Introduction to this Guide
I

One in 17 hospital stays in Canada involves harmful events related to healthcare and medication errors, as highlighted by the Institute for Safe Medication Practices (ISMP) Canada and the Canadian Institute for Health Information (CIHI). In light of the significant concern for patient safety related to medication errors in Canada, this guide is designed for clinical instructors. A focus on patient safety underscores the crucial role instructors play as they aim to effectively guide students through the complexities of safe medication administration practices, while reducing the anxiety that students experience.
References
Canadian Institute for Health Information. (2024). Canadian Institute for Health Information. Retrieved from https://www.cihi.ca/en
Institute for Safe Medication Practices Canada. (2024). ISMP Canada Safety Bulletins. Retrieved from https://ismpcanada.ca/safety-bulletins/
By the end of this book, clinical instructors will be able to:
- Understand the role of the clinical instructor in supporting student learning of medication administration.
- Review common approaches to clinical instructor support when students are learning to administer medications.
- Understand factors that contribute to student success when learning medication administration:
- Develop strategies to reduce student anxiety using a pre-briefing model
- Reflect on current practices with safe medication administration and identify where new practices can be integrated.
Traditional Student Learning
The traditional practice of nursing students administering medications in the clinical setting involves a structured, supervised process designed to integrate theoretical knowledge with practical skills, ensuring safe and effective patient care. This practice typically includes several key steps:
- Pre-Clinical (Classroom and Lab) Preparation: Students study pharmacology, medication administration techniques, dosage calculations, and the six to ten rights of medication administration. Depending on the institution, this may include formative testing of their skills and simulated activities.
- Supervised Clinical Experience: During clinical rotations in healthcare settings, students administer medications under the close supervision of a clinical instructor or a licensed nurse, gradually gaining confidence and competency.
- Direct Observation and Verification: Instructors or preceptors closely observe students as they prepare and administer medications, ensuring adherence to safety protocols and correct techniques.
- Documentation: Students accurately document the medication administration process in the patient’s medical record.
- Increasing Independence: As students demonstrate competence, they are granted more independence in medication administration, balancing this autonomy with the need for ongoing supervision to ensure patient safety.
- Feedback, Evaluation and Reflection: Students receive continuous feedback and formal evaluations from instructors and preceptors, encouraging them to reflect on their strengths, areas for improvement, and overall clinical performance.
College of Nurses of Ontario. (2024). Medication Decision Tool. Retrieved from https://www.cno.org/en/learn-about-standards-guidelines/educational-tools/decision-tool-medication/
Clinical Instructor Accountability
II
It is important to note, as per the College of Nurses of Ontario (2024), Registered Nurses in the role of instructors are accountable to:
- Ensure they have the knowledge, skill, and judgment to guide, supervise or support the learner safely and competently
- Support learners in developing and refining competencies needed for safe, ethical and effective practice
- Provide orientation, direction, collaborate, and share knowledge and expertise
- Monitor and document their evaluation (as per organizational policies, if applicable)
- Provide feedback on their practice and encourage self-reflection to identify learning needs
While nurses are accountable to support learners, their primary accountability is to place patient safety and well-being above all other objectives.
Checking In with the Standards
- Nursing students are accountable to their educational institutions and placement organization (CNO).
- While students initially learn safe medication administration through classroom and lab instruction, learning all of the components and pharmacology can take weeks or even semesters.
- Foundational training, guided by Ontario’s College of Nurses standards and adopted nursing textbooks, culminates in supervised clinical practice.
- The “3 checks” and “10 Rights of Medication Administration” best practice that is widely taught in nursing and pharmacology courses is central to this learning. It ensures students verify critical factors like the correct patient, medication, dose, time, and route to enhance patient safety and minimize errors in medication administration.
For more detail, refer to
Safe Med Admin CNO and 10 Rights of Medication Administration (4).docx
(Condensed from CNO.org)
Expecting students to flawlessly execute all components of medication research and the “10 Rights of Medication Administration” from the outset may not be reasonable, considering that learning is a process that involves building upon knowledge and skills through practice and making mistakes. While the “10 Rights” serve as a critical framework for ensuring patient safety and minimizing medication errors, an overly rigid expectation for perfection might contribute to student anxiety, fear of making mistakes, hindering the learning process, and increasing the likelihood of error. It’s important to foster an environment where students can learn under clinical supervision, encouraging growth and confidence in their clinical judgment and skills, yet not be entirely responsible for all aspects of the patient’s safety. The partnership of a clinical instructor with the student allows for responsibility to be shared until the student has mastered the knowledge, skills and judgment to have more autonomy.
Adopting strategies such as preparation, pre-briefing, and a layered learning approach is vital in teaching nursing students medication administration. Preparation ensures students are familiar with the clinical setting and common medications, while pre-briefing sets clear expectations and emphasizes safety. A layered learning approach builds foundational knowledge, which is reinforced through guided experiences, critical thinking exercises, and peer learning. These methods collectively foster a supportive environment that encourages growth, critical thinking, and independence. Implementing these strategies helps students develop the competence and confidence needed for safe and effective patient care, making them crucial for clinical instructors committed to nurturing skilled healthcare professionals.
Pre-briefing with the student involves a preliminary discussion to assess their readiness, outline the day’s objectives and expectations, and emphasize safety responsibilities and communication protocols. Pre-briefing is a critical component of simulation-based education, as outlined by the International Nursing Association for Clinical Simulation and Learning ((INACSL), 2021). The principles of pre-briefing can be effectively applied to prepare nursing students for administering medications in the clinical environment.
Here is a suggested outline based on INACSL’s principles for an effective pre-briefing session:
- Introduction and Welcome:
- Welcome the students warmly to create a comfortable learning environment.
- Introduce the purpose of the pre-briefing session to review safety, roles, details, expectations, communication and answer any questions.
- Establish Psychological Safety:
- Identify the importance of a safe learning environment where students can ask questions, make mistakes, and learn from them without fear of judgment.
- Encourage open communication and respect, this includes a discussion on how to approach students to correct or prevent an error.
- Discuss Roles and Responsibilities:
- Define the roles of the students, instructors, and any other participants in the clinical setting.
- Outline the expectations for student performance and behavior, including professionalism, communication with the healthcare team, and patient interaction. This includes:
- Student expectations such as: correctly selecting the medications, calculating dosages, and doing the 3 checks, and a number of the rights.
- Clinical instructor responsibilities, such as understanding medication actions and side effects and monitoring for correct steps and intervening to prevent errors.
- Staff nurse responsibilities
- It is important to identify who will administer medications that are not within the current skill set of the student (this is a discussion between the Clinical instructor and the Staff Nurse
- Operational details:
- Go over any logistical details, such as the schedule for the day, the location of medications and supplies, and the use of any electronic health records or medication administration records.
- Explain the process for medication verification and administration, including any checks and balances in place.
- Ensure familiarity with relevant protocols and policies
- Safety Emphasis:
- Emphasize the critical importance of patient safety and error prevention strategies.
- Discuss the procedures for handling medication errors, should they occur.
- Communication Protocols:
- Review the protocols for communicating with clinical staff, instructors, and patients.
- Highlight the importance of using clear, professional communication and proper documentation.
- Q&A and Reassurance:
- Open the floor for any questions or concerns from the students, providing clear and concise answers.
- Reassure students about the support available to them throughout the clinical experience.
- Closure:
- Summarize the key points discussed during the pre-briefing.
- Encourage students to approach the medication administration experience with confidence and a readiness to learn.
- Evaluation and Feedback:
- Briefly explain how students will be evaluated on their medication administration skills.
- Highlight the importance of self-reflection and feedback in the learning process.
Pre-briefing Example Dialogue
Using the pre-briefing process requires practice and preparation. An example of how this dialogue may be structured is provided.
“We are going to be administering PO medications today, and for most of you it is your first time. First off, how’s everyone feeling about administering medications? It is okay to have some nerves; it shows you care about doing it right. My role is to support you, so if there’s anything on your mind, let’s hear it.”
“I want to talk about how we’ll handle situations where a mistake might be about to happen. My job is to guide you and ensure patient safety. If I see that an error may occur, I will step in promptly. However, I want to do this in a way that feels supportive and constructive to you. How would you prefer I provide this feedback or interrupt in such situations? Would you like a discrete signal or direct intervention?”
“Remember, our primary goal is safety—for you and the patients. While making mistakes is part of learning, we will do everything to avoid that from happening. I’m here to help navigate any situations and handle any errors before they happen”.
“Let’s make sure you’re familiar with where everything is and how to use the electronic records. This knowledge will help reduce stress and minimize errors. And if you’re unsure, please ask before taking action.”
“For today you will be administering only the PO medications for your patient. For today we are just going to focus on the first 5 of the 10 rights. As the clinical instructor I am overall responsible for all aspects of patient safety. As you get more confident with the medication administration process I will add more responsibility to you”
“Any questions or concerns before we begin? Know that I am here for you, not just as an instructor but as a mentor and support system.”
“Alright, let’s move forward with confidence and care. Remember, open communication is key, let me know immediately if things are not going well. I’m here to support you every step of the way. Let’s focus on providing the best care to our patients and learning as much as we can today.”
References
International Nursing Association for Clinical Simulation and Learning. (2021). Healthcare Simulation Standards of Best PracticeTM Prebriefing: Preparation and Briefing. Retrieved from https://www.nursingsimulation.org/article/S1876-1399(21)00095-5/fulltext
Healthcare Excellence Canada. (2023). Healthcare Excellence Canada. Retrieved from https://www.healthcareexcellence.ca/en/what-we-do/all-programs/teamstepps-canada-essentials-course/
Harris, M. A., Pittiglio, L., Newton, S. E., & Moore, G. (2014). Using simulation to improve the medication administration skills of undergraduate nursing students. Nursing Education Perspectives, 35(1), 26–29.
Parvan, K., Hosseini, F., & Bagherian, S. (2018). The relationship between nursing instructors’ clinical teaching behaviors and nursing students’ learning in Tabriz University of Medical Sciences in 2016. Education for Health (Abingdon, England), 31(1), 32–38.
Clinical Instructor Preparation for Medication Administration in the Clinical Setting
IV
Beginning the process of safe medication administration requires the clinical instructor to be aware of many factors that will impact how students are supervised and ensure patient safety is maintained.
Understanding Policies and Procedures
- Familiarize yourself with the facility’s specific medication standardization, policies and procedures and protocols.
- Understand the limitations or restrictions for students at their current stage of education. For example, many institutions do not allow students to administer high risk medications such as insulin.
Access to Medication and Training
- Arrange access to computerized medication carts or Medication dispensing units.
- Gain knowledge of the systems used for medication administration, including electronic patient record, documentation requirements and order entry and MAR.
Medication Administration Handling
Starting with PO Medications
- Students often begin their practical experience by administering oral (PO) and topical medications.
- Progression to other routes of administration is typically phased throughout the semester.
Handling Medications Beyond Initial Scope
- Coordinate with nursing staff to understand how medications outside the student’s current scope will be administered. If the Clinical Instructor will need to administer out of scope medications (IV, SC, insulins etc) or if the staff nurse will cover these.
- Clarify roles and responsibilities to ensure all medications are administered safely and within regulatory guidelines.
Collaboration and Communication
Engagement with Nursing Staff
- Discuss with the nursing staff ahead of time how student involvement in medication administration will be managed.
- Ensure clear communication channels are established for questions and guidance.
Safety and Supervision
- Emphasize how you (the Clinical Instructor) will be responsible for direct supervision and safety checks, when students are administering medications
- Determine under what circumstances the students will be allowed to administer medications under the supervision of the staff nurse.
- Establish a protocol for students to follow when they are unsure about a medication or administration technique.
Optimizing Supervision for Medication Safety
A medication pass is the scheduled process by which healthcare providers, typically nurses, distribute and administer prescribed medications to patients under their care within 1 hour of their scheduled time (refer to individual institutional policy)
The ratio of students to clinical instructors during medication passes must prioritize patient safety and foster a conducive learning environment.
Flexible Ratio Adjustments
Adapt the student-to-instructor ratio to align with the unique demands of the clinical setting and the specific needs of patients under care.
Focused Supervision for Beginners
Initially, instructors should closely supervise a smaller group, ideally 2 to 3 students, to provide focused guidance during their first medication administration experiences.
Adjusting as Competency Grows
As students demonstrate increased proficiency, the supervision ratio can be cautiously expanded, taking into account the instructor’s judgment and confidence in the students’ abilities.
References
College of Nurses of Ontario. (2024). Medication Decision Tool. Retrieved from https://www.cno.org/en/learn-about-standards-guidelines/educational-tools/decision-tool-medication/
Disclaimer
Suggestions based on expert clinical experience and application of CNO Standards of Practice.
Guided Clinical Experiences in Medication Administration
V

In the clinical setting, closely supervise and guide students through the medication administration process. Early on, this might involve walking them through each step and even taking on some aspects of the medication administration. As the students gain confidence and competence, the clinical instructor should step back and let them take more initiative, while remaining available for consultation.
Incremental Responsibility/Layering
Gradually increase the level of responsibility given to students, allowing them to make decisions under supervision. Start with simpler medications and procedures, moving to more complex situations as their confidence and competence grow.
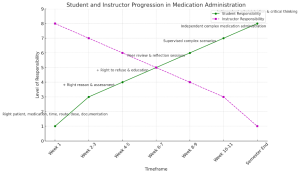
This diagram includes a visual representation of both student and clinical instructor responsibilities in the medication administration process. The green line illustrates the student’s progression, starting with foundational skills and gradually taking on more responsibility as they gain confidence and competence. The magenta dashed line represents the clinical instructor’s responsibility, which is initially high, covering the skills and tasks not yet taken on by the student. As the semester progresses and the student becomes more independent, the instructor’s direct responsibility decreases, shifting towards more of a supervisory and support role. This visual representation underscores the dynamic balance between teaching, supervision, and the gradual transition of responsibility from instructor to student in the clinical learning environment.
Initial Phase: Mastering PO Medications
Direct Guidance on PO Medication Administration
Initially, clinical instructors closely supervise students administering oral medications. This might involve the clinical instructor walking a student through the process of verifying the prescriber’s orders, double-checking patient allergies, calculating doses if necessary, and ensuring adherence to the “10 rights” of medication administration, which the clinical instructor may take some on instead of the student.
Demonstrations and Hands-On Practice
Under certain circumstances or upon student request, clinical instructors may demonstrate techniques for administering various forms of medications, including tablets, capsules, and liquids, and address how to manage patients with swallowing difficulties. Students then practice these skills, for instance, preparing a liquid antibiotic dose for a patient, under the instructor’s watchful eye.
Progression to More Complex Administration Routes
Introduction to Parenteral Routes
As students display proficiency with non-parenteral medications, they are ready to be introduced to more complex administration routes such as subcutaneous (SubCut), intramuscular (IM), and intravenous (IV) medication. Initially learning these routes in the class and lab environments, they will then begin to administer them in the clinical environment. Supervision might focus on the principles of aseptic technique, needle selection, and site rotation among other safety considerations during actual medication administration.
Supervised Practice with Parenteral routes
A student might learn to administer SC anticoagulants or insulins, or IM injections. Initially, the instructor might have the student practice the steps before the student performs the injection under close supervision.
Managing IV Medications

The transition to IV medications involves understanding IV pump operation, calculating drip rates, and mixing IV medications according to sterile procedures. A guided experience might start with an instructor demonstrating how to set up an IV antibiotic, followed by the student preparing and administering an IV saline flush under supervision.
Continuous Support and Advanced Scenarios
Encouraging Autonomy with Safety Net
- Even as students gain independence, clinical instructors stay accessible for queries and support. This ensures students feel confident to take initiative, knowing guidance is available if complex situations arise, like adjusting medication plans for patients with renal impairment.
- The clinical instructor will determine when the student has achieved an adequate level of competency in medication administration to practice under the supervision of a staff nurse, providing this is a mutual agreement and as per CNO practice standards.
- Scenario-Based Learning for Complex Care: Clinical instructors might present scenarios requiring students to manage patients with multiple medications across different routes, challenging them to prioritize care and monitor for interactions and side effects. For example, managing a patient’s transition from IV pain medication to PO analgesics post-surgery, requiring adjustments based on pain assessment and side effect monitoring.
Documentation of Medications
Direct Guidance of Medication Documentation
Initially, clinical instructors closely supervise students’ documentation of any administered, held or refused medications. This might involve the clinical instructor walking a student through the process and ensuring adherence to the policy of medication documentation. As students demonstrate proficiency in documentation, the clinical instructor must still ensure accurate documentation has occurred, as per CNO.

Debriefing, Feedback and Reflective Practice
VI
Debriefing, feedback, and reflective practice are essential components following medication administration in a clinical learning environment. They serve as a powerful trio that promotes learning and improvement. Debriefing helps students and clinical instructors analyze what transpired, understand outcomes, and identify areas for improvement. It enables the translation of experiences into actionable insights. Debriefing can occur immediately after the medication administration or as part of post conference discussion.

Feedback from clinical instructors is critical for reinforcing positive actions and correcting missteps, ensuring that students understand the practical implications of their actions. Feedback should be given individually, in private, after consent from the student has been obtained (If a student is not ready to receive feedback at that moment, then negotiate a more favorable time within the same day).
Reflective practice further engrains the learning, empowering students to self-assess and internalize lessons, fostering a mindset geared towards continuous personal and professional development.
The 3D Model of Debriefing, which stands for Defusing, Discovering, and Deepening, offers a structured approach to reflection and learning from experiences. This model can be particularly effective following medication administration sessions in clinical settings, helping both clinical instructors and students to reflect on the experience, understand the learning outcomes, and identify areas for improvement.
Here are some guidelines for conducting a post-medication administration debriefing using the 3D model:
Defusing
Objective
To reduce tension and normalize the emotional climate, making it conducive to open discussion.
Guidelines
- Start with a brief relaxation exercise or a few moments of silence to allow everyone to calm down and collect their thoughts.
- Acknowledge the emotional aspects of the experience, allowing students to express initial feelings about the medication administration process in a safe environment.
- Emphasize that the debriefing is a non-judgmental space focused on learning and growth.
Discovering
Objective
To explore the events and actions taken during the medication administration process, focusing on understanding what happened and why.
Guidelines
- Ask open-ended questions to guide students through a reflective analysis of the medication administration experience. For example, “What was your thought process when selecting the medication?” or “How did you ensure you were administering the medication safely?”
- Encourage students to describe their actions, decisions, and any challenges they encountered. Highlight both positive outcomes and areas where there was a deviation from the expected process.
- Facilitate a discussion on the rationale behind medication administration practices, including the importance of the 10 rights, patient interaction, and response monitoring.
Deepening
Objective
To consolidate learning by connecting the experience to broader nursing principles and identifying future learning opportunities.
Guidelines
- Guide students to reflect on how this experience has impacted their understanding of safe medication administration and patient care.
- Discuss how the lessons learned can be applied to future clinical situations. For example, “How will this experience influence your approach to checking patient allergies or confirming patient identity in the future?”
- Set specific, actionable goals for improvement, such as practicing medication calculations or developing strategies for managing anxiety during medication administration.
- Conclude the debriefing by summarizing key learnings and affirming the value of continuous improvement and reflection in clinical practice.
Examples of Feedback Models
When guiding students through their clinical education, it is important to offer feedback in a way that is structured and encourages learning and growth. There are many feedback models and techniques available:
Constructive Feedback Model
Emphasizes offering feedback that is specific, objective, and actionable, enabling students to understand their performance clearly and how to improve it.
How the Best Clinical Educators Give Feedback https://www.keithrn.com/2017/10/student-feedback/
Shared Responsibility Model
Views feedback as a collaborative process where both students and instructors share the responsibility. This model encourages students to actively seek feedback, engage in reflective practices, and implement suggestions for improvement.
Shared Responsibility Model https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8182567/
Situation, Behavior, Impact model (SBI)
This is a particularly effective method. It’s designed to be specific, objective, and aimed at fostering improvement.
- Situation: We start by pinpointing the exact moment the behavior was observed. This grounds the conversation in a shared reality, ensuring everyone is on the same page about when and where the feedback applies.
- Behavior: Here, objectively describe what was observed, focusing strictly on actions and words without inferring motives or casting judgments. This step is crucial for maintaining a constructive tone.
- Impact: The conversation then shifts to the effect of the observed behavior. Whether positive or negative, discussing the impact helps the receiver grasp the significance of their actions and the ripple effects they have on others and the broader environment.
Examples Using the SBI model
For clinical instructors, applying this model can significantly enhance feedback sessions. Here’s how it might look in practice:
Corrective feedback example
Situation
Initiate with a clear reference to the observed event. E.g., “In today’s medication round, when you were administering the IM injection to Mr. Smith…”
Behavior
Detail the behavior without bias. E.g., “I noticed you didn’t fully explain the procedure to the patient before administering the injection, and your technique seemed hurried”
Impact
Clarify the consequences of the behavior. E.g., “Mr. Smith seemed anxious, uncomfortable and surprised that he was getting an injection”
Positive feedback example
Situation
“This morning, when you were giving medications…”
Behavior
“You checked the patient’s ID carefully and explained the meds clearly.”
Impact
“This made sure the patient got the right treatment and felt informed. Great work!”
This feedback is concise and gets straight to the point, highlighting the student’s correct actions and their positive impact on patient care.
After laying out the SBI framework, discuss possible improvements and collaboratively develop a plan for skill enhancement, including practice sessions, additional readings, or setting specific objectives for future clinical tasks. This approach not only clarifies areas for improvement but also empowers students to actively engage in their learning journey, fostering a more enriching educational experience.
How do you use the SBI (situation, behavior, impact) model to deliver clear and specific feedback?
Encourage Reflective Practice
Invite the student to reflect on the situation and consider alternative actions they might take in the future. This encourages critical thinking and self-assessment. Reflective practice may occur through dialogue or as a written practice.
Feedback in the clinical setting – PMC (nih.gov)
https://www.mindtools.com/ay86376/the-situation-behavior-impact-feedback-tool
How to Give Clear Feedback with the SBI Model (linkedin.com)
Zigmont, P. D., Jason J., Kappus, M. E., Liana J., & Sudikoff, M. D., Stephanie N. (2011). The 3D Model of Debriefing: Defusing, Discovering, and Deepening. Seminars in Perinatology, 35(2), 52–58.
Challenging Situations
VII
Dealing with challenging student situations during medication administration requires a blend of patience, clear communication, and strategic intervention from clinical instructors. Next are some common scenarios and suggestions for handling them effectively.
Scenario
A student arrives for their clinical rotation and demonstrates a lack of readiness to perform medication administration, such as not understanding medication dosages or the assigned rights of medication administration.
Handling Strategy
Immediate Feedback and Support
Address the lack of preparation with the student privately, expressing concern for patient safety and the importance of being prepared.
Remedial Learning
Assign specific tasks or readings to improve their knowledge and understanding. This could include reviewing medication calculations or the knowledge of assigned medications.
Supervised Practice
Provide opportunities for the student to observe medication administration closely before attempting it again under direct supervision.
Student Refuses to Participate
Scenario
A student refuses to participate in medication administration tasks, citing anxiety, lack of confidence, feeling unprepared or not engaged in learning.
Handling Strategy
Understanding and Empathy
Have a private conversation to understand the root causes of their reluctance. Acknowledge their feelings and stress the importance of facing these challenges for their growth and patient care.
Gradual Exposure
Start with less complex medication administration tasks to build their confidence. Pair them with a more experienced peer for shadowing or assisting initially.
Mentoring and Encouragement
Provide positive reinforcement and constructive feedback to build their confidence. Share personal experiences or stories of overcoming similar challenges.
Student Makes a Medication Error
Scenario
A student makes a medication error, such as administering the wrong dosage or wrong medication to a patient.
Handling Strategy
Immediate Correction and Reporting
Check-in with the student’s emotional wellbeing. Ensure the student follows the facility’s protocol for medication errors, including reporting the error to the necessary healthcare team members and documenting it appropriately.
Reflective Learning
Use the incident as a learning opportunity, discussing what went wrong and how it can be prevented in the future without assigning blame. Identify root causes such as interruptions, system failures, lack of clarity, time pressures.
Supportive Follow-up
Monitor the student’s emotional response to the error and provide support, emphasizing that errors are part of the learning process and the importance of learning from them.
Student Demonstrates Lack of Confidence
Scenario
A student consistently expresses a lack of confidence in their ability to administer medications safely, affecting their performance.
Handling Strategy
Positive Reinforcement
Highlight what the student is doing right and provide praise for their efforts and successes, no matter how small.
Skill Building
Identify specific areas for improvement and provide resources or additional practice opportunities in these areas.
Peer Support
Encourage peer learning opportunities where the student can observe and learn from classmates, fostering a supportive learning environment.
Student Challenges Clinical Practices
Scenario
A student questions or challenges the medication administration practices at the clinical site, based on their theoretical knowledge or previous experiences.
Handling Strategy
Open Discussion
Encourage a respectful dialogue where the student can express their concerns and provide evidence-based reasoning for the current clinical practices.
Educational Insight
Use this as an opportunity to discuss the rationale behind different practices and the importance of evidence-based care. Highlight how practices may vary between settings due to policy, patient population, or resource availability.
Professional Development
Stress the importance of adaptability and continuous learning in nursing practice, encouraging the student to keep an open mind and learn from the diverse approaches observed in clinical settings.
Koharchik, L,. & Flavin, M.L. (2017). Teaching for Practice. The American Journal of Nursing, 117, 62-66.
Parvan, K., Hosseini, F., & Bagherian, S. (2018). The relationship between nursing instructors’ clinical teaching behaviors and nursing students’ learning in Tabriz University of Medical Sciences in 2016. Education for Health (Abingdon, England), 31(1), 32–38.
Reid-Searl, K., Moxham, L., Walker, S., & Happell, B. (2010). Nursing students administering medication: appreciating and seeking appropriate supervision. Journal of Advanced Nursing, 66(3), 532–541.
Valdez, L. P. M., de Guzman, A. B., & Escolar-Chua, R. L. (2013). Every move counts in learning: Filipino clinical instructors’ scaffolding behaviors in teaching medication administration. Nurse Education Today, 33(10), 1214–1218.
Interactive and Supportive Strategies for Teaching Medication Administration
Discussions for Post Conference
Exploration of Common Diagnoses and Medications
Design an activity where students research and present on the top 10 diagnoses or co-morbidities and the top 15-20 medications commonly encountered in the clinical area. This task encourages familiarity with frequent health conditions and their pharmacological management, linking clinical practice to patient care scenarios. See Appendix for example
Case Studies and Problem-Solving Exercises
Employ post-conference time to delve into case studies that showcase potential complications and ethical challenges in medication administration. Encourage students to participate in problem-solving exercises, fostering critical thinking and discussion on navigating complex situations.
Peer Learning Opportunities
Facilitate environments for peer learning where students can exchange and benefit from each other’s experiences and insights. This can involve paired or group tasks in clinical settings, peer evaluation of medication plans, or discussion circles, enhancing collaborative learning.
Encouraging Questioning and Critical Thinking
Nurture a setting that promotes questioning and critical analysis. Motivate students to inquire about and critically evaluate the actions and principles behind medication administration practices, deepening their understanding and application of these practices.
Use of Checklists and Protocols
Introduce checklists and protocols related to medication administration early in training. These aids help ensure adherence to safety and accuracy, supporting students in remembering and applying key steps in the medication administration process.
Discussion of common medication errors and organizational strategies to prevent them
Review protocols, policies, and restrictions. Explore factors that contribute to errors such as noise, time constraints, lighting, how orders are entered.
To facilitate putting all of these strategies together, a downloadable resource has been provided: Medication Administration Planner (1)
Top 10 Medical conditions and the common medication therapies
| Condition |
Common Medications |
Medication Action |
Notes/Considerations |
| Pneumonia and Lower Respiratory Infections |
– Antibiotics (e.g., amoxicillin, azithromycin, levofloxacin) |
Fight bacterial infection |
Review culture and sensitivity results |
|
– Antipyretics (e.g., acetaminophen) |
Reduce fever and alleviate pain |
Reassess temperature/ pain level |
| Heart Failure |
– Diuretics (e.g., furosemide, spironolactone) |
Reduce fluid overload by increasing urine production |
Monitor electrolytes and renal function. |
|
– ACE inhibitors (e.g., lisinopril) or ARBs (e.g., losartan) |
Lower blood pressure and decrease workload on the heart |
Monitor for hypotension and renal function changes. |
|
– Beta-blockers (e.g., carvedilol, metoprolol) |
Slow heart rate and reduce blood pressure |
Start low and go slow, especially in acute exacerbations. |
| COPD Exacerbations |
– Bronchodilators (e.g., albuterol, ipratropium) |
Relax muscles in the airways and increase air flow to the lungs |
Use as needed for symptom control. |
|
– Corticosteroids (e.g., prednisone) |
Reduce inflammation in the airways |
Short courses for acute exacerbations. |
|
– Antibiotics (if bacterial infection is suspected) |
Fight bacterial infection |
Based on clinical signs of bacterial infection. |
| Acute Coronary Syndromes |
– Antiplatelets (e.g., aspirin, clopidogrel) |
Prevent blood clots |
Essential for all patients unless contraindicated. |
|
– Statins (e.g., atorvastatin) |
Lower cholesterol and stabilize plaque |
Initiate early in management. |
|
– Beta-blockers |
Reduce myocardial oxygen demand |
Monitor heart rate and blood pressure. |
|
– Nitroglycerin |
Dilate coronary arteries and relieve chest pain |
Use for chest pain relief and coronary artery dilation. |
| Complications of Diabetes |
– Insulin |
Lower blood glucose levels |
Close monitoring of blood glucose levels is necessary. |
| Gastrointestinal Bleeds |
– Proton pump inhibitors (e.g., omeprazole) |
Reduce stomach acid production |
Administer IV for acute bleeds. |
|
– Blood transfusions (if necessary) |
Replace lost blood |
Based on hemoglobin levels and clinical status. |
| Acute Kidney Injury |
Adjustments or discontinuation of nephrotoxic medications |
Support kidney function and prevent further damage |
Monitor renal function and adjust medications as necessary. |
| Sepsis and Septic Shock |
– Broad-spectrum antibiotics |
Combat widespread infection |
Early initiation is critical for outcomes. |
|
– Vasopressors (e.g., norepinephrine) |
Increase blood pressure to critical organs |
For maintaining adequate blood pressure after initial management. |
| Stroke (CVA) |
– Thrombolytics (e.g., alteplase) |
Dissolve blood clots in the brain |
For eligible patients with ischemic stroke within the therapeutic window. |
|
– Antiplatelets (e.g., aspirin) |
Prevent further clot formation |
Prevent secondary stroke prevention. |
|
– Statins |
Lower cholesterol and prevent further arterial plaque buildup |
For cholesterol management and secondary prevention. |
| DVT and PE |
– Anticoagulants (e.g., heparin, warfarin, DOACs like apixaban) |
Prevent and treat blood clots |
Long-term anticoagulation based on guidelines. |
Al Mutair, A., Ambani, Z., & Bashiri, F. A. (2021). The Effective Strategies to Avoid Medication Errors and Improving Reporting. NCBI. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8468915/
Al Mutair, A., & Ambani, Z. (2021). Medication error and patient safety. PubMed. https://pubmed.ncbi.nlm.nih.gov/34564088/
Tariq, R. A., Vashisht, R., & Sinha, A. (2022). Medication Dispensing Errors and Prevention. NCBI. https://www.ncbi.nlm.nih.gov/books/NBK519065/
Rodziewicz, T. L., & Hipskind, J. E. (2022). Medical Error Reduction and Prevention. NCBI. https://www.ncbi.nlm.nih.gov/books/NBK499956/
Elden, N. M. K., & Ismail, A. (2016). The Importance of Medication Errors Reporting in Improving the Quality of Clinical Care Services. NCBI. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5016354/

