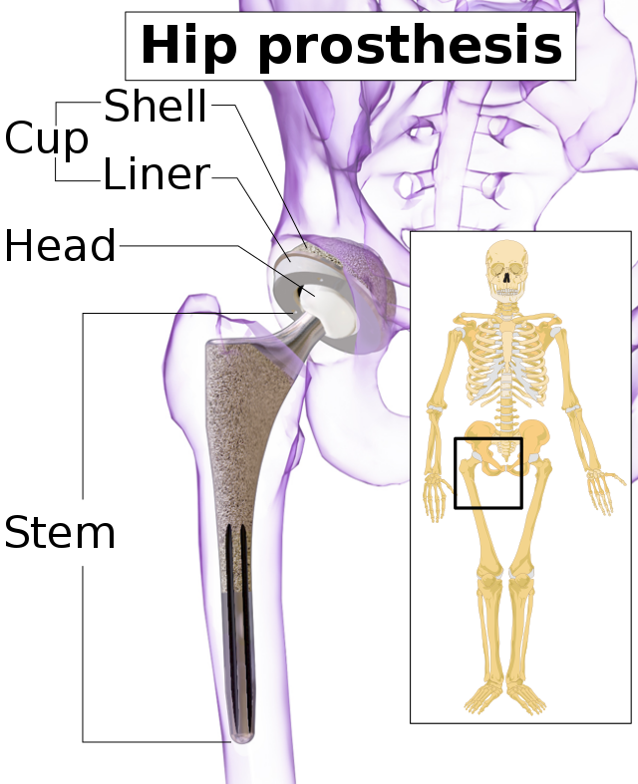

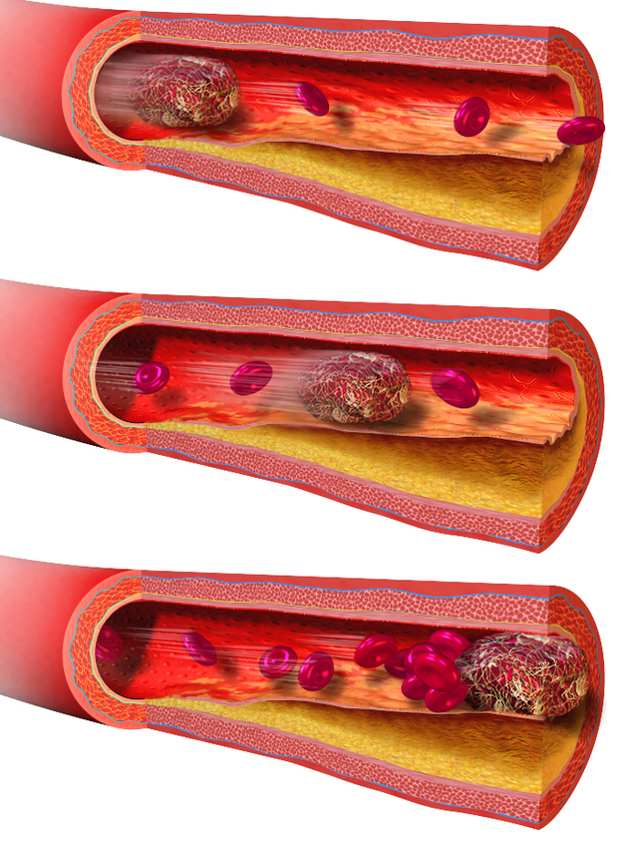
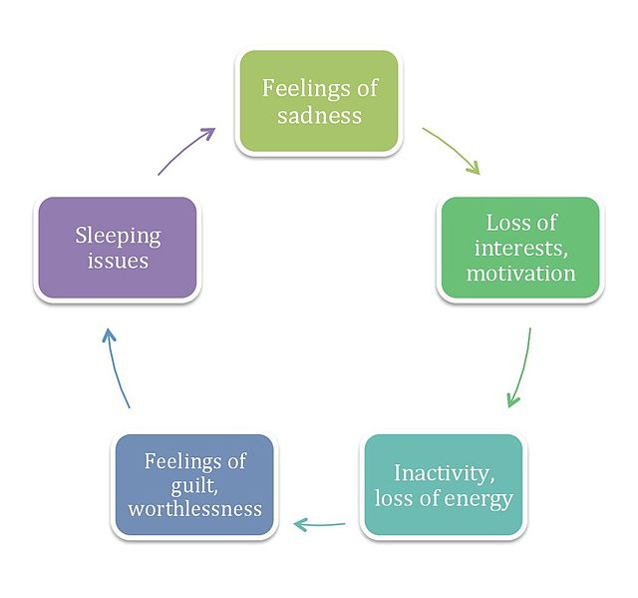





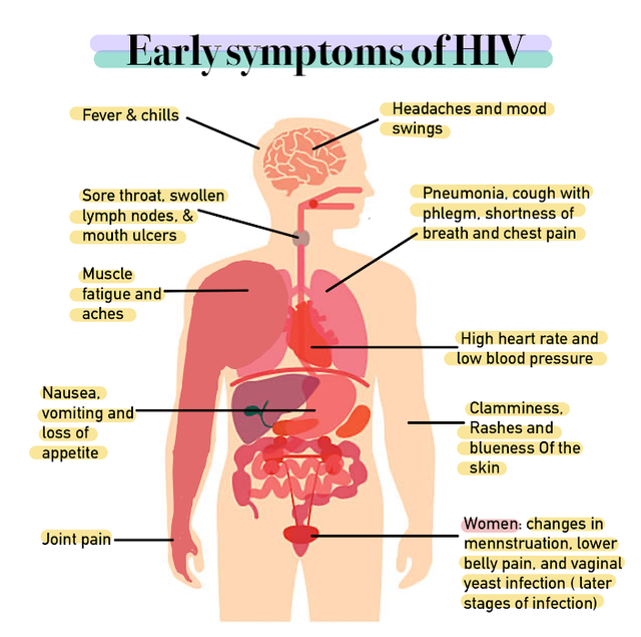
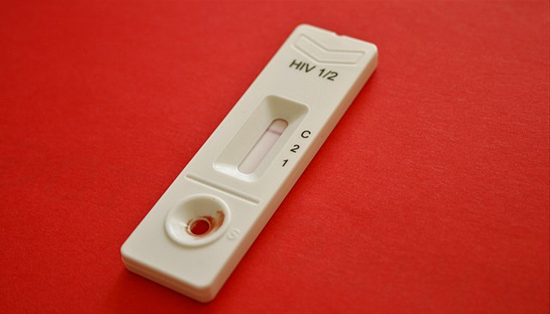


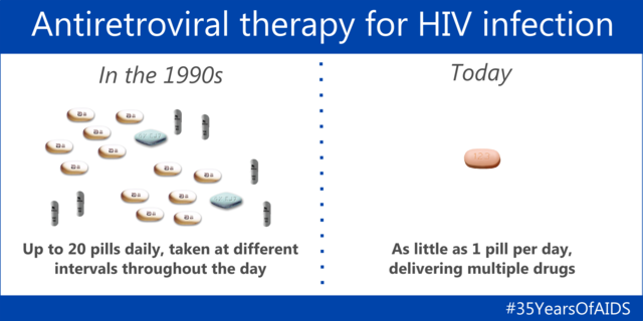
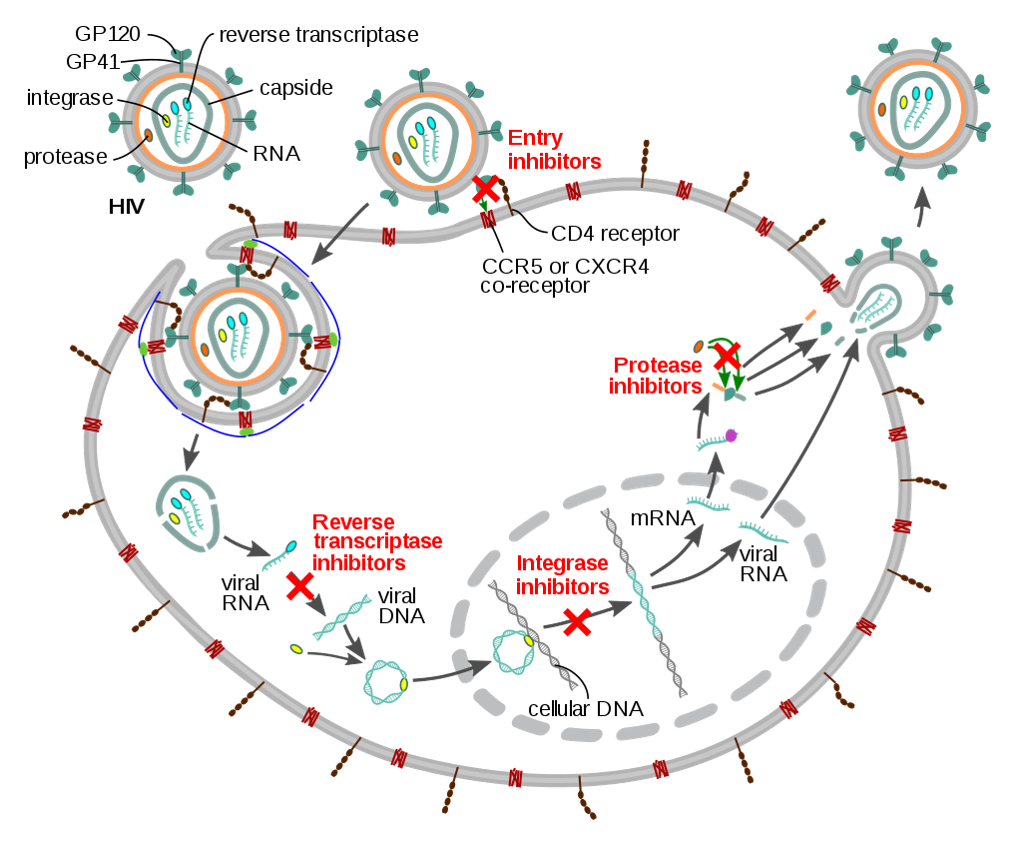


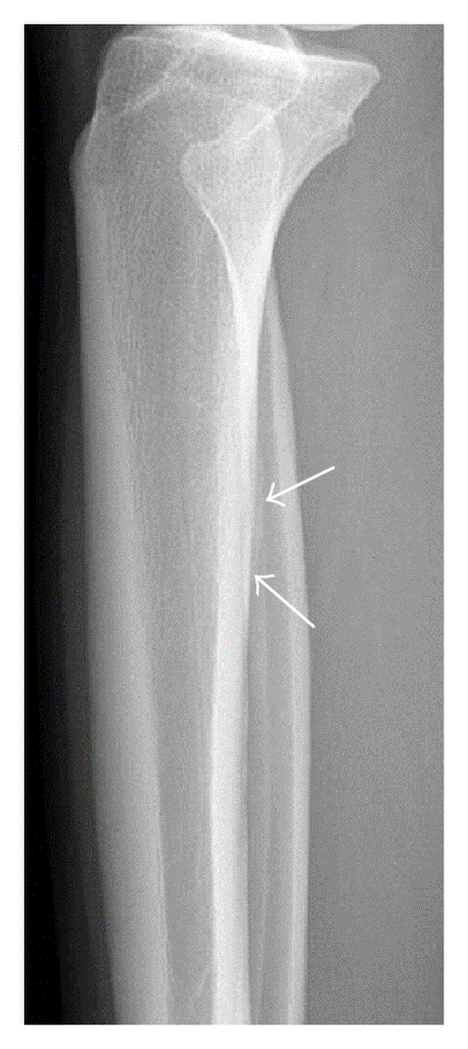
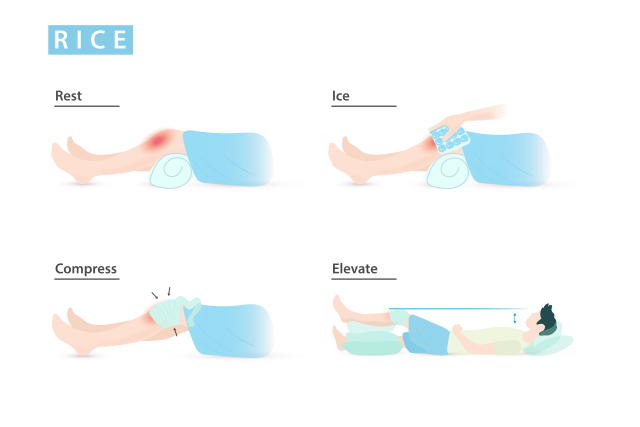
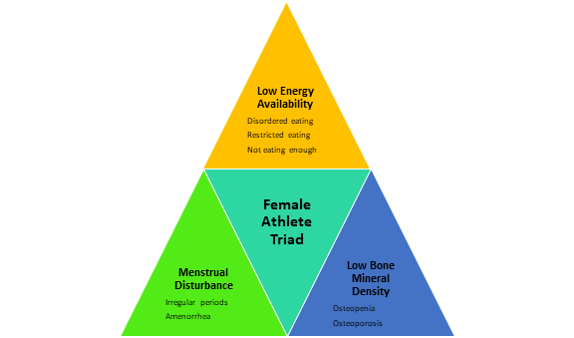
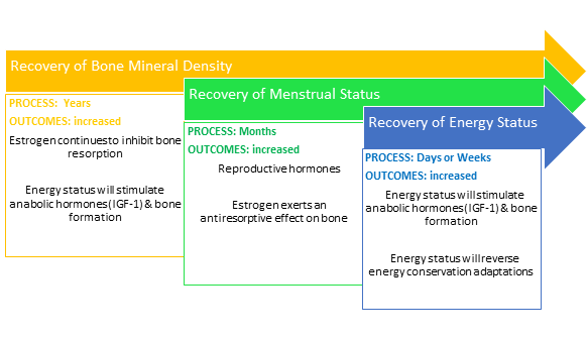
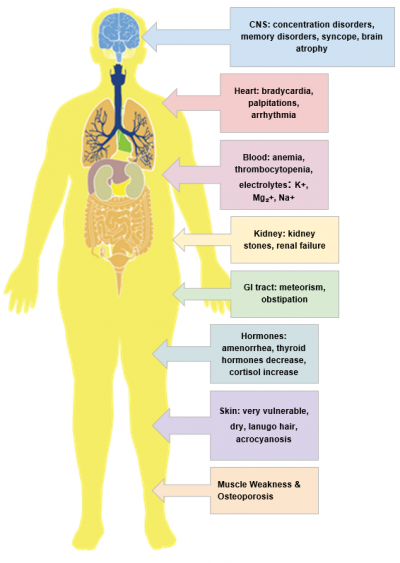

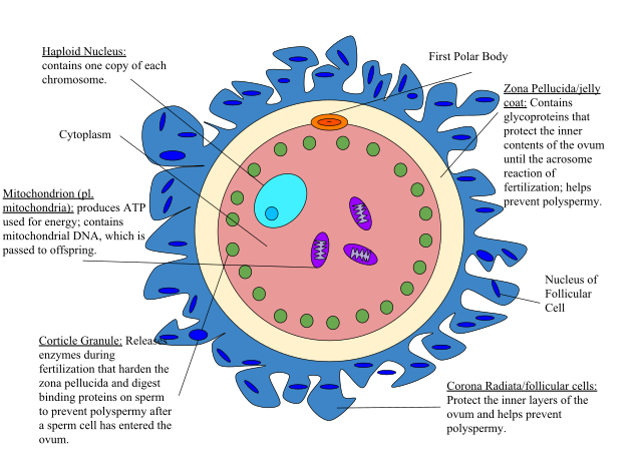
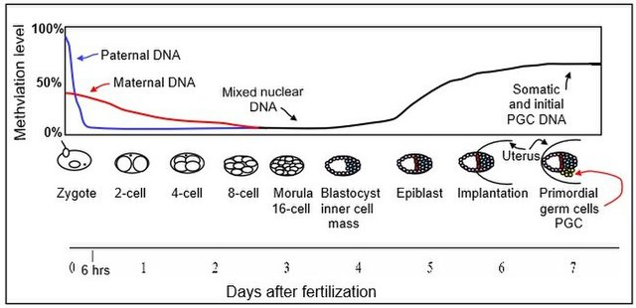
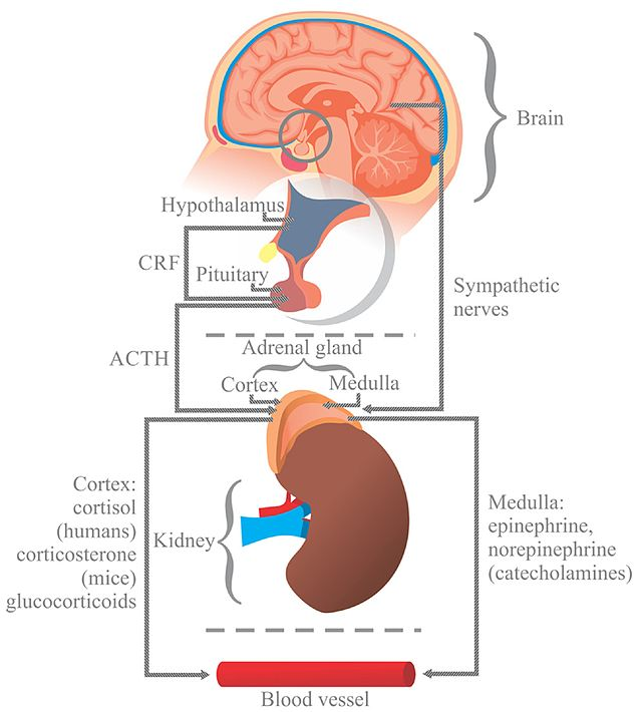
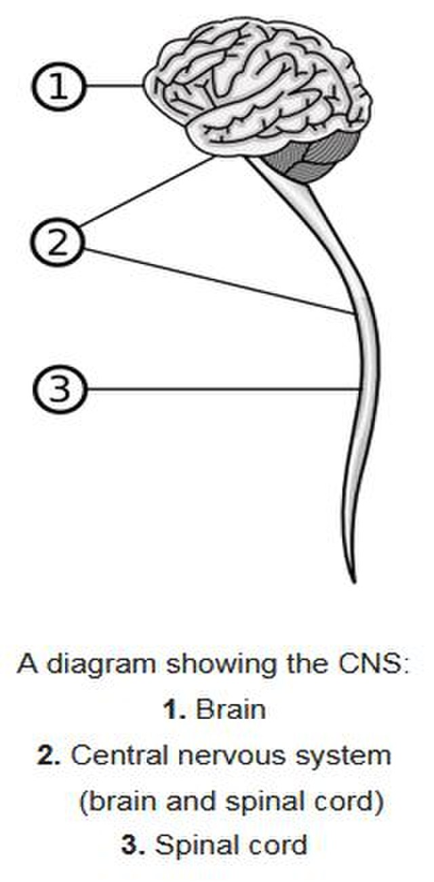
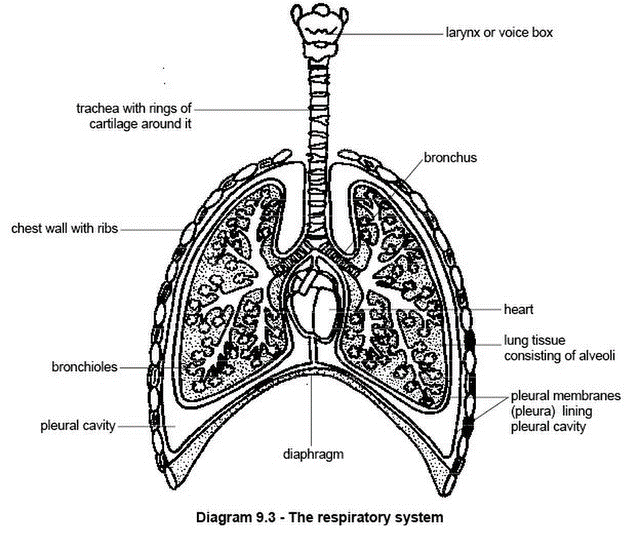
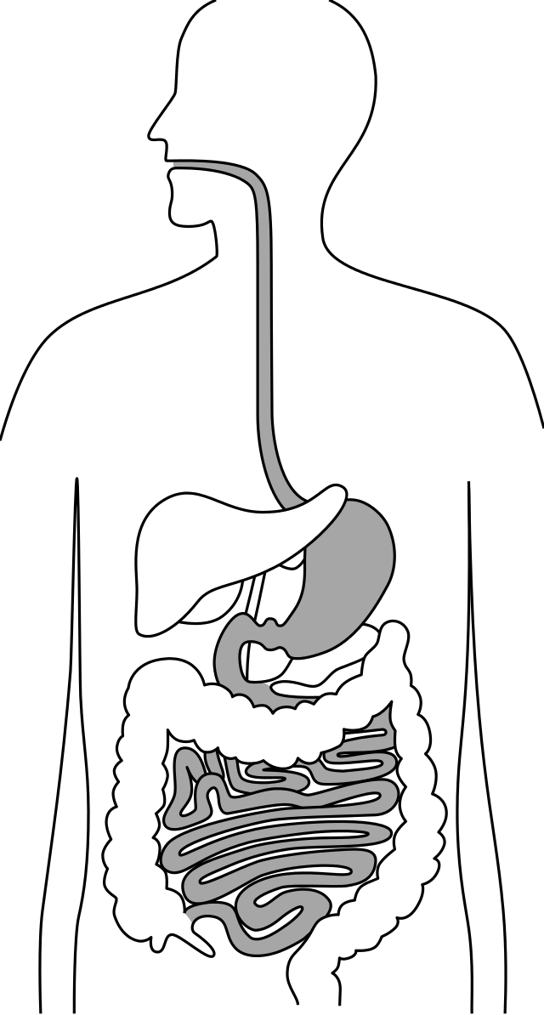

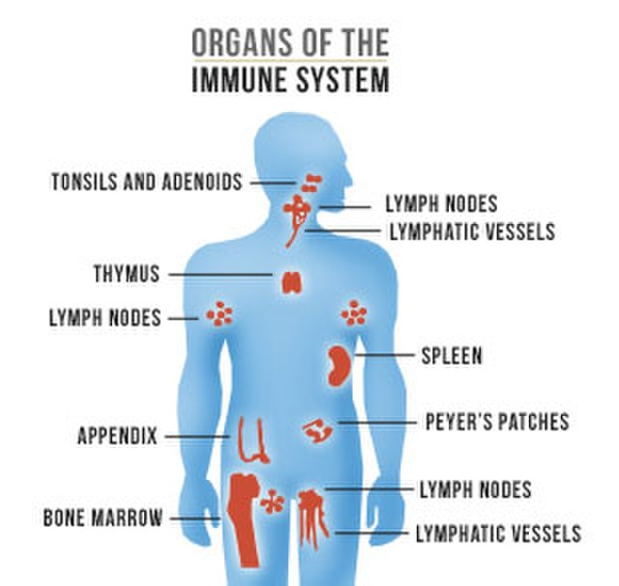

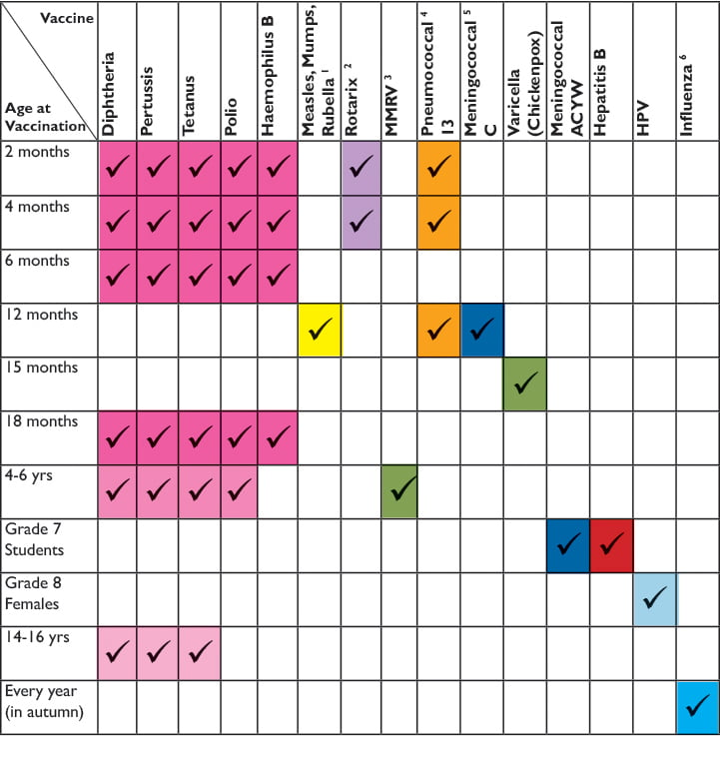

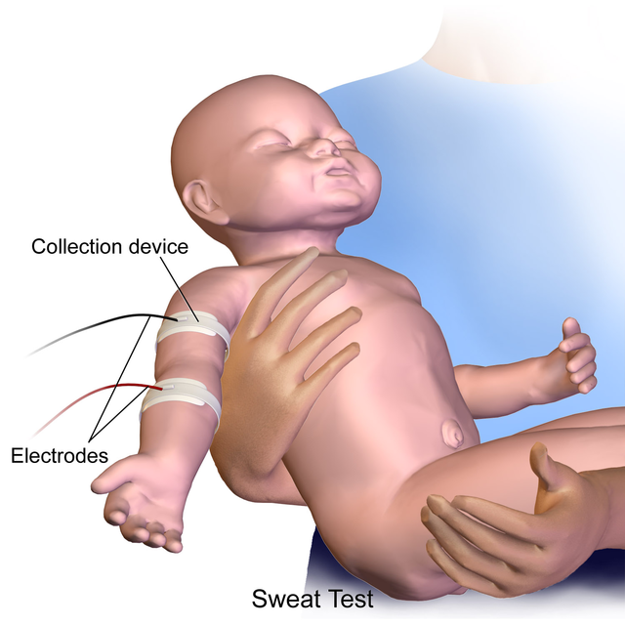

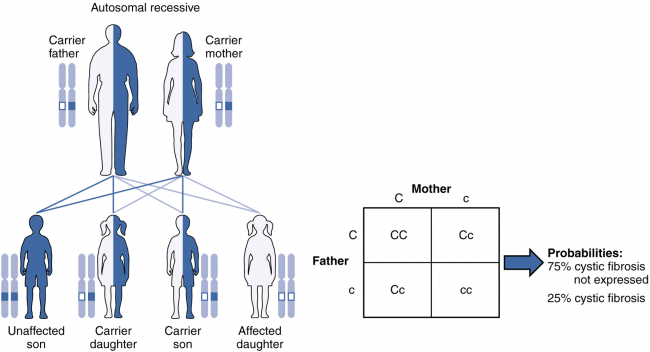
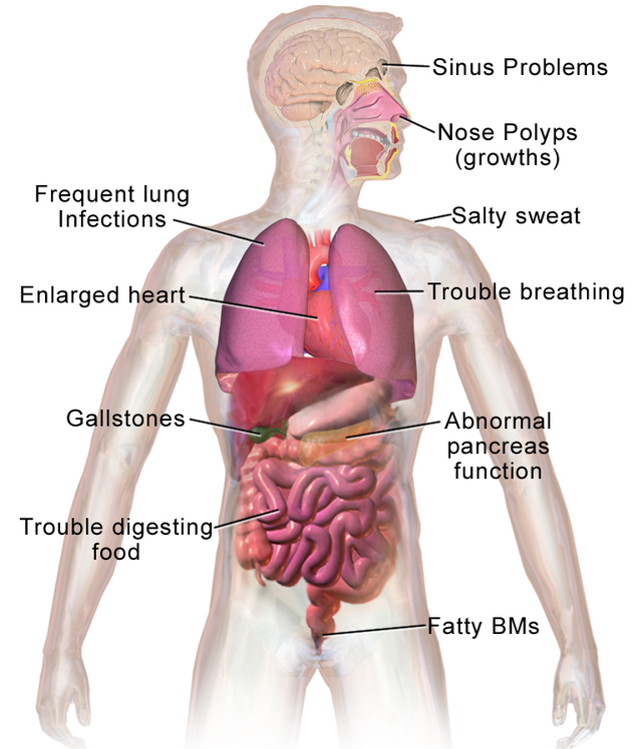
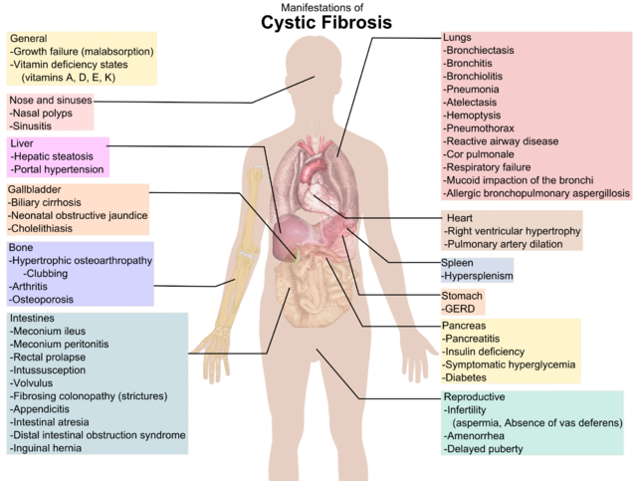
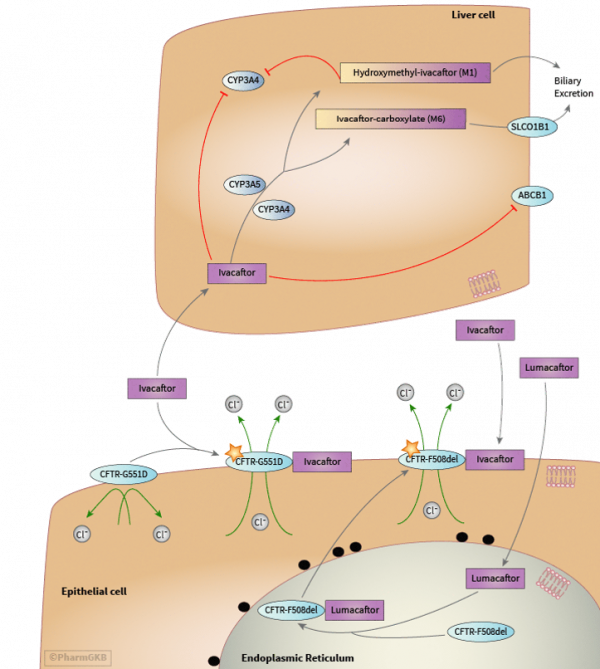



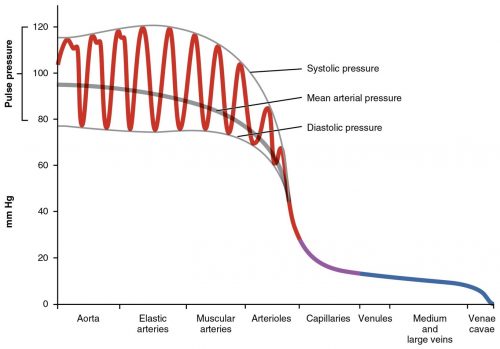
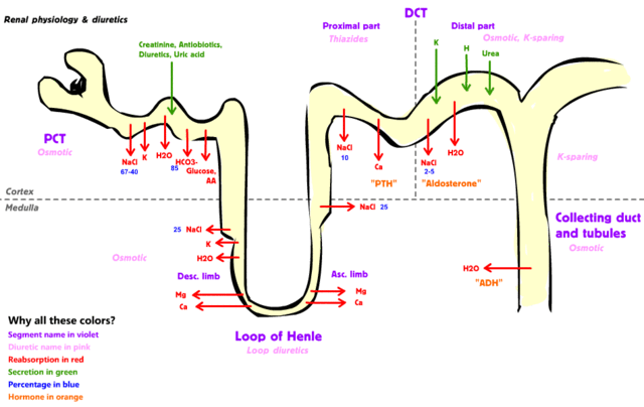

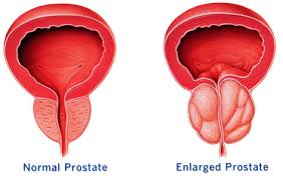
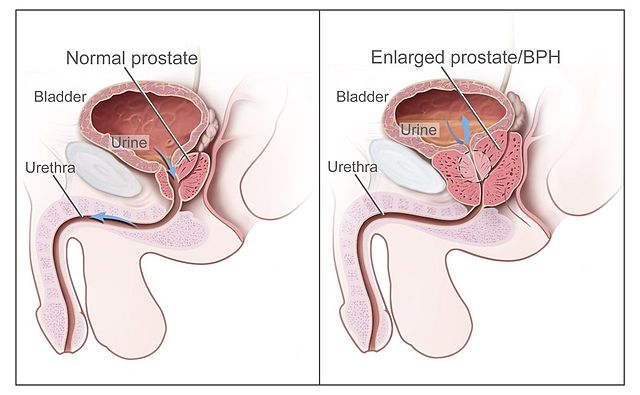
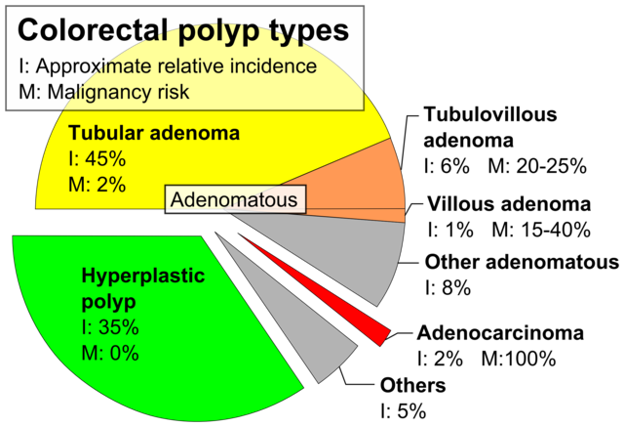
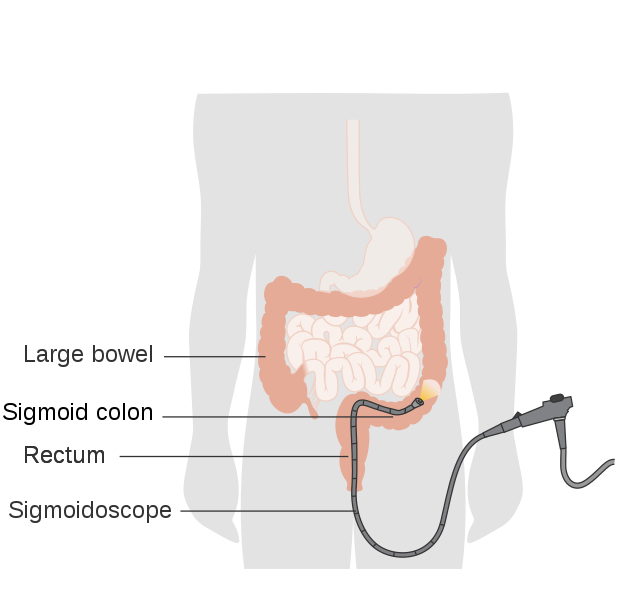


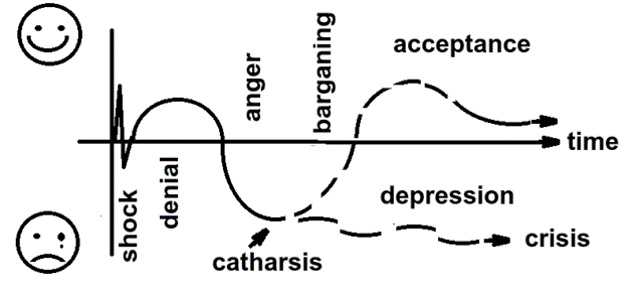



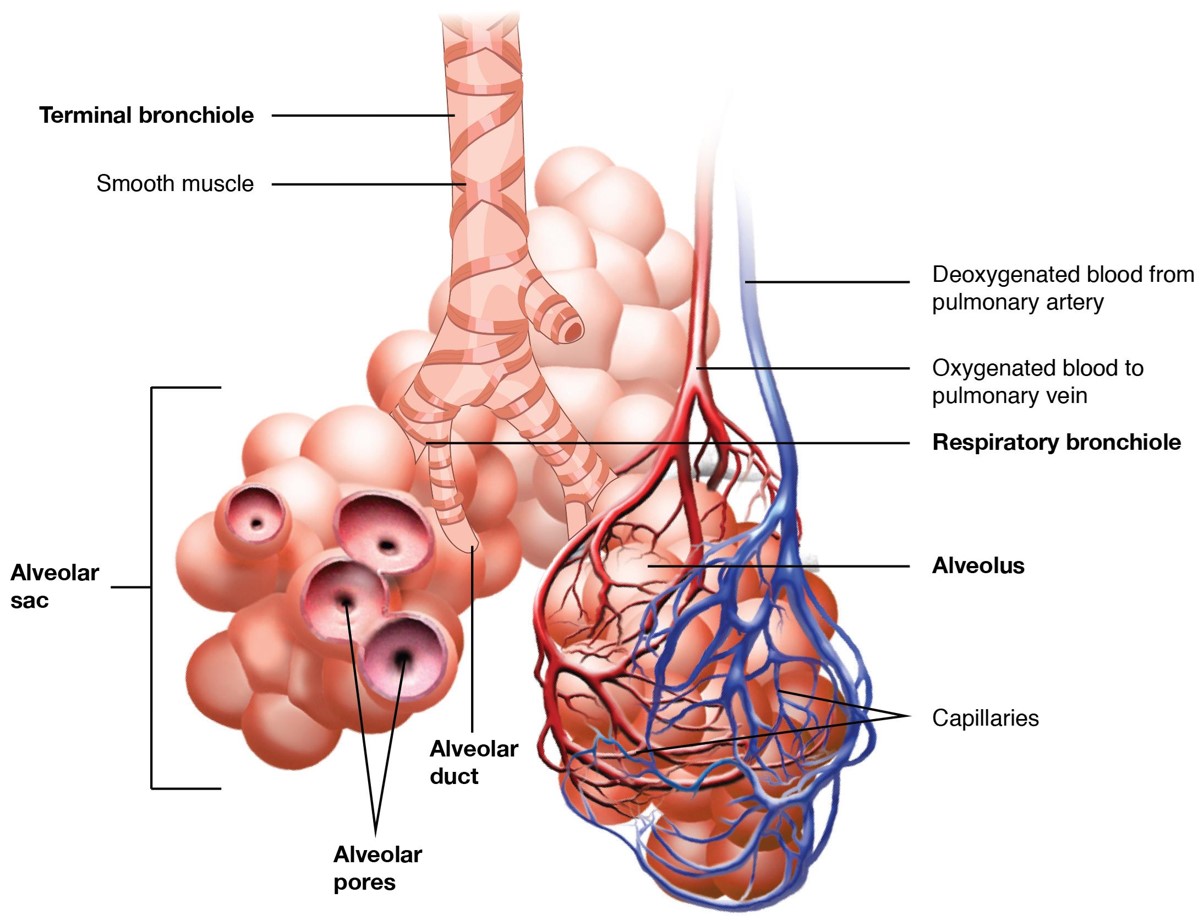
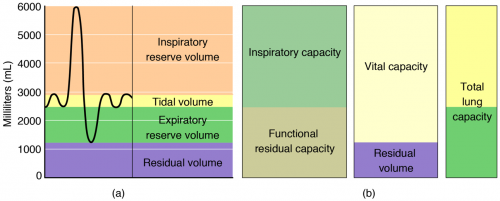
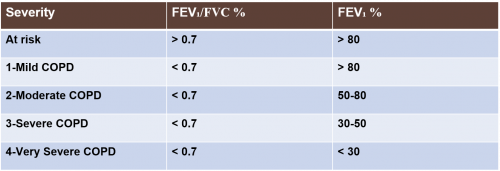


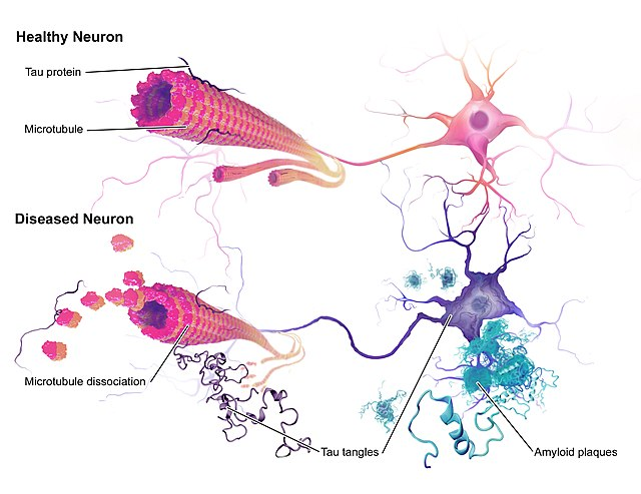
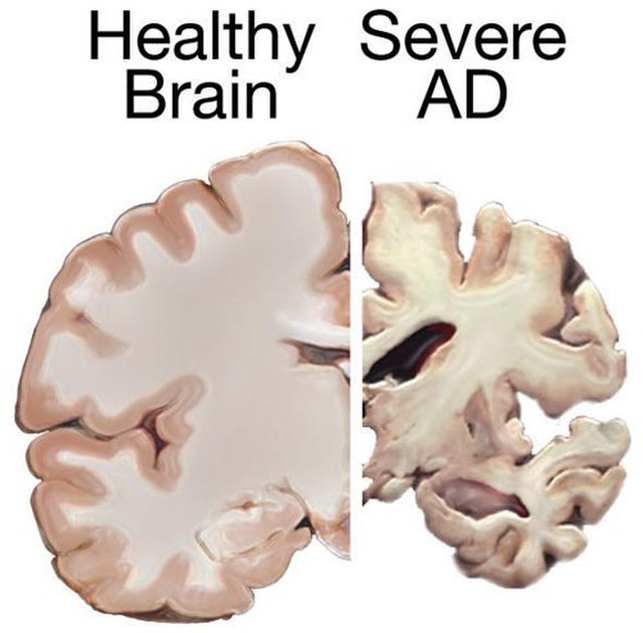
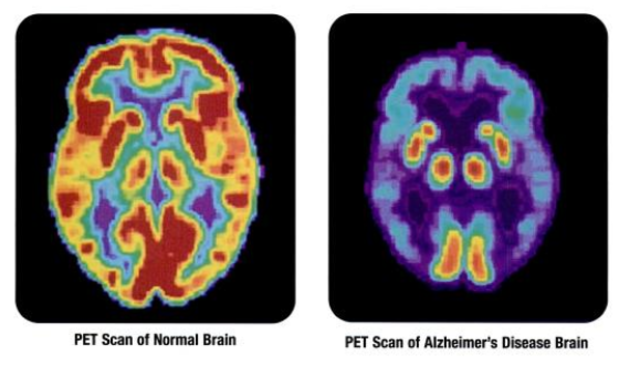



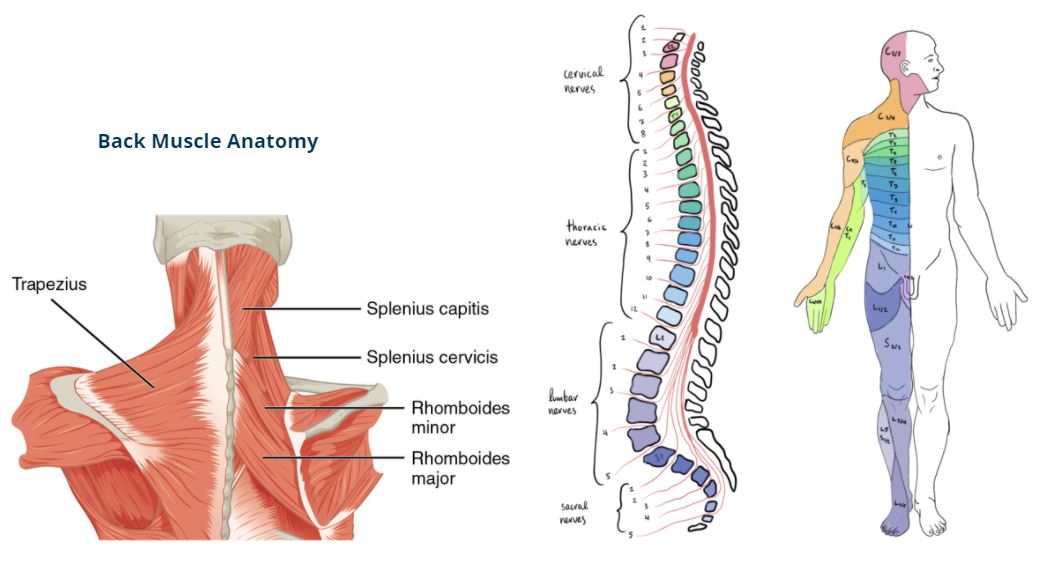
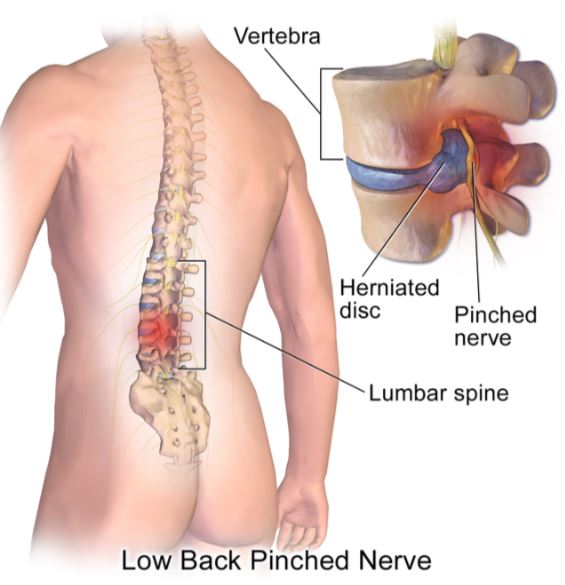
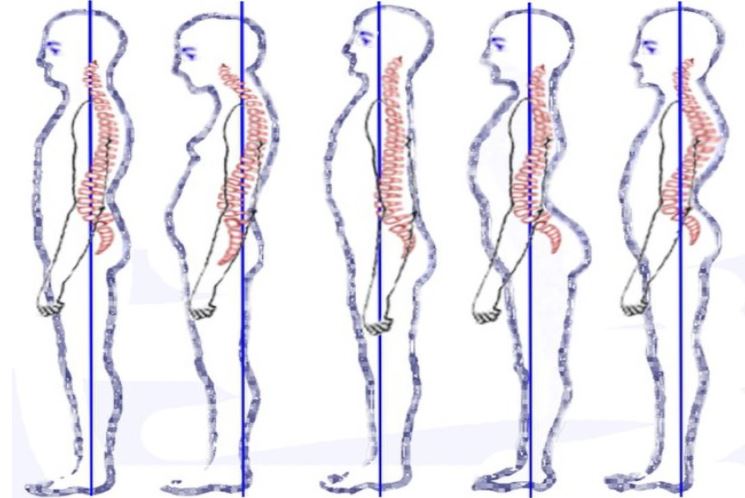
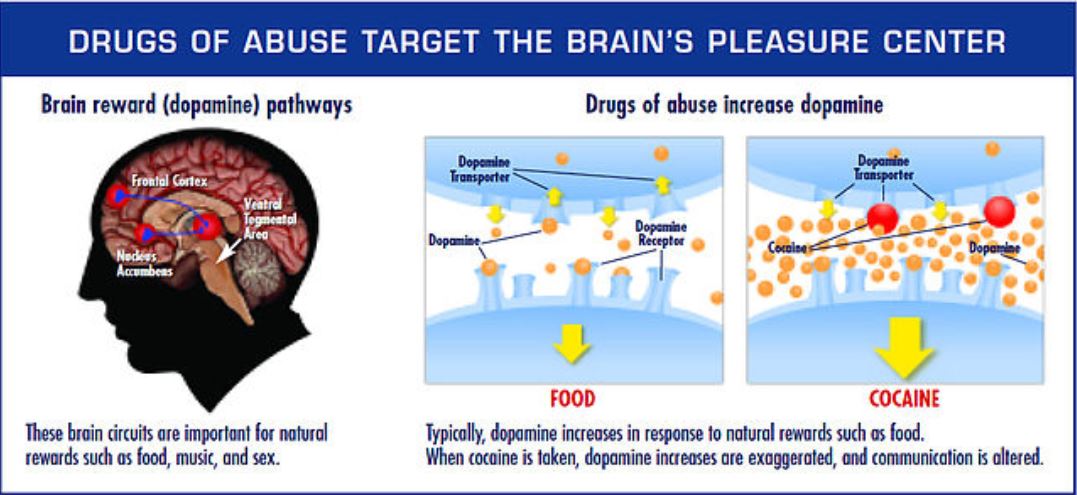
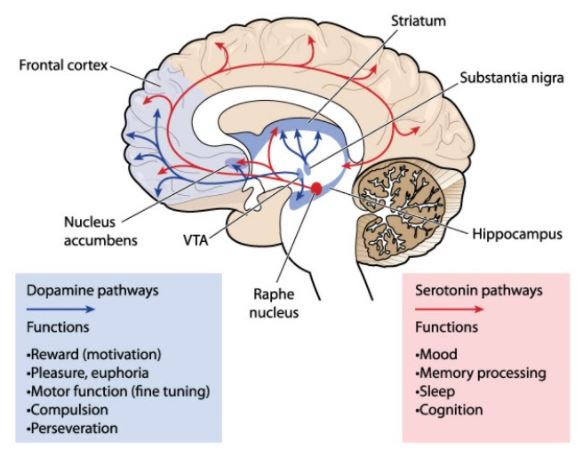



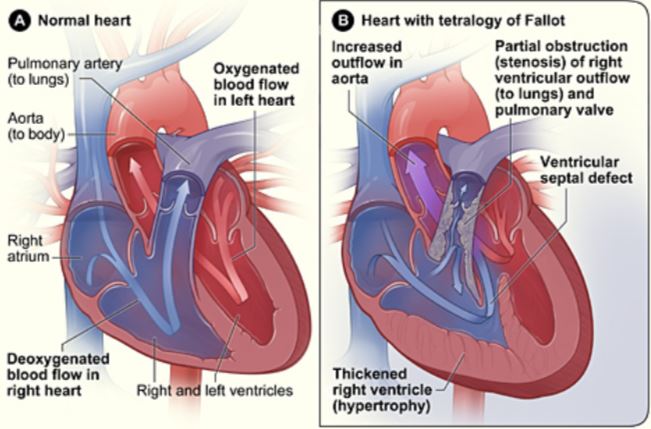
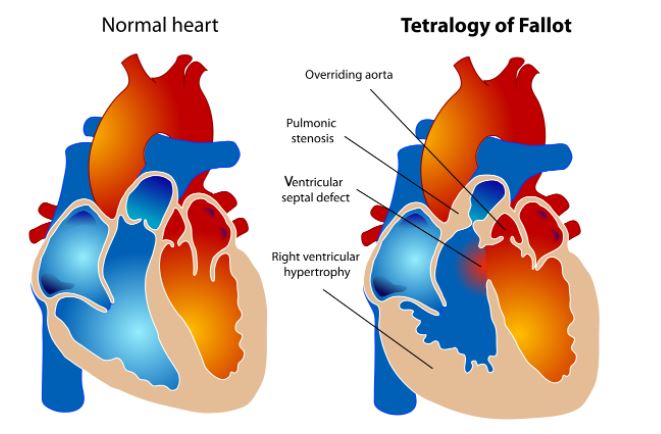

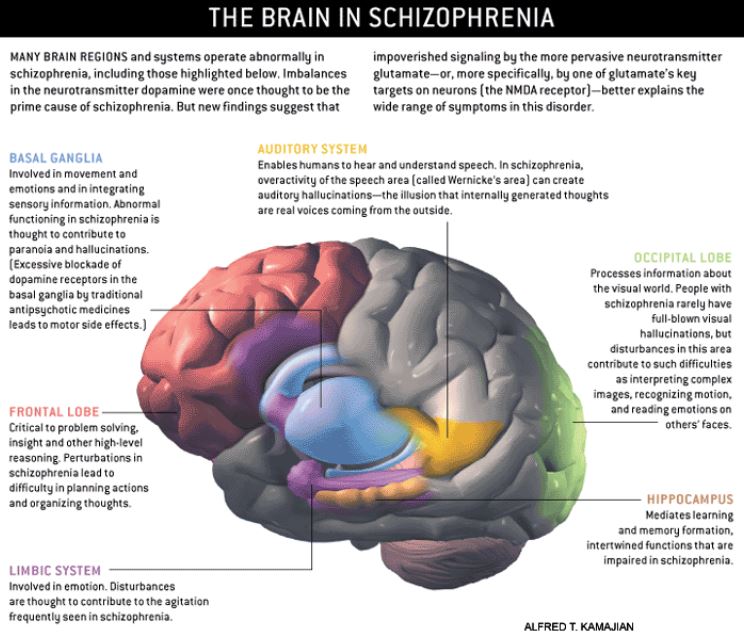
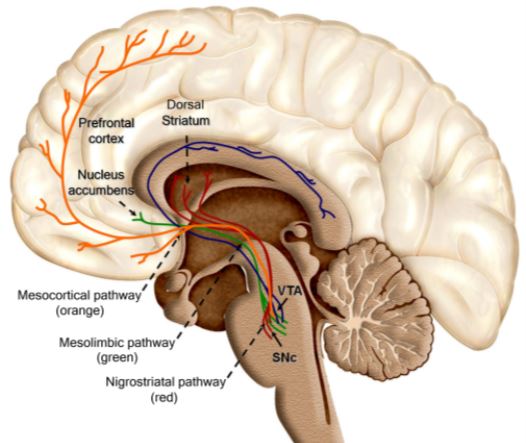
{kind=link}